
Human Acellular Dermal Matrix in Reconstructive Surgery—A Review
 , ,
, ,  and
and
Abstract
:1. Introduction
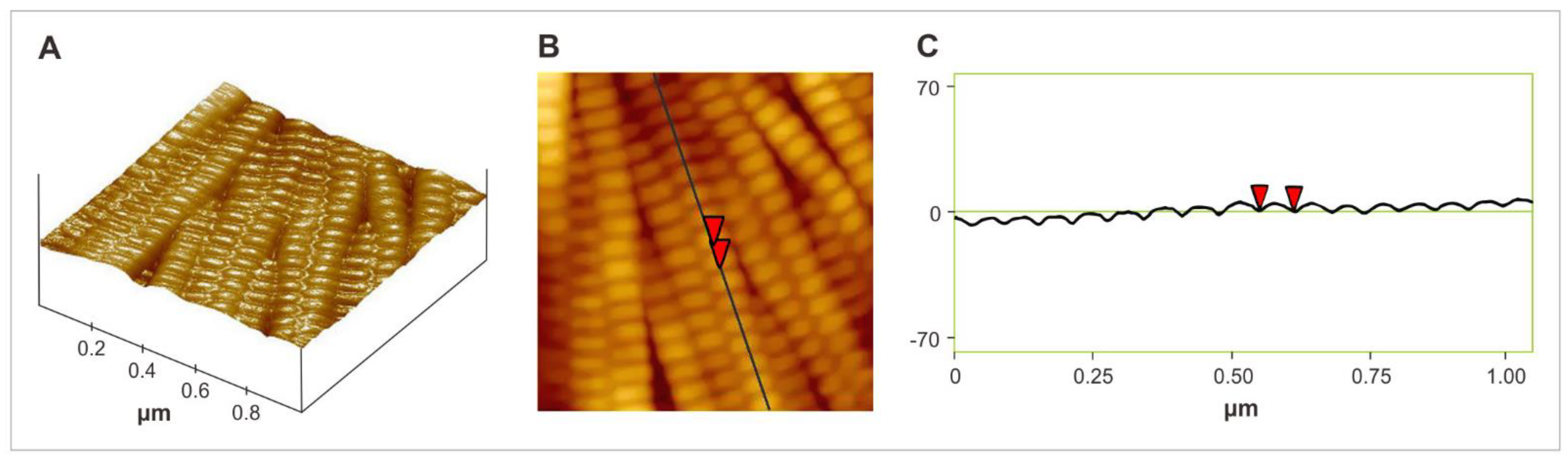
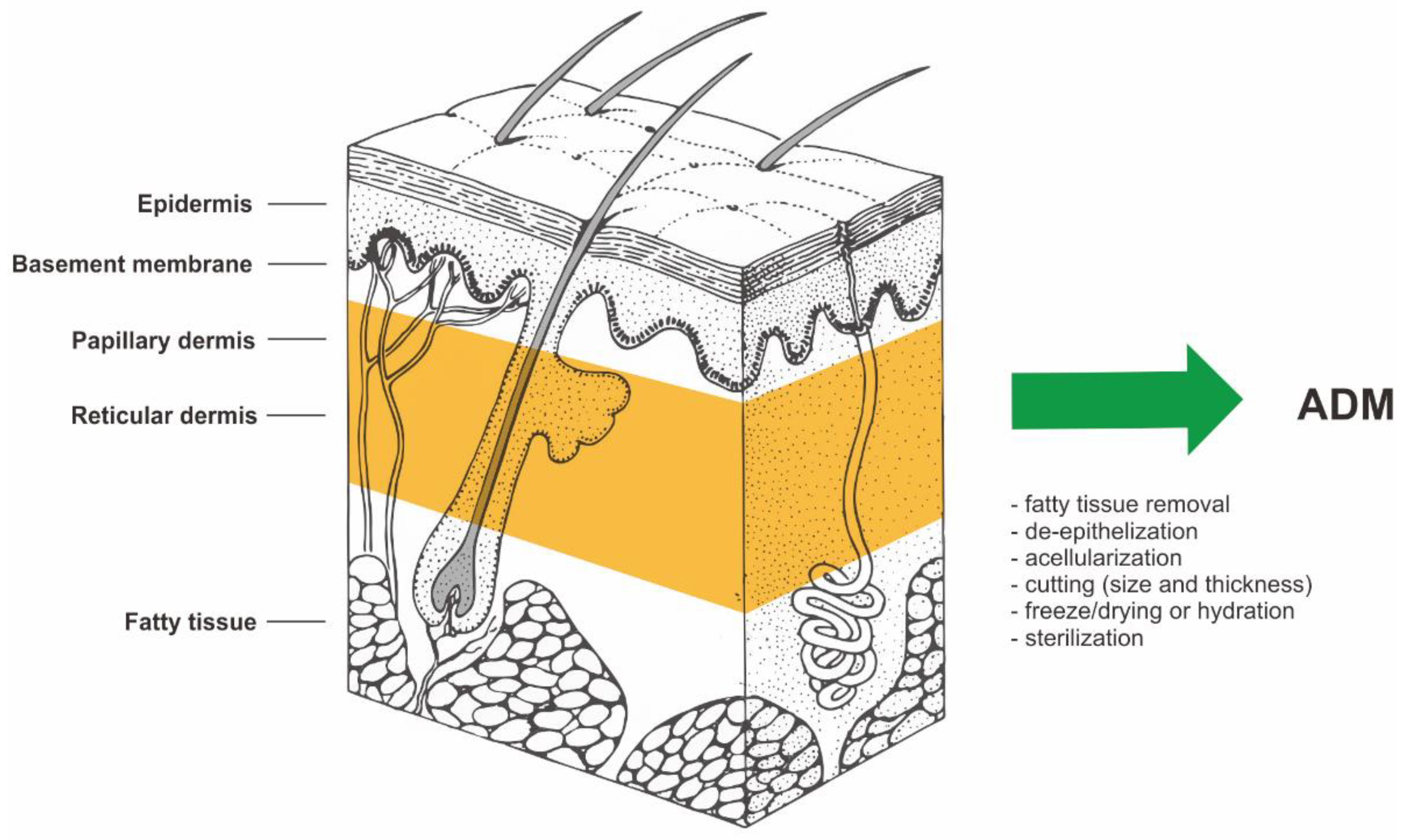
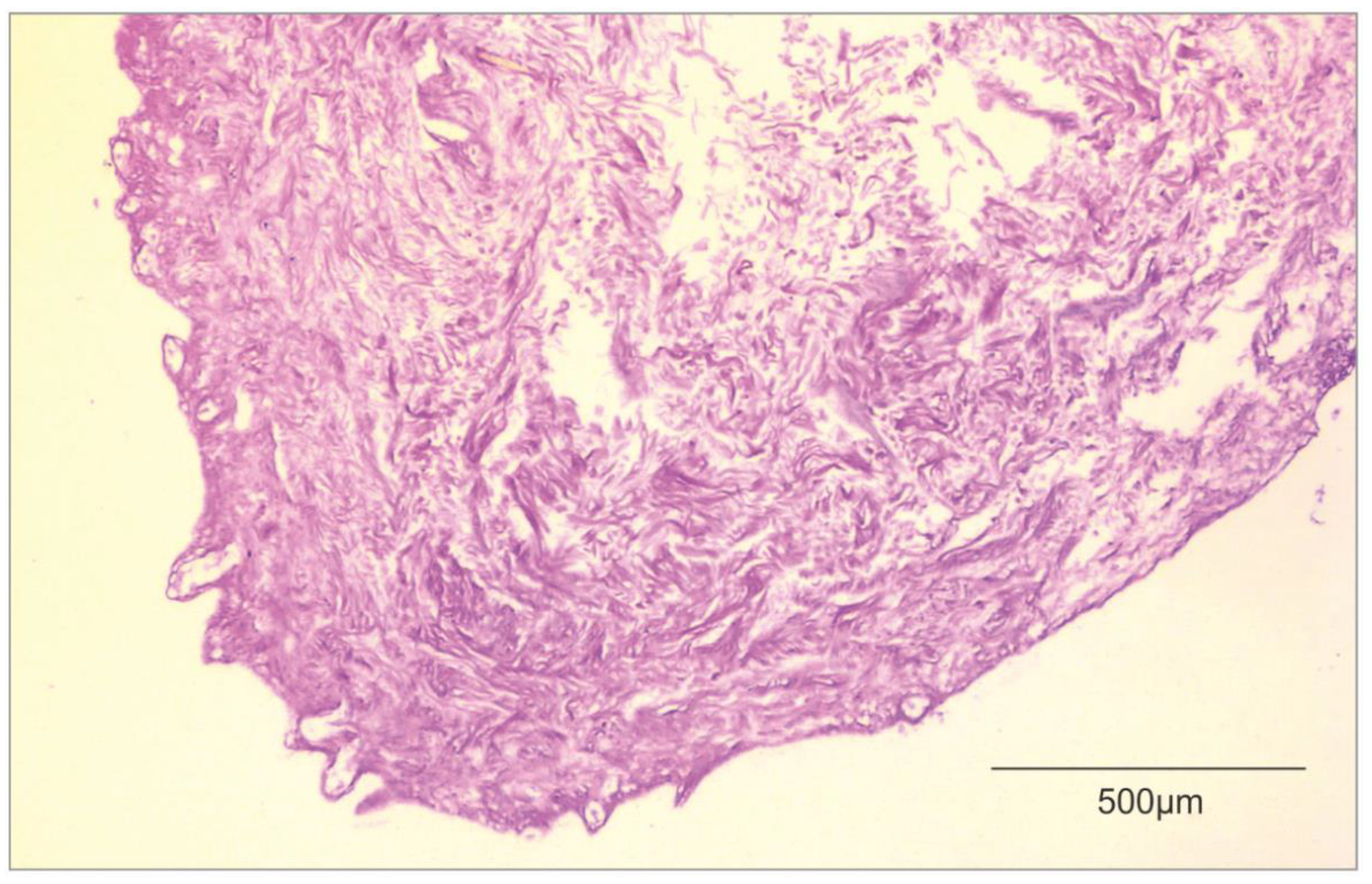
2. Decellularization of Human Allogeneic Skin
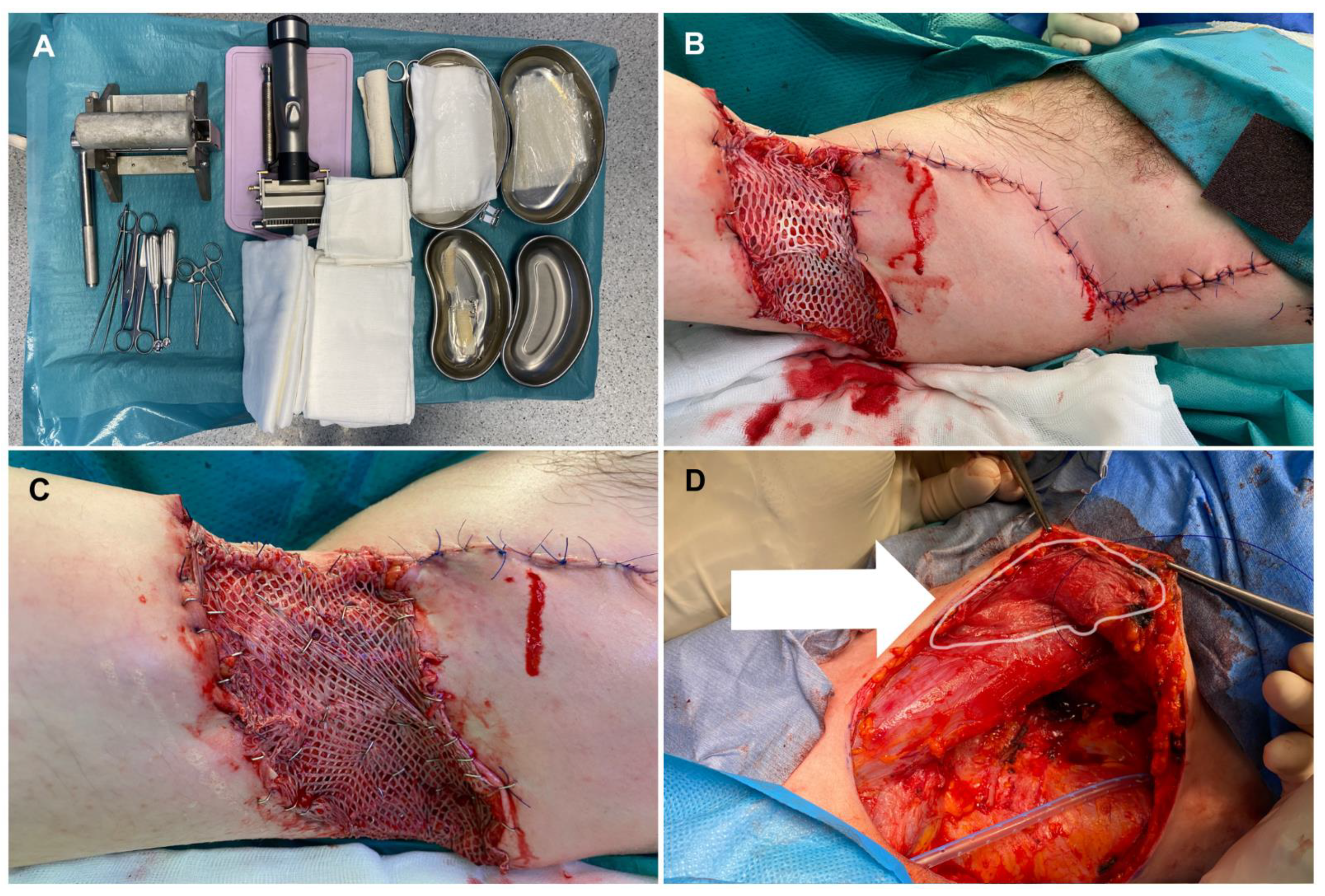
3. Burns and Wound Management
4. Reconstructive Breast Procedures
5. Hernia Repair
6. Reconstructive Gynecology
7. Other Surgical Applications
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crapo, P.M.; Gilbert, T.W.; Badylak, S.F. An overview of tissue and whole organ decellularization processes. Biomaterials 2011, 32, 3233. [Google Scholar] [CrossRef] [Green Version]
- Gierek, M.; Kawecki, M.; Mikuś, K.; Klama-Baryła, A.; Nowak, M. Biological dressings as a substitutes of the skin in the treatment of burn wounds. Pol. Przegląd Chir. 2013, 85, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keane, T.J.; Swinehart, I.T.; Badylak, S.F. Methods of tissue decellularization used for preparation of biologic scaffolds and in vivo relevance. Methods 2015, 84, 25. [Google Scholar] [CrossRef] [Green Version]
- Brown, B.N.; Freund, J.M.; Han, L.; Rubin, J.P.; Reing, J.E.; Jeffries, E.M.; Wolf, M.T.; Tottey, S.; Barnes, C.A.; Ratner, B.D.; et al. Comparison of Three Methods for the Derivation of a Biologic Scaffold Composed of Adipose Tissue Extracellular Matrix. Tissue Eng. Part C Methods 2011, 17, 411. [Google Scholar] [CrossRef]
- Brown, B.N.; Badylak, S.B. Extracellular matrix as an inductive scaffold for functional tissue reconstruction. Transl. Res. 2014, 163, 268. [Google Scholar] [CrossRef] [Green Version]
- Łabuś, W.; Kawecki, M.; Glik, J.; Maj, M.; Kitala, D.; Misiuga, M.; Klama-Baryła, A.; Kraut, M.; Nowak, M. Own experience from the use of a substitute of an allogeneic acellular dermal matrix revitalized with in vitro cultured skin cells in clinical practice. Pol. Przegląd Chir. 2015, 10, 929. [Google Scholar] [CrossRef]
- Vorotnikova, E.; McIntosh, D.; Dewilde, A.; Zhang, J.; Reing, J.E.; Zhang, L. Extracellular matrix derived products modulate endothelial and progenitor cell migration and proliferation in vitro and stimulate regenerative healing in vivo. Matrix Biol. 2010, 29, 690–700. [Google Scholar] [CrossRef]
- Barkan, D.; Green, J.E.; Chambers, A.F. Extracellular matrix: A gatekeeper in the transition from dormancy to metastatic growth. Eur. J. Cancer 2010, 46, 1181–1188. [Google Scholar] [CrossRef] [Green Version]
- Łabuś, W.; Kawecki, M.; Nowak, M. The role of tissue engineering in the treatment of burn wounds. Pol. Przegląd Chir. 2012, 3, 167–171. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://visualsonline.cancer.gov/details.cfm?imageid=2496 (accessed on 1 January 2001).
- Carson, A.E.; Barker, T.H. Emerging concepts in engineering extracellular matrix variants for directing cell phenotype. Regen. Med. 2009, 4, 593–600. [Google Scholar] [CrossRef]
- Ott, H.C.; Matthiesen, T.S.; Goh, S.K.; Black, L.D.; Kren, S.M.; Netoff, T.I. Perfusiondecellularized matrix: Using nature’s platform to engineer a bioartificial heart. Nat. Med. 2008, 14, 213–221. [Google Scholar] [CrossRef]
- Uygun, B.E.; Soto-Gutierrez, A.; Yagi, H.; Izamis, M.L.; Guzzardi, M.A.; Shulman, C. Organ reengineering through development of a transplantable recellularized liver graft using decellularized liver matrix. Nat. Med. 2010, 16, 814–820. [Google Scholar] [CrossRef]
- Livesey, S.A.; Herndon, D.N.; Hollyoak, M.A.; Atkinson, Y.H.; Nag, A. Transplanted acellular allograft dermal matrix. Potential as a template for the reconstruction of viable dermis. Transplantation 1995, 60, 1–9. [Google Scholar] [CrossRef]
- Clark, J.M.; Saffold, S.H.; Israel, J.M. Decellularized dermal grafting in cleft palate repair. Arch. Facial Plast. Surg. 2003, 5, 40–44. [Google Scholar] [CrossRef]
- Wainwright, D.; Madden, M.; Luterman, A. Clinical evaluation of an acellular allograft dermal matrix in full-thickness burns. J. Burn Care Rehabil. 1996, 17, 124–136. [Google Scholar] [CrossRef]
- Schwanholt, C.; Greenhalgh, D.G.; Warden, G.D. A comparison of full-thickness versus split- thickness autografts for the coverage of deep palm burns in the very young pediatric patient. J. Burn Care Rehabil. 1993, 14, 29–33. [Google Scholar] [CrossRef]
- Wainwright, D.J. Use of an acellular allograft dermal matrix (AlloDerm) in the management of full-thickness burns. Burns 1995, 21, 243–248. [Google Scholar] [CrossRef]
- Freitas-Silva, R.; Conde, D.M.; de Freitas-Junior, R.; Martinez, E.Z. Comparison of quality of life, satisfaction with surgery and shoulder-arm morbidity in breast cancer survivors submitted to breast-conserving therapy or mastectomy followed by immediate breast reconstruction. Clinics 2010, 65, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Rawlani, V.; Buck, D.W., 2nd; Johnson, S.A.; Heyer, K.S.; Kim, J.Y. Tissue expander breast reconstruction using prehydrated human acellular dermis. Ann. Plast. Surg. 2011, 66, 593–597. [Google Scholar] [CrossRef] [Green Version]
- Cuomo, R. Submuscular and pre-pectoral ADM assisted immediate breast reconstruction: A literature review. Medicina 2020, 56, 256. [Google Scholar] [CrossRef]
- Duncan, D.I. Correction of implant rippling using allograft dermis. Aesthetic Surg. J. 2001, 21, 81–84. [Google Scholar] [CrossRef]
- Breuing, K.H.; Warren, S.M. Immediate bilateral breast reconstruction with implants and infero- lateral AlloDerm slings. Ann. Plast. Surg. 2005, 55, 232–239. [Google Scholar] [CrossRef]
- Fosnot, J.; Kovach, S.J.; Scarlatti, J.M. Acellular Dermal Matrix: General Principles for the Plastic Surgeon. Aesthetic Surg. J. 2011, 31 (Suppl. 7), 5S–12S. [Google Scholar] [CrossRef] [Green Version]
- Tevlin, R.; Borrelli, M.R.; Irizarry, D.; Nguyen, D.; Wan, D.C.; Momeni, A. Acellular Dermal Matrix Reduces Myofibroblast Presence in the Breast Capsule. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2213. [Google Scholar] [CrossRef]
- Hartzell, T.L.; Taghinia, A.H.; Chang, J.; Lin, S.J.; Slavin, S.A. The use of human acellular dermal matrix for the correction of secondary deformities after breast augmentation: Results and costs. Plast. Reconstr. Surg. 2010, 126, 1711–1720. [Google Scholar] [CrossRef]
- McCarthy, C.M.; Lee, C.N.; Halvorson, E.G. The use of acellular dermal matrices in two-stage expander/implant reconstruction: A multicenter, blinded, randomized controlled trial. Plast. Reconstr. Surg. 2012, 130 (Suppl. 2), 57S–66S. [Google Scholar] [CrossRef] [Green Version]
- Davila, A.A.; Seth, A.K.; Wang, E. Human acellular dermis versus submuscular tissue expander breast reconstruction: A multivariate analysis of short-term complications. Arch. Plast. Surg. 2013, 40, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Mendenhall, S.D.; Anderson, L.A.; Ying, J. The BREASTrial: Stage I. Outcomes from the time of tissue expander and acellular dermal matrix placement to definitive reconstruction. Plast. Reconstr. Surg. 2015, 135, 29e–42e.v. [Google Scholar] [CrossRef]
- Allergan. Company Document. Important Information for Women About Breast Augmenta-Tion with Natrelle® Gel-Filled Breast Implants. 2015. Available online: http://www.allergan.com/assets/pdf/ca_natrelle_gel_aug_info_en.pdf (accessed on 1 January 2015).
- Lee, J.; Yang, J.D.; Lee, J.W.; Li, J.; Jung, J.H.; Kim, W.W.; Park, C.S.; Lee, J.S.; Park, H.Y. Acellular dermal matrix combined with oxidized regenerated cellulose for partial breast reconstruction: Two case reports. Medicine 2020, 99, e21217. [Google Scholar] [CrossRef]
- Gwak, H.; Jeon, Y.W.; Lim, S.T.; Park, S.Y.; Suh, Y.J. Volume replacement with diced acellular dermal matrix in oncoplastic breast-conserving surgery: A prospective single-center experience. World J. Surg. Oncol. 2020, 18, 60. [Google Scholar] [CrossRef]
- Broyles, J.M.; Liao, E.C.; Kim, J.; Heistein, J.; Sisco, M.; Karp, N.; Lau, F.H.; Chun, Y.S. Acellular Dermal Matrix-Associated Complications in Implant-Based Breast Reconstruction: A Multicenter, Prospective, Randomized Controlled Clinical Trial Comparing Two Human Tissues. Plast. Reconstr. Surg. 2021, 148, 493–500. [Google Scholar] [CrossRef]
- Zhu, K.Q.; Carrougher, G.J.; Gibran, N.S.; Isik, F.F.; Engrav, L.H. Review of the female Duroc/Yorkshire pig model of human fibroproliferative scarring. Wound Repair Regen. 2007, 15, S32–S39. [Google Scholar] [CrossRef] [Green Version]
- Diaz, J.J., Jr.; Conquest, A.M.; Ferzoco, S.J. Multi-institutional experience using human acellular dermal matrix for ventral hernia repair in a compromised surgical field. Arch. Surg. 2009, 144, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Candage, R.; Jones, K.; Luchette, F.A.; Sinacore, J.M.; Vandevender, D.; Reed, R.L. Use of human acellular dermal matrix for hernia repair: Friend or foe? Surgery 2008, 144, 703–709. [Google Scholar] [CrossRef]
- Garvey, P.B.; Martinez, R.A.; Baumann, D.P.; Liu, J.; Butler, C.E. Outcomes of abdominal wall recon- struction with acellular dermal matrix are not affected by wound contamination. J. Am. Coll. Surg. 2014, 219, 853–864. [Google Scholar] [CrossRef]
- Guerra, O. Noncrosslinked porcine-derived acellular dermal matrix for single-stage com- plex abdominal wall herniorrhaphy after removal of infected synthetic mesh: A retrospective review. Am. Surg. 2014, 80, 489–495. [Google Scholar] [CrossRef]
- Stanizzi, A.; Torresetti, M.; Salati, M.; Benedetto, G.D. Use of porcine acellular dermal matrix to repair lung Hernia after minithoracotomy: A case report with 6-Year follow-up. JPRAS Open 2021, 28, 56–60. [Google Scholar] [CrossRef]
- Lightfoot, R.W.; Thrash, C.; Thompson, S.; Richmond, B.K. A Comparison of Component Separation with Porcine Acellular Dermal Reinforcement to Bovine Acellular Dermal Matrix in the Repair of Significant Midline Ventral Hernia Defects. Am. Surg. 2021, 00031348211050844. [Google Scholar] [CrossRef]
- Peró, M.; Casani, L.; Castells-Sala, C. Rabbit as an animal model for the study of biological grafts in pelvic floor dysfunctions. Sci. Rep. 2021, 11, 10545. [Google Scholar] [CrossRef]
- Banacu, M.; Socea, B.; Palinaru, A.; Lascar, I. Extracellular Matrices in Gynecological Surgery—Literature Review. Arch. Balk. Med. Union 2020, 55, 304–311. [Google Scholar] [CrossRef]
- Ward, R.M.; Sung, V.W.; Clemons, J.L.; Myers, D.L. Vaginal paravaginal repair with an AlloDerm graft: Long-term outcomes. Am. J. Obstet. Gynecol. 2007, 197, e1–e5. [Google Scholar] [CrossRef]
- Clemons, J.L.; Myers, D.L.; Aguilar, V.C.; Arya, L.A. Vaginal paravaginal repair with an AlloDerm graft. Am. J. Obstet. Gynecol. 2003, 189, 1612–1618, discussion 1618-9. [Google Scholar] [CrossRef]
- Karon, M.; Chatterjee, S. Sacrocolpopexy: Patient Outcomes Support the Use of Non-Crosslinked Acellular Dermal Matrix as an Alternative to the Synthetic Polypropylene Mesh. J. Gynecol. Surg. 2019, 35, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.J.; Park, M.C.; Park, D.H.; Hahn, H.M.; Kim, S.M.; Lee, I.J. Effectiveness of Acellular Dermal Matrix on Autologous Split-Thickness Skin Graft in Treatment of Deep Tissue Defect: Esthetic Subjective and Objective Evaluation. Aesthetic Plast. Surg. 2017, 41, 1049–1057. [Google Scholar] [CrossRef]
- Chaffin, A.E.; Buckley, M.C. Extracellular matrix graft for the surgical management of Hurley stage III hidradenitis suppurativa: A pilot case series. J. Wound Care 2020, 29, 624–630. [Google Scholar] [CrossRef]
- Gierek, M.; Łabuś, W.; Słaboń, A.; Ziółkowska, K.; Ochała-Gierek, G.; Kitala, D.; Szyluk, K.; Niemiec, P. Co-Graft of Acellular Dermal Matrix and Split Thickness Skin Graft—A New Reconstructive Surgical Method in the Treatment of Hidradenitis Suppurativa. Bioengineering 2022, 9, 389. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of the Product (Commercial ADM) | Manufacturer | Origin | General Characteristics |
|---|---|---|---|
| AlloDerm | Lifecell Corp., USA | Human dermis | Intended to be used for repair or replacement of damaged tissue |
| Cymetra | Lifecell Corp., USA | Human dermis | Micronized AlloDerm tissue for injections |
| NeoForm | Mentor, USA | Human dermis | Used in breast surgery |
| DermaMatrix | Musculoskeletal Transplant Foundation and Synthesis, USA | Human dermis | Rehydrates very quickly, does not require refrigerated storage |
| Glyaderm | Euroskinbank, NL | Human dermis | Depending on the dimension of the patient’s wound, donor skin is available from 40 cm2 to 150 cm2. |
| Permacol, | Tissue Science Laboratories, USA | Porcine dermis | Used in hernia repair. Available in large sheets for abdominal wall use, cross-linked for enhanced durability. |
| Matriderm | Skin and Healthcare, USA | Bovine dermis | Used for skin defects |
| Pelnac | Gunze Corp., JP | Bovine dermis | Used for skin defects |
| Renoskin | Perouse Plastie, FR | Bovine dermis | Silicone outer layer; used for skin defects |
| Year of Publication | Reconstruction | Author/Number of Reference | General Information |
|---|---|---|---|
| 1995 | Burns | Livesey et al. [14] | First concept of ADM |
| 1995 | Burns | Wainwright et al. [18] | First use of ADM in burns |
| 2001 | Breast surgery | Duncan et al. [25] | First use of ADM in breast surgery |
| 2005 | Breast reconstruction (surgical oncology) | Breuing et al. [23] | First use of ADM after mastectomies |
| 2008 | Hernia repair | Candage et al. [36] | ADM as an alternative in synthetic mesh in hernia repair |
| 2014 | Hernia repair | Garvey et al. [37] | ADM is preventing the infection comparing to the synthetic mesh |
| 2003 | Reconstructive gynecology | Clemons et al. [44] | Paravaginal reconstruction using the AlloDerm |
| 2007 * | Reconstructive gynecology | Ward et al. [43] | Reconstruction of prolapsy with Alloderm |
| 2022 | Hidradenitis suppurativa | Gierek et al. [48] | First use of co-graft of ADM and STSG in hidradenitis suppurativa |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gierek, M.; Łabuś, W.; Kitala, D.; Lorek, A.; Ochała-Gierek, G.; Zagórska, K.M.; Waniczek, D.; Szyluk, K.; Niemiec, P. Human Acellular Dermal Matrix in Reconstructive Surgery—A Review. Biomedicines 2022, 10, 2870. https://doi.org/10.3390/biomedicines10112870
Gierek M, Łabuś W, Kitala D, Lorek A, Ochała-Gierek G, Zagórska KM, Waniczek D, Szyluk K, Niemiec P. Human Acellular Dermal Matrix in Reconstructive Surgery—A Review. Biomedicines. 2022; 10(11):2870. https://doi.org/10.3390/biomedicines10112870
Chicago/Turabian StyleGierek, Marcin, Wojciech Łabuś, Diana Kitala, Andrzej Lorek, Gabriela Ochała-Gierek, Karolina Mikuś Zagórska, Dariusz Waniczek, Karol Szyluk, and Paweł Niemiec. 2022. "Human Acellular Dermal Matrix in Reconstructive Surgery—A Review" Biomedicines 10, no. 11: 2870. https://doi.org/10.3390/biomedicines10112870