
Mitomycin C in Homologous Recombination Deficient Metastatic Pancreatic Cancer after Disease Progression on Platinum-Based Chemotherapy and Olaparib
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Genetic Information
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Cases
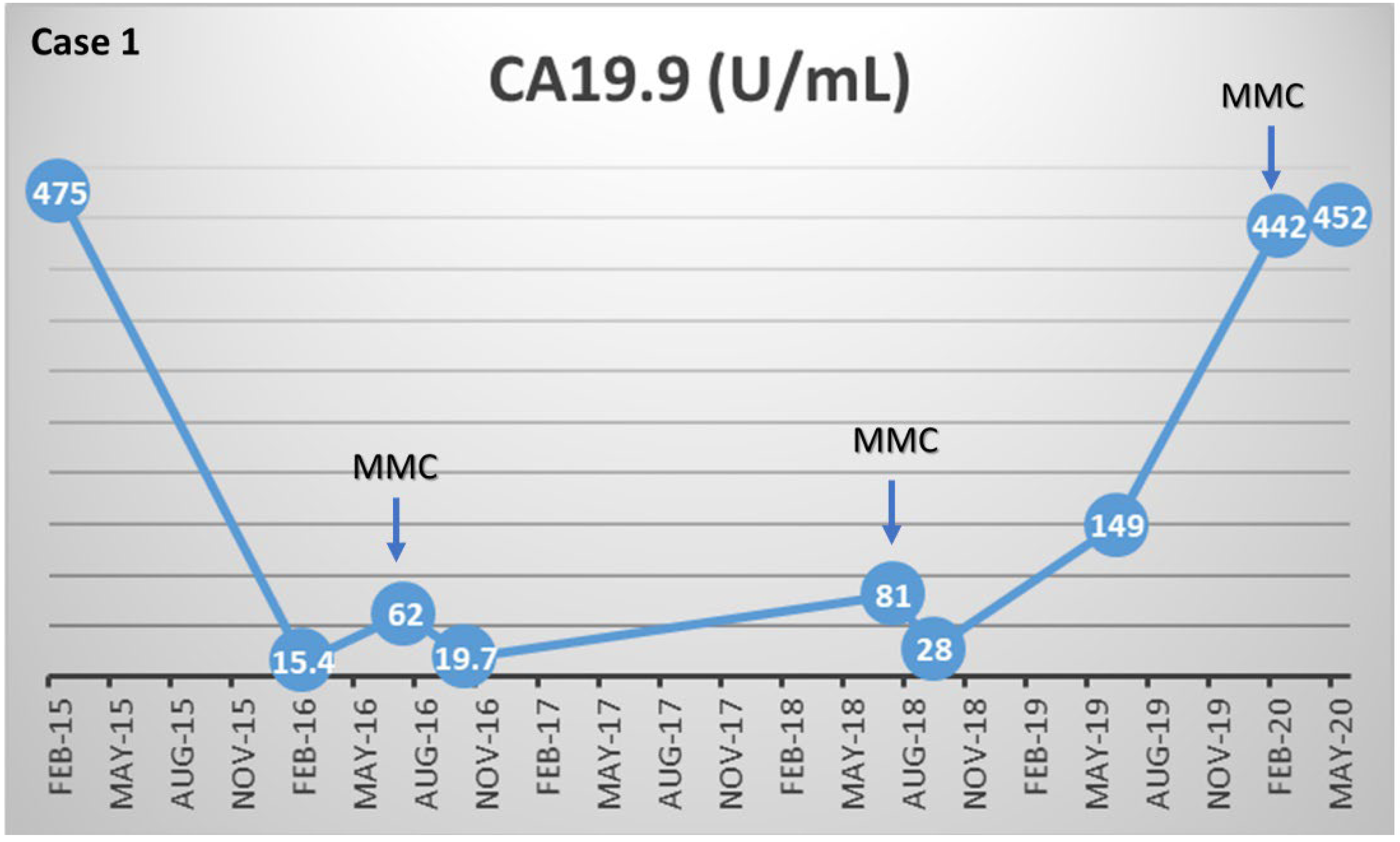
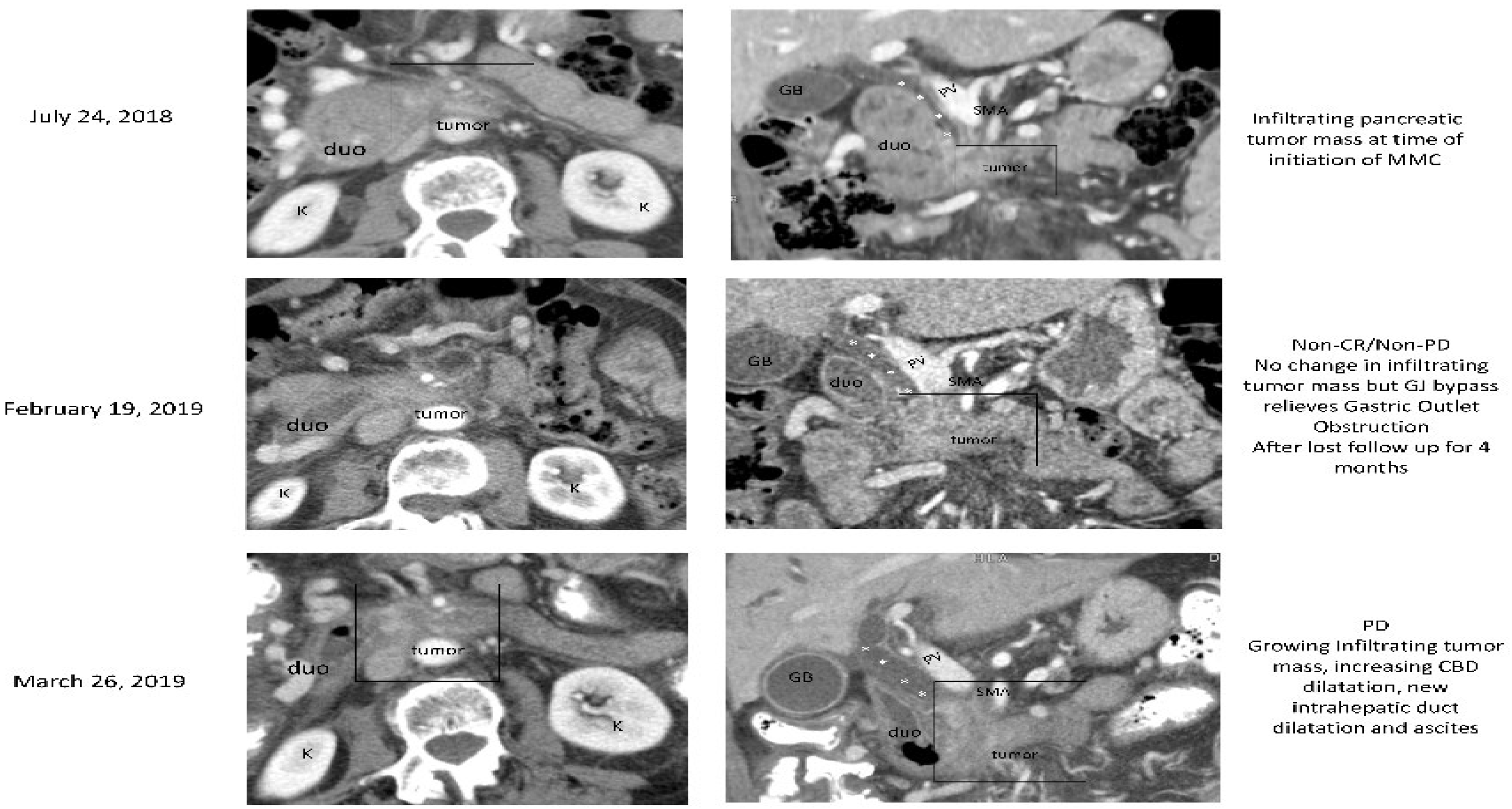
3.2.1. Case (1)
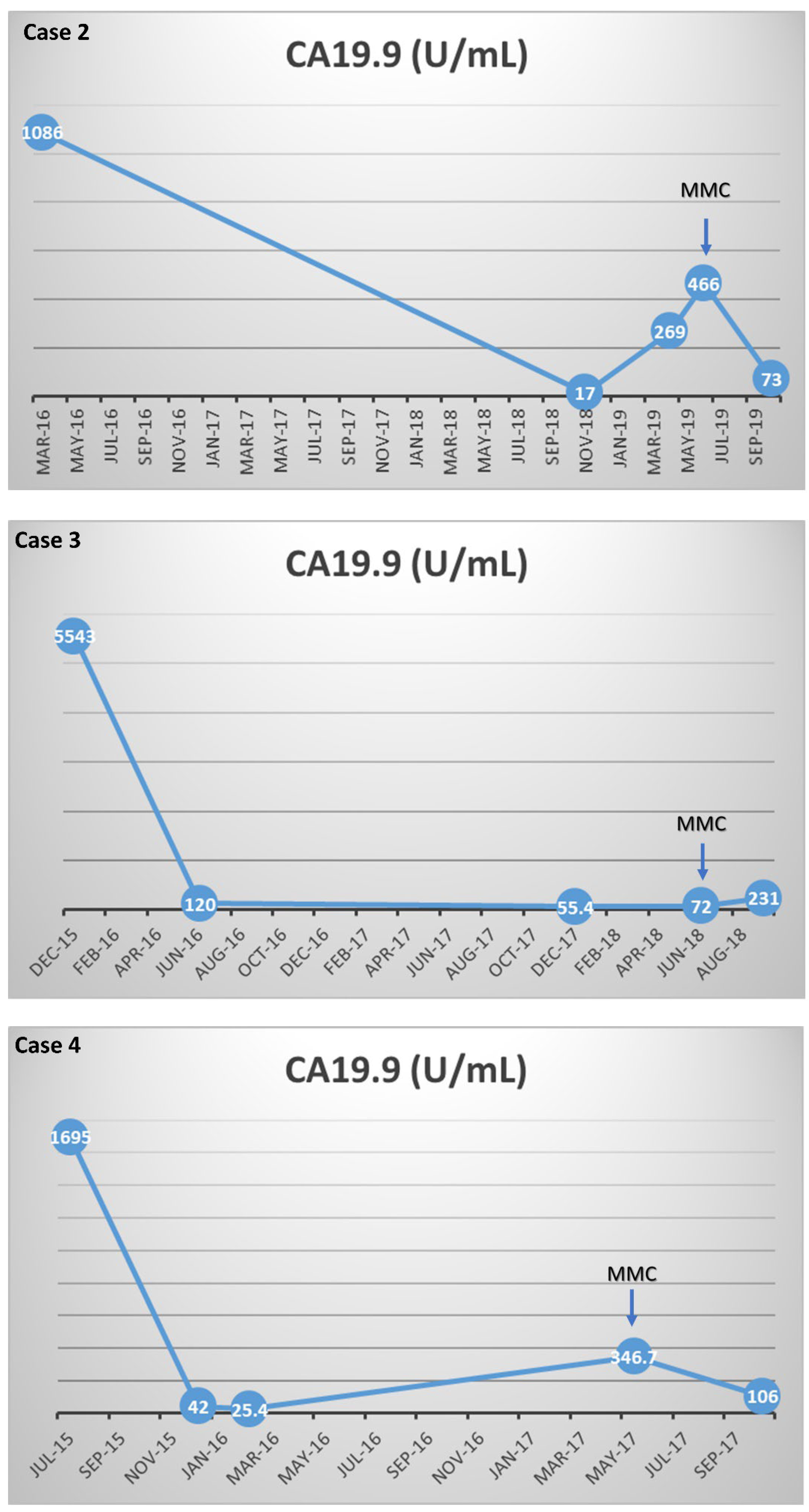
3.2.2. Case (2)
3.2.3. Case (3)
3.2.4. Case (4)
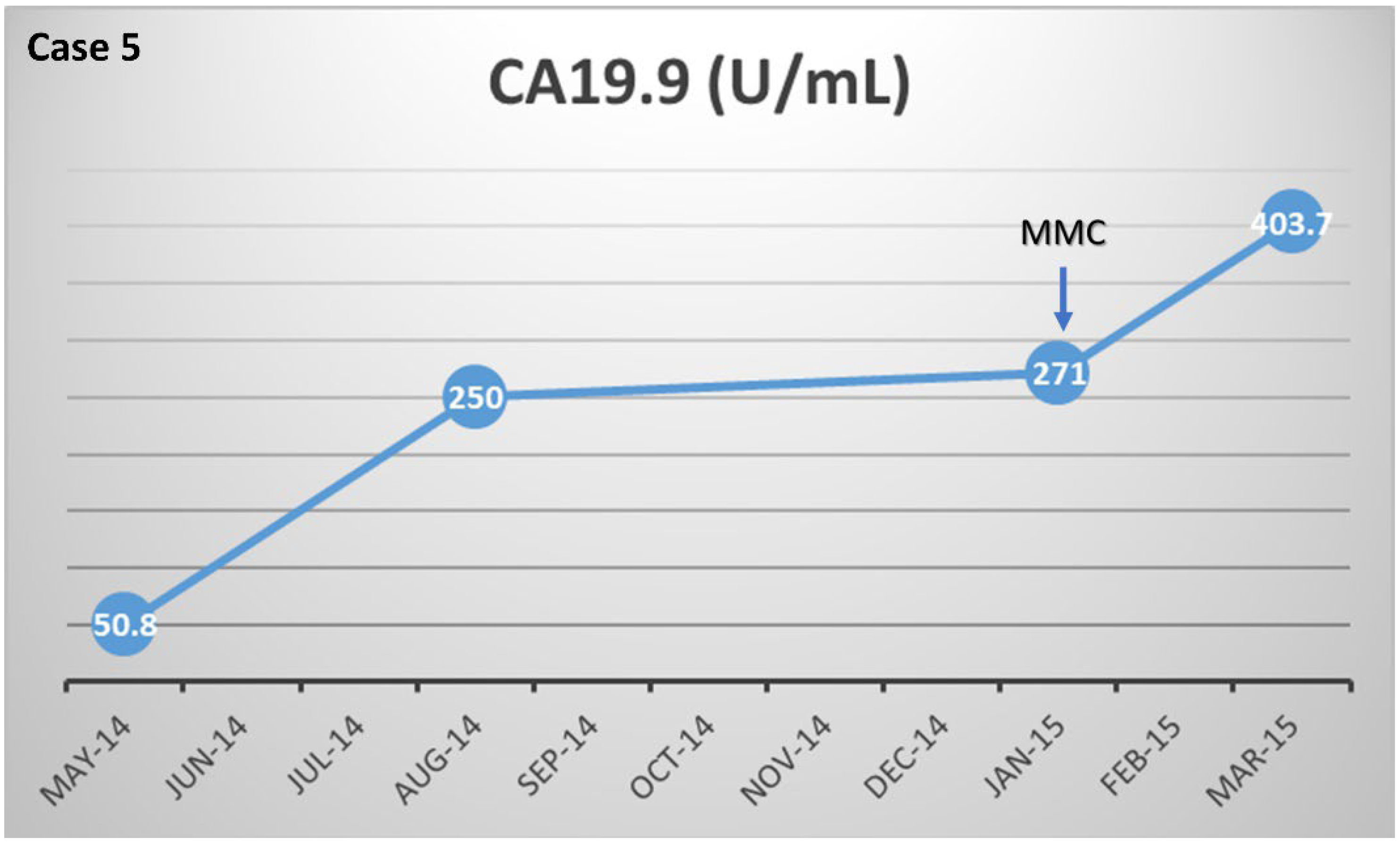
3.2.5. Case (5)
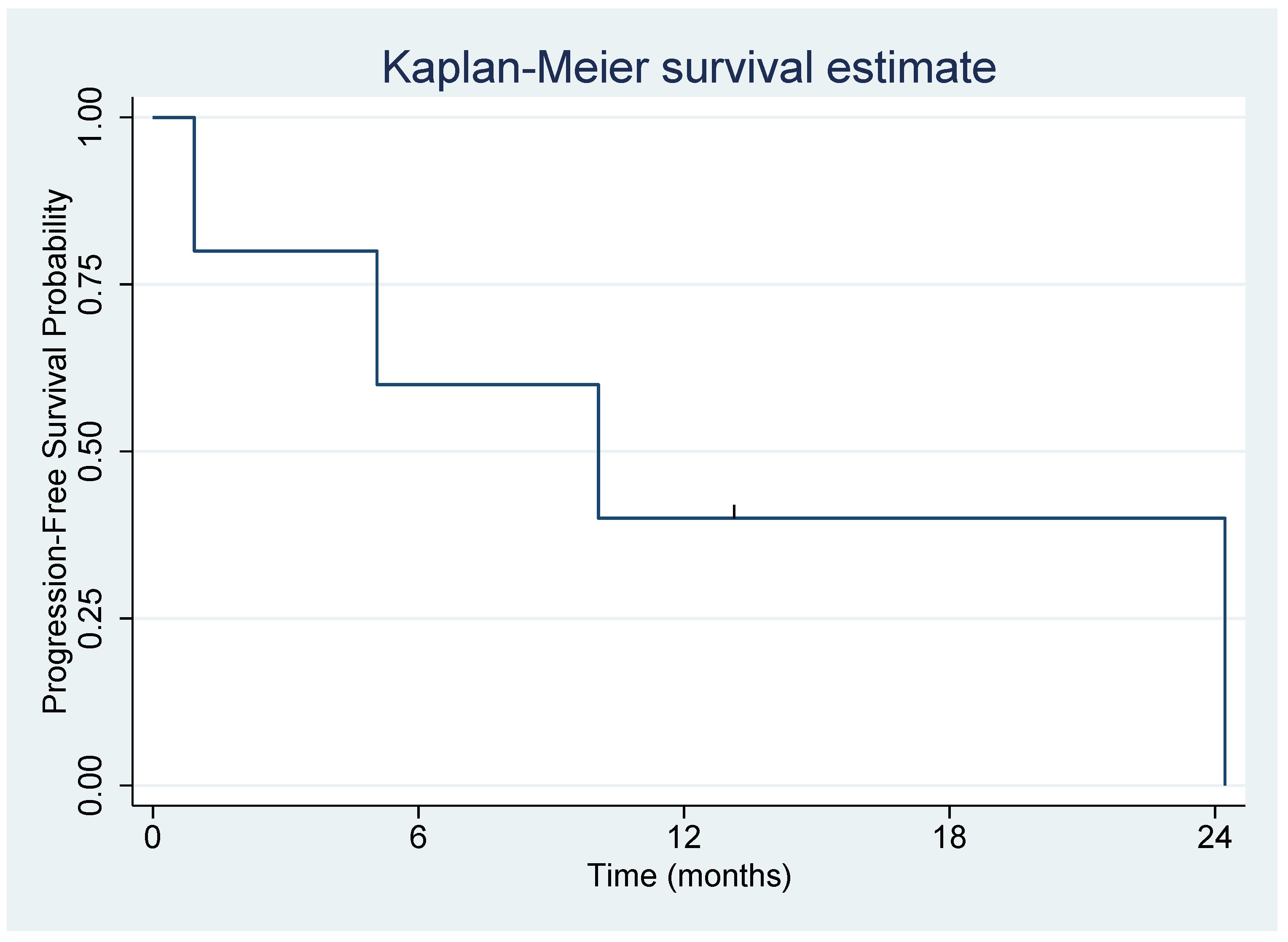
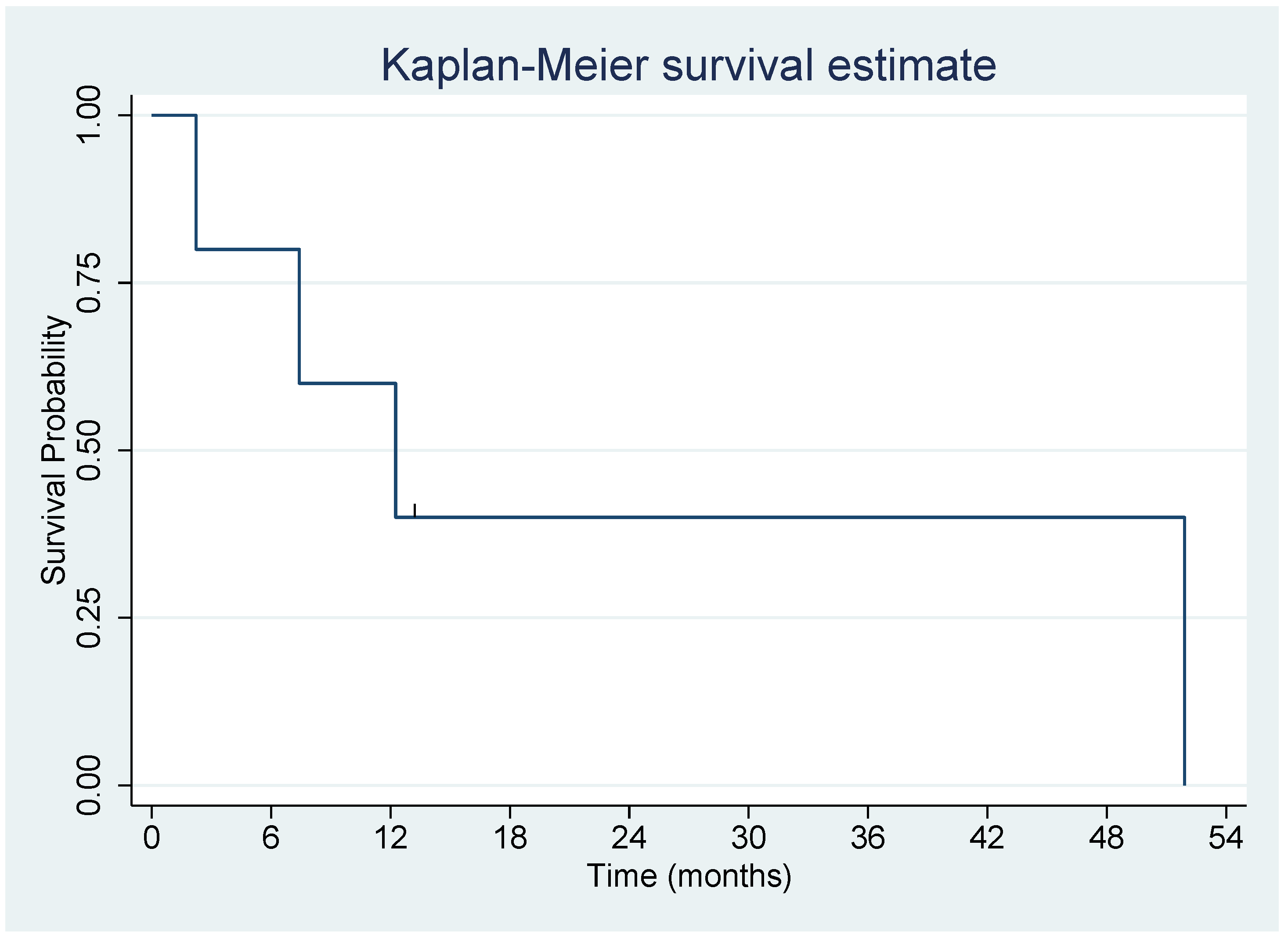
3.3. Outcomes
3.4. Safety
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Facts & Figures 2022; American Cancer Society: Atlanta, GA, USA, 2022; Available online: https://www.cancer.org/cancer/pancreatic-cancer/about/key-statistics.html (accessed on 10 October 2022).
- Sarantis, P.; Koustas, E.; Papadimitropoulou, A.; Papavassiliou, A.G.; Karamouzis, M.V. Pancreatic ductal adenocarcinoma: Treatment hurdles, tumor microenvironment and immunotherapy. World J. Gastrointest. Oncol. 2020, 12, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Singhi, A.D.; Koay, E.J.; Chari, S.T.; Maitra, A. Early Detection of Pancreatic Cancer: Opportunities and Challenges. Gastroenterology 2019, 156, 2024–2040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER Research Data, 8 Registries, Nov 2021 Sub (1975–2019)—Linked To County Attributes—Time Dependent (1990–2019) Income/Rurality, 1969–2020 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, Released April 2022, Based on the November 2021 Submission. Available online: www.seer.cancer.gov (accessed on 10 October 2022).
- Klein, A.P. Genetic susceptibility to pancreatic cancer. Mol. Carcinog. 2011, 51, 14–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dréan, A.; Lord, C.J.; Ashworth, A. PARP inhibitor combination therapy. Crit. Rev. Oncol. 2016, 108, 73–85. [Google Scholar] [CrossRef]
- Ren, N.; Zhang, L.; Yu, J.; Guan, S.; Dai, X.; Sun, L.; Ying, M. Efficacy and Safety of PARP Inhibitor Combination Therapy in Recurrent Ovarian Cancer: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 638295. [Google Scholar] [CrossRef]
- Patel, K.J.; Yu, V.P.; Lee, H.; Corcoran, A.; Thistlethwaite, F.C.; Evans, M.J.; Colledge, W.H.; Friedman, L.S.; Ponder, B.A.; Venkitaraman, A.R. Involvement of Brca2 in DNA Repair. Mol. Cell 1998, 1, 347–357. [Google Scholar] [CrossRef]
- Kaufman, B.; Shapira-Frommer, R.; Schmutzler, R.K.; Audeh, M.W.; Friedlander, M.; Balmaña, J.; Mitchell, G.; Fried, G.; Stemmer, S.M.; Hubert, A.; et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J. Clin. Oncol. 2015, 33, 244. [Google Scholar] [CrossRef]
- FDA Approves Olaparib for gBRCAm Metastatic Pancreatic Adenocarcinoma. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-olaparib-gbrcam-metastatic-pancreatic-adenocarcinoma (accessed on 20 May 2022).
- Jones, S.; Hruban, R.H.; Kamiyama, M.; Borges, M.; Zhang, X.; Parsons, D.W.; Lin, J.C.-H.; Palmisano, E.; Brune, K.; Jaffee, E.M.; et al. Exomic Sequencing Identifies PALB2 as a Pancreatic Cancer Susceptibility Gene. Science 2009, 324, 217. [Google Scholar] [CrossRef] [Green Version]
- Villarroel, M.C.; Rajeshkumar, N.; Garrido-Laguna, I.; De Jesus-Acosta, A.; Jones, S.; Maitra, A.; Hruban, R.H.; Eshleman, J.R.; Klein, A.; Laheru, D.; et al. Personalizing Cancer Treatment in the Age of Global Genomic Analyses: PALB2 Gene Mutations and the Response to DNA Damaging Agents in Pancreatic Cancer. Mol. Cancer Ther. 2011, 10, 3–8. [Google Scholar] [CrossRef]
- Puccini, A.; Ponzano, M.; Dalmasso, B.; Vanni, I.; Gandini, A.; Puglisi, S.; Borea, R.; Cremante, M.; Bruno, W.; Andreotti, V.; et al. Clinical Significance of Germline Pathogenic Variants among 51 Cancer Predisposition Genes in an Unselected Cohort of Italian Pancreatic Cancer Patients. Cancers 2022, 14, 4447. [Google Scholar] [CrossRef]
- Shroff, R.T.; Hendifar, A.; McWilliams, R.R.; Geva, R.; Epelbaum, R.; Rolfe, L.; Goble, S.; Lin, K.K.; Biankin, A.V.; Giordano, H.; et al. Rucaparib Monotherapy in Patients with Pancreatic Cancer and a Known Deleterious BRCA Mutation. JCO Precis. Oncol. 2018, 2, 1–15. [Google Scholar] [CrossRef]
- Pishvaian, M.J.; Blais, E.M.; Brody, J.R.; Lyons, E.; DeArbeloa, P.; Hendifar, A.; Mikhail, S.; Chung, V.; Sahai, V.; Sohal, D.P.S.; et al. Overall survival in patients with pancreatic cancer receiving matched therapies following molecular profiling: A retrospective analysis of the Know Your Tumor registry trial. Lancet Oncol. 2020, 21, 508–518. [Google Scholar] [CrossRef]
- van der Heijden, M.S.; Brody, J.R.; Dezentje, D.A.; Gallmeier, E.; Cunningham, S.C.; Swartz, M.J.; DeMarzo, A.M.; Offerhaus, G.J.A.; Isacoff, W.H.; Hruban, R.H.; et al. In vivo Therapeutic Responses Contingent on Fanconi Anemia/BRCA2 Status of the Tumor. Clin. Cancer Res. 2005, 11, 7508–7515. [Google Scholar] [CrossRef] [Green Version]
- FDA Approves First Therapy for Treatment of Low-Grade Upper Tract Urothelial Cancer. FDA; Published 15 April 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-therapy-treatment-low-grade-upper-tract-urothelial-cancer (accessed on 11 October 2022).
- Avendano, C.; Menendez, J.C. Chapter 6—Anticancer Drugs That Interact with the DNA Minor Groove. In Medicinal Chemistry of Anticancer Drugs, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2015; pp. 243–271. [Google Scholar]
- Chen, X.; Peng, F.; Ji, Y.; Xiang, H.; Wang, X.; Liu, T.; Wang, H.; Han, Y.; Wang, C.; Zhang, Y.; et al. Brca2 deficiency drives gastrointestinal tumor formation and is selectively inhibited by mitomycin C. Cell Death Dis. 2020, 11, 812. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 21 May 2022).
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef]
- O’Reilly, E.M.; Lee, J.W.; Zalupski, M.; Capanu, M.; Park, J.; Golan, T.; Tahover, E.; Lowery, M.A.; Chou, J.F.; Sahai, V.; et al. Randomized, Multicenter, Phase II Trial of Gemcitabine and Cisplatin With or Without Veliparib in Patients With Pancreas Adenocarcinoma and a Germline BRCA/PALB2 Mutation. J. Clin. Oncol. 2020, 38, 1378–1388. [Google Scholar] [CrossRef]
- Helleday, T. Homologous recombination in cancer development, treatment and development of drug resistance. Carcinogenesis 2010, 31, 955–960. [Google Scholar] [CrossRef] [Green Version]
- Uson, P.L.S., Jr.; Samadder, N.J.; Riegert-Johnson, D.; Boardman, L.; Borad, M.J.; Ahn, D.; Sonbol, M.B.; Faigel, D.O.; Fukami, N.; Pannala, R.; et al. Clinical impact of pathogenic germline variants in pancreatic cancer: Results from a multicenter, prospective, universal genetic testing study. Clin. Transl. Gastroenterol. 2021, 12, e00414. [Google Scholar] [CrossRef]
- Lowery, M.; Wong, W.; Jordan, E.J.; Lee, J.W.; Kemel, Y.; Vijai, J.; Mandelker, D.; Zehir, A.; Capanu, M.; Salo-Mullen, E.; et al. Prospective Evaluation of Germline Alterations in Patients With Exocrine Pancreatic Neoplasms. J. Natl. Cancer Inst. 2018, 110, 1067–1074. [Google Scholar] [CrossRef]
- Paz, M.M.; Zhang, X.; Lu, J.; Holmgren, A. A New Mechanism of Action for the Anticancer Drug Mitomycin C: Mechanism-Based Inhibition of Thioredoxin Reductase. Chem. Res. Toxicol. 2012, 25, 1502–1511. [Google Scholar] [CrossRef] [PubMed]
- El-Ghobashy, S.; El-Leithy, T.R.; Roshdy, M.M.; El-Ganzoury, H.M. Effectiveness of a single immediate mitomycin C instillation in patients with low risk superficial bladder cancer: Short and long-term follow-up. J. Egypt. Natl. Cancer Inst. 2007, 19, 121–126. [Google Scholar]
- Godfrey, T.E. Mitomycin C in advanced breast cancer: An update. Semin. Oncol. 1988, 15 (Suppl. S4), 71–73. [Google Scholar] [PubMed]
- Spasic, J.; Stanic, N.; Djordjevic, F.; Ristic, M.; Nikolić, V.; Radosavljevic, D. Mitomycin-c (mtc) as salvage therapy for patients with metastatic colorectal cancer (mCRC). Ann. Oncol. 2017, 28, iii114–iii115. [Google Scholar] [CrossRef] [Green Version]
- Moiseyenko, V.; Chubenko, V.A.; Moiseyenko, F.V.; Zhabina, A.S.; Gorodnova, T.V.; Komarov, Y.I.; Bogdanov, A.A.; Sokolenko, A.; Imyanitov, E.N. Evidence for clinical efficacy of mitomycin C in heavily pretreated ovarian cancer patients carrying germ-line BRCA1 mutation. Med. Oncol. 2014, 31, 199. [Google Scholar] [CrossRef]
- Tanabe, M. Combination chemotherapy of mitomycin C and methotrexate was effective on metastatic breast cancer resistant to eribulin, vinorelbine, and bevacizumab after anthracycline, taxane, and capecitabine. Case Rep. Oncol. 2016, 9, 422–426. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, S.; Kraft, D.; Staib-Sebler, E.; Schwarz, W.; Gog, C.; Vogl, T.; Lorenz, M. Phase II study on combined intravenous and intra-arterial chemotherapy with gemcitabine and mitomycin C in patients with advanced pancreatic cancer. Hepatogastroenterology 2013, 60, 1492–1496. [Google Scholar] [CrossRef]
- Yarchoan, M.; Myzak, M.C.; Johnson, B.A.; De Jesus-Acosta, A.; Le, D.T.; Jaffee, E.M.; Azad, N.S.; Donehower, R.C.; Zheng, L.; Oberstein, P.E.; et al. Olaparib in combination with irinotecan, cisplatin, and mitomycin C in patients with advanced pancreatic cancer. Oncotarget 2017, 8, 44073–44081. [Google Scholar] [CrossRef]
- Lee, S.; Oh, S.Y.; Kim, B.G.; Kwon, H.-C.; Kim, S.-H.; Rho, M.H.; Kim, Y.-H.; Rho, M.-S.; Jeong, J.-S.; Kim, H.-J. Second-Line Treatment With a Combination of Continuous 5-Fluorouracil, Doxorubicin, and Mitomycin-C (Conti-Fam) in Gemcitabine-Pretreated Pancreatic and Biliary Tract Cancer. Am. J. Clin. Oncol. 2009, 32, 348–352. [Google Scholar] [CrossRef]
- Ge, L.; Pan, B.; Song, F.; Ma, J.; Zeraatkar, D.; Zhou, J.; Tian, J. Comparing the diagnostic accuracy of five common tumour biomarkers and CA19-9 for pancreatic cancer: A protocol for a network meta-analysis of diagnostic test accuracy. BMJ Open 2017, 7, e018175. [Google Scholar] [CrossRef] [Green Version]
- Van Manen, L.; Groen, J.V.; Putter, H.; Vahrmeijer, A.L.; Swijnenburg, R.-J.; Bonsing, B.A.; Mieog, J.S.D. Elevated CEA and CA19-9 serum levels independently predict advanced pancreatic cancer at diagnosis. Biomarkers 2020, 25, 186–193. [Google Scholar] [CrossRef]
- Chen, L.-T.; Macarulla, T.; Blanc, J.-F.; Mirakhur, B.; de Jong, F.A.; Belanger, B.; Bekaii-Saab, T.; Siveke, J.T. Nomogram for Predicting Survival in Patients Treated with Liposomal Irinotecan Plus Fluorouracil and Leucovorin in Metastatic Pancreatic Cancer. Cancers 2019, 11, 1068. [Google Scholar] [CrossRef] [Green Version]
- Chiorean, E.G.; Von Hoff, D.D.; Reni, M.; Arena, F.P.; Infante, J.R.; Bathini, V.G.; Wood, T.E.; Mainwaring, P.N.; Muldoon, R.T.; Clingan, P.R.; et al. CA19-9 decrease at 8 weeks as a predictor of overall survival in a randomized phase III trial (MPACT) of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone in patients with metastatic pancreatic cancer. Ann. Oncol. 2016, 27, 654–660. [Google Scholar] [CrossRef]
- Wang-Gillam, A.; Hubner, R.A.; Siveke, J.T.; Von Hoff, D.D.; Belanger, B.; de Jong, F.A.; Mirakhur, B.; Chen, L.-T. NAPOLI-1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: Final overall survival analysis and characteristics of long-term survivors. Eur. J. Cancer 2019, 108, 78–87. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pancreatic Cancer (5 Patients) | ||
|---|---|---|
| Patient characteristics | No. | % |
| Age at diagnosis (years): | ||
| Median ± SD | 58.3 ± 16.5 | |
| Range | 30–70 | |
| Sex: | ||
| Female | 3 | 60 |
| Male | 2 | 40 |
| Site(s) of Metastatic Disease: | ||
| Liver | 4 | 80 |
| Lung/Bone | 1 | 20 |
| No. of prior regimens for advanced disease prior to Mitomycin C therapy: | ||
| Mean | 3.2 | |
| SD | 1.6 | |
| Personal history of prior malignancy: | ||
| Any malignancy | 2 | 40 |
| DNA repair-associated malignancy | 1 | 20 |
| Family history of malignancy: | ||
| Any malignancy | 4 | 80 |
| DNA repair-associated malignancy | 4 | 80 |
| Abbreviations: SD, standard deviation | ||
| Patient # | Age of PC Diagnosis | Sex | Germline Mutation (s) | Somatic Mutation (s) | Personal Hx of Another Cancer | FPC | HBOC | Lynch |
|---|---|---|---|---|---|---|---|---|
| 1 | 69 | F | BRCA2 c.3103G > T; p.E1035 | BRCA2 E1035, CDKN2A/2B deletion, KRAS Q61R, TP 53 S166, Low TMB 4, MSS | No | N | Y | N |
| 2 | 61 | F | BRCA2 | MSS, ATM L1675, BRCA2 Y3092fs 11, KRAS G12D, CDKN2A/B, MTAP loss exon 2-8, SMAD4 Q250 | Breast | N | Y | N |
| 3 | 70 | M | BRCA2 c.3362C > G (pathogenic); BRCA2 c.2892A > T (VUS); MSH6 (c.-16C > A; POLD1 c.46A > G | BRCA2 (pathogenic); BRCA2 exon 11 p.K964N (VUS); MGMT pos, ARID1A pathogenic; KRAS mutated; ERCC1 pos; TOPO1 pos; TUBB3 pos | Lung | N | Y | N |
| 4 | 58 | F | BRCA2, c.5946delT(p.Ser1982Argfs 22 | Not tested | No | N | Y | N |
| 5 | 30 | M | PALB2 c.1675_1676delinsTG (p.Gln559) (pathogenic); ATM c.2494C > T (p.Arg932Cys) (VUS); MLH1 c.1050A > G (silent) (VUS); CDK4 c.522 + 8G > A (intronic) (VUS); BRCA1 c.5411T > A (p.Val1804Asp) (VUS) | ATM (P604S), TP53 (W146X) (Pathogenic), BRCA1 mutation (V1804D) (VUS), low RRM1, PGP, TLE3, TUBB3, TOP2A | No | N | N | N |
| Patient | Response | CA 19.9 Change (%) | PFS (Months) | OS (Months) |
|---|---|---|---|---|
| 1 | PR | ↓ 68 | 24 | 51 |
| 2 | SD | ↓ 84 | 10 | 12 |
| 3 | PR | ↑ 220 | 13 # | 13 # |
| 4 | SD | ↓ 69 | 5 | 7 |
| 5 | PD | ↑ 49 | 1 | 2 |
| Patient | Nausea/Vomiting | Hematologic | Diarrhea |
|---|---|---|---|
| 1 | G2 | Thrombocytopenia G2 Anemia G2 | * G4 |
| 2 | G2 | Thrombocytopenia G3 Anemia G2 | G2 |
| 3 | G2 | Thrombocytopenia G2 Anemia G2 | None |
| 4 | G2 | Thrombocytopenia G1 Anemia G3 | None |
| 5 | G2 | None | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botrus, G.; Roe, D.; Jameson, G.S.; Junior, P.L.S.U.; Korn, R.L.; Caldwell, L.; Bargenquast, T.; Miller, M.; Borazanci, E.H. Mitomycin C in Homologous Recombination Deficient Metastatic Pancreatic Cancer after Disease Progression on Platinum-Based Chemotherapy and Olaparib. Biomedicines 2022, 10, 2705. https://doi.org/10.3390/biomedicines10112705
Botrus G, Roe D, Jameson GS, Junior PLSU, Korn RL, Caldwell L, Bargenquast T, Miller M, Borazanci EH. Mitomycin C in Homologous Recombination Deficient Metastatic Pancreatic Cancer after Disease Progression on Platinum-Based Chemotherapy and Olaparib. Biomedicines. 2022; 10(11):2705. https://doi.org/10.3390/biomedicines10112705
Chicago/Turabian StyleBotrus, Gehan, Denise Roe, Gayle S. Jameson, Pedro Luiz Serrano Uson Junior, Ronald Lee Korn, Lana Caldwell, Taylor Bargenquast, Max Miller, and Erkut Hasan Borazanci. 2022. "Mitomycin C in Homologous Recombination Deficient Metastatic Pancreatic Cancer after Disease Progression on Platinum-Based Chemotherapy and Olaparib" Biomedicines 10, no. 11: 2705. https://doi.org/10.3390/biomedicines10112705