1. Introduction
Three-dimensional (3D)-printed scaffolds are increasingly being used in medical bioengineering for reconstruction, tissue regeneration, and tissue repair [
1]. As a production method, 3D printing allows biomaterials to be precisely controlled and easily produced, promoting attachment to surrounding tissues and organs while providing structural support [
2]. This lends importance to fields such as plastic/reconstructive surgery and neurosurgery, where 3D-printed scaffold implants can be integrated with the surrounding bone to restore defects in areas such as maxillofacial reconstruction [
3], cranioplasty [
4] and, recently, for burrhole restoration after chronic subdural hematoma (cSDH) evacuation. Increasingly, implants of polycaprolactone (PCL)—a semicrystalline linear polymer—have become a favorable option for biomedical and commercial applications [
5].
Various materials for burrhole covers have been proposed, including autologous bone grafts and dust [
6,
7], biomaterials such as porous polyethylene [
8], poly(methyl methacrylate) (PMMA) [
9], hydroxyapatite (HA) [
10,
11], mineralized collagen [
12], and titanium [
13]. These materials can potentially be toxic to cells [
14], lack appropriate structures and interconnected porosity for vascular infiltration, or have limited biodegradability, introducing concerns for potential long-term complications. Finally, current burrhole cover designs limit drain placement.
An original bioresorbable PCL burrhole cover named Osteoplug
TM was designed by a team from the National University Hospital, Singapore, along with the Department of Biomedical Engineering at the National University of Singapore in 2006 to provide a scaffold for tissue regeneration in skull defects [
15]. Developed by Osteopore International Pte Ltd., this implant was subsequently patented and has since received US Food and Drug Administration (FDA) approval for human clinical use. The PCL material of Osteoplug
TM has previously demonstrated radiological and histopathological evidence for vascular ingrowth and osseous integration of the implant into surrounding calvarial bone, owing to its interconnected porous microstructure, and leaves no foreign material remaining in the long term [
16,
17].
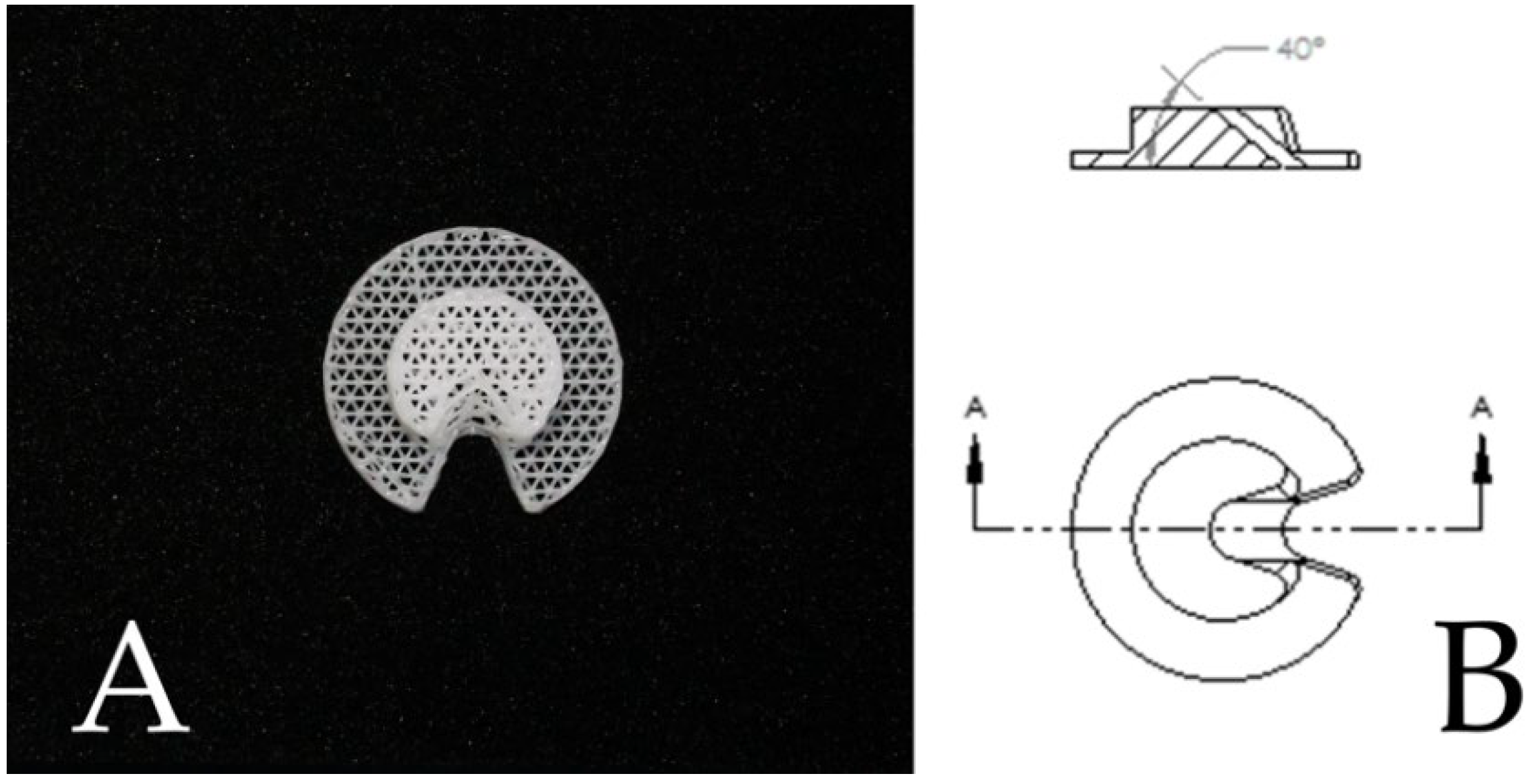
The most recent iteration of Osteoplug
TM is Osteoplug
TM-C. Introduced in 2017, it has been modified to include a chamfered hole at a 40-degree angle to allow for a drain to be easily passed through to the subdural space through its “C”-shaped opening, and its roof fits snugly into a burrhole without additional screws (
Figure 1). This redesign is useful, as drains are increasingly used for cSDH surgery to safely reduce recurrence and improve outcomes [
18]. The older versions of Osteoplug
TM have been described in our institution to have low infection rates [
17] and low cSDH recurrence rates comparable to those found in other published literature [
16]. However, no direct evaluation of the latest Osteoplug
TM-C compared to patients without burrhole covers has been performed, and no objective data on cosmetic differences have been studied. The designs of older versions of Osteoplug
TM and Osteoplug
TM-C are henceforth referred to as Design 1 and Design 2, respectively, as shown in
Table 1.
Burrhole craniostomy is a commonly used technique in neurosurgery for evacuation of cSDH. cSDH is defined as a collection of blood and blood breakdown products between the brain’s surface and the dura overlying it [
19]. Diagnosis of this condition is made via computed tomography (CT) scan. In the procedure, a hole is drilled into the skull, approximately 14 mm × 14 mm in dimensions. A burrhole cover may or may not be placed to cover the defect as part of the surgical procedure.
After burrhole craniostomy, patients experience variable degrees of wound healing, wound swelling reduction, and overlying soft tissue atrophy, resulting in postoperative scalp skin depressions [
13]. While clinical outcomes of burrhole craniostomy are generally favorable, patients may often feel embarrassed and troubled from the residual scalp depression over the uncovered burrhole [
20]. Im et al. reported that up to 64% of patients reported unacceptable cosmetic outcomes from uncovered burrhole craniostomy, resulting in functional handicaps in activities of daily living (ADLs) [
13]. A clinical photograph to demonstrate a burrhole depression is depicted in
Figure 2A, while in
Figure 2B the craniostomy has been covered with the burrhole cover (Design 2).
Despite the availability of burrhole covers, not all neurosurgeons place burrhole covers after craniotomies. A survey of neurosurgeons suggests that the reasons for this include a lack of proven benefit, technical difficulty, and fear of increased complications [
21]. Given this hesitancy and the paucity of research investigating the utility of burrhole covers in clinical practice, we sought to evaluate Design 2 in three domains: cosmesis, quality of life, and clinical safety.
2. Materials and Methods
We conducted a cross-sectional study of consecutive patients who underwent burrhole drainage of chronic subdural hematoma with and without burrhole cover placement in the National University Hospital, Singapore from 1 April 2017 to 30 March 2021. Institutional review board approval was received for this study (domain-specific review board (DSRB) (National Healthcare Group) number: 2020-01458). Written informed consent was not required for electronic medical record collection, and verbal informed consent needed for interviews was obtained by the two investigators (E.M.S.T. and A.A.T.). The inclusion criteria included all patients who had undergone burrhole drainage for cSDH, and the exclusion criteria were patients who were under 21 years of age, underwent a mini-craniotomy as the initial operation for cSDH, or received burrhole craniostomy for other neurosurgical conditions. Patients were identified retrospectively from the Operative Theatre Records System by searching for patients who had undergone burrhole drainage, and then they were screened for eligibility by the two investigators (E.M.S.T. and A.A.T.). The independent variable was the use of a burrhole cover to cover burrhole craniostomy. Other dependent variables and potential confounders—including patient characteristics such as age and gender, comorbidities, use of antiplatelet and anticoagulant drugs, and follow-up time—were also collected.
The three primary outcomes measured and collected were as follows:
- (1)
Cosmesis, as measured by Aesthetic Numeric Analog (ANA)—a patient-rated cosmetic satisfaction score.
- (2)
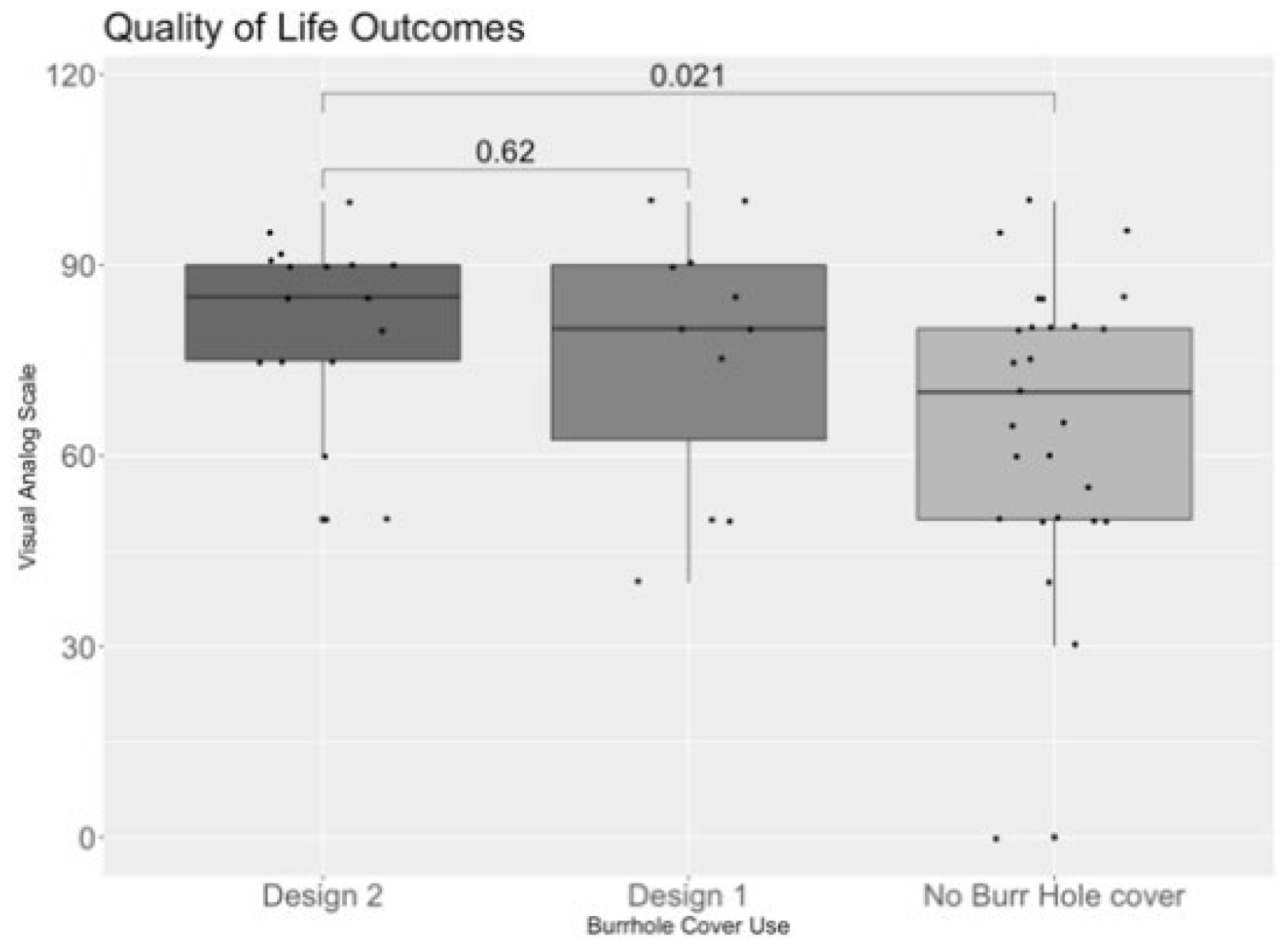
Quality of life, as measured by the EQ-5D-3L and the Visual Analog Scale (VAS).
- (3)
Safety, as measured primarily by rate of infection and cSDH recurrence. Secondary safety outcomes such as functional independence were also recorded.
2.1. Data Source and Collection
Electronic medical records from the primary institution were collected and reviewed by 2 independent investigators. The data collected included patient demographics such as age, gender, and race; comorbidities such as hypertension, hyperlipidemia, and diabetes mellitus; and current medications, such as antiplatelet or anticoagulant drugs; as well as operative procedures, postoperative course, follow-up history, complications, and relevant imaging findings, such as radiological depth of depression.
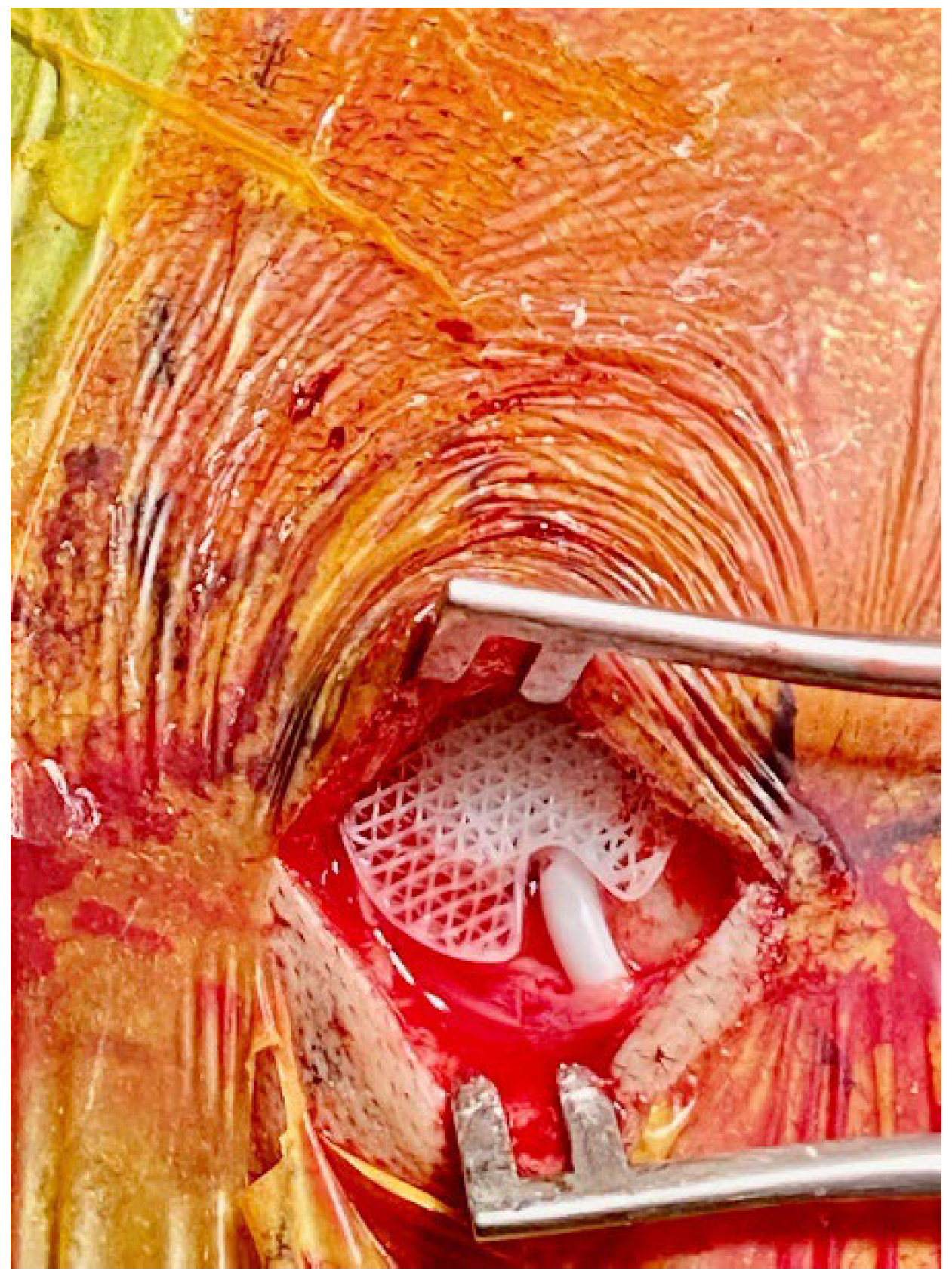
The standardized operative technique for burrhole craniostomy was practiced in the institution. The number of burrholes (either 1 or 2) was decided based on the extent of the cSDH. The subdural hematoma was then flushed with gentamicin-impregnated Hartmann solution until clear returns were achieved. A subdural or extraosseous drain was then placed into either burrhole incision. Patients who received Design 2 all had about 2–3 cm of the distal tip of the drain placed in the subdural space under direct vision. The subdural drain used was the Medtronic standard barium-impregnated ventricular catheter (Medtronic). The Design 2 implant was then fitted snugly over the drain (
Figure 3). This drain was tunneled through the skin away from the incision, anchored to the skin, and connected to a Becker
® External Drainage and Monitoring System (Medtronic). The external drainage system was positioned 20–30 cm below the external acoustic meatus to facilitate the drainage of subdural fluid. Of those who received Design 1 without Design 2, all received extraosseous drains. For those with extraosseous drains, Design 1 was first placed, before a Steril MVAC System drainage catheter, size 10 Fr (Steril Medical, Singapore), was connected to a passive drainage bottle without suction and placed at the bottom of the bed. For the remaining burrholes where a drain was not placed, they received either Design 1 or no burrhole cover. Postoperatively, patients were sent to the neurosurgical high-dependency unit and kept supine on bedrest for 24–48 h prior to being transferred to the general ward. Drains were kept in situ for 24–48 h following the operation, and a postoperative CT scan was obtained prior to drain removal.
Medical records for both hospitalization and future follow-ups were recorded for clinical outcome measures, including recurrent cSDH, postoperative wound and central nervous system infections and drain-related complications (including iatrogenic acute subdural hemorrhage), and length of hospital stay. Patients who had bilateral cSDH burrhole craniotomies had two sets of data collected—one for each side. The definition of recurrence was in accordance with the Cambridge cSDH trial—a symptomatic, ipsilateral re-accumulation of cSDH seen on radiological imaging and requiring reoperation within 6 months of the index operation [
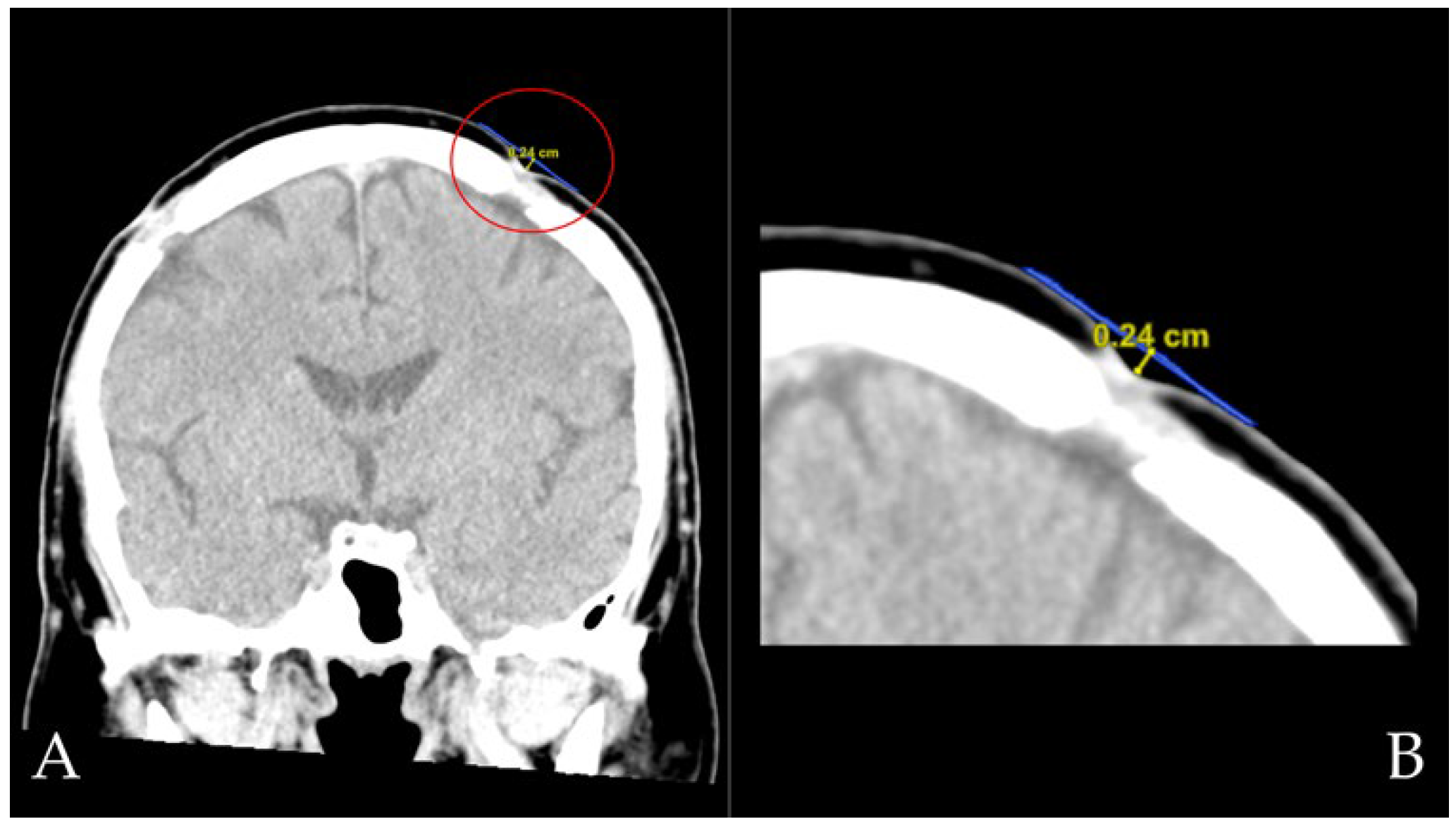
22]. Radiological scalp depression was measured per burrhole. A radiological depression was noted if a scalp depression was seen on a coronal-view CT scan at least 2 months postoperatively. The depth of scalp depressions was measured from the patient’s most recent coronal brain CT if available. An increased contrast level was used to best visualize the surrounding scalp skin, and the depth of the depression was then measured as the distance from the hypothetical scalp line (extended from the adjacent normal scalp surfaces) to the deepest point of the depression (
Figure 4).
Telephone interviews consisted of questions from the Aesthetic Numeric Analog (ANA) Scale and the EQ-5D-3L. Assessment of the patient’s mRS at the time of the interview was performed using the simplified modified Rankin Scale Questionnaire [
23]. Contact information of patients who received burrhole craniostomy was first identified from the original sample. All patients who were not labelled as deceased at the point of data collection were contacted via a letter of invitation, to which they could respond with a convenient interview timing. Patients were subsequently called by the two investigators (E.M.S.T. and A.A.T.) with a preapproved script and questionnaire. Interviews were conducted in a language suitable for the participant (English, Chinese, Malay, or Tamil), where validated translations from the EuroQol Group were used. For patients who were unable to answer the questionnaire at the point of the telephone interview, caregivers responded as proxies on the patients’ behalf, where validated proxy versions of the questionnaire were used. The EQ-5D-3L [
24] is a widely used generic measure of health status consisting of two parts: The first part is the EQ-5D descriptive system, which assesses health in five dimensions (i.e., mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each of which has three levels of responses (i.e., no problems, some problems, or extreme problems/inability). These 5 descriptive dimensions were combined into an EQ-5D summary index for each patient, calculated using the EQ-5D-3L value set validated in Singapore by the time trade-off (TTO) method. [
25] The second part of the EQ-5D questionnaire consists of a Visual Analog Scale (VAS), on which the patient rates their perceived health state from 0 (the worst imaginable health) to 100 (the best imaginable health). The ANA represents a patient’s satisfaction with the aesthetic results of the scar or depression created by burrhole craniostomy. The ANA was first used for evaluating the cosmetic outcomes of burrhole craniostomy by Vasella et al in 2018 [
20], while it was first introduced to analyze cosmetic outcomes after maxillofacial and plastic surgery by Funk et al. [
26] Patients ranked their satisfaction from 0 (not satisfied) to 10 (perfectly satisfied). This version and the appropriate translations used were approved by the DSRB and slightly modified from the original version by Funk et al, as demonstrated in
Supplementary Materials. Patients also discussed in the interview whether their scalp depressions were visible to themselves, which was referred to as visible scalp depression. Across all study groups, the same sets of standardized interview scripts and questionnaires were used to minimize interviewer bias. Non-response bias was minimized by contacting each participant via letters of invitation, repeated attempts at calling (up to three times), and allowing participants to respond in various languages or via proxy if necessary. The number of cases of cSDH during the study period determined the sample size.
2.2. Statistical Analysis
All statistical analysis was performed using R version 4.0.2 (2020-06-22). The Shapiro–Wilk test was used to test variables for normality. Statistical analysis using the Mann–Whitney U test or the Kruskal-Wallis test was performed for non-normally distributed continuous variables, while the chi-squared test was used for categorical variables. An adjusted multivariate logistic regression model was also used to identify independent associations of burrhole cover use with aesthetic outcomes, which included confounding for age, gender, EQ-5D Index, and months from follow-up. Adjusted odds ratios were calculated and presented as an adjusted odds ratio (adj OR) with a 95% confidence interval (CI). Any p-values < 0.05 were considered statistically significant. Analyses of patient demographics, clinical outcomes (i.e., infections, functional outcomes, and hospital stay), and interview outcomes were performed per patient, but analyses of cSDH recurrence and drain complications were analyzed per burrhole surgery. Analysis of radiological depth of depression was measured per burrhole. Patients who had received at least one Design 2 were analyzed in the Design 2 group. There were minimal missing data (<12%), and any missing data were removed by complete-case analysis. Sensitivity and subgroup analyses were not conducted.
4. Discussion
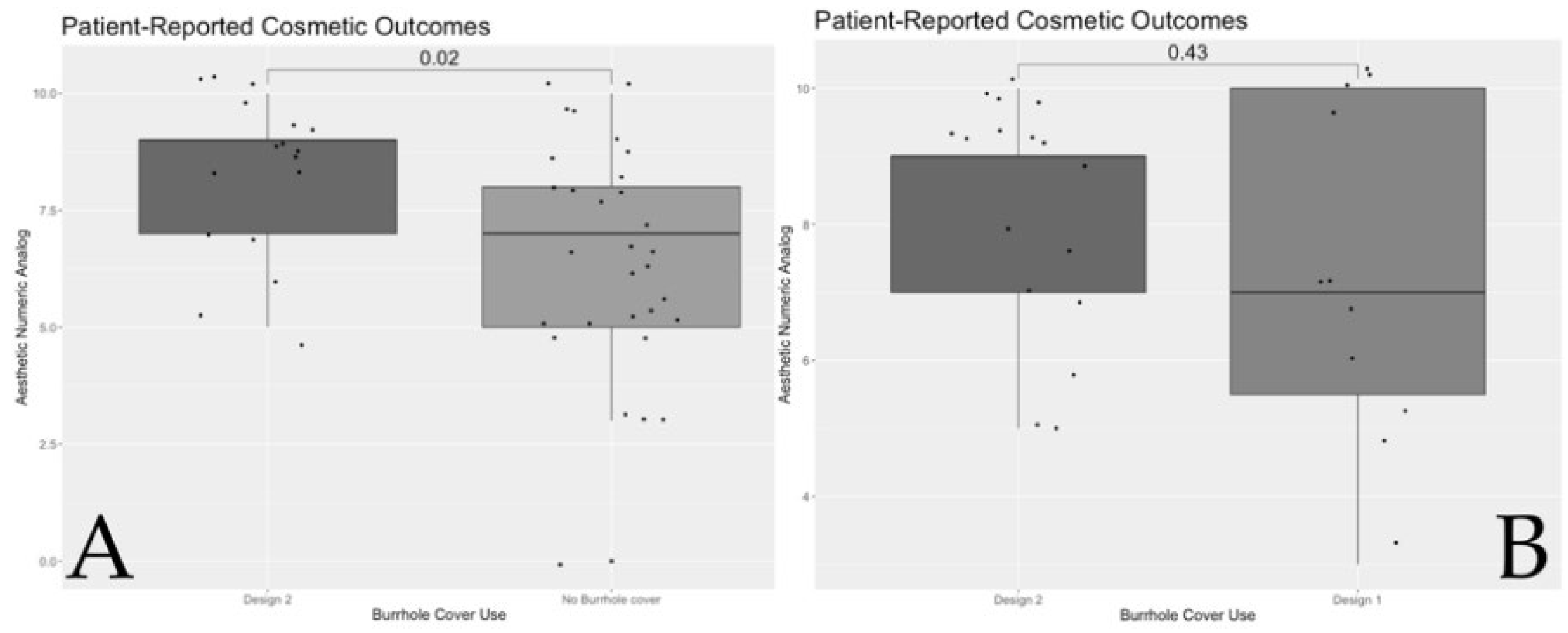
Our findings indicate that patients with Design 2 had better cosmetic outcomes and quality of life than patients with no burrhole covers, with similar cosmetic and quality of life outcomes to the previously studied Design 1. Furthermore, Design 2 had good clinical safety outcomes and no association with increased SDH recurrence, infection, or drain-related complications.
Cosmetic outcomes in neurosurgery tend to be overlooked as an outcome measure, as they are not perceived to be immediately crucial to medical outcomes [
27]. Multiple studies have investigated the cosmetic outcomes of patients after 3D reconstruction, typically for cranioplasty [
28,
29], and only two studies have analyzed the cosmetic outcomes after burrhole reconstruction with titanium burrhole covers. In other surgical disciplines, cosmetic outcomes are associated with quality of life, impaired social and emotional functioning, and depressive symptom scores [
30]. Our results are consistent with the findings of previous studies that reported significantly higher patient satisfaction in those who received burrhole covers than in those who did not [
13,
20]. This could be attributed to objective and subjective scalp depression reduction. Similarly, the quality of life interview scores of patients with Design 2 were higher than those with no burrhole cover. In general, health-related quality of life (HRQoL) has not previously been well-reported in groups who underwent burrhole craniostomy. However, notably, Im et al reported an increase in quality-of-life outcomes after titanium burrhole reconstruction [
13]. Hence, Design 2 may similarly improve quality-of-life outcomes by removing scalp depressions.
Our study also showed no significant differences in safety outcomes between the three groups. No association was observed between Design 2 use and cSDH recurrence or rates of infection and drain-related complications; this finding is comparable to our previously published studies on Design 1 [
16], as well as similar studies on titanium burrhole covers [
13,
20]. This could encourage surgeons to use burrhole covers, given that increased complications were among the top five reasons cited for not using burrhole covers [
21]. One complication was found in a Design 1 product, where the extraosseous drain became stuck to its superior surface. Despite extensive investigation by both surgeons and the manufacturers, no specific cause of this complication was identified.
Materials used for 3D-printed scaffolds must have several criteria for successful utilization, some of which include biocompatibility, biodegradability, strength and stiffness comparable to biological tissues [
31] and, crucially, porosity. Biocompatibility refers to integrating well with the host material so as not to provoke an adverse immune response [
32], while biodegradability is necessary for the scaffold to support tissue regrowth during its natural lifespan before being naturally resorbed into the body [
33]. The rate of bioresorption of the scaffold in vivo should also be controlled and well-defined specifically to the host tissue [
34]. Mechanical strength refers to the structural integrity of the scaffold to support the region at the scaffold–tissue interface and prevent collapse during daily activities, while not impeding bone formation [
35,
36]. Finally, scaffold microarchitecture and the size, distribution, and connection of pores affect patterns of bony ingrowth [
37] and vessel development [
38], and promote further tissue regrowth via cell entrapment [
36]. It has been suggested that pore sizes greater than 250 μm allow for greater vessel ingrowth than smaller pores [
39,
40]. Significantly, an interconnected porous architecture leads to excellent tissue regeneration and vascularization [
41], while pore pathways that are only partially connected inhibit cell migration [
42]. This is closely linked to osseointegration properties, describe a material’s ability to encourage immature and pluripotent stem cells to differentiate into chondrocytes and osteoblasts, allowing for vascular integration [
43]. Poor osseointegration could impair consequential bone repair and long-term implant functionality by decreasing mechanical stability [
36]. Our PCL burrhole covers prove advantageous in these respects compared to existing popular alternatives, including the titanium burrhole covers whose cosmetic outcomes were previously studied [
13,
44], or porous polyethylene [
8]. Other materials previously reported to cover burrhole defects include PMMA [
9], HA [
13], mineralized collagen [
12], and autologous bone [
6,
7]. These materials are less ideal for use as burrhole covers, for reasons such as poor cost-effectiveness, time-consuming application, or the lack of interconnected pores, which are important for tissue integration [
8,
13]. In comparison, our study on Design 2 reaffirms the benefits of using PCL, which is highly biocompatible and biodegradable, has high biomechanical strength, and has a fixed interconnected pore microarchitecture that allows integration with osseous tissue [
8,
13].
With reference to biocompatibility, while titanium is biologically inert [
45], PMMA may exhibit a toxic exothermic reaction, which could potentially be neurotoxic [
14]. Meanwhile, PCL and PCL-incorporated tricalcium phosphate (PCL/TCP) have been shown to promote cell regeneration for traumatic brain injury and do not cause inflammation, emphasizing their safety to tissues [
46,
47]. Additionally, the biodegradation properties of PCL and PCL/TCP scaffolds have shown an appropriately lengthy degradation life, according to the initial molecular weight [
48], allowing time for the replacement and healing of bone and vascular tissues over their functional lifespan before resorption [
34]. The high biodegradability of PCL implants is achieved via hydrolytic and lipase-type enzymatic degradation [
49]. This can be compared to permanent non-resorbable implants made of porous polyethylene, HA, and titanium [
36,
50], which could introduce additional concerns, including a theoretical delayed onset of infection, and some case reports of porous-polyethylene-related intense foreign body reaction have emerged [
51,
52]. Furthermore, the snap-fit design of the PCL burrhole covers does not require additional screws [
15]. Titanium screws, in contrast, could theoretically result in screw displacement or scalp injury.
PCL has shown to be used under harsh mechanical, physical, and chemical conditions without significant loss of properties [
53]. Similarly, PCL scaffolds have previously been shown to demonstrate biomechanical strength 60% that of normal bone in vivo [
54]. Recent studies on PCL have demonstrated enhanced mechanical stability [
55] in comparison to ceramic materials, which have high brittleness and high fatigue strength [
36].
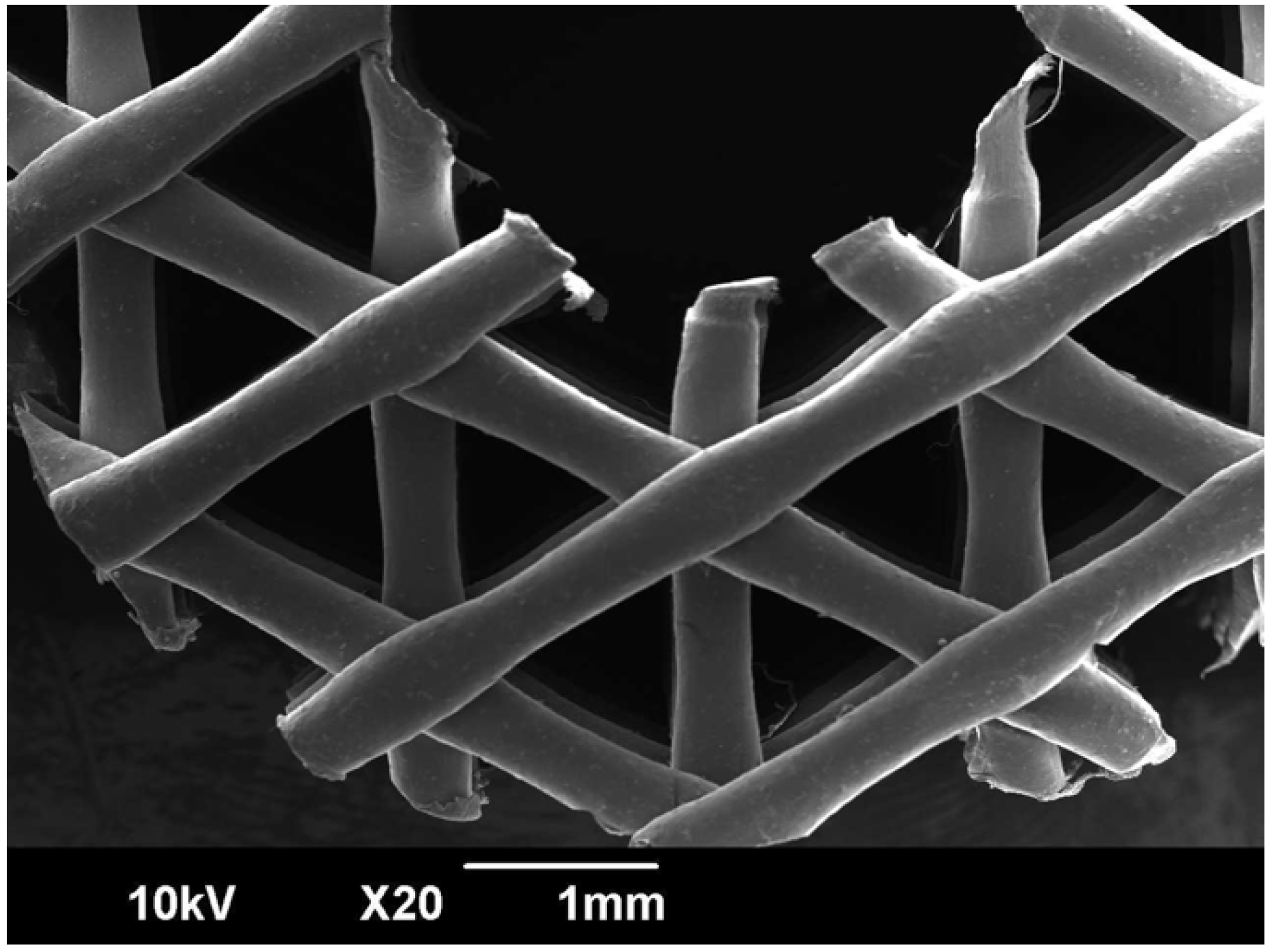
Finally, PCL has a 400–600 μm pore size with a porosity of 60%–70% [
17], as demonstrated by the scanning electron microscope image shown in
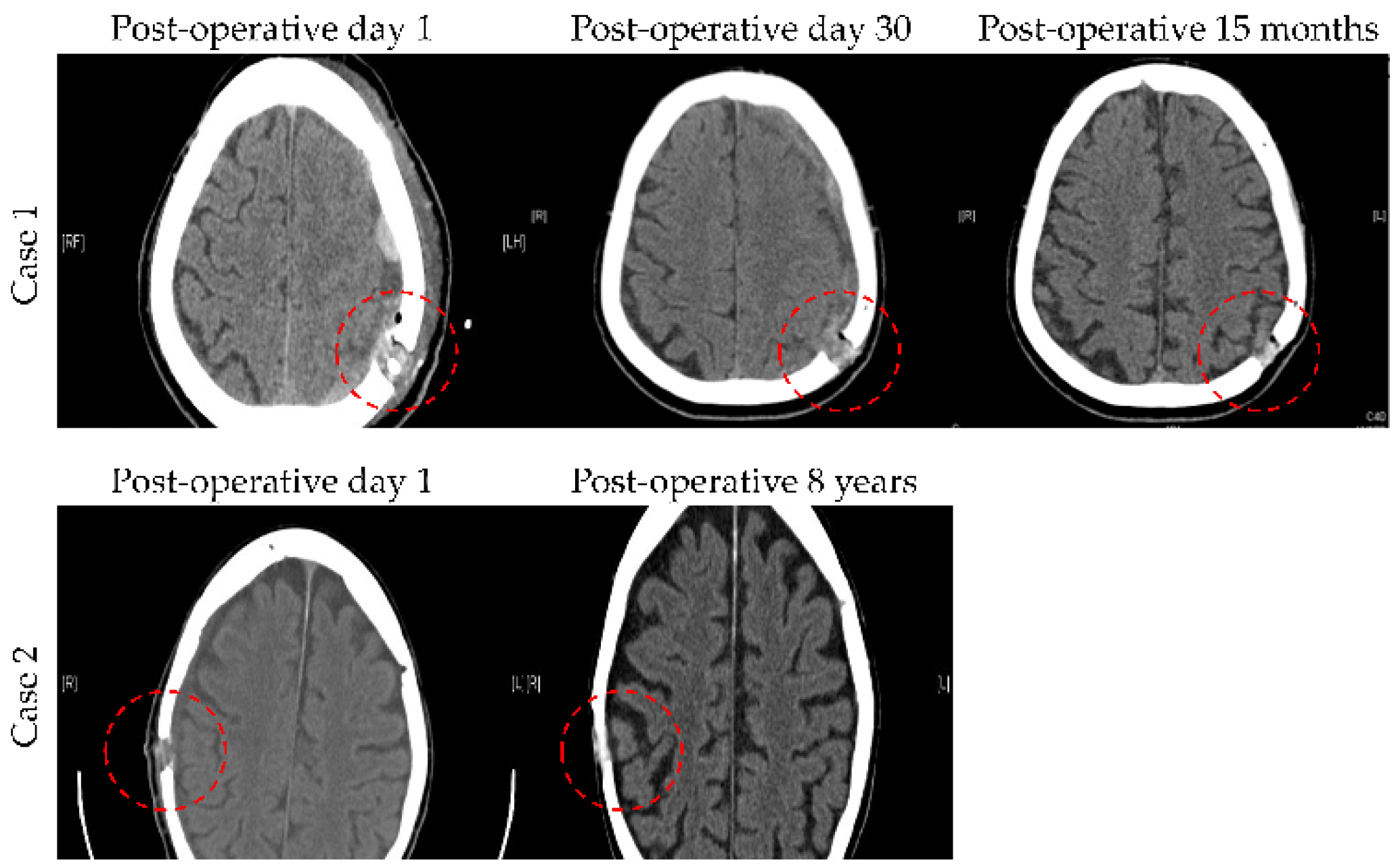
Figure 7. This structured interconnected porosity allows PCL burrhole covers to achieve bony growth over time, as shown in
Figure 8 [
16]. Together with micro-computed tomography scans and histological staining, this provides evidence to confirm significant tissue infiltration, i.e., sufficient bone growth to cover the previous burrhole defect [
16]. In comparison, titanium burrhole covers have single isolated pores, which could cause discontinuous patterns of bone ingrowth [
37].
Our results add to the scarce body of literature to demonstrate how burrhole covers are safe and suitable for use in patients following evacuation of cSDH, achieving good cosmetic outcomes. As a pilot, this study also sets the stage for further research into the potential for the use of both PCL and Osteoplug
TM-C (Design 2) on a larger scale. The limitations of our study include the retrospective nature of the electronic medical record collection, where potential confounders may not have been collected and adjusted for. Another limitation was the relatively low response rate among the participants approached for interview. The reasons stated for non-response mainly included time limitations, participants having moved to a nursing home, or communication difficulties. There were also several participants who were uncontactable. Patients may also not have been technologically adept or may have been wary of scam calls, which were prevalent over the interview period. However, our response rate was comparable to those of other studies analyzing quality-of-life data in Singapore [
25]. Patients were not able to be interviewed at the same timepoint postoperatively, although this was accounted for in the multivariate analysis. Some patients underwent revision operations or were lost to follow-up, so postoperative radiological depth of burrhole depressions was unable to be measured. The Aesthetic Numeric Analog was also not a scale that had been officially validated in a Singaporean cohort in different languages, which could have limited the interpretability of the patient-reported outcomes.
As this was a pilot study with a relatively small cohort, further research with a larger population will be crucial for confirming the clinical and cosmetic outcomes of Design 2. Future work could also involve interviewing surgeons as to their preference and the ease of use of Design 1 to ascertain whether Design 2 is the preferred burrhole cover version among surgeons.

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


