
Retinal Microvascular Abnormalities and Systemic Arterial Stiffness Are the First Manifestation of Cardiovascular Abnormalities in Patients with Untreated Moderate to Severe Obstructive Sleep Apnoea and with Low to Intermediate Cardiovascular Risk—A Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Polysomnography
2.3. Sleep Questionnaires
2.3.1. General Health and Quality of Life Questionnaire: Short Form-36 (SF-36®)
2.3.2. Functional Outcomes of Sleep Questionnaire (FOSQ)
2.4. General Investigations
2.5. Blood and Urine Analyses
2.6. Measurement of Glutathione Redox Index
2.7. Measurement of Nitric Oxide
2.8. Macro- and Microvascular Assessments
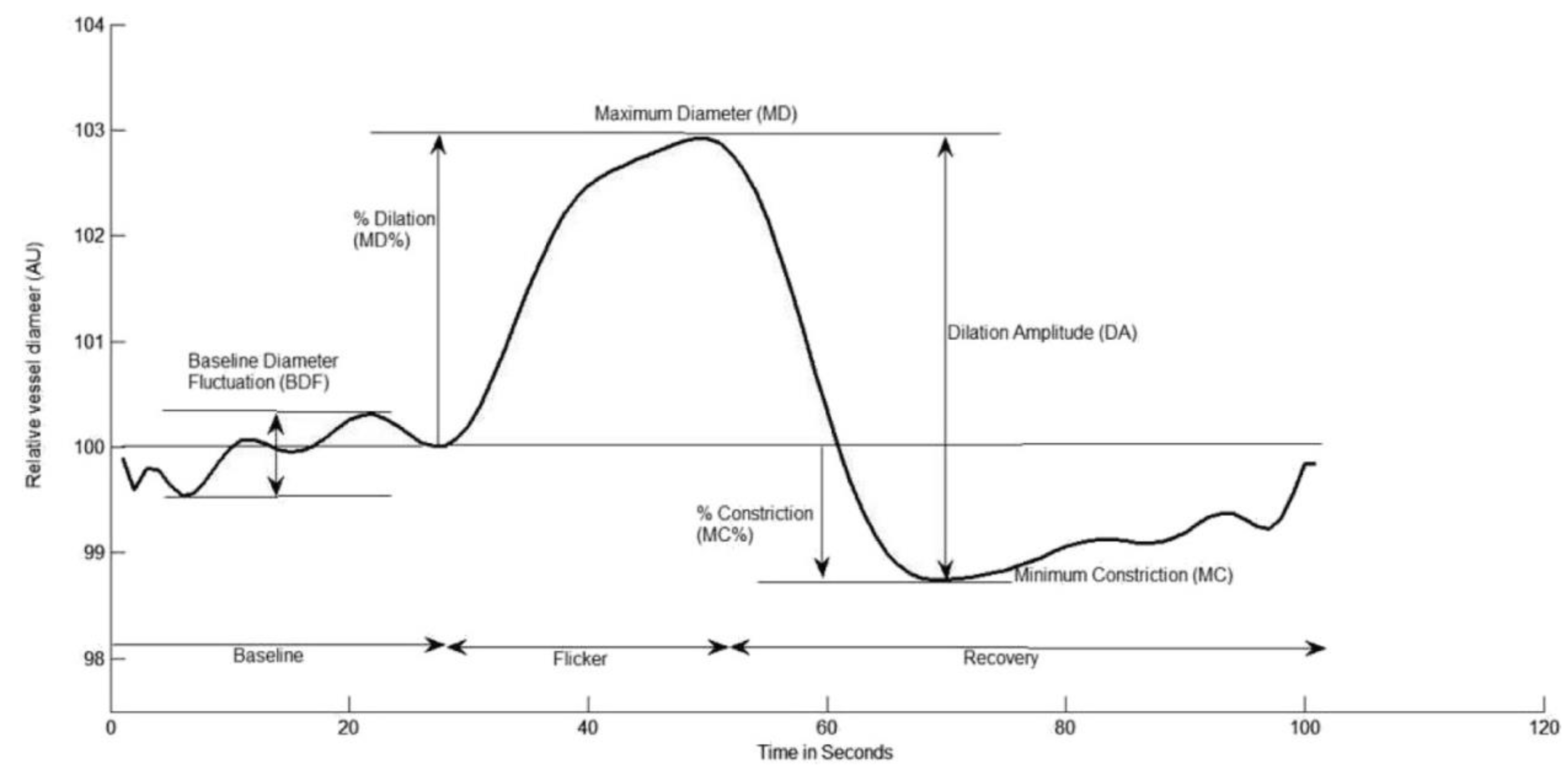
2.8.1. Dynamic Retinal Microvascular Function Vessel Analysis
2.8.2. Pulse Wave Analysis (PWA)
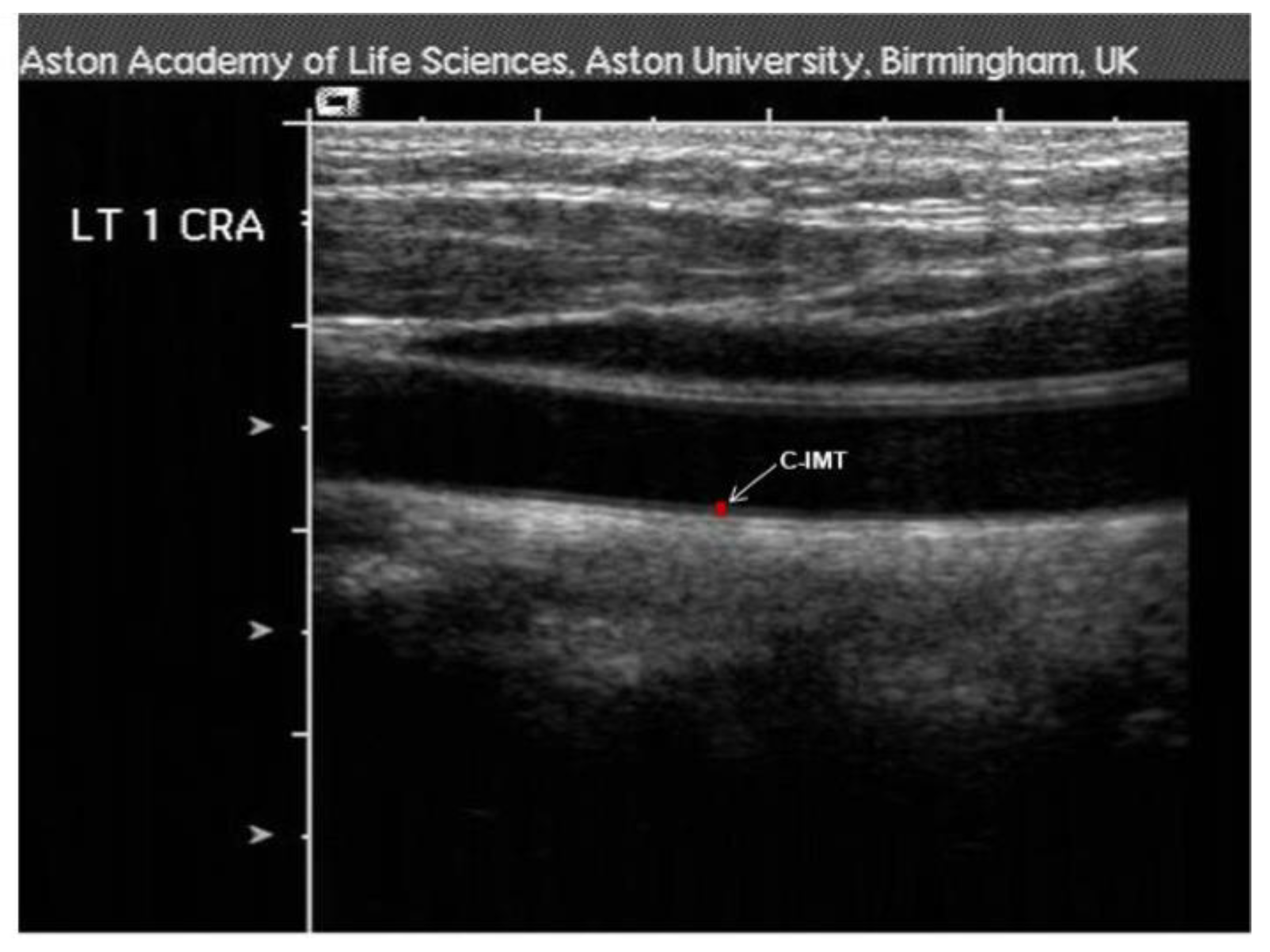
2.8.3. Carotid-Intima-Media Thickness (c-IMT)
2.8.4. Flow-Mediated Dilation
2.9. Statistical Analysis
Sample Size Calculation
3. Results
3.1. General and Respiratory Measurements
3.2. Retinal Vascular Function
3.3. Correlation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Drager, L.F.; McEvoy, R.D.; Barbe, F.; Lorenzi-Filho, G.; Redline, S. Sleep Apnea and Cardiovascular Disease: Lessons from Recent Trials and Need for Team Science. Circulation 2017, 136, 1840–1850. [Google Scholar] [CrossRef]
- Garvey, J.F.; Taylor, C.T.; McNicholas, W.T. Cardiovascular Disease in Obstructive Sleep Apnoea Syndrome: The Role of Intermittent Hypoxia and Inflammation. Eur. Respir. J. 2009, 33, 1195–1205. [Google Scholar] [CrossRef] [Green Version]
- Maeder, M.T.; Mueller, C.; Schoch, O.D.; Ammann, P.; Rickli, H. Biomarkers of Cardiovascular Stress in Obstructive Sleep Apnea. Clin. Chim. Acta 2016, 460, 152–163. [Google Scholar] [CrossRef]
- Heitmar, R.; Cubbidge, R.P.; Lip, G.Y.H.; Gherghel, D.; Blann, A.D. Altered Blood Vessel Responses in the Eye and Finger in Coronary Artery Disease. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6199–6205. [Google Scholar] [CrossRef] [Green Version]
- Vita, J.A.; Keaney, J.F. Endothelial Function. Circulation 2002, 106, 640–642. [Google Scholar] [CrossRef] [Green Version]
- Seshadri, S.; Karimzad, S.E.; Shokr, H.; Gherghel, D. Retinal Vascular Function in Asymptomatic Individuals with a Positive Family History of Cardiovascular Disease. Acta Ophthalmol. 2018, 96, e956–e962. [Google Scholar] [CrossRef] [Green Version]
- Shokr, H.; Dias, I.H.K.; Gherghel, D. Oxysterols and Retinal Microvascular Dysfunction as Early Risk Markers for Cardiovascular Disease in Normal, Ageing Individuals. Antioxidants 2021, 10, 1756. [Google Scholar] [CrossRef]
- Shokr, H.; Wolffsohn, J.S.; Trave Huarte, S.; Scarpello, E.; Gherghel, D.; Ophthalmol, A. Dry Eye Disease Is Associated with Retinal Microvascular Dysfunction and Possible Risk for Cardiovascular Disease. Acta Ophthalmol. 2021, 99, e1236–e1242. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Gandek, B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Wells, R.D.; Freedland, K.E.; Carney, R.M.; Duntley, S.P.; Stepanski, E.J. Adherence, Reports of Benefits, and Depression among Patients Treated with Continuous Positive Airway Pressure. Psychosom. Med. 2007, 69, 449–454. [Google Scholar] [CrossRef]
- Gooneratne, N.S.; Weaver, T.E.; Cater, J.R.; Pack, F.M.; Arner, H.M.; Greenberg, A.S.; Pack, A.I. Functional Outcomes of Excessive Daytime Sleepiness in Older Adults. J. Am. Geriatr. Soc. 2003, 51, 642–649. [Google Scholar] [CrossRef]
- Karimzad, S.E.; Shokr, H.; Gherghel, D. Retinal and Peripheral Vascular Function in Healthy Individuals with Low Cardiovascular Risk. Microvasc. Res. 2019, 126, 103908. [Google Scholar] [CrossRef]
- Shokr, H.; Gherghel, D. European Society of Cardiology/European Society of Hypertension versus the American College of Cardiology/American Heart Association Guidelines on the Cut-off Values for Early Hypertension: A Microvascular Perspective. Sci. Rep. 2021, 11, 3473. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Wilson, P.W.F.; Castelli, W.P.; Kannel, W.B. Coronary Risk Prediction in Adults (The Framingham Heart Study). Am. J. Cardiol. 1987, 59, 91–94. [Google Scholar] [CrossRef]
- Ford, E.S.; Giles, W.H.; Mokdad, A.H. The Distribution of 10-Year Risk for Coronary Heart Disease among U.S. Adults: Findings from the National Health and Nutrition Examination Survey III. J. Am. Coll. Cardiol. 2004, 49, 1791–1796. [Google Scholar] [CrossRef] [Green Version]
- Gherghel, D.; Mroczkowska, S.; Qin, L. Reduction in Blood Glutathione Levels Occurs Similarly in Patients with Primary-Open Angle or Normal Tension Glaucoma. Investig. Ophthalmol. Vis. Sci. 2013, 54, 3333–3339. [Google Scholar] [CrossRef]
- Jones, D.P.; Carlson, J.L.; Samiec, P.S.; Sternberg, P.; Mody, V.C.; Reed, R.L.; Brown, L.A.S. Glutathione Measurement in Human Plasma. Evaluation of Sample Collection, Storage and Derivatization Conditions for Analysis of Dansyl Derivatives by HPLC. Clin. Chim. Acta 1998, 275, 175–184. [Google Scholar] [CrossRef]
- Tietze, F. Enzymic Method for Quantitative Determination of Nanogram Amounts of Total and Oxidized Glutathione: Applications to Mammalian Blood and other Tissues. Anal. Biochem. 1969, 27, 502–522. [Google Scholar] [CrossRef]
- Anderson, M.E. Glutathione: An Overview of Biosynthesis and Modulation. Chem.-Biol. Interact. 1998, 111–112, 1–14. [Google Scholar] [CrossRef]
- Nagel, E.; Vilser, W.; Lanzl, I. Age, Blood Pressure, and Vessel Diameter as Factors Influencing the Arterial Retinal Flicker Response. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1486–1492. [Google Scholar] [CrossRef]
- Shokr, H.; Dias, I.H.K.; Gherghel, D. Microvascular Function and Oxidative Stress in Adult Individuals with Early Onset of Cardiovascular Disease. Sci. Rep. 2020, 10, 4881. [Google Scholar] [CrossRef] [Green Version]
- O’Rourke, M.F.; Jiang, A.P.X.J. Pulse Wave Analysis. Br. J. Clin. Pharmacol. 2001, 51, 507. [Google Scholar] [CrossRef]
- Salonen, R.; Haapanen, A.; Salonen, J.T. Measurement of Intima-Media Thickness of Common Carotid Arteries with High-Resolution B-Mode Ultrasonography: Inter- and Intra-Observer Variability. Ultrasound Med. Biol. 1991, 17, 225–230. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the Ultrasound Assessment of Endothelial-Dependent Flow-Mediated Vasodilation of the Brachial Artery: A Report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Kraiczi, H.; Caidahl, K.; Samuelsson, A.; Peker, Y.; Hedner, J. Impairment of Vascular Endothelial Function and Left Ventricular Filling: Association with the Severity of Apnea-Induced Hypoxemia during Sleep. Chest 2001, 119, 1085–1091. [Google Scholar] [CrossRef] [Green Version]
- Bayram, N.A.; Ciftci, B.; Keles, T.; Durmaz, T.; Turhan, S.; Bozkurt, E.; Peker, Y. Endothelial Function in Normotensive Men with Obstructive Sleep Apnea Before and 6 Months after CPAP Treatment. Sleep 2009, 32, 1257–1263. [Google Scholar] [CrossRef] [Green Version]
- Mroczkowska, S.; Benavente-Perez, A.; Negi, A.; Sung, V.; Patel, S.R.; Gherghel, D. Primary Open-Angle Glaucoma vs. Normal-Tension Glaucoma: The Vascular Perspective. Arch. Ophthalmol. 2013, 131, 36–43. [Google Scholar] [CrossRef]
- Dyugovskaya, L.; Lavie, P.; Lavie, L. Increased Adhesion Molecules Expression and Production of Reactive Oxygen Species in Leukocytes of Sleep Apnea Patients. Am. J. Respir. Crit. Care Med. 2012, 165, 934–939. [Google Scholar] [CrossRef]
- Schulz, R.; Mahmoudi, S.; Hattar, K.; Sibelius, U.L.F.; Olschewski, H.; Mayer, K.; Seeger, W.; Grimminger, F. Enhanced Release of Superoxide from Polymorphonuclear Neutrophils in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2012, 162, 566–570. [Google Scholar] [CrossRef]
- Yokoe, T.; Minoguchi, K.; Matsuo, H.; Oda, N.; Minoguchi, H.; Yoshino, G.; Hirano, T.; Adachi, M. Elevated Levels of C-Reactive Protein and Interleukin-6 in Patients with Obstructive Sleep Apnea Syndrome Are Decreased by Nasal Continuous Positive Airway Pressure. Circulation 2003, 107, 1129–1134. [Google Scholar] [CrossRef] [Green Version]
- Ryan, S.; Taylor, C.T.; McNicholas, W.T. Selective Activation of Inflammatory Pathways by Intermittent Hypoxia in Obstructive Sleep Apnea Syndrome. Circulation 2005, 112, 2660–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokr, H.; Lush, V.; Dias, I.H.; Ekárt, A.; De Moraes, G.; Gherghel, D. The Use of Retinal Microvascular Function and Telomere Length in Age and Blood Pressure Prediction in Individuals with Low Cardiovascular Risk. Cells 2022, 11, 3037. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.; Sasongko, M.B.; Ikram, M.K.; Lamoureux, E.; Wang, J.J.; Wong, T.Y.; Cheung, C.Y. Systemic Associations of Dynamic Retinal Vessel Analysis: A Review of Current Literature. Microcirculation 2013, 20, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Liu, V.W.T.; Huang, P.L. Cardiovascular Roles of Nitric Oxide: A Review of Insights from Nitric Oxide Synthase Gene Disrupted Mice. Cardiovasc. Res. 2008, 77, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Lott, M.E.J.; Slocomb, J.E.; Shivkumar, V.; Smith, B.; Gabbay, R.A.; Quillen, D.; Gardner, T.W.; Bettermann, K. Comparison of Retinal Vasodilator and Constrictor Responses in Type 2 Diabetes. Acta Ophthalmol. 2012, 90, e434–e441. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.R.; Bellary, S.; Karimzad, S.; Gherghel, D. Overweight Status Is Associated with Extensive Signs of Microvascular Dysfunction and Cardiovascular Risk. Sci. Rep. 2016, 6, 32282. [Google Scholar] [CrossRef] [Green Version]
- Karimzad, S.; Bilkhu, P.S.; Wolffsohn, J.S.; Bellary, S.; Shokr, H.; Singhal, R.; Gherghel, D. Impact of Bariatric Surgery-Induced Weight Loss on Anterior Eye Health in Patients with Obesity. Nutrients 2022, 14, 2462. [Google Scholar] [CrossRef]
- Patel, S.R.; Bellary, S.; Qin, L.; Gill, P.S.; Taheri, S.; Heitmar, R.; Gibson, J.M.; Gherghel, D. Abnormal Retinal Vascular Function and Lipid Levels in a Sample of Healthy UK South Asians. Br. J. Ophthalmol. 2011, 95, 1573–1576. [Google Scholar] [CrossRef]
- Koller, A.; Balasko, M.; Bagi, Z. Endothelial Regulation of Coronary Microcirculation in Health and Cardiometabolic Diseases. Intern. Emerg. Med. 2013, 8, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Bagi, Z.; Broskova, Z.; Feher, A. Obesity and Coronary Microvascular Disease—Implications for Adipose Tissue-Mediated Remote Inflammatory Response. In Current Vascular Pharmacology; Bentham Science Publishers: Karachi, Pakistan, 2014; Available online: https://www.ingentaconnect.com/content/ben/cvp/2014/00000012/00000003/art00012 (accessed on 17 June 2022).




{kind=link}
{kind=link}
{kind=link}
| Mean (SD) | |||
|---|---|---|---|
| Variable | Group (1) | Group (2) | p-Value (t-Test) |
| OSA | Control | ||
| N | 14 | 14 | - |
| Gender | 10M/4W | 9M/5W | 0.987 |
| Age (years) | 59 (7) | 60 (9) | 0.890 |
| BMI (kg/m2) | 34.09 (6.50) | 28.04 (3.35) | 0.003 * |
| SBP (mmHg) | 130 (15) | 125 (15) | 0.690 |
| DBP (mmHg) | 80 (5) | 80 (7) | 0.968 |
| HR (bpm) | 83 (8) | 77 (11) | 0.480 |
| IOP (mmHg) | 16 (3) | 15 (2) | 0.650 |
| GLUC (mmol/L) | 4.65 (0.55) | 4.61 (0.63) | 0.927 |
| TG (mmol/L) | 2.12 (1.50) | 1.32 (0.50) | 0.094 |
| CHOL (mmol/L) | 5.25 (1.32) | 5.21 (0.80) | 0.947 |
| HDL-C (mmol/L) | 1.23 (0.50) | 1.21 (0.35) | 0.950 |
| LDL-C (mmol/L) | 3.00 (1.05) | 3.30 (0.80) | 0.475 |
| tGSH (µmol/L) | 975 (350) | 1200 (552) | 0.100 |
| GSH (µmol/L) | 838 (320) | 1154 (492) | 0.085 |
| GSSG (µmol/L) | 75 (22) | 87 (45) | 0.480 |
| NO (µmol/L) | 6.50 (3.85) | 5.40 (2.00) | 0.285 |
| FRS (%) | 10.00 (4.50) | 8.85 (6.00) | 0.700 |
| AHI (n/h) | 42 (24) | 2 (2) | <0.001 * |
| Mean (SD) | |||
|---|---|---|---|
| Parameter | Group (1) | Group (2) | p-Value (t-Test/ANCOVA) |
| OSA | Control | ||
| c-IMT | |||
| R-IMT (cm) | 0.75 (0.15) | 0.70 (0.11) | 0.300 |
| L-IMT (cm) | |||
| PWA | |||
| AIx | 25 (12) | 19 (12) | 0.025 * |
| FMD | |||
| FMDED (%) | 12.35 (10.50) | 14.00 (11.25) | 0.780 |
| Mean (SD) | |||
|---|---|---|---|
| DVA Parameter | Group (1) | Group (2) | p-Value |
| OSA | Control | ||
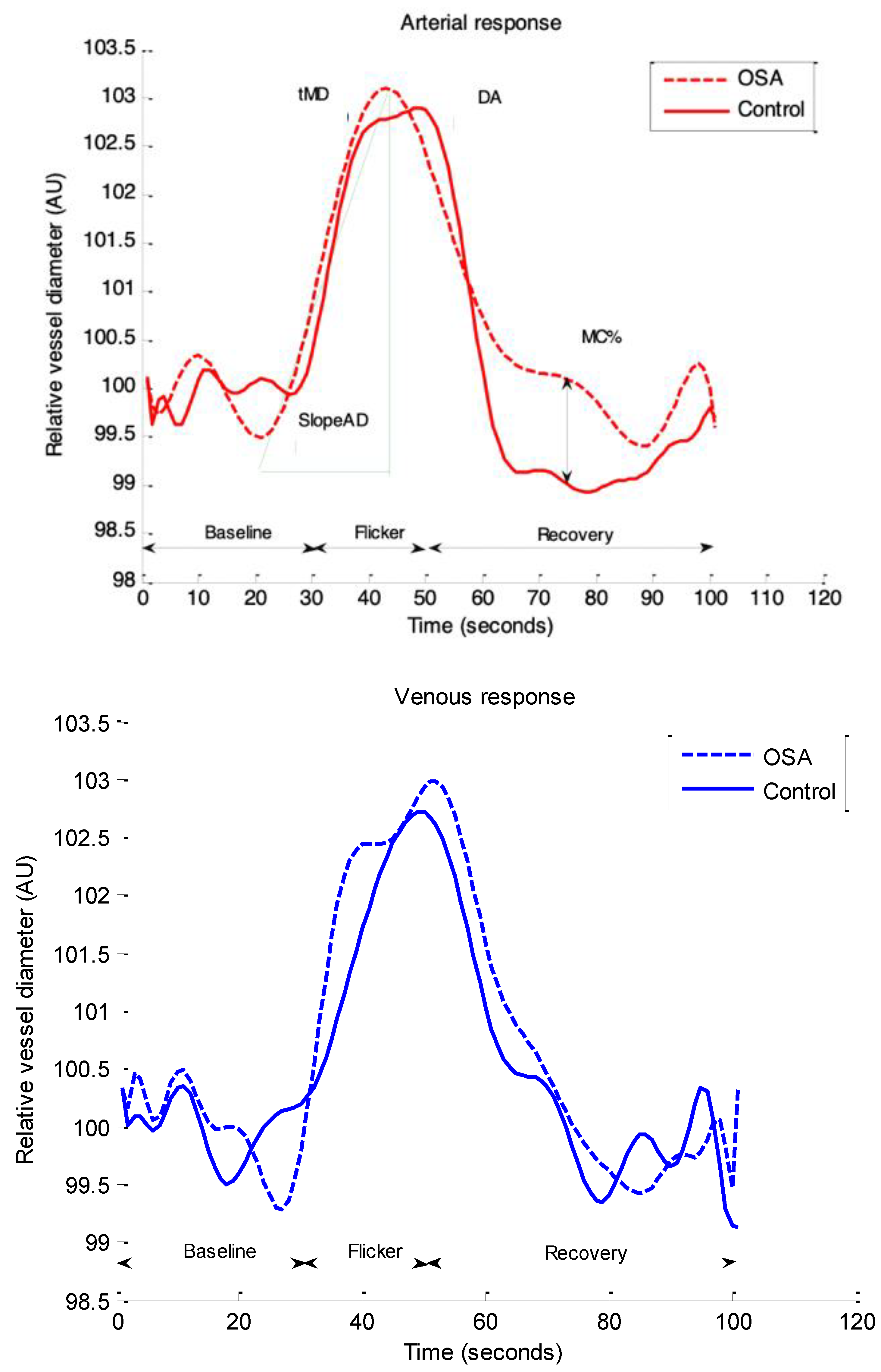
| Arteries: | |||
| Baseline | 99.55 (0.50) | 99.80 (0.20) | 0.901 |
| BDF | 5.77 (2.31) | 5.85 (2.35) | 0.888 |
| BCFR | −1.09 (3.54) | −0.60 (2.36) | 0.449 |
| DA | 4.89 (2.00) | 6.50 (2.00) | 0.004 * |
| MD% | 3.65 (2.00) | 3.70 (2.48) | 0.780 |
| MC% | −0.90 (3.54) | −2.25 (3.00) | 0.015 * |
| tMD (seconds) | 23 (10) | 18 (10) | 0.047 * |
| tMC (seconds) | 29 (10) | 29 (12) | 0.964 |
| SlopeAD | 0.22 (0.21) | 0.43 (0.40) | 0.004 * |
| SlopeAC | −0.20 (0.10) | −0.27 (0.15) | 0.410 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seshadri, S.; Shokr, H.; Gherghel, D. Retinal Microvascular Abnormalities and Systemic Arterial Stiffness Are the First Manifestation of Cardiovascular Abnormalities in Patients with Untreated Moderate to Severe Obstructive Sleep Apnoea and with Low to Intermediate Cardiovascular Risk—A Pilot Study. Biomedicines 2022, 10, 2669. https://doi.org/10.3390/biomedicines10102669
Seshadri S, Shokr H, Gherghel D. Retinal Microvascular Abnormalities and Systemic Arterial Stiffness Are the First Manifestation of Cardiovascular Abnormalities in Patients with Untreated Moderate to Severe Obstructive Sleep Apnoea and with Low to Intermediate Cardiovascular Risk—A Pilot Study. Biomedicines. 2022; 10(10):2669. https://doi.org/10.3390/biomedicines10102669
Chicago/Turabian StyleSeshadri, Swathi, Hala Shokr, and Doina Gherghel. 2022. "Retinal Microvascular Abnormalities and Systemic Arterial Stiffness Are the First Manifestation of Cardiovascular Abnormalities in Patients with Untreated Moderate to Severe Obstructive Sleep Apnoea and with Low to Intermediate Cardiovascular Risk—A Pilot Study" Biomedicines 10, no. 10: 2669. https://doi.org/10.3390/biomedicines10102669