
A Novel Automated Chemiluminescence Method for Detecting Cerebrospinal Fluid Amyloid-Beta 1-42 and 1-40, Total Tau and Phosphorylated-Tau: Implications for Improving Diagnostic Performance in Alzheimer’s Disease
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. CSF Collection
2.3. ELISA Assay
2.4. CLEIA Assay
2.5. Statistical Analysis
3. Results
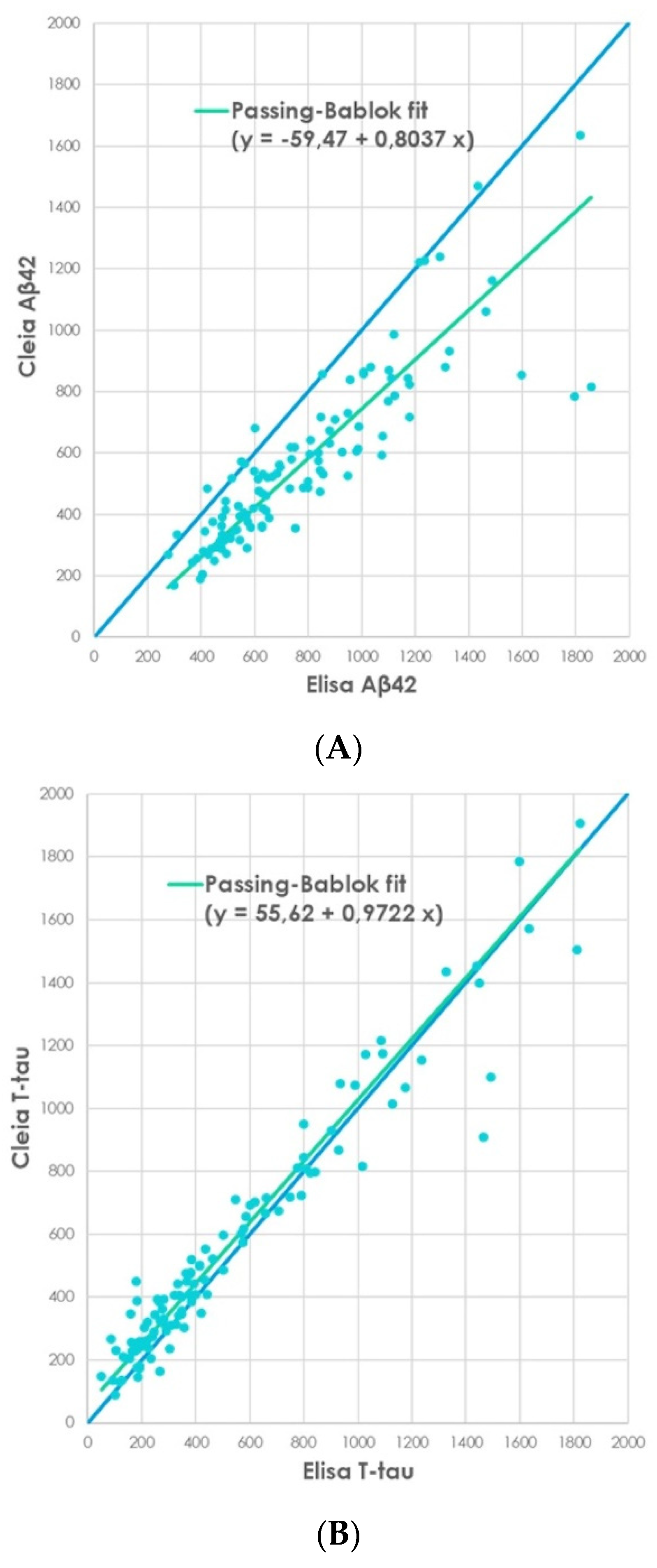
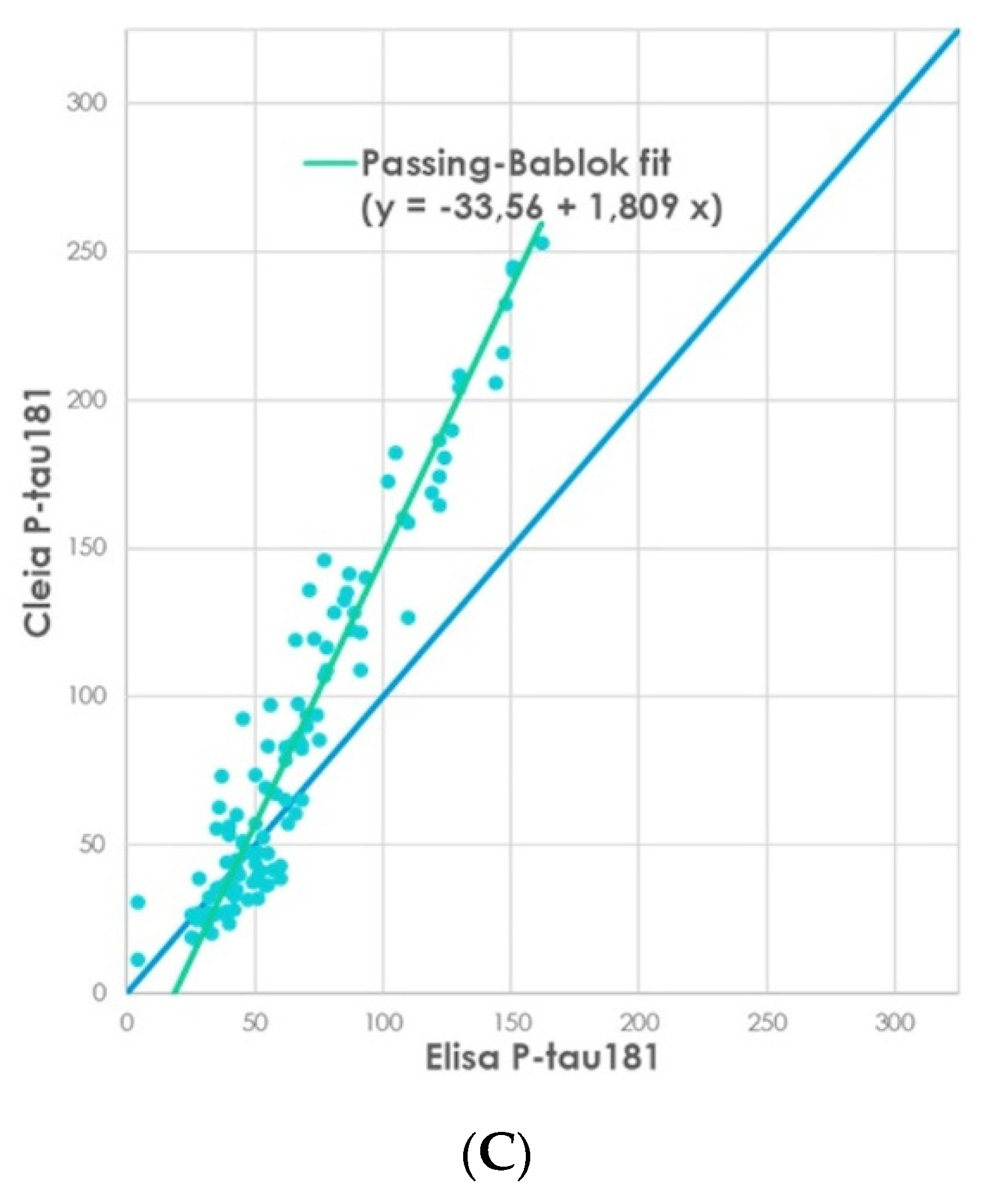
3.1. Passing-Bablok Regression Analysis in Method Comparison between INNOTEST and Lumipulse Assays
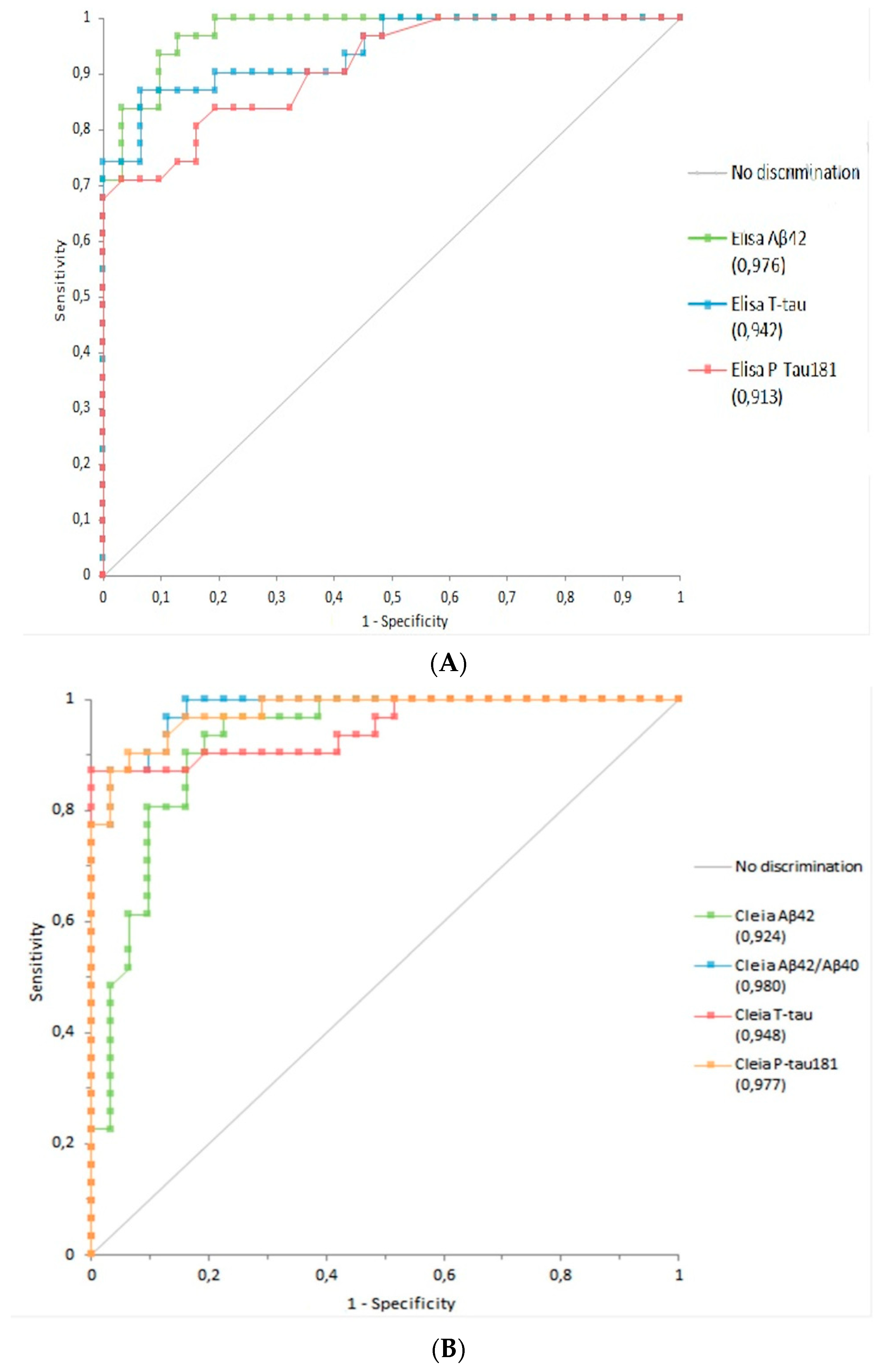
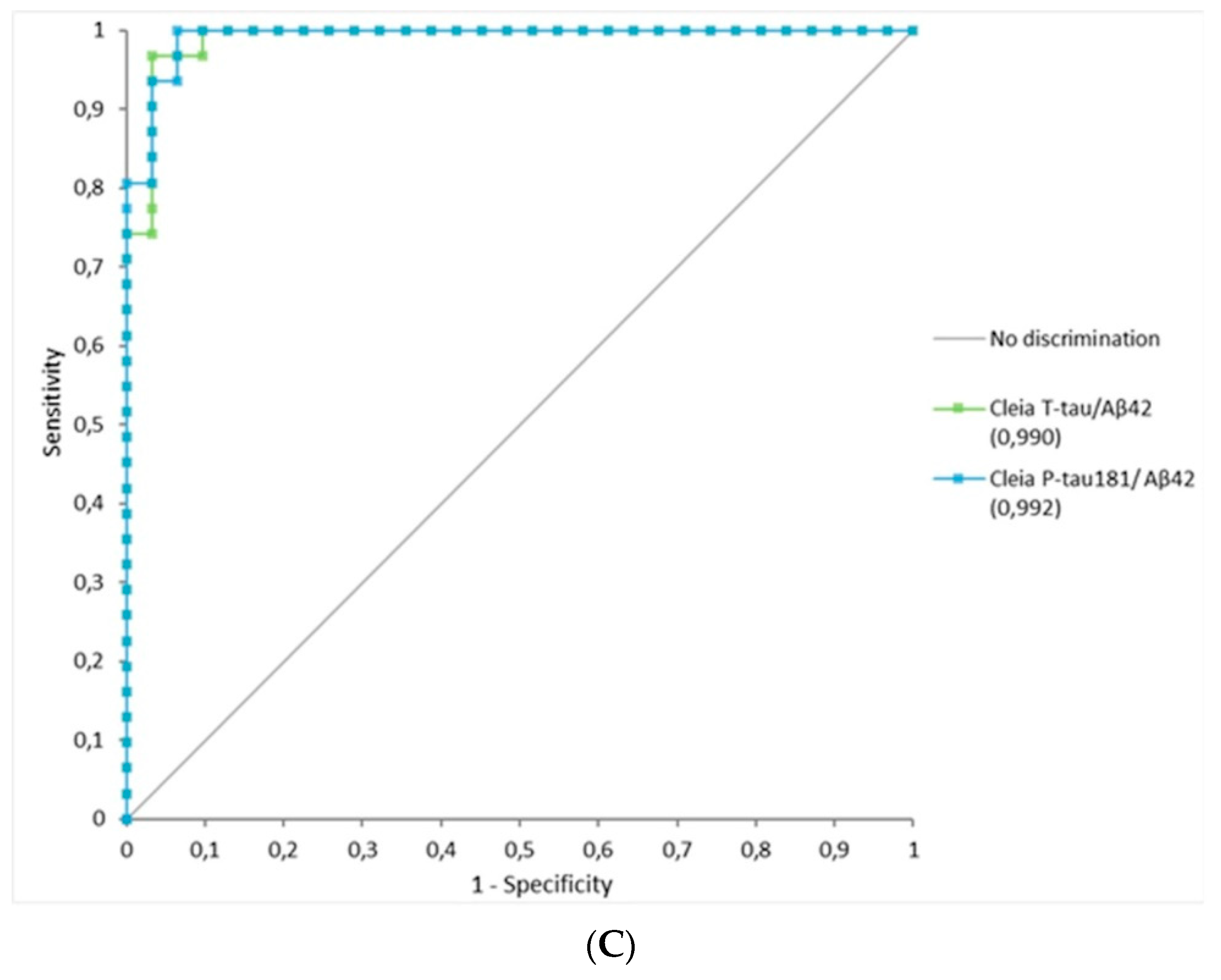
3.2. Diagnostic Performance of Lumipulse Using ROC Analysis between Both Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Blennow, K.; Dubois, B.; Fagan, A.M.; Lewczuk, P.; de Leon, M.J.; Hampel, H. Clinical Utility of Cerebrospinal Fluid Biomarkers in the Diagnosis of Early Alzheimer’s Disease. Alzheimer’s Dement. 2015, 11, 58–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattsson-Carlgren, N.; Grinberg, L.T.; Boxer, A.; Ossenkoppele, R.; Jonsson, M.; Seeley, W.; Ehrenberg, A.; Spina, S.; Janelidze, S.; Rojas-Martinex, J.; et al. Cerebrospinal Fluid Biomarkers in Autopsy-Confirmed Alzheimer Disease and Frontotemporal Lobar Degeneration. Neurology 2022, 98, e1137–e1150. [Google Scholar] [CrossRef] [PubMed]
- Sancesario, G.M.; Toniolo, S.; Chiasserini, D.; Di Santo, S.G.; Zegeer, J.; Bernardi, G.; Musicco, M.; Caltagirone, C.; SIBioC-Study Group of Clinical Biochemistry of Biological Fluids other than Blood; SINdem-ITALPLANED; et al. The Clinical Use of Cerebrospinal Fluid Biomarkers for Alzheimer’s Disease Diagnosis: The Italian Selfie. J. Alzheimer’s Dis. 2017, 55, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, S.; Dumurgier, J.; Ayrignac, X.; Marelli, C.; Alcolea, D.; Ormaechea, J.F.; Thouvenot, E.; Delaby, C.; Hirtz, C.; Vialaret, J.; et al. Cerebrospinal Fluid A Beta 1-40 Peptides Increase in Alzheimer’s Disease and Are Highly Correlated with Phospho-Tau in Control Individuals. Alzheimer’s Res. Ther. 2020, 12, 123. [Google Scholar] [CrossRef] [PubMed]
- Alcolea, D.; Pegueroles, J.; Muñoz, L.; Camacho, V.; López-Mora, D.; Fernández-León, A.; Le Bastard, N.; Huyck, E.; Nadal, A.; Olmedo, V.; et al. Agreement of Amyloid PET and CSF Biomarkers for Alzheimer’s Disease on Lumipulse. Ann. Clin. Transl. Neurol. 2019, 6, 1815–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacchi, L.; Carandini, T.; Fumagalli, G.G.; Pietroboni, A.M.; Contarino, V.E.; Siggillino, S.; Arcaro, M.; Fenoglio, C.; Zito, F.; Marotta, G.; et al. Unravelling the Association between Amyloid-PET and Cerebrospinal Fluid Biomarkers in the Alzheimer’s Disease Spectrum: Who Really Deserves an A+? J. Alzheimer’s Dis. 2022, 85, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Hampel, H.; Cummings, J.; Blennow, K.; Gao, P.; Jack, C.R.; Vergallo, A. Developing the ATX(N) Classification for Use across the Alzheimer Disease Continuum. Nat. Rev. Neurol. 2021, 17, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Vanmechelen, E.; Vanderstichele, H.; Davidsson, P.; Van Kerschaver, E.; Van Der Perre, B.; Sjögren, M.; Andreasen, N.; Blennow, K. Quantification of Tau Phosphorylated at Threonine 181 in Human Cerebrospinal Fluid: A Sandwich ELISA with a Synthetic Phosphopeptide for Standardization. Neurosci. Lett. 2000, 285, 49–52. [Google Scholar] [CrossRef]
- Blennow, K.; Wallin, A.; Agren, H.; Spenger, C.; Siegfried, J.; Vanmechelen, E. Tau Protein in Cerebrospinal Fluid: A Biochemical Marker for Axonal Degeneration in Alzheimer Disease? Mol. Chem. Neuropathol. 1995, 26, 231–245. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, N.; Hesse, C.; Davidsson, P.; Minthon, L.; Wallin, A.; Winblad, B.; Vanderstichele, H.; Vanmechelen, E.; Blennow, K. Cerebrospinal Fluid Beta-Amyloid(1-42) in Alzheimer Disease: Differences between Early- and Late-Onset Alzheimer Disease and Stability during the Course of Disease. Arch. Neurol. 1999, 56, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Delaby, C.; Teunissen, C.E.; Blennow, K.; Alcolea, D.; Arisi, I.; Amar, E.B.; Beaume, A.; Bedel, A.; Bellomo, G.; Bigot-Corbel, E.; et al. Clinical Reporting Following the Quantification of Cerebrospinal Fluid Biomarkers in Alzheimer’s Disease: An International Overview. Alzheimer’s Dement. 2021, 17, e057528. [Google Scholar] [CrossRef]
- Marlet, J.; Bernard, M. Comparison of LUMIPULSE(®) G1200 with Kryptor and Modular E170 for the Measurement of Seven Tumor Markers. J. Clin. Lab. Anal. 2016, 30, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Song, G.; Guan, W.; Wang, Q.; Liu, Y.; Wei, L. The Lumipulse G HBsAg-Quant Assay for Screening and Quantification of the Hepatitis B Surface Antigen. J. Virol. Methods 2016, 228, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Paciotti, S.; Sepe, F.N.; Eusebi, P.; Farotti, L.; Cataldi, S.; Gatticchi, L.; Parnetti, L. Diagnostic Performance of a Fully Automated Chemiluminescent Enzyme Immunoassay for Alzheimer’s Disease Diagnosis. Clin. Chim. Acta 2019, 494, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Leitão, M.J.; Silva-Spínola, A.; Santana, I.; Olmedo, V.; Nadal, A.; Le Bastard, N.; Baldeiras, I. Clinical Validation of the Lumipulse G Cerebrospinal Fluid Assays for Routine Diagnosis of Alzheimer’s Disease. Alzheimer’s Res. Ther. 2019, 11, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dakterzada, F.; López-Ortega, R.; Arias, A.; Riba-Llena, I.; Ruiz-Julián, M.; Huerto, R.; Tahan, N.; Piñol-Ripoll, G. Assessment of the Concordance and Diagnostic Accuracy between Elecsys and Lumipulse Fully Automated Platforms and Innotest. Front. Aging Neurosci. 2021, 13, 604119. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing Research Diagnostic Criteria for Alzheimer’s Disease: The IWG-2 Criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; van Swieten, J.C.; Seelaar, H.; Dopper, E.G.P.; Onyike, C.U.; et al. Sensitivity of Revised Diagnostic Criteria for the Behavioural Variant of Frontotemporal Dementia. Brain 2011, 134, 2456–2477. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I.G.; Ferman, T.J.; Thomas, A.J.; Blanc, F.; Boeve, B.F.; Fujishiro, H.; Kantarci, K.; Muscio, C.; O’Brien, J.T.; Postuma, R.B.; et al. Research Criteria for the Diagnosis of Prodromal Dementia with Lewy Bodies. Neurology 2020, 94, 743–755. [Google Scholar] [CrossRef]
- Bilić-Zulle, L. Comparison of Methods: Passing and Bablok Regression. Biochem. Med. 2011, 21, 49–52. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Kollhoff, A.L.; Howell, J.C.; Hu, W.T. Automation vs. Experience: Measuring Alzheimer’s Beta-Amyloid 1-42 Peptide in the CSF. Front. Aging Neurosci. 2018, 10, 253. [Google Scholar] [CrossRef] [PubMed]
- Gobom, J.; Parnetti, L.; Rosa-Neto, P.; Vyhnalek, M.; Gauthier, S.; Cataldi, S.; Lerch, O.; Laczo, J.; Cechova, K.; Clarin, M.; et al. Validation of the LUMIPULSE Automated Immunoassay for the Measurement of Core AD Biomarkers in Cerebrospinal Fluid. Clin. Chem. Lab. Med. 2022, 60, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Bouwman, F.H.; Frisoni, G.B.; Johnson, S.C.; Chen, X.; Engelborghs, S.; Ikeuchi, T.; Paquet, C.; Ritchie, C.; Bozeat, S.; Quevenco, F.-C.; et al. Clinical Application of CSF Biomarkers for Alzheimer’s Disease: From Rationale to Ratios. Alzheimer’s Dement. 2022, 14, e12314. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, G.; Indaco, A.; Chiasserini, D.; Maderna, E.; Paolini Paoletti, F.; Gaetani, L.; Paciotti, S.; Petricciuolo, M.; Tagliavini, F.; Giaccone, G.; et al. Machine Learning Driven Profiling of Cerebrospinal Fluid Core Biomarkers in Alzheimer’s Disease and Other Neurological Disorders. Front. Neurosci. 2021, 15, 647783. [Google Scholar] [CrossRef] [PubMed]
- Delaby, C.; Estellés, T.; Zhu, N.; Arranz, J.; Barroeta, I.; Carmona-Iragui, M.; Illán-Gala, I.; Santos-Santos, M.Á.; Altuna, M.; Sala, I.; et al. The Aβ1-42/Aβ1-40 Ratio in CSF Is More Strongly Associated to Tau Markers and Clinical Progression than Aβ1-42 Alone. Alzheimer’s Res. Ther. 2022, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Keshavan, A.; Wellington, H.; Chen, Z.; Khatun, A.; Chapman, M.; Hart, M.; Cash, D.M.; Coath, W.; Parker, T.D.; Buchanan, S.M.; et al. Concordance of CSF Measures of Alzheimer’s Pathology with Amyloid PET Status in a Preclinical Cohort: A Comparison of Lumipulse and Established Immunoassays. Alzheimer’s Dement. 2021, 13, e12131. [Google Scholar] [CrossRef] [PubMed]
- Delaby, C.; Muñoz, L.; Torres, S.; Nadal, A.; Le Bastard, N.; Lehmann, S.; Lleó, A.; Alcolea, D. Impact of CSF Storage Volume on the Analysis of Alzheimer’s Disease Biomarkers on an Automated Platform. Clin. Chim. Acta 2019, 490, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, R.; Zhu, N.; Arranz, J.; Porcel, I.; El Bounasri, S.; Sánchez, O.; Torres, S.; Julve, J.; Lleó, A.; Blanco-Vaca, F.; et al. Importance of Cerebrospinal Fluid Storage Conditions for the Alzheimer’s Disease Diagnostics on an Automated Platform. Clin. Chem. Lab. Med. 2022, 60, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Brickman, A.M.; Manly, J.J.; Honig, L.S.; Sanchez, D.; Reyes-Dumeyer, D.; Lantigua, R.A.; Lao, P.J.; Stern, Y.; Vonsattel, J.P.; Teich, A.F.; et al. Plasma P-Tau181, p-Tau217, and Other Blood-Based Alzheimer’s Disease Biomarkers in a Multi-Ethnic, Community Study. Alzheimer’s Dement. 2021, 17, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Serpente, M.; Fenoglio, C.; D’Anca, M.; Arcaro, M.; Sorrentino, F.; Visconte, C.; Arighi, A.; Fumagalli, G.G.; Porretti, L.; Cattaneo, A.; et al. MiRNA Profiling in Plasma Neural-Derived Small Extracellular Vesicles from Patients with Alzheimer’s Disease. Cells 2020, 9, 1443. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Pedrini, S.; Ashton, N.J.; Tegg, M.; Goozee, K.; Singh, A.K.; Karikari, T.K.; Simrén, J.; Vanmechelen, E.; Armstrong, N.J.; et al. Diagnostic and Prognostic Plasma Biomarkers for Preclinical Alzheimer’s Disease. Alzheimer’s Dement. 2022, 18, 1141–1154. [Google Scholar] [CrossRef] [PubMed]
- Smirnov, D.S.; Ashton, N.J.; Blennow, K.; Zetterberg, H.; Simrén, J.; Lantero-Rodriguez, J.; Karikari, T.K.; Hiniker, A.; Rissman, R.A.; Salmon, D.P.; et al. Plasma Biomarkers for Alzheimer’s Disease in Relation to Neuropathology and Cognitive Change. Acta Neuropathol. 2022, 143, 487–503. [Google Scholar] [CrossRef] [PubMed]
- Mankhong, S.; Kim, S.; Lee, S.; Kwak, H.-B.; Park, D.-H.; Joa, K.-L.; Kang, J.-H. Development of Alzheimer’s Disease Biomarkers: From CSF- to Blood-Based Biomarkers. Biomedicines 2022, 10, 850. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AD | Controls | Other Dementia | |
|---|---|---|---|
| N | 31 | 31 | 49 |
| Gender (F/M) | 14/17 | 10/21 | 15/34 |
| Age (years ± SEM) | 75 ± 2 | 73 ± 1 | 75 ± 1 |
| CSF Aβ42 ELISA (pg/mL ± SEM) | 520 ± 15 | 1063 ± 65 | 756 ± 41 |
| CSF Aβ42 CLEIA (pg/mL ± SEM) | 379 ± 21 | 788 ± 55 | 683 ± 50 |
| CSF T-tau ELISA (pg/mL ± SEM) | 603 ± 77 | 233 ± 16 | 651 ± 74 |
| CSF T-tau CLEIA (pg/mL ± SEM) | 610 ± 37 | 285 ± 16 | 683 ± 71 |
| CSF P-tau181 ELISA (pg/mL ± SEM) | 72 ± 4 | 43 ± 3 | 77 ± 6 |
| CSF P-tau181 CLEIA (pg/mL ± SEM) | 105 ± 6 | 42 ± 2 | 105 ± 12 |
| CSF Aβ42/Aβ40 CLEIA | 0.043 ± 0.002 | 0.081 ± 0.003 | 0.060 ± 0.003 |
| CSF T-tau/Aβ42 ELISA | 1.189 ± 0.001 | 0.243 ± 0.001 | 0.076 ± 0.008 |
| CSF T-tau/Aβ42 CLEIA | 1.727 ± 0.133 | 0.402 ± 0.036 | 1.806 ± 0.290 |
| CSF P-tau181/Aβ42 ELISA | 0.142 ± 0.009 | 0.045 ± 0.004 | 0.147 ± 0.023 |
| CSF P-tau181/Aβ42 CLEIA | 0.295 ± 0.021 | 0.061 ± 0.007 | 0.011 ± 0.001 |
| Biomarkers | AUC 95% CI AD vs. Controls | Sensitivity 95% CI AD vs. Controls | Specificity 95% CI AD vs. Controls | Thresholds 95% CI AD vs. Controls |
|---|---|---|---|---|
| ELISA Aβ42 | 0.98 (0.95, 0.10) | 0.90 (0.78, 0.99) | 0.84 (0.64, 0.91) | 533 (521, 550) pg/mL |
| CLEIA Aβ42 | 0.92 (0.86, 0.99) | 0.94 (0.79, 0.99) | 0.81 (0.64, 0.91) | 544 (543, 550) pg/mL |
| CLEIA Aβ42/Aβ40 | 0.98 (0.96, 0.10) | 0.90 (0.75, 0.97) | 0.90 (0.75, 0.97) | 0.055 (0.053, 0.058) |
| ELISA T-tau | 0.94 (0.89, 0.99) | 0.81 (0.57, 0.86) | 0.94 (0.79, 0.99) | 365 (353, 373) pg/mL |
| CLEIA T-tau | 0.95 (0.89, 0.10) | 0.87 (0.72, 0.95) | 0.94 (0.79, 0.99) | 402 (398, 404) pg/mL |
| ELISA P-tau181 | 0.91 (0.85, 0.98) | 0.81 (0.57, 0.86) | 0.94 (0.67, 0.95) | 55 (54.5, 57.0) pg/mL |
| CLEIA P-tau181 | 0.98 (0.95, 0.10) | 0.90 (0.75, 0.97) | 0.90 (0.72, 0.95) | 60.5 (58.5, 63.0) pg/mL |
| ELISA T-tau/Aβ42 | 0.99 (0.97, 0.10) | 0.97 (0.83, 0.10) | 0.94 (0.79, 0.99) | 0.47 (0.42, 0.84) |
| CLEIA T-tau/Aβ42 | 0.98 (0.97, 0.10) | 0.97 (0.84, 0.10) | 0.97 (0.79, 0.99) | 0.75 (0.72, 0.84) |
| ELISA P-tau181/Aβ42 | 0.98 (0.97, 0.10) | 0.96 (0.89, 0.10) | 0.90 (0.79, 0.99) | 0.07 (0.04, 0.08) |
| CLEIA P-tau181/Aβ42 | 0.99 (0.97, 0.10) | 0.97 (0.83, 0.10) | 0.94 (0.79, 0.99) | 0.13 (0.11, 0.16) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arcaro, M.; Fenoglio, C.; Serpente, M.; Arighi, A.; Fumagalli, G.G.; Sacchi, L.; Floro, S.; D’Anca, M.; Sorrentino, F.; Visconte, C.; et al. A Novel Automated Chemiluminescence Method for Detecting Cerebrospinal Fluid Amyloid-Beta 1-42 and 1-40, Total Tau and Phosphorylated-Tau: Implications for Improving Diagnostic Performance in Alzheimer’s Disease. Biomedicines 2022, 10, 2667. https://doi.org/10.3390/biomedicines10102667
Arcaro M, Fenoglio C, Serpente M, Arighi A, Fumagalli GG, Sacchi L, Floro S, D’Anca M, Sorrentino F, Visconte C, et al. A Novel Automated Chemiluminescence Method for Detecting Cerebrospinal Fluid Amyloid-Beta 1-42 and 1-40, Total Tau and Phosphorylated-Tau: Implications for Improving Diagnostic Performance in Alzheimer’s Disease. Biomedicines. 2022; 10(10):2667. https://doi.org/10.3390/biomedicines10102667
Chicago/Turabian StyleArcaro, Marina, Chiara Fenoglio, Maria Serpente, Andrea Arighi, Giorgio G. Fumagalli, Luca Sacchi, Stefano Floro, Marianna D’Anca, Federica Sorrentino, Caterina Visconte, and et al. 2022. "A Novel Automated Chemiluminescence Method for Detecting Cerebrospinal Fluid Amyloid-Beta 1-42 and 1-40, Total Tau and Phosphorylated-Tau: Implications for Improving Diagnostic Performance in Alzheimer’s Disease" Biomedicines 10, no. 10: 2667. https://doi.org/10.3390/biomedicines10102667