
Bacterial Pulmonary Co-Infections on ICU Admission: Comparison in Patients with SARS-CoV-2 and Influenza Acute Respiratory Failure: A Multicentre Cohort Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
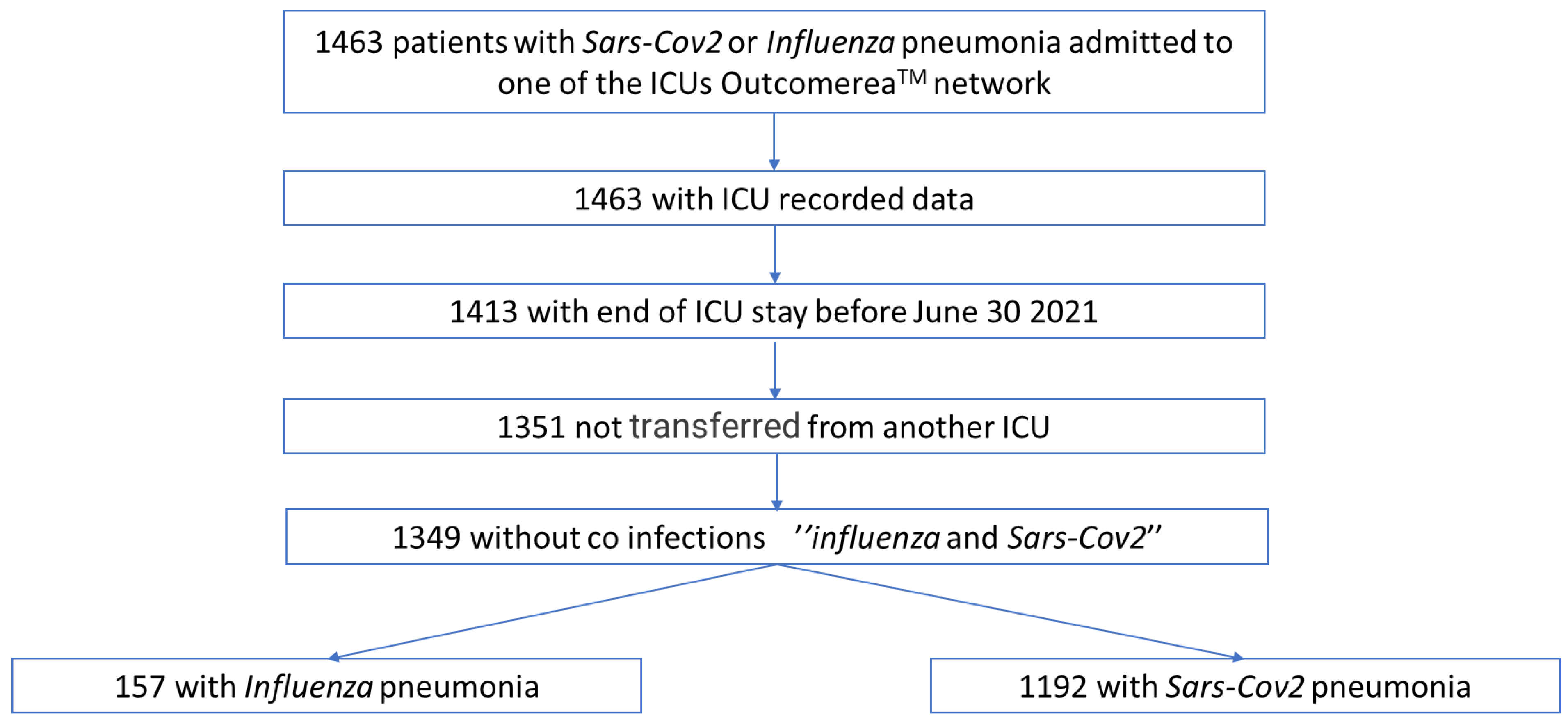
2.2. Study Population
2.3. Data Collection
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Comparison of Patients with Influenza Pneumonia versus SARS-CoV-2 Pneumonia
3.2. Comparison between Influenza Pneumonia and SARS-CoV-2 Pneumonia with and without Respiratory Bacterial Co-Infection at ICU Admission (Table 2)
3.2.1. Analysis of the Subgroup of Patients with Influenza Pneumonia

{kind=link}
{kind=link}
| Variables (n (%)/Median [IQR]) | 1. No FluRespCoBact | 2. FluRespCoBact | P 1|2 | 3. No CovRespCoBact | 4. CovRespCoBact | p 3|4 | p All | p 1|3 | p 2|4 |
|---|---|---|---|---|---|---|---|---|---|
| Number of patients | 118 | 39 | 1094 | 98 | |||||
| Time from hospital admission to ICU (days) | 1 [1; 3] | 1 [1; 2] | 0.14 | 2 [1; 4] | 2 [1; 6] | 0.33 | <0.01 | <0.01 | <0.01 |
| Age (years) | 59.8 [52.1; 71.4] | 61.1 [44.6; 72] | 0.57 | 64.4 [54.3; 73.0] | 64.1 [55.2; 70.2] | 0.48 | 0.09 | 0.07 | 0.21 |
| Sex (male) | 71 (60.2) | 22 (56.4) | 0.68 | 790 (72.2) | 74 (75.5) | 0.48 | <0.01 | <0.01 | 0.03 |
| Body mass index, kg/m² | 27.3 [24.0; 31.7] | 25.6 [21.2; 27.6] | <0.01 | 28.41 [25.1; 32.1] | 27.54 [23.9; 34.4] | 0.59 | <0.01 | 0.11 | <0.01 |
| Comorbidities | |||||||||
| Charlson score | 2 [1; 4] | 1 [0; 2] | <0.01 | 1 [0; 3] | 2 [0; 4] | 0.02 | <0.01 | <0.01 | 0.05 |
| Chronic cardiovascular disease | 20 (17.0) | 2 (5.1) | 0.07 | 275 (25.1) | 31 (31.6) | 0.16 | <0.01 | 0.05 | <0.01 |
| Chronic lung disease | 37 (31.4) | 12 (30.8) | 0.95 | 123 (11.2) | 10 (10.2) | 0.75 | <0.01 | <0.01 | <0.01 |
| Chronic kidney disease | 16 (13.6) | 2 (5.1) | 0.15 | 98 (8.96) | 10 (10.2) | 0.68 | 0.31 | 0.10 | 0.34 |
| Immunodepression * | 51 (43.2) | 8 (20.5) | 0.01 | 132 (12.1) | 14 (14.3) | 0.52 | <0.01 | <0.01 | 0.37 |
| Diabetes | 21 (17.8) | 5 (12.8) | 0.47 | 165 (15.1) | 19 (19.4) | 0.26 | 0.58 | 0.44 | 0.36 |
| Characteristics on admission | |||||||||
| SAPS II score | 39.5 [27; 51] | 42 [32; 64] | 0.10 | 33 [24; 43] | 33.5 [26; 48] | 0.16 | <0.01 | <0.01 | 0.02 |
| SOFA score | 5 [3; 7] | 7 [5; 10] | <0.01 | 5 [4; 7] | 6 [4; 8] | <0.01 | <0.01 | 0.73 | 0.08 |
| PaO2/FiO2 (missing data = 60) | 150 [103; 238] | 133 [82; 199] | 0.10 | 107 [74; 180] | 110 [75; 154] | 0.66 | <0.01 | <0.01 | 0.20 |
| Organ support at admisison | |||||||||
| Invasive mechanical ventilation | 52 (44.1) | 27 (69.2) | <0.01 | 304 (27.8) | 41 (41.8) | <0.01 | <0.01 | <0.01 | <0.01 |
| ECMO | 0 | 2 (5.1) | 0.01 | 17 (1.6) | 4 (4.1) | 0.07 | 0.04 | 0.17 | 0.79 |
| Vasopressors | 10 (8.5) | 8 (20.5) | 0.04 | 204 (18.7) | 27 (27.6) | 0.03 | <0.01 | <0.01 | 0.39 |
| Renal replacement therapy | 4 (3.4) | 5 (12.8) | 0.03 | 35 (3.2) | 10 (10.2) | <0.01 | <0.01 | 0.91 | 0.66 |
| Corticoids | 30 (25.4) | 9 (23.1) | 0.77 | 634 (57.9) | 69 (70.4) | 0.02 | <0.01 | <0.01 | <0.01 |
| Anti-Il-6 or anti-Il-1 | 0 | 0 | . | 83 (7.6) | 3 (3.1) | 0.02 | <0.01 | <0.01 | . |
| Ozeltamivir | 36 (30.5) | 15 (38.5) | 0.36 | 29 (2.7) | 0 | 0.10 | <0.01 | <0.01 | <0.01 |
| Other anti-infectious treatments on admission | |||||||||
| Antibiotics | 55 (46.6) | 26 (66.7) | 0.03 | 631 (57.7) | 73 (74.5) | <0.01 | <0.01 | 0.02 | 0.36 |
| Amoxicillin/clavulanic acid | 16 (13.5) | 11 (28.2) | 0.13 | 66 (6.1) | 13 (13.2) | <0.01 | <0.01 | <0.01 | 0.16 |
| Ureido-carboxypenicillins | 21 (17.8) | 6 (15.4) | 0.73 | 55 (5.0) | 8 (8.16) | 0.18 | <0.01 | <0.01 | 0.21 |
| 3rd-generation cephalosporin | 28 (23.7) | 17 (43.6) | 0.02 | 453 (41.5) | 50 (51.0) | 0.07 | <0.01 | <0.01 | 0.43 |
| 4th-generation cephalosporin | 3 (2.5) | 1 (2.6) | 0.99 | 46 (4.2) | 8 (8.2) | 0.07 | 0.19 | 0.38 | 0.23 |
| Macrolides | 27 (22.9) | 16 (41.0) | 0.03 | 312 (28.6) | 25 (25.5) | 0.52 | 0.16 | 0.19 | 0.07 |
| Aminosides | 10 (8.5) | 3 (7.7) | 0.88 | 40 (3.7) | 14 (14.3) | <0.01 | <0.01 | 0.01 | 0.29 |
| Fluoroquinolones | 8 (6.8) | 5 (12.8) | 0.24 | 43 (3.9) | 11 (11.2) | <0.01 | <0.01 | 0.14 | 0.79 |
| Anti-MSSA and anti-MRSA § | 5 (4.2) | 5 (12.8) | 0.16 | 22 (2.0) | 9 (9.2) | <0.01 | <0.01 | 0.05 | 0.55 |
| Bacteraemia on admission | 2 (1.7) | 4 (10.3) | 0.02 | 31 (2.8) | 11 (11.2) | <0.01 | <0.01 | 0.47 | 0.87 |
| Organ support during stay in ICU | |||||||||
| Invasive mechanical ventilation | 61 (51.7) | 28 (71.8) | 0.03 | 484 (44.2) | 62 (63.3) | <0.01 | <0.01 | 0.12 | 0.34 |
| ECMO | 1 (0.9) | 4 (10.3) | <0.01 | 50 (4.6) | 10 (10.2) | 0.01 | <0.01 | 0.06 | 0.99 |
| Vasopressors | 12 (10.2) | 9 (23.1) | 0.04 | 347 (31.7) | 43 (43.9) | 0.01 | <0.01 | <0.01 | 0.02 |
| Renal replacement therapy | 18 (15.3) | 10 (25.6) | 0.14 | 161 (14.7) | 24 (24.5) | 0.01 | 0.02 | 0.88 | 0.89 |
| VAP | 14 (11.9) | 9 (23.1) | 0.09 | 187 (17.1) | 22 (22.5) | 0.18 | 0.16 | 0.15 | 0.94 |
| Outcome | |||||||||
| Duration of invasive mechanical ventilation (days) | 11 [4; 18] | 16 [7; 23.5] | 0.68 | 12 [6; 21] | 12 [5; 18] | 0.68 | 0.45 | 0.77 | 0.77 |
| Duration of oxygenation (days) | 8 [3; 17] | 12 [6; 25] | 0.09 | 8 [4; 15] | 8 [4; 16.5] | 0.09 | 0.13 | 0.35 | 0.35 |
| Duration of ECMO (days) | 1 [1; 1] | 3.5 [2; 11.5] | 0.65 | 10.5 [3; 16] | 15 [6; 24] | 0.65 | 0.17 | 0.08 | 0.08 |
| Duration of RRT (days) | 9 [5; 14] | 3 [1; 14] | 0.20 | 8 [3; 17] | 5.5 [2; 14.5] | 0.20 | 0.61 | 0.74 | 0.74 |
| Duration of ICU stay (days) | 6 [3; 14] | 13 [7; 28] | <0.01 | 8 [4; 16] | 9.5 [5; 18] | 0.07 | <0.01 | <0.01 | 0.09 |
| Duration of hospital stay (days) | 15 [8; 35] | 27.5 [16; 50.5] | <0.01 | 15 [10; 27] | 15.5 [9; 30] | 0.95 | <0.01 | 0.69 | <0.01 |
| Mortality at D60 | 23 (19.5) | 5 (12.8) | 0.35 | 321 (29.3) | 35 (35.7) | 0.19 | <0.01 | 0.02 | <0.01 |
3.2.2. Analysis of the Subgroup of Patients with SARS-CoV-2 Pneumonia
3.2.3. Analysis of Patients in SARS-CoV-2 and Influenza Groups without RespCoBact
3.2.4. Analysis of Patients in SARS-CoV-2 and Influenza Groups with RespCoBact
3.3. Microbiological Description of Lung Co-Infections on Admission
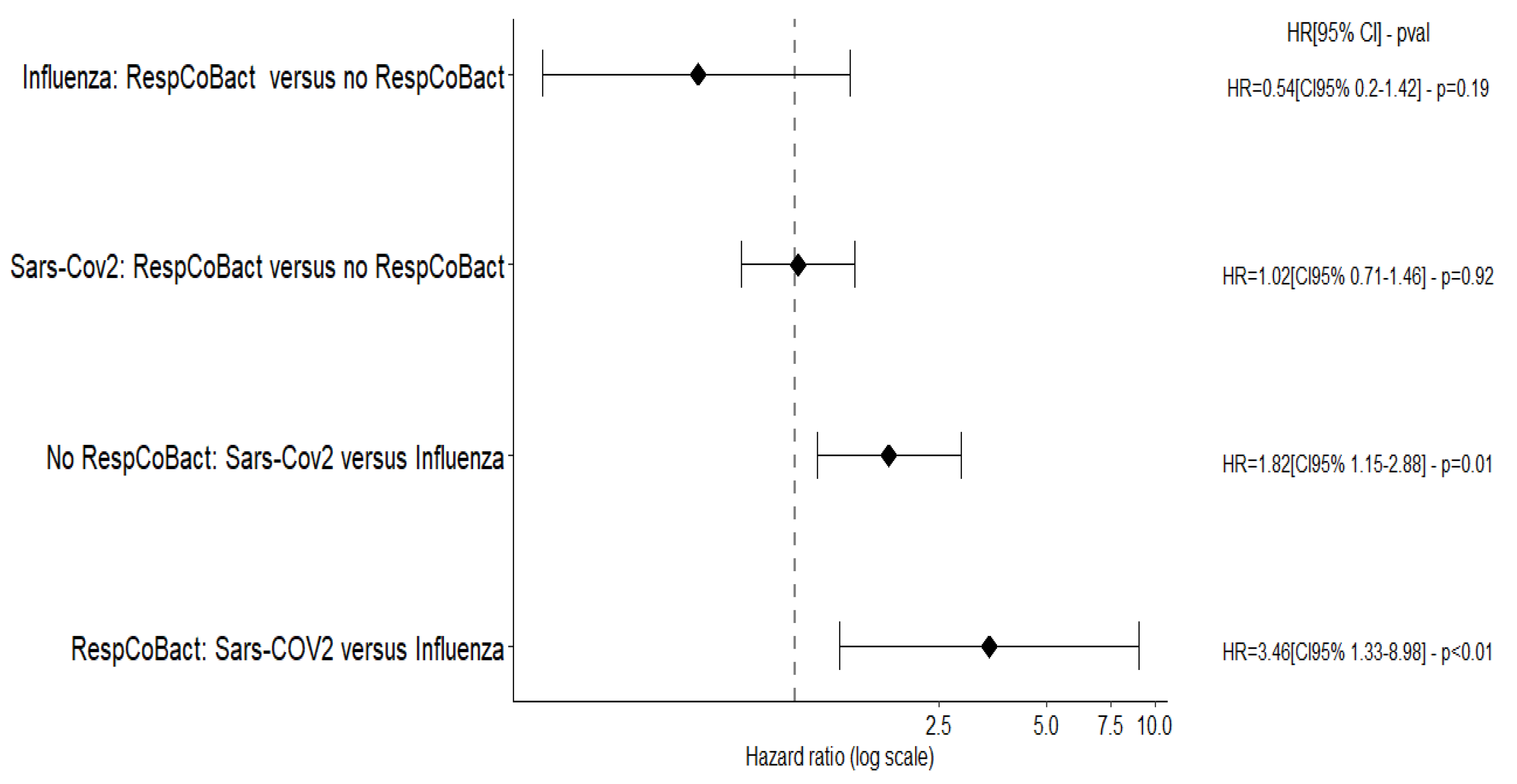
3.4. Risk Factors for Death at D60 (Figure 2; Tables S2 and S3)

3.5. Risk Factors for VAP (Tables S4 and S5)
3.6. Risk Factors for Co-Infections (Table S6)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacIntyre, C.R.; Chughtai, A.A.; Barnes, M.; Ridda, I.; Seale, H.; Toms, R.; Heywood, A. The role of pneumonia and secondary bacterial infection in fatal and serious outcomes of pandemic influenza a(H1N1)pdm09. BMC Infect. Dis. 2018, 18, 637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercat, A.; Reva-Grippe-Srlf, P.L.R.; Pham, T.; Rozé, H.; Cuquemelle, E.; Brun-Buisson, C.; Brochard, L.; Richard, J.C.M. Formes graves de la grippe H1N1 2009 chez l’adulte: L’expérience française. Réanimation 2011, 20, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Luyt, C.-E.; Combes, A.; Becquemin, M.-H.; Beigelman-Aubry, C.; Hatem, S.; Brun, A.-L.; Zraik, N.; Carrat, F.; Grenier, P.A.; Richard, J.-C.M.; et al. Long-term Outcomes of Pandemic 2009 Influenza A(H1N1)-Associated Severe ARDS. Chest 2012, 142, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Simon, M.S.; Satlin, M.J. Bacterial Coinfections in Coronavirus Disease 2019. Trends Microbiol. 2021, 29, 930–941. [Google Scholar] [CrossRef]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Metzelard, M.; Du Cheyron, D.; Lambiotte, F.; Tamion, F.; Labruyere, M.; Geronimi, C.B.; Nieszkowska, A.; et al. Early Bacterial Identification among Intubated Patients with COVID-19 or Influenza Pneumonia: A European Multicenter Comparative Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 546–556. [Google Scholar] [CrossRef]
- Calandra, T.; Cohen, J. International Sepsis Forum Definition of Infection in the ICU Consensus Conference The International Sepsis Forum Consensus Conference on Definitions of Infection in the Intensive Care Unit. Crit. Care Med. 2005, 33, 1538–1548. [Google Scholar] [CrossRef]
- Plachouras, D.; Lepape, A.; Suetens, C. ECDC definitions and methods for the surveillance of healthcare-associated infections in intensive care units. Intensive Care Med. 2018, 44, 2216–2218. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2020, 27, 83–88. [Google Scholar] [CrossRef]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Flandre, P.L.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef]
- Baskaran, V.; Lawrence, H.; Lansbury, L.E.; Webb, K.; Safavi, S.; Zainuddin, N.I.; Huq, T.; Eggleston, C.; Ellis, J.; Thakker, C.; et al. Co-infection in critically ill patients with COVID-19: An observational cohort study from England. J. Med. Microbiol. 2021, 70, 001350. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A.H. Bacterial and Fungal Coinfection in Individuals With Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- De Santis, V.; Corona, A.; Vitale, D.; Nencini, C.; Potalivo, A.; Prete, A.; Zani, G.; Malfatto, A.; Tritapepe, L.; Taddei, S.; et al. Bacterial infections in critically ill patients with SARS-2-COVID-19 infection: Results of a prospective observational multicenter study. Infection 2021, 50, 139–148. [Google Scholar] [CrossRef]
- Elabbadi, A.; Turpin, M.; Gerotziafas, G.T.; Teulier, M.; Voiriot, G.; Fartoukh, M. Bacterial coinfection in critically ill COVID-19 patients with severe pneumonia. Infection 2021, 49, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.D.; Fairfield, C.J.; Drake, T.M.; Turtle, L.; Seaton, R.A.; Wootton, D.G.; Sigfrid, L.; Harrison, E.M.; Docherty, A.B.; de Silva, T.I.; et al. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: A multicentre, prospective cohort study. Lancet Microbe 2021, 2, e354–e365. [Google Scholar] [CrossRef]
- Santos, A.P.; Gonçalves, L.C.; Oliveira, A.C.C.; Queiroz, P.H.P.; Ito, C.R.M.; Santos, M.O.; Carneiro, L.C. Bacterial Co-Infection in Patients with COVID-19 Hospitalized (ICU and Not ICU): Review and Meta-Analysis. Antibiotics 2022, 11, 894. [Google Scholar] [CrossRef]
- Pandey, M.; May, A.; Tan, L.; Hughes, H.; Jones, J.P.; Harrison, W.; Bradburn, S.; Tyrrel, S.; Muthuswamy, B.; Berry, N.; et al. Comparative incidence of early and late bloodstream and respiratory tract co-infection in patients admitted to ICU with COVID-19 pneumonia versus Influenza A or B pneumonia versus no viral pneumonia: Wales multicentre ICU cohort study. Crit. Care 2022, 26, 1–12. [Google Scholar] [CrossRef]
- Sarton, B.; Grare, M.; Vardon-Bounes, F.; Gaubert, A.; Silva, S.; Crognier, L.; Riu, B.; Seguin, T.; Georges, B.; Minville, V.; et al. Co-Infection and Ventilator-Associated Pneumonia in Critically Ill COVID-19 Patients Requiring Mechanical Ventilation: A Retrospective Cohort Study. Biomedicines 2022, 10, 1952. [Google Scholar] [CrossRef]
- Auvinen, R.; Nohynek, H.; Syrjänen, R.; Ollgren, J.; Kerttula, T.; Mäntylä, J.; Ikonen, N.; Loginov, R.; Haveri, A.; Kurkela, S.; et al. Comparison of the clinical characteristics and outcomes of hospitalized adult COVID-19 and influenza patients—A prospective observational study. Infect. Dis. 2020, 53, 111–121. [Google Scholar] [CrossRef]
- Cobb, N.L.; Sathe, N.A.; Duan, K.I.; Seitz, K.P.; Thau, M.R.; Sung, C.C.; Morrell, E.D.; Mikacenic, C.; Kim, H.N.; Liles, W.C.; et al. Comparison of Clinical Features and Outcomes in Critically Ill Patients Hospitalized with COVID-19 versus Influenza. Ann. Am. Thorac. Soc. 2021, 18, 632–640. [Google Scholar] [CrossRef]
- Zhu, L.; Yang, P.; Zhao, Y.; Zhuang, Z.; Wang, Z.; Song, R.; Zhang, J.; Liu, C.; Gao, Q.; Xu, Q.; et al. Single-Cell Sequencing of Peripheral Mononuclear Cells Reveals Distinct Immune Response Landscapes of COVID-19 and Influenza Patients. Immunity 2020, 53, 685–696.e3. [Google Scholar] [CrossRef] [PubMed]
- McElvaney, O.J.; McEvoy, N.L.; McElvaney, O.F.; Carroll, T.P.; Murphy, M.P.; Dunlea, D.M.; Ni Choileain, O.; Clarke, J.; O’Connor, E.; Hogan, G.; et al. Characterization of the Inflammatory Response to Severe COVID-19 Illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Gaunt, K.A.; Spilman, S.K.; Halub, M.E.; Jackson, J.A.; Lamb, K.D.; Sahr, S.M. High-Flow Nasal Cannula in a Mixed Adult ICU. Respir. Care 2015, 60, 1383–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R.; Higgs, E.; Randolph, A.; Smoot, B.E.; Thompson, B.T. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States*. Crit. Care Med. 2012, 40, 1487–1498. [Google Scholar] [CrossRef] [Green Version]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Patel, B.V.; Arachchillage, D.J.; Ridge, C.A.; Bianchi, P.; Doyle, J.F.; Garfield, B.; Ledot, S.; Morgan, C.; Passariello, M.; Price, S.; et al. Pulmonary Angiopathy in Severe COVID-19: Physiologic, Imaging, and Hematologic Observations. Am. J. Respir. Crit. Care Med. 2020, 202, 690–699. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.; Mafham, M.; Bell, J.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Effect of Dexamethasone in Hospitalized Patients with COVID-19—Preliminary Report. medRxiv 2020. [Google Scholar] [CrossRef]
- Morris, A.C.; Kohler, K.; De Corte, T.; Ercole, A.; De Grooth, H.-J.; Elbers, P.W.G.; Povoa, P.; Morais, R.; Koulenti, D.; Jog, S.; et al. Co-infection and ICU-acquired infection in COVID-19 ICU patients: A secondary analysis of the UNITE-COVID data set. Crit. Care 2022, 26, 1–13. [Google Scholar] [CrossRef]
- Llitjos, J.-F.; Bredin, S.; Lascarrou, J.-B.; Soumagne, T.; Cojocaru, M.; Leclerc, M.; Lepetit, A.; Gouhier, A.; Charpentier, J.; Piton, G.; et al. Increased susceptibility to intensive care unit-acquired pneumonia in severe COVID-19 patients: A multicentre retrospective cohort study. Ann. Intensive Care 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Martin-Loeches, I. Current Concepts in Community and Ventilator Associated Lower Respiratory Tract Infections in ICU Patients. Antibiotics 2020, 9, 380. [Google Scholar] [CrossRef]
- Papazian, L.; Klompas, M.; Luyt, C.-E. Ventilator-associated pneumonia in adults: A narrative review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupuis, C.; Bouadma, L.; de Montmollin, E.; Goldgran-Toledano, D.; Schwebel, C.; Reignier, J.; Neuville, M.; Ursino, M.; Siami, S.; Ruckly, S.; et al. Association Between Early Invasive Mechanical Ventilation and Day-60 Mortality in Acute Hypoxemic Respiratory Failure Related to Coronavirus Disease-2019 Pneumonia. Crit. Care Explor. 2021, 3, e0329. [Google Scholar] [CrossRef] [PubMed]

| Variables (n (%)/Median [IQR]) | Influenza (n = 157) | SARS-CoV-2 (n = 1192) | p |
|---|---|---|---|
| Time from hospital admission to ICU (days) | 1 [1; 2] | 2 [1; 4] | <0.01 |
| Age (years) | 60.1 [51.5; 71.6] | 64.4 [54.5; 72.7] | 0.02 |
| Sex (% male) | 93 (59.2) | 864 (72.5) | <0.01 |
| Body mass index (BMI) (kg/m²) | 26.8 [23.5; 30.9] | 28.4 [25; 32.2] | <0.01 |
| Comorbidities | |||
| Charlson score | 2 [1; 3] | 1 [0; 3] | <0.01 |
| Chronic cardiovascular disease | 22 (14) | 306 (25.7) | <0.01 |
| Chronic lung disease | 49 (31.2) | 133 (11.2) | <0.01 |
| Chronic kidney disease | 18 (11.5) | 108 (9.1) | 0.33 |
| Chronic liver disease | 7 (4.5) | 26 (2.2) | 0.08 |
| Immunodepression * | 59 (37.6) | 146 (12.2) | <0.01 |
| Diabetes | 26 (16.6) | 184 (15.4) | 0.71 |
| Characteristics on admission | |||
| SAPS II score | 40 [28; 54] | 33 [24; 43] | <0.01 |
| SOFA score | 5 [4; 8] | 5 [4; 7] | 0.06 |
| Biological data | |||
| Leucocytes elts/mm3 (missing data = 24) | 9385 [4520; 14,700] | 9000 [6660; 12,200] | 0.48 |
| PaO2/FiO2 (missing data = 61) | 148 [95; 215] | 108 [74; 177] | <0.01 |
| Pulmonary embolism | 0 (0) | 36 (3) | 0.03 |
| Ventilatory support on admission | |||
| Invasive mechanical ventilation | 79 (50.3) | 345 (29) | <0.01 |
| High-flow nasal cannula | 13 (8.3) | 530 (44.5) | <0.01 |
| Continuous positive airway pressure | 30 (19.1) | 138 (11.6) | <0.01 |
| ECMO | 2 (1.3) | 21 (1.8) | 0.66 |
| Vasopressors | 18 (11.5) | 231 (19.4) | 0.02 |
| Renal replacement therapy | 9 (5.7) | 45 (3.8) | 0.24 |
| Corticoids | 39 (24.8) | 703 (59) | <0.01 |
| Il1 or Il6 receptor antagonists | 0 (0) | 86 (7.2) | <0.01 |
| Lopinavir, ritonavir | 0 (0) | 171 (14.4) | <0.01 |
| Hydroxychloroquine | 0 (0) | 64 (5.4) | <0.01 |
| Remdesivir | 0 (0) | 169 (14.2) | <0.01 |
| Ozeltamivir | 51 (32.5) | 29 (2.4) | <0.01 |
| Antibiotics | 81 (51.6) | 704 (59.1) | 0.07 |
| Amoxicillin/clavulanic acid | 27 (17.2) | 79 (1.7) | <0.01 |
| Ureido-carboxypenicillins | 27 (17.2) | 63 (5.3) | <0.01 |
| 3rd-generation cephalosporin | 45 (28.7) | 503 (42.2) | <0.01 |
| 4th-generation cephalosporin | 4 (2.5) | 54 (4.5) | 0.25 |
| Macrolides | 43 (27.4) | 337 (28.3) | 0.81 |
| Aminoglycosides | 13 (8.3) | 54 (4.5) | 0.04 |
| Fluoroquinolones | 13 (8.3) | 54 (4.5) | 0.04 |
| Anti-MSSA and anti-MRSA § | 12 (7.6) | 31 (2.6) | <0.01 |
| Co-infections on admission | |||
| Bacterial pneumonia | 39 (24.8) | 98 (8.2) | <0.01 |
| Hospital-acquired pneumonia | 6 (3.8) | 41 (3.4) | 0.81 |
| Organ support during hospital stay | |||
| Invasive mechanical ventilation | 89 (56.7) | 546 (45.8) | 0.01 |
| Prone position | 20 (12.7) | 293 (24.6) | <0.01 |
| ECMO | 5 (3.2) | 60 (5) | 0.31 |
| Vasopressors | 21 (13.4) | 390 (32.7) | <0.01 |
| Renal replacement therapy | 28 (17.8) | 185 (15.5) | 0.45 |
| VAP | 23 (14.6) | 209 (17.5) | 0.37 |
| VAP among the patients at risk of VAP | 23/84 (27.3) | 209/522 (40.0) | 0.03 |
| Outcome | |||
| Duration of invasive mechanical ventilation (days) | 12 [5; 20] | 12 [6; 21] | 0.77 |
| Duration of ECMO (days) | 3 [1; 4] | 11 [4; 16.5] | 0.08 |
| Duration of RRT (days) | 8.5 [2.5; 14] | 8 [3; 16] | 0.74 |
| Duration of ICU stay (days) | 7 [4; 17] | 8 [4; 16] | 0.23 |
| Duration of hospital stay (days) | 17 [9; 36] | 15 [9.5; 27] | 0.15 |
| Mortality at D60 | 28 (17.8) | 356 (29.9) | <0.01 |
| All | Community-Acquired | Hospital-Acquired | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Flu | Cov | p | All | Flu | Cov | p | All | Flu | Cov | p | |
| Number of infections | 135 | 36 | 99 | 88 | 31 | 57 | . | 47 | 5 | 42 | . | |
| Gram-positive cocci | 64 (47.4) | 16 (44.4) | 48 (48.5) | 0.68 | 43 (48.8) | 13 (41.9) | 30 (52.6) | 0.34 | 21 (44.6) | 3 (60) | 18 (42.9) | 0.47 |
| Streptococcus pneumoniae | 20 (14.8) | 8 (22.2) | 12 (12.1) | 0.14 | 12 (13.6) | 6 (19.4) | 6 (10.5) | 0.25 | 8 (17) | 2 (40) | 6 (14.3) | 0.15 |
| Staphyloccus aureus | 35 (26) | 7 (19.4) | 28 (28.3) | 0.30 | 28 (31.8) | 6 (19.4) | 22 (38.6) | 0.06 | 7 (14.8) | 1 (20) | 6 (14.3) | 0.73 |
| Enterococcussp. | 3 (2.2) | 0 (0) | 3 (3) | 0.29 | 1 (1.2) | 0 (0) | 1 (1.8) | 0.46 | 2 (4.2) | 0 (0) | 2 (4.8) | 0.62 |
| Moraxella catarrhalis | 4 (3) | 1 (2.8) | 3 (3) | 0.94 | 2 (2.2) | 0 (0) | 2 (3.5) | 0.29 | 2 (4.2) | 1 (20) | 1 (2.4) | 0.07 |
| Gram-negative bacilli | 67 (49.6) | 11 (30.6) | 56 (56.6) | <0.01 | 41 (46.6) | 11 (35.5) | 30 (52.6) | 0.12 | 26 (55.4) | 0 (0) | 26 (61.9) | <0.01 |
| Haemophilus | 25 (18.6) | 10 (27.8) | 15 (15.2) | 0.09 | 21 (23.8) | 10 (32.3) | 11 (19.3) | 0.17 | 4 (8.6) | 0 (0) | 4 (9.5) | 0.47 |
| Enterobacteriaceae | 43 (31.8) | 6 (16.7) | 37 (37.4) | 0.02 | 21 (23.8) | 5 (16.1) | 16 (28.1) | 0.21 | 22 (46.8) | 1 (20) | 21 (50) | 0.20 |
| Group 1 or 2 enteric bacteria | 26 (19.2) | 2 (5.6) | 24 (24.2) | 0.01 | 13 (14.8) | 1 (3.2) | 12 (21.1) | 0.02 | 13 (27.6) | 1 (20) | 12 (28.6) | 0.69 |
| Proteus | 2 (1.4) | 1 (2.8) | 1 (1) | 0.45 | 2 (2.2) | 1 (3.2) | 1 (1.8) | 0.66 | 0 | . | ||
| Escherichia coli | 12 (8.8) | 2 (5.6) | 10 (10.1) | 0.41 | 6 (6.8) | 1 (3.2) | 5 (8.8) | 0.32 | 6 (12.8) | 1 (20) | 5 (11.9) | 0.61 |
| Klebsiella | 11 (8.2) | 0 (0) | 11 (11.1) | 0.04 | 6 (6.8) | 0 (0) | 6 (10.5) | 0.06 | 5 (10.6) | 0 (0) | 5 (11.9) | 0.41 |
| Citrobacter koseri | 2 (1.4) | 0 (0) | 2 (2) | 0.39 | 0 | . | 2 (4.2) | 0 (0) | 2 (4.8) | 0.62 | ||
| Group 3 enteric bacteria | 20 (14.8) | 0 (0) | 20 (20.2) | <0.01 | 7 (8) | 0 (0) | 7 (12.3) | 0.04 | 13 (27.6) | 0 (0) | 13 (31) | 0.14 |
| Enterobacter | 13 (9.6) | 0 (0) | 13 (13.1) | 0.02 | 4 (4.6) | 0 (0) | 4 (7) | 0.13 | 9 (19.2) | 0 (0) | 9 (21.4) | 0.25 |
| Serratia | 6 (4.4) | 0 (0) | 6 (6.1) | 0.13 | 3 (3.4) | 0 (0) | 3 (5.3) | 0.19 | 3 (6.4) | 0 (0) | 3 (7.1) | 0.54 |
| Citrobacter freundii | 1 (0.8) | 0 (0) | 1 (1) | 0.55 | 0 | . | 1 (2.2) | 0 (0) | 1 (2.4) | 0.73 | ||
| Morganella | 1 (0.8) | 0 (0) | 1 (1) | 0.55 | 0 | . | 1 (2.2) | 0 (0) | 1 (2.4) | 0.73 | ||
| Nonfermentative bacteria | 11 (8.2) | 1 (2.8) | 10 (10.1) | 0.17 | 6 (6.8) | 1 (3.2) | 5 (8.8) | 0.32 | 5 (10.6) | 0 (0) | 5 (11.9) | 0.41 |
| Pseudomonas aeruginosa | 7 (5.2) | 1 (2.8) | 6 (6.1) | 0.45 | 4 (4.6) | 1 (3.2) | 3 (5.3) | 0.66 | 3 (6.4) | 0 (0) | 3 (7.1) | 0.54 |
| Stenotrophomonas maltophilia | 3 (2.2) | 1 (2.8) | 2 (2) | 0.79 | 2 (2.2) | 1 (3.2) | 1 (1.8) | 0.66 | 1 (2.2) | 0 (0) | 1 (2.4) | 0.73 |
| Acinetobacter baumannii | 3 (2.2) | 0 (0) | 3 (3) | 0.29 | 2 (2.2) | 0 (0) | 2 (3.5) | 0.29 | 1 (2.2) | 0 (0) | 1 (2.4) | 0.73 |
| Intracellular bacteria | 1 (0.8) | 0 (0) | 1 (1) | 0.55 | 1 (1.2) | 0 (0) | 1 (1.8) | 0.46 | 0 | . | ||
| Drug-resistant bacteria | 49 (36.2) | 20 (55.6) | 29 (29.3) | <0.01 | 34 (38.6) | 17 (54.8) | 17 (29.8) | 0.02 | 15 (32) | 3 (60) | 12 (28.6) | 0.15 |
| Extended-spectrum beta-lactamase | 5 (3.8) | 0 (0) | 5 (5.1) | 0.17 | 1 (1.2) | 0 (0) | 1 (1.8) | 0.46 | 4 (8.6) | 0 (0) | 4 (9.5) | 0.47 |
| Carbapenemase | 0 | 0 | 0 | |||||||||
| AmpC-hyperproduction | 0 | 0 | 0 | |||||||||
| Resistant Pseudomonas aeruginosa | 2 (1.4) | 1 (2.8) | 1 (1) | 0.45 | 2 (2.2) | 1 (3.2) | 1 (1.8) | 0.66 | 0 | |||
| Methicillin-resistant Staphyloccus aureus | 2 (1.4) | 1 (2.8) | 1 (1) | 0.45 | 2 (2.2) | 1 (3.2) | 1 (1.8) | 0.66 | 0 | . | ||
| More than one pathogen | 15 (11.2) | 1 (2.8) | 14 (14.1) | 0.06 | 9 (10.2) | 1 (3.2) | 8 (14) | 0.11 | 6 (12.8) | 0 (0) | 6 (14.3) | 0.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delhommeau, G.; Buetti, N.; Neuville, M.; Siami, S.; Cohen, Y.; Laurent, V.; Mourvillier, B.; Reignier, J.; Goldgran-Toledano, D.; Schwebel, C.; et al. Bacterial Pulmonary Co-Infections on ICU Admission: Comparison in Patients with SARS-CoV-2 and Influenza Acute Respiratory Failure: A Multicentre Cohort Study. Biomedicines 2022, 10, 2646. https://doi.org/10.3390/biomedicines10102646
Delhommeau G, Buetti N, Neuville M, Siami S, Cohen Y, Laurent V, Mourvillier B, Reignier J, Goldgran-Toledano D, Schwebel C, et al. Bacterial Pulmonary Co-Infections on ICU Admission: Comparison in Patients with SARS-CoV-2 and Influenza Acute Respiratory Failure: A Multicentre Cohort Study. Biomedicines. 2022; 10(10):2646. https://doi.org/10.3390/biomedicines10102646
Chicago/Turabian StyleDelhommeau, Grégoire, Niccolò Buetti, Mathilde Neuville, Shidasp Siami, Yves Cohen, Virginie Laurent, Bruno Mourvillier, Jean Reignier, Dany Goldgran-Toledano, Carole Schwebel, and et al. 2022. "Bacterial Pulmonary Co-Infections on ICU Admission: Comparison in Patients with SARS-CoV-2 and Influenza Acute Respiratory Failure: A Multicentre Cohort Study" Biomedicines 10, no. 10: 2646. https://doi.org/10.3390/biomedicines10102646