
Bronchial Asthma as a Cardiovascular Risk Factor: A Prospective Observational Study
 , , ,
, , , 
Abstract
:1. Introduction
2. Aims
3. Materials and Methods
3.1. Study Population
3.2. Reactive Hyperemia Index Measurements
3.3. Laboratory Analysis
3.4. Statistical Analysis
3.5. Ethics
4. Results
4.1. Demographic Data of the Study Population
4.2. RHI and Biomarkers
4.3. Correlation Analysis
5. Discussion
Benefits and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACT | asthma control test |
| ADMA | asymmetric dimethyl arginine |
| AS | atherosclerosis |
| BMI | body mass index |
| CF | cystic fibrosis |
| COPD | chronic obstructive pulmonary disease |
| CVD | cardiovascular disease |
| ECP | eosinophil cationic protein |
| ED | endothelial dysfunction |
| FENO | fractional exhaled nitric oxide |
| FEF25-50 | the forced expiratory flow between 25 and 50% of the forced vital capacity |
| FMD | flow-mediated dilatation |
| HI | healthy individuals |
| hsCRP | high-sensitive C-reactive protein |
| ICS | inhaled corticosteroids |
| IgE | immunoglobulin E |
| sIgE | specific immunoglobulin E |
| LABA | long-acting beta-agonist |
| LAMA | long-acting muscarinic antagonist |
| LTRA | leukotriene receptor antagonist |
| NO | nitric oxide |
| OCS | oral corticosteroid |
| OMA | omalizumab |
| PAT | peripheral arterial tone |
| RHI | reactive hyperemia index |
| TPH | theophylline |
| VCAM-1 | vascular cells adhesive molecule |
| VEGF | vascular endothelial growth factor |
References
- Green, F.H.Y.; Butt, J.C.; James, A.L.; Carroll, N.G. Abnormalities of the Bronchial Arteries in Asthma. Chest 2006, 130, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Fleming, L.; Murray, C.; Bansal, A.T.; Hashimoto, S.; Bisgaard, H.; Bush, A.; Frey, U.; Hedlin, G.; Singer, F.; van Aalderen, W.M.; et al. The Burden of Severe Asthma in Childhood and Adolescence: Results from the Paediatric U-BIOPRED Cohorts. Eur. Respir. J. 2015, 46, 1322–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makieieva, N.; Butov, D.; Vasylchenko, Y.; Biriukova, M.; Serhiienko, K.; Morozov, O. Endothelial Dysfunction in Children with Clinically Stable and Exacerbated Asthma. Adv. Respir. Med. 2019, 87, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.M.; Truong, S.T.; Wong, N.D. Association of Adult-Onset Asthma with Specific Cardiovascular Conditions. Respir. Med. 2012, 106, 948–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Fu, Y.; Wang, K. Asthma and Risk of Coronary Heart Disease. Ann. Allergy Asthma Immunol. 2017, 118, 689–695. [Google Scholar] [CrossRef] [Green Version]
- Voelkel, N.F.; Gomez-Arroyo, J.; Mizuno, S. COPD/Emphysema: The Vascular Story. Pulm. Circ. 2011, 1, 320–326. [Google Scholar] [CrossRef] [Green Version]
- Green, C.E.; Turner, A.M. The Role of the Endothelium in Asthma and Chronic Obstructive Pulmonary Disease (COPD). Respir. Res. 2017, 18, 20. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Kobayashi, S.; Fujino, N.; Suzuki, T.; Ota, C.; Tando, Y.; Yamada, M.; Yanai, M.; Yamaya, M.; Kurosawa, S.; et al. Annual FEV1Changes and Numbers of Circulating Endothelial Microparticles in Patients with COPD: A Prospective Study. BMJ Open 2014, 4, e004571. [Google Scholar] [CrossRef] [Green Version]
- Thomashow, M.A.; Shimbo, D.; Parikh, M.A.; Hoffman, E.A.; Vogel-Claussen, J.; Hueper, K.; Fu, J.; Liu, C.-Y.; Bluemke, D.A.; Ventetuolo, C.E.; et al. Endothelial Microparticles in Mild Chronic Obstructive Pulmonary Disease and Emphysema. The Multi-Ethnic Study of Atherosclerosis Chronic Obstructive Pulmonary Disease Study. Am. J. Respir. Crit. Care Med. 2013, 188, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Hisata, S.; Racanelli, A.C.; Kermani, P.; Schreiner, R.; Houghton, S.; Palikuqi, B.; Kunar, B.; Zhou, A.; McConn, K.; Capili, A.; et al. Reversal of Emphysema by Restoration of Pulmonary Endothelial Cells. J. Exp. Med. 2021, 218, e20200938. [Google Scholar] [CrossRef]
- Reverri, E.J.; Morrissey, B.M.; Cross, C.E.; Steinberg, F.M. Inflammation, Oxidative Stress, and Cardiovascular Disease Risk Factors in Adults with Cystic Fibrosis. Free Radic. Biol. Med. 2014, 76, 261–277. [Google Scholar] [CrossRef] [PubMed]
- Tucker, M.A.; Fox, B.M.; Seigler, N.; Rodriguez-Miguelez, P.; Looney, J.; Thomas, J.; McKie, K.T.; Forseen, C.; Davison, G.W.; Harris, R.A. Endothelial Dysfunction in Cystic Fibrosis: Role of Oxidative Stress. Oxid. Med. Cell. Longev. 2019, 1629638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olveira, G.; Olveira, C.; Dorado, A.; García-Fuentes, E.; Rubio, E.; Tinahones, F.; Soriguer, F.; Murri, M. Cellular and Plasma Oxidative Stress Biomarkers Are Raised in Adults with Bronchiectasis. Clin. Nutr. 2013, 32, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Declercq, M.; Treps, L.; Carmeliet, P.; Witters, P. The Role of Endothelial Cells in Cystic Fibrosis. J. Cyst. Fibros. 2019, 18, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Curjuric, I.; Imboden, M.; Bettschart, R.; Caviezel, S.; Dratva, J.; Pons, M.; Rothe, T.; Schmidt-Trucksäss, A.; Stolz, D.; Thun, G.A.; et al. Alpha-1 Antitrypsin Deficiency: From the Lung to the Heart? Atherosclerosis 2018, 270, 166–172. [Google Scholar] [CrossRef]
- Duckers, J.M.; Shale, D.J.; Stockley, R.A.; Gale, N.S.; Evans, B.A.; Cockcroft, J.R.; Bolton, C.E. Cardiovascular and Musculoskeletal Co-Morbidities in Patients with Alpha 1 Antitrypsin Deficiency. Respir. Res. 2010, 11, 173. [Google Scholar] [CrossRef]
- Lavie, L. Oxidative Stress in Obstructive Sleep Apnea and Intermittent Hypoxia—Revisited—The Bad Ugly and Good: Implications to the Heart and Brain. Sleep Med. Rev. 2015, 20, 27–45. [Google Scholar] [CrossRef]
- Heck, S.; Nguyen, J.; Le, D.-D.; Bals, R.; Dinh, Q.T. Pharmacological Therapy of Bronchial Asthma: The Role of Biologicals. Int. Arch. Allergy Immunol. 2015, 168, 241–252. [Google Scholar] [CrossRef]
- Bäck, M.; Hansson, G.K. Anti-Inflammatory Therapies for Atherosclerosis. Nat. Rev. Cardiol. 2015, 12, 199–211. [Google Scholar] [CrossRef]
- Hamburg, N.M.; Keyes, M.J.; Larson, M.G.; Vasan, R.S.; Schnabel, R.; Pryde, M.M.; Mitchell, G.F.; Sheffy, J.; Vita, J.A.; Benjamin, E.J. Cross-Sectional Relations of Digital Vascular Function to Cardiovascular Risk Factors in the Framingham Heart Study. Circulation 2008, 117, 2467–2474. [Google Scholar] [CrossRef]
- Kanazawa, H.; Nomura, S.; Asai, K. Roles of Angiopoietin-1 and Angiopoietin-2 on Airway Microvascular Permeability in Asthmatic Patients. Chest 2007, 131, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Simcock, D.E.; Kanabar, V.; Clarke, G.W.; O’Connor, B.J.; Lee, T.H.; Hirst, S.J. Proangiogenic Activity in Bronchoalveolar Lavage Fluid from Patients with Asthma. Am. J. Respir. Crit. Care Med. 2007, 176, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Kreslová, M.; Sýkorová, A.; Jehlička, P.; Kobr, J.; Sýkora, J. Endothelial Dysfunction in Children and Young Adults: Clinical Implications and New Perspectives. In Advances in Medicine and Biology; Berhardt, L.V., Ed.; Nova Science Publishers: New York, NY, USA, 2022; Volume 192, pp. 99–195. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.-C.; Plummer, A.L.; Taylor, D.R. An Official ATS Clinical Practice Guideline: Interpretation of Exhaled Nitric Oxide Levels (FeNO) for Clinical Applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widlansky, M.E.; Gokce, N.; Keaney, J.F., Jr.; Vita, J.A. The Clinical Implications of Endothelial Dysfunction. J. Am. Coll. Cardiol. 2003, 42, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Cheng, G.; He, L.; Liao, B.; Du, Y.; Xie, X.; Zhang, S.; Li, G.; Wang, Y.; Zhang, Y. Adults with Current Asthma but Not Former Asthma Have Higher All-Cause and Cardiovascular Mortality: A Population-Based Prospective Cohort Study. Sci. Rep. 2021, 11, 1329. [Google Scholar] [CrossRef]
- Yildiz, P.; Oflaz, H.; Cine, N.; Genchallac, H.; Erginel-Ünaltuna, N.; Yildiz, A.; Yilmaz, V. Endothelial Dysfunction in Patients with Asthma: The Role of Polymorphisms of ACE and Endothelial NOS Genes. J. Asthma 2004, 41, 159–166. [Google Scholar] [CrossRef]
- Cortez e Castro, M.; Ferreira, J.; Matos, A.; Bicho, M. Endothelial Dysfunction in Asthma: Enos, Inos and Ace Polymorphisms. ERJ Open Res. 2020, 6, 45. [Google Scholar] [CrossRef]
- Bonetti, P.O.; Pumper, G.M.; Higano, S.T.; Holmes, D.R., Jr.; Kuvin, J.T.; Lerman, A. Noninvasive Identification of Patients with Early Coronary Atherosclerosis by Assessment of Digital Reactive Hyperemia. J. Am. Coll. Cardiol. 2004, 44, 2137–2141. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, A.; Tomiyama, H.; Maruhashi, T.; Matsuzawa, Y.; Miyoshi, T.; Kabutoya, T.; Kario, K.; Sugiyama, S.; Munakata, M.; Ito, H.; et al. Physiological Diagnostic Criteria for Vascular Failure. Hypertension 2018, 72, 1060–1071. [Google Scholar] [CrossRef]
- Terl, M.; Sedlák, V.; Cap, P.; Dvořáková, R.; Kašák, V.; Kočí, T.; Novotna, B.; Seberova, E.; Panzner, P.; Zindr, V. Asthma management: A new phenotype-based approach using presence of eosinophilia and allergy. Allergy 2017, 72, 1279–1287. [Google Scholar] [CrossRef] [Green Version]
- Nichols, M.; Teufel, R.; Miller, S.; Madisetti, M.; Giovanni, C.S.; Chike-Harris, K.; Jones, L.; Prentice, M.; Ruggiero, K.; Kelechi, T. Managing Asthma and Obesity Related Symptoms (MATADORS): An MHealth Intervention to Facilitate Symptom Self-Management among Youth. Int. J. Environ. Res. Public Health 2020, 17, 7750. [Google Scholar] [CrossRef] [PubMed]
- Hadi, H.A.; Carr, C.S.; Al Suwaidi, J. Endothelial dysfunction: Cardiovascular risk factors, therapy, and outcome. Vasc. Health Risk Manag. 2005, 1, 183–198. [Google Scholar]
- Tattersall, M.C.; Guo, M.; Korcarz, C.E.; Gepner, A.D.; Kaufman, J.D.; Liu, K.J.; Barr, R.G.; Donohue, K.M.; McClelland, R.L.; Delaney, J.A.; et al. Asthma Predicts Cardiovascular Disease Events. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 1520–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinmann, M.; Abbas, C.; Singer, F.; Casaulta, C.; Regamey, N.; Haffner, D.; Fischer, D.-C.; Simonetti, G.D. Arterial Stiffness Is Increased in Asthmatic Children. Eur. J. Pediatr. 2014, 174, 519–523. [Google Scholar] [CrossRef]
- Vijayakumar, J.; Subramanian, S.; Singh, P.; Corsini, E.; Fontanez, S.; Lawler, M.; Kaplan, R.; Brady, T.J.; Hoffmann, U.; Tawakol, A. Arterial Inflammation in Bronchial Asthma. J. Nucl. Cardiol. 2013, 20, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Holguin, F.; Grasemann, H.; Sharma, S.; Winnica, D.; Wasil, K.; Smith, V.; Cruse, M.H.; Perez, N.; Coleman, E.; Scialla, T.J.; et al. L-Citrulline increases nitric oxide and improves control in obese asthmatics. JCI Insight 2019, 4, e131733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreslová, M.; Sýkorová, A.; Bittenglová, R.; Schwarz, J.; Pomahačová, R.; Jehlička, P.; Kobr, J.; Trefil, L.; Sýkora, J. Age-Related Progression of Microvascular Dysfunction in Cystic Fibrosis: New Detection Ways and Clinical Outcomes. Physiol. Res. 2021, 70, 893–903. [Google Scholar] [CrossRef]
- Hamzaoui, A.; Ammar, J.; El Mekki, F.; Borgi, O.; Ghrairi, H.; Ben Brahim, M.; Hamzaoui, K. Elevation of Serum Soluble E-Selectin and VCAM-1 in Severe Asthma. Mediat. Inflamm. 2001, 10, 339–342. [Google Scholar] [CrossRef] [Green Version]
- Kadakal, F.; Aras, G.; Kanmaz, D.; Purisa, S.; Uzumcu, M.; Iatk, E.; Bratfalean, D. The assessment of high sensitivity C-reactive protein as a systemic marker in moderate asthma patients and changing levels by inhaled corticosteroids. JPMA J. Pak. Med. Assoc. 2013, 63, 893–898. [Google Scholar]
- Morrison, K.M.; Dyal, L.; Conner, W.; Helden, E.; Newkirk, L.; Yusuf, S.; Lonn, E. Cardiovascular Risk Factors and Non-Invasive Assessment of Subclinical Atherosclerosis in Youth. Atherosclerosis 2010, 208, 501–505. [Google Scholar] [CrossRef]
- Karthikeyan, R.; Krishnamoorthy, S.; Maamidi, S.; Kaza, A.M.; Balasubramanian, N. Effect of inhaled corticosteroids on systemic inflammation in asthma. Perspect. Clin. Res. 2014, 5, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Atsuta, J.; Plitt, J.; Bochner, B.S.; Schleimer, R.P. Inhibition of VCAM-1 expression in human bronchial epithelial cells by glucocorticoids. Am. J. Respir. Cell Mol. Biol. 1999, 20, 643–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masopustová, A.; Kreslová, M.; Sýkora, J.; Jehlička, P.; Trefil, L.; Kobr, J. Endothelial dysfunction in Children and Young Adults: A combined Diagnostic Approach of Plethysmographic and Biochemical Markers. In Advances in Health and Disease, 1st ed.; Duncan, L.T., Ed.; Nova Science Publishers: New York, NY, USA, 2018; Volume 6, pp. 189–202. [Google Scholar]
- Jehlička, P.; Huml, M.; Schwarz, J.; Trefil, L.; Kobr, J.; Sýkora, J. Reactive Hyperaemia Index as a Marker of Endothelial Dysfunction in Children with Crohn’s Disease Is Significantly Lower than Healthy Controls. Acta Paediatr. 2014, 103, e55–e60. [Google Scholar] [CrossRef]
- Masopustová, A.; Jehlička, P.; Huml, M.; Votava, T.; Trefil, L.; Kreslová, M.; Sýkora, J. Plethysmographic and Biochemical Markers in the Diagnosis of Endothelial Dysfunction in Pediatric Acute Lymphoblastic Leukemia Survivors—New Applications. Physiol. Res. 2018, 67, 903–909. [Google Scholar] [CrossRef]
- Hoshino, M.; Takahashi, M.; Takai, Y.; Sim, J.; Aoike, N. Inhaled Corticosteroids Decrease Vascularity of the Bronchial Mucosa in Patients with Asthma. Clin. Exp. Allergy 2001, 31, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Liu, C.-T.; Wu, Y.-H.; Feng, Y.-L.; Bai, H. Budesonide/Formoterol Decreases Expression of Vascular Endothelial Growth Factor (VEGF) and VEGF Receptor 1 within Airway Remodelling in Asthma. Adv. Ther. 2008, 25, 342–354. [Google Scholar] [CrossRef]
- Li, J.; Panganiban, R.; Kho, A.T.; McGeachie, M.J.; Farnam, L.; Chase, R.P.; Weiss, S.T.; Lu, Q.; Tantisira, K.G. Circulating MicroRNAs and Treatment Response in Childhood Asthma. Am. J. Respir. Cell Mol. Biol. 2020, 202, 65–72. [Google Scholar] [CrossRef]
- Wei, B.; Dang, Y.H.; Liu, X.P.; Li, M. Protective effect of inhaled corticosteroid on children with asthma with Mycoplasma pneumoniae pneumonia. Front. Pediatr. 2022, 10, 908857. [Google Scholar] [CrossRef]
- Glassberg, J.; Minnitti, C.; Cromwell, C.; Cytryn, L.; Kraus, T.; Skloot, G.S.; Connor, J.T.; Rahman, A.H.; Meurer, W.J. Inhaled steroids reduce pain and sVCAM levels in individuals with sickle cell disease: A triple-blind, randomized trial. Am. J. Hematol. 2017, 92, 622–631. [Google Scholar] [CrossRef] [Green Version]
- Wanner, A.; Mendes, E.S. Airway Endothelial Dysfunction in Asthma and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2010, 182, 1344–1351. [Google Scholar] [CrossRef]
- Hoxha, M.; Tedesco, C.C.; Quaglin, S.; Malaj, V.; Pustina, L.; Capra, V.; Evans, J.F.; Sala, A.; Rovati, G.E. Montelukast Use Decreases Cardiovascular Events in Asthmatics. Front. Pharmacol. 2021, 11, 611561. [Google Scholar] [CrossRef] [PubMed]
- Yeryomenko, G.; Bezditko, T.; Dubuske, L. Endothelial Dysfunction in Patients Having Asthma with Diabetes Mellitus Type 2 and Obesity. J. Allergy Clin. Immunol. 2020, 145, AB73. [Google Scholar] [CrossRef]
- Lee, H.M.; Liu, M.A.; Barrett-Connor, E.; Wong, N.D. Association of Lung Function with Coronary Heart Disease and Cardiovascular Disease Outcomes in Elderly: The Rancho Bernardo Study. Respir. Med. 2014, 108, 1779–1785. [Google Scholar] [CrossRef] [Green Version]
- Kato, G.; Takahashi, K.; Izuhara, K.; Komiya, K.; Kimura, S.; Hayashi, S. Markers that can Reflect Asthmatic Activity before and after Reduction of Inhaled Corticosteroids: A Pilot Study. Biomark. Insights 2013, 8, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fricker, M.; Heaney, L.G.; Upham, J.W. Can biomarkers help us hit targets in difficult-to-treat asthma? Respirology 2017, 22, 430–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, M.-L.; Li, L.; Diao, L.-L. Bronchial Asthma and Risk of 4 Specific Cardiovascular Diseases and Cardiovascular Mortality: A Meta-Analysis of Cohort Studies. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 5081–5091. [Google Scholar] [CrossRef]
- Keselman, A.; Heller, N. Estrogen Signaling Modulates Allergic Inflammation and Contributes to Sex Differences in Asthma. Front. Immunol. 2015, 6, 568. [Google Scholar] [CrossRef] [Green Version]
- Çelebi Sözener, Z.; Aydın, Ö.; Mungan, D.; Mısırlıgil, Z. Obesity-Asthma Phenotype: Effect of Weight Gain on Asthma Control in Adults. Allergy Asthma Proc. 2016, 37, 311–317. [Google Scholar] [CrossRef]
- Bel, E.H.; Sousa, A.; Fleming, L.; Bush, A.; Chung, K.F.; Versnel, J.; Wagener, A.H.; Wagers, S.S.; Sterk, P.J.; Compton, C.H. Diagnosis and Definition of Severe Refractory Asthma: An International Consensus Statement from the Innovative Medicine Initiative (IMI). Thorax 2010, 66, 910–917. [Google Scholar] [CrossRef] [Green Version]
- Salonen, I.; Huttunen, K.; Hirvonen, M.-R.; Dufva, J.; Groundstroem, K.; Dufva, H.; Salonen, R.O. Exhaled Nitric Oxide and Atherosclerosis. Eur. J. Clin. Investig. 2012, 42, 873–880. [Google Scholar] [CrossRef]
- Shoda, T.; Futamura, K.; Orihara, K.; Emi-Sugie, M.; Saito, H.; Matsumoto, K.; Matsuda, A. Recent Advances in Understanding the Roles of Vascular Endothelial Cells in Allergic Inflammation. Allergol. Int. 2016, 65, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Ghiro, L.; Zanconato, S.; Rampon, O.; Piovan, V.; Pasquale, M.F.; Baraldi, E. Effect of montelukast added to inhaled corticosteroids on fractional exhaled nitric oxide in asthmatic children. Eur. Respir. J. 2002, 20, 630–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, S.S.; Liu, H.; Gao, X. Elevated fractional exhaled nitric oxide (FeNO) is a clinical indicator of uncontrolled asthma in children receiving inhaled corticosteroids. Int. J. Clin. Pharmacol. Ther. 2017, 55, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Syk, J.; Malinovschi, A.; Borres, M.P.; Undén, A.L.; Andreasson, A.; Lekander, M.; Alving, K. Parallel reductions of IgE and exhaled nitric oxide after optimized anti-inflammatory asthma treatment. Immun. Inflamm. Dis. 2016, 4, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Rossi, B.; Constantin, G. Anti-selectin therapy for the treatment of inflammatory diseases. Inflamm. Allergy Drug Targets 2008, 7, 85–93. [Google Scholar] [CrossRef]
- Wolkerstorfer, A.; Savelkoul, H.F.; de Waard van der Spek, F.B.; Neijens, H.J.; van Meurs, T.; Oranje, A.P. Soluble E-selectin and soluble ICAM-1 levels as markers of the activity of atopic dermatitis in children. Pediatr. Allergy Immunol. 2003, 14, 302–306. [Google Scholar] [CrossRef]
- Jahnova, E.; Horvathova, M.; Gazdik, F.; Weissova, S. Effects of selenium supplementation on expression of adhesion molecules in corticoid-dependent asthmatics. Bratisl. Lek. Listy 2002, 103, 12–16. [Google Scholar]
- Matera, M.G.; Page, C.P.; Calzetta, L.; Rogliani, P.; Cazzola, M. Pharmacology and Therapeutics of Bronchodilators Revisited. Pharmacol. Rev. 2020, 72, 218–252. [Google Scholar] [CrossRef]
- Page, C.P.; Cotter, T.; Kilfeather, S.; Sullivan, P.; Spina, D.; Costello, J.F. Effect of chronic theophylline treatment on the methacholine dose-response curve in allergic asthmatic subjects. Eur. Respir. J. 1998, 12, 24–29. [Google Scholar] [CrossRef] [Green Version]
- Campisi, R.; Crimi, C.; Intravaia, R.; Strano, S.; Noto, A.; Foschino, M.P.; Valenti, G.; Viviano, V.; Pelaia, C.; Ricciardi, L.; et al. Adherence to omalizumab: A multicenter “real-world” study. World Allergy Organ. J. 2020, 13, 100103. [Google Scholar] [CrossRef]
- Crimi, C.; Campisi, R.; Nolasco, S.; Cacopardo, G.; Intravaia, R.; Porto, M.; Impellizzeri, P.; Pelaia, C.; Crimi, N. Mepolizumab effectiveness in patients with severe eosinophilic asthma and co-presence of bronchiectasis: A real-world retrospective pilot study. Respir. Med. 2021, 185, 106491. [Google Scholar] [CrossRef] [PubMed]
- Pasha, M.A.; Jourd’heuil, D.; Jourd’heuil, F.; Mahon, L.; Romero, F.; Feustel, P.J.; Evans, M.; Smith, T.; Mitchell, J.; Gendapodi, P.; et al. The effect of omalizumab on small airway inflammation as measured by exhaled nitric oxide in moderate-to-severe asthmatic patients. Allergy Asthma Proc. 2014, 35, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Tajiri, T.; Niimi, A.; Matsumoto, H.; Ito, I.; Oguma, T.; Otsuka, K.; Takeda, T.; Nakaji, H.; Inoue, H.; Iwata, T.; et al. Comprehensive efficacy of omalizumab for severe refractory asthma: A time-series observational study. Ann. Allergy Asthma Immunol. 2014, 113, 470–475.e2. [Google Scholar] [CrossRef] [PubMed]
- Bakakos, A.; Schleich, F.; Bakakos, P. Biological Therapy of Severe Asthma and Nasal Polyps. J. Personal. Med. 2022, 12, 976. [Google Scholar] [CrossRef] [PubMed]
- Kirchnerová, O.R.; Valena, T.; Novosad, J.; Teřl, M.; Czech eXpeRience Study Group. Real-world effectiveness and safety of omalizumab in patients with uncontrolled severe allergic asthma from the Czech Republic. Postepy Dermatol. Alergol. 2019, 36, 34–43. [Google Scholar] [CrossRef] [Green Version]
- Parulekar, A.D.; Diamant, Z.; Hanania, N.A. Role of biologics targeting type 2 airway inflammation in asthma: What have we learned so far? Curr. Opin. Pulm. Med. 2017, 23, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Quaranta, V.N.; Dragonieri, S.; Crimi, N.; Crimi, C.; Santus, P.; Menzella, F.; Pelaia, C.; Scioscia, G.; Caruso, C.; Bargagli, E.; et al. Can Leukotriene Receptor Antagonist Therapy Improve the Control of Patients with Severe Asthma on Biological Therapy and Coexisting Bronchiectasis? A Pilot Study. J. Clin. Med. 2022, 11, 4702. [Google Scholar] [CrossRef]
- Ishibashi, T.; Kawamoto, K.; Matsuno, K.; Ishihara, G.; Baba, T.; Komori, N. Peripheral Endothelial Function Can Be Improved by Daily Consumption of Water Containing over 7 Ppm of Dissolved Hydrogen: A Randomized Controlled Trial. PLoS ONE 2020, 15, e0233484. [Google Scholar] [CrossRef]
- Selamet Tierney, E.S.; Newburger, J.W.; Gauvreau, K.; Geva, J.; Coogan, E.; Colan, S.D.; de Ferranti, S.D. Endothelial Pulse Amplitude Testing: Feasibility and Reproducibility in Adolescents. J. Pediatr. 2009, 154, 901–905. [Google Scholar] [CrossRef]
- Kelly, A.S.; Marlatt, K.L.; Steinberger, J.; Dengel, D.R. Younger Age Is Associated with Lower Reactive Hyperemic Index but Not Lower Flow-Mediated Dilation among Children and Adolescents. Atherosclerosis 2014, 234, 410–414. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Data | Asthma Group Median (min; max) | Comparison Group Median (min; max) | Statistical Significance |
|---|---|---|---|
| Number | 52 | 45 | |
| Gender (male/female) | 22/30 | 18/27 | Equivalency (±20) |
| Age (y) | 25.22 (13.97; 49.85) | 17.04 (11.79; 28.32) | p < 0.005 |
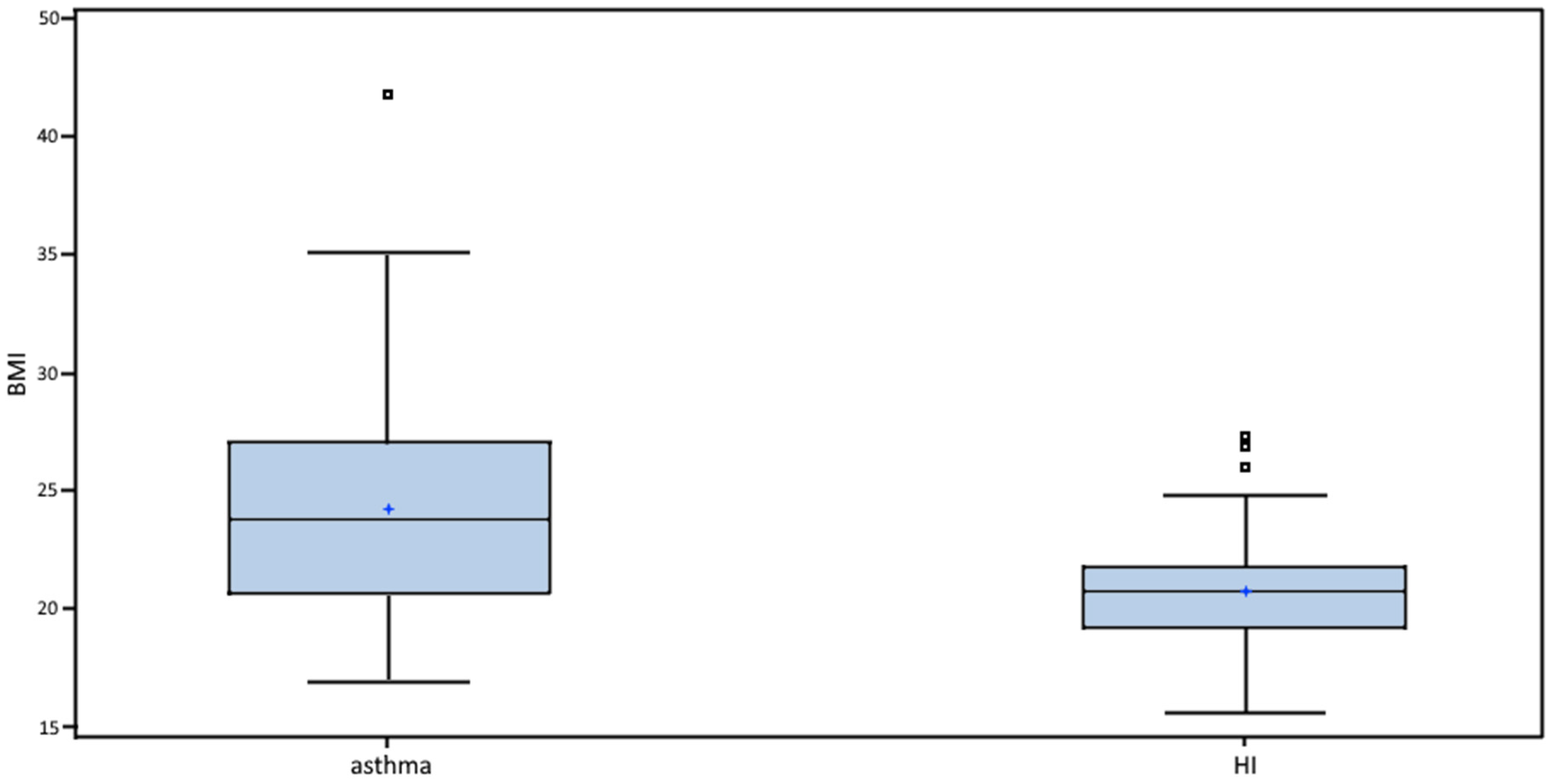
| BMI (kg/m2) | 23.77 (16.96; 41.87) | 20.73 (15.56; 27.31) | p < 0.001 |
| Systolic blood pressure (mm Hg) | 119 (98; 150) | 116 (90; 136) | NS |
| Diastolic blood pressure (mm Hg) | 74.5 (56; 95) | 70 (50; 88) | p < 0.005 |
| Data | Number | % |
|---|---|---|
| Asthma type | ||
| Allergic: persistent mild | 28 | 53.85 |
| Allergic: persistent moderate | 8 | 15.38 |
| Allergic: persistent severe and severe refractory | 10 | 19.23 |
| Exercise-induced | 6 | 11.54 |
| FENO (ppb) | ||
| Normal (<25) | 31 | 59.62 |
| Mid-range (25–50) | 10 | 19.23 |
| Positive (>50) | 11 | 21.15 |
| Spirometry: peripheral airway obstruction | ||
| Normal (FEF25–50 > 66%) | 33 | 63.46 |
| Mild (FEF25–50 55–66%) | 9 | 17.31 |
| Moderate (FEF25–50 45–54%) | 4 | 7.69 |
| Severe and very severe (FEF25–50 < 45%) | 6 | 11.54 |
| Asthma control test (score 5–25) | ||
| Full-controlled asthma (score 25) | 24 | 46.15 |
| Well-controlled asthma (score 20–24) | 12 | 23.08 |
| Poor control of asthma (score < 20) | 16 | 30.77 |
| Asthma Severity | |||||
|---|---|---|---|---|---|
| Type of Treatment | Mild | Moderate | Severe | Exercise Induced | Total |
| LTRA | 4 | 0 | 0 | 0 | 4 |
| LTRA + antiHIS | 3 | 0 | 0 | 0 | 3 |
| ICS | 3 | 1 | 0 | 1 | 5 |
| ICS + LTRA | 2 | 0 | 0 | 0 | 2 |
| ICS + antiHIS | 2 | 0 | 0 | 0 | 2 |
| ICS + antiHIS + LTRA | 3 | 0 | 0 | 0 | 3 |
| ICS + LABA | 2 | 2 | 0 | 2 | 6 |
| ICS + LABA + LTRA | 0 | 0 | 1 | 0 | 1 |
| ICS + LABA + antiHIS | 5 | 3 | 0 | 3 | 11 |
| ICS + LABA + antiHIS + LTRA | 4 | 2 | 0 | 0 | 6 |
| ICS + LABA + LTRA + antiHIS + OMA | 0 | 0 | 2 | 0 | 2 |
| ICS + LABA + LAMA + LTRA + OMA | 0 | 0 | 1 | 0 | 1 |
| ICS + LABA + OCS + OMA | 0 | 0 | 1 | 0 | 1 |
| ICS + LABA + LAMA + antiHIS + OCS + OMA | 0 | 0 | 1 | 0 | 1 |
| ICS + LABA + LAMA + LTRA + antiHIS + OCS + OMA | 0 | 0 | 1 | 0 | 1 |
| ICS + LABA + LAMA + LTRA + antiHIS + TPH + OMA | 0 | 0 | 1 | 0 | 1 |
| ICS + LABA + LAMA + antiHIS + TPH + OCS + OMA | 0 | 0 | 2 | 0 | 2 |
| Marker | Asthma Type | Positive Patients | Average (min; max) | |
|---|---|---|---|---|
| Count | % of all Positive | |||
| Total IgE (positive >100 kIU/L) | Mild | 15 | 47 | 421.5 (108.0; 1770.0) |
| Moderate | 7 | 22 | 705.5 (159.0; 2340.0) | |
| Severe | 9 | 28 | 755.3 (178.0; 1060.0) | |
| Exercise-induced | 1 | 3 | 110.0 | |
| Allergen-specific IgE (positive >0.35 U/mL) | Mild | 25 | 54 | |
| Moderate | 6 | 13 | ||
| Severe | 10 | 22 | ||
| Exercise-induced | 5 | 11 | ||
| ECP (positive >24 µg/L) | Mild | 14 | 50 | 23.8 (24.0; 83.60) |
| Moderate | 3 | 11 | 97.2 (31.9; 200.0) | |
| Severe | 9 | 32 | 78.0 (34.1; 200.0) | |
| Exercise-induced | 2 | 7 | 55.9 (52.80; 59.0) | |
| Blood Absolute Eosinophil Count (positive ≥0.3 × 10⁹/L) | Mild | 11 | 50 | 0.46 (0.30; 1.00) |
| Moderate | 5 | 23 | 0.52 (0.30; 1.20) | |
| Severe | 5 | 23 | 0.68 (0.30; 1.30) | |
| Exercise-induced | 1 | 4 | 0.30 | |
| Data | Asthma Group Median (min; max) | Comparison Group Median (min; max) | Statistical Significance |
|---|---|---|---|
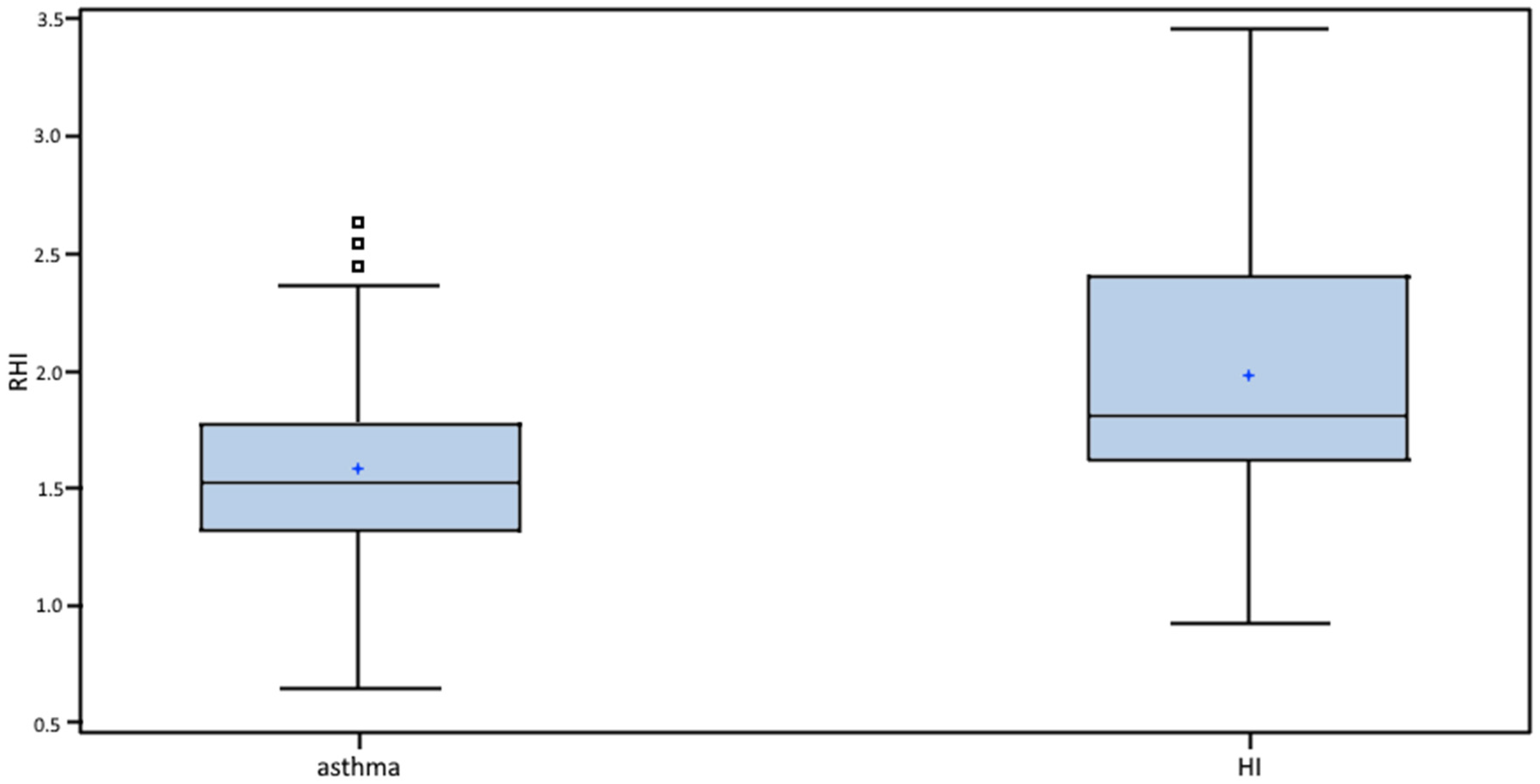
| RHI | 1.53 (0.65; 2.64) | 1.81 (0.93; 3.46) | p < 0.001 |
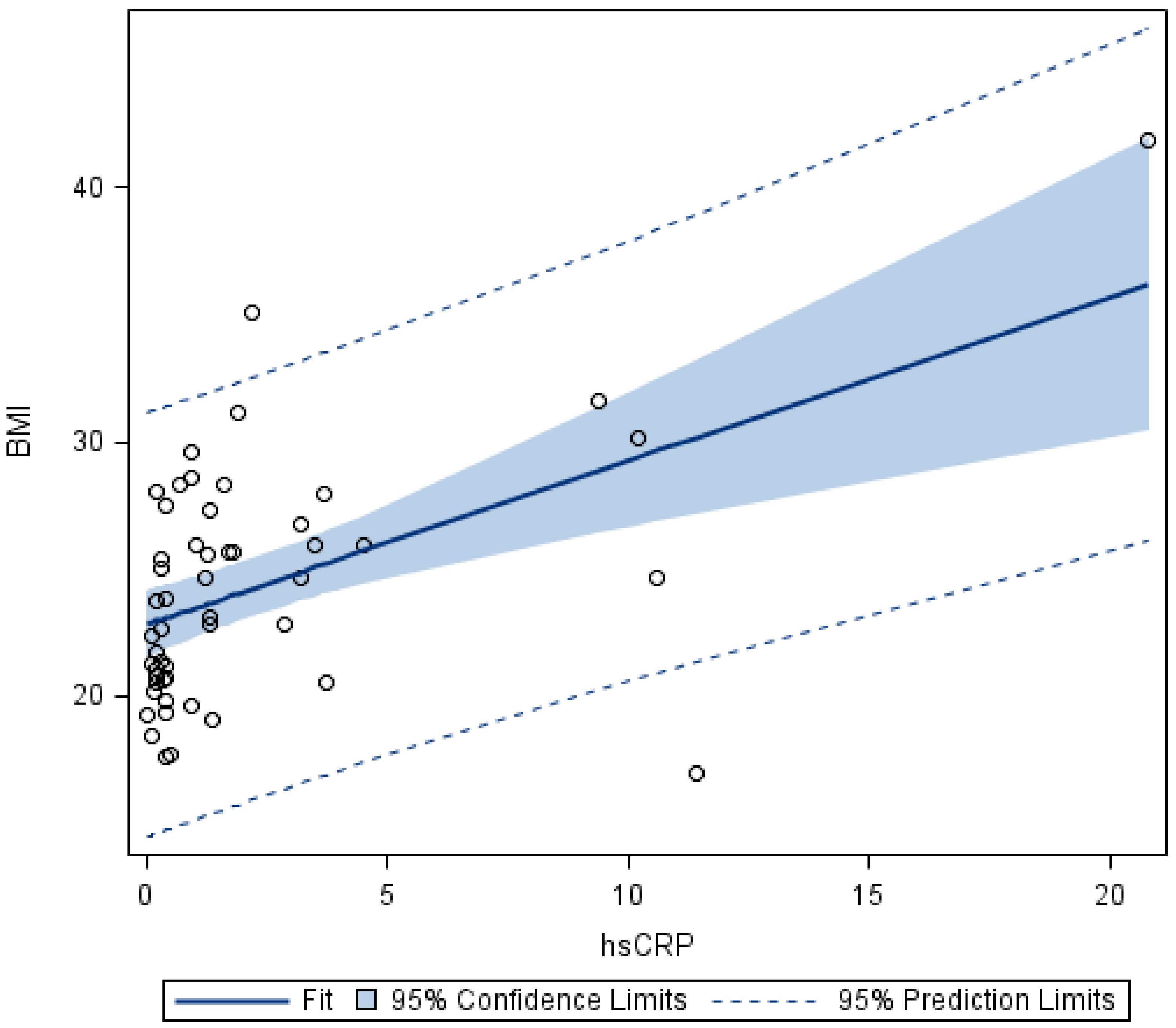
| hsCRP (mg/L) | 0.90 (0.02; 20.80) | 0.25 (0.02; 1.64) | p < 0.001 |
| VCAM-1 (μg/L) | 758.10 (403.1; 1414.9) | 942.15 (555.5; 1518.4) | p < 0.01 |
| E-selectin (μg/L) | 53.00 (10.10; 141.80) | 53.20 (18.70; 145.80) | NS |
| ADMA (μmol/L) | 0.44 (0.25; 0.83) | 0.54 (0.31; 0.89) | p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kreslová, M.; Kirchnerová, O.; Rajdl, D.; Sudová, V.; Blažek, J.; Sýkorová, A.; Jehlička, P.; Trefil, L.; Schwarz, J.; Pomahačová, R.; et al. Bronchial Asthma as a Cardiovascular Risk Factor: A Prospective Observational Study. Biomedicines 2022, 10, 2614. https://doi.org/10.3390/biomedicines10102614
Kreslová M, Kirchnerová O, Rajdl D, Sudová V, Blažek J, Sýkorová A, Jehlička P, Trefil L, Schwarz J, Pomahačová R, et al. Bronchial Asthma as a Cardiovascular Risk Factor: A Prospective Observational Study. Biomedicines. 2022; 10(10):2614. https://doi.org/10.3390/biomedicines10102614
Chicago/Turabian StyleKreslová, Marcela, Olga Kirchnerová, Daniel Rajdl, Vendula Sudová, Jiří Blažek, Aneta Sýkorová, Petr Jehlička, Ladislav Trefil, Jan Schwarz, Renata Pomahačová, and et al. 2022. "Bronchial Asthma as a Cardiovascular Risk Factor: A Prospective Observational Study" Biomedicines 10, no. 10: 2614. https://doi.org/10.3390/biomedicines10102614