
Signal and Texture Features from T2 Maps for the Prediction of Mild Cognitive Impairment to Alzheimer’s Disease Progression

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Subject Inclusion
2.3. MRI Processing
2.4. Feature Extraction
2.5. Statistical Analysis
2.6. Experiment Design
3. Results
3.1. Univariate Analysis for Neuropsychological Studies and Volumes
3.2. Univariate Analysis for Signal and Texture Features
3.3. Multivariate Analysis for Neuropsychological Studies
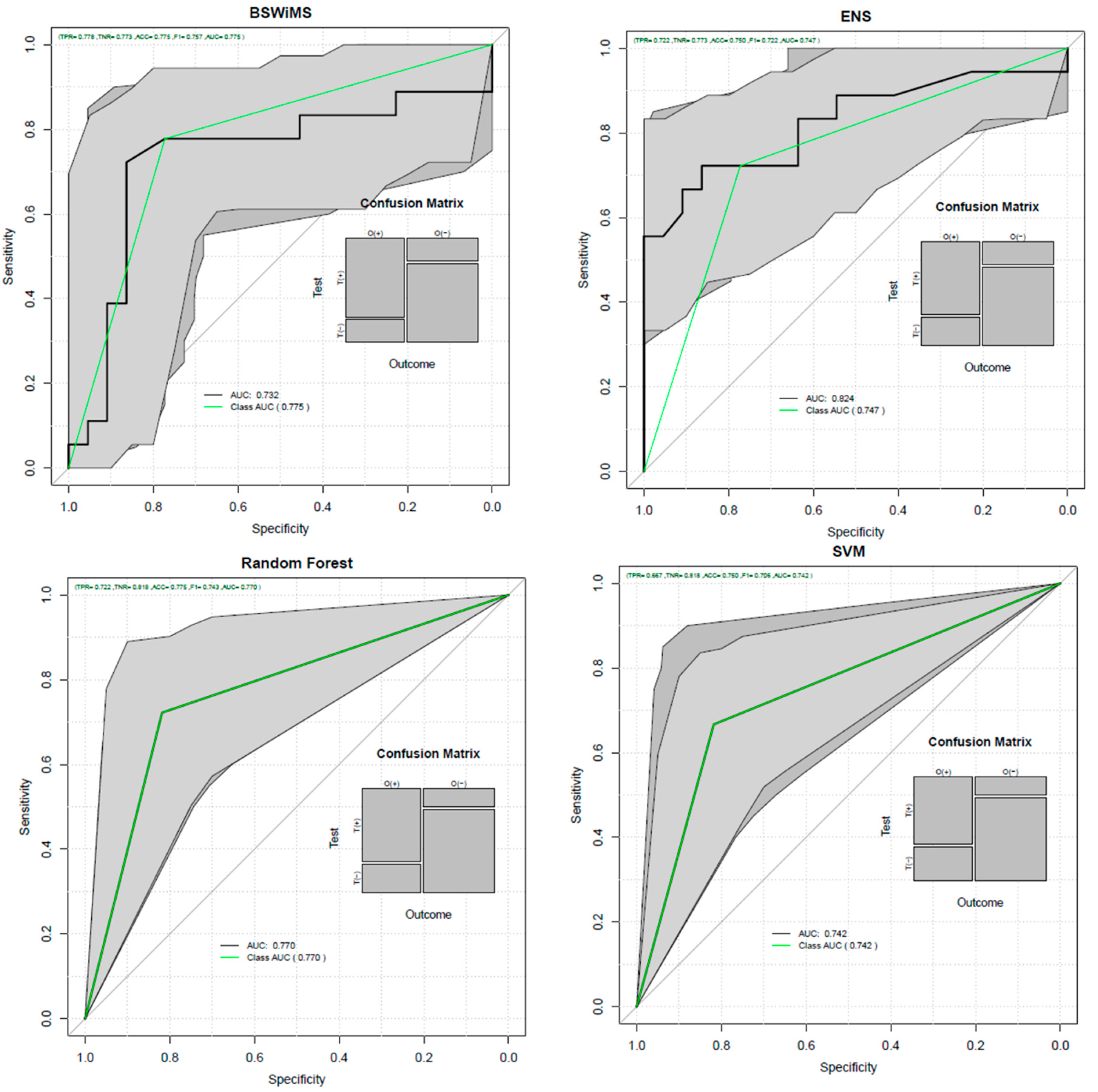
3.4. Multivariate Analysis for Neuropsychological Studies and Imaging Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erkkinen, M.G.; Kim, M.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2018, 10, a033118. [Google Scholar] [CrossRef] [Green Version]
- Blennow, K.; Mattsson, N.; Schöll, M.; Hansson, O.; Zetterberg, H. Amyloid biomarkers in Alzheimer’s disease. Trends Pharmacol. Sci. 2015, 36, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Zvěřová, M. Clinical aspects of Alzheimer’s disease. Clin. Biochem. 2019, 72, 3–6. [Google Scholar] [CrossRef]
- Stelzmann, R.A.; Schnitzlein, H.N.; Murtagh, F.R. An english translation of alzheimer’s 1907 paper, ‘über eine eigenartige erkankung der hirnrinde. Clin. Anat. 1995, 8, 429–431. [Google Scholar] [CrossRef]
- Sosa-Ortiz, A.L.; Acosta-Castillo, I.; Prince, M.J. Epidemiology of Dementias and Alzheimer’s Disease. Arch. Med. Res. 2012, 43, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Association. 2019 Alzheimer’s disease facts and figures. Alzheimers Dement. 2019, 15, 321–387. [Google Scholar]
- Cadena-Hernandez, A.G.; Trejo-Castro, A.I.; Celaya-Padilla, J.M.; Tamez-Pena, J.; Martinez-Torteya, A. Longitudinal gender-specific differences in the conversion from mild cognitive impairment to Alzheimer’s disease. In Proceedings of the 2018 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Las Vegas, NV, USA, 4–7 March 2018; pp. 202–205. [Google Scholar]
- Martinez-Torteya, A.; Trejo-Castro, A.I.; Celaya-Padill, J.M.; Tamez-Pena, J.G. Differences in the Progression from Mild Cognitive Impairment to Alzheimer’s Disease between APOE4 Carriers and Non-Carriers. In Proceedings of the 2019 IEEE 19th International Conference on Bioinformatics and Bioengineering (BIBE), Athens, Greece, 28–30 October 2019; pp. 199–203. [Google Scholar]
- Tangalos, E.G.; Petersen, R.C. Mild Cognitive Impairment in Geriatrics. Clin. Geriatr. Med. 2018, 34, 563–589. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild Cognitive Impairment. N. Engl. J. Med. 2011, 364, 2227–2234. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group* under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939. [Google Scholar] [CrossRef] [Green Version]
- Folstein, F.M.; Folstein, S.E.; McHugh, P.R. Mini-mental state. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Kaplan, E.; Goodglass, H.; Weintrab, S. The Boston Naming Test; Lea & Febiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Rosen, W.G.; Mohs, R.C.; Davis, K.L. A new rating scale for Alzheimer’s disease. Am. J. Psychiatry 1984, 141, 1356–1364. [Google Scholar] [PubMed]
- Jack, C.R., Jr.; Albert, M.S.; Knopman, D.S.; McKhann, G.M.; Sperling, R.A.; Carrillo, M.C.; Thies, B.; Phelps, C.H. Introduction to the recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 257–262. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.H.; He, Y.; Zhong, X.L.; Lei, H.; Wang, F.; Luo, G.H.; Zhao, H.; Liu, J.C. MMagnetic Resonance Texture Analysis in Alzheimer’s disease. Acad. Radiol. 2020, in press. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wachinger, C.; Salat, D.H.; Weiner, M.; Reuter, M. Whole-brain analysis reveals increased neuroanatomical asymmetries in dementia for hippocampus and amygdala. Brain 2016, 139, 3253–3266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Torteya, A.; Rodriguez-Rojas, J.; Celaya-Padilla, J.M.; Galván-Tejada, J.I.; Treviño, V.; Tamez-Peña, J. Magnetization-prepared rapid acquisition with gradient echo magnetic resonance imaging signal and texture features for the prediction of mild cognitive impairment to Alzheimer’s disease progression. J. Med. Imaging 2014, 1, 031005. [Google Scholar] [CrossRef] [Green Version]
- Trejo-Castro, A.I. Texture and signal features from hippocampal T2 maps as biomarkers for MCI to AD progression. In Proceedings of the 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Seoul, South Korea, 16–19 December 2020; pp. 772–777. [Google Scholar]
- Yu, H.; Touret, A.S.; Li, B.; O’Brien, M.; Qureshi, M.M.; Soto, J.A.; Jara, H.; Anderson, S.W. Application of texture analysis on parametric T 1 and T 2 maps for detection of hepatic fibrosis. J. Magn. Reson. Imaging 2017, 45, 250–259. [Google Scholar] [CrossRef]
- Baessler, B.; Luecke, C.; Lurz, J.; Klingel, K.; Das, A.; von Roeder, M.; de Waha-Thiele, S.; Besler, C.; Rommel, K.P.; Maintz, D.; et al. Cardiac MRI and Texture Analysis of Myocardial T1 and T2 Maps in Myocarditis with Acute versus Chronic Symptoms of Heart Failure. Radiology 2019, 292, 608–617. [Google Scholar] [CrossRef]
- Jack, C.R.; Bernstein, M.A.; Borowski, B.J.; Gunter, J.L.; Fox, N.C.; Thompson, P.M.; Schuff, N.; Krueger, G.; Killiany, R.J.; Decarli, C.S.; et al. Update on the Magnetic Resonance Imaging core of the Alzheimer’s Disease Neuroimaging Initiative. Alzheimers Dement. 2010, 6, 212–220. [Google Scholar] [CrossRef] [Green Version]
- Heckemann, R.A.; Keihaninejad, S.; Aljabar, P.; Rueckert, D.; Hajnal, J.V.; Hammers, A. Improving intersubject image registration using tissue-class information benefits robustness and accuracy of multi-atlas based anatomical segmentation. Neuroimage 2010, 51, 221–227. [Google Scholar] [CrossRef]
- Petersen, R.C.; Aisen, P.S.; Beckett, L.A.; Donohue, M.C.; Gamst, A.C.; Harvey, D.J.; Jack, C.R., Jr.; Jagust, W.J.; Shaw, L.M.; Toga, A.W.; et al. Alzheimer’s Disease Neuroimaging Initiative (ADNI): Clinical characterization. Neurology 2010, 74, 201–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milford, D.; Rosbach, N.; Bendszus, M.; Heiland, S. Mono-exponential fitting in T2-relaxometry: Relevance of offset and first echo. PLoS ONE 2015, 10, e0145255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, H.J.; McCormick, M.M.; Ibanez, L. The Insight Software Consortium. In The ITK Software Guide, 4th ed.; Kitware, Inc.: Chapelhill, NC, USA, 2015. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Martinez-Torteya, A.; Alanis, I.; Tamez-Pena, J. FeatuRE Selection Algortihms for Computer-Aided Diagnosis: An R package. The Comprehensive R Archive Network. 2018. Available online: https://cran.r-project.org/web/packages/FRESA.CAD/index.html (assessed on 21 July 2021).
- Oriol, J.D.; Martinez-Torteya, A.; Trevino, V.; Alanis, I.; Vallejo, E.; Tamez-Pena, J.G. Benchmarking machine learning models for the analysis of genetic data using FRESA.CAD Binary Classification Benchmarking. bioRxiv 2019. preprint. [Google Scholar]
- Oriol, J.D.; Vallejo, E.E.; Estrada, K.; Peña, J.G.T. The Alzheimer’s Disease Neuroimaging Initiative Benchmarking machine learning models for late-onset alzheimer’s disease prediction from genomic data. BMC Bioinform. 2019, 20, 709. [Google Scholar]
- Aisen, P.S.; Petersen, R.C.; Donohue, M.C.; Gamst, A.; Raman, R.; Thomas, R.G.; Walter, S.; Trojanowski, J.Q.; Shaw, L.M.; Beckett, L.A.; et al. Clinical core of the Alzheimer’s disease neuroimaging initiative: Progress and plans. Alzheimers Dement. 2010, 6, 239–246. [Google Scholar] [CrossRef] [Green Version]
- Crane, P.K.; Carle, A.; Gibbons, L.E.; Insel, P.; Mackin, R.S.; Gross, A.; Jones, R.N.; Mukherjee, S.; Curtis, S.M.; Harvey, D.; et al. Development and assessment of a composite score for memory in the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Brain Imaging Behav. 2012, 6, 502–516. [Google Scholar] [CrossRef] [Green Version]
- Gibbons, L.; Carle, A.; Mackin, R.; Harvey, D. A composite score for executive functioning, validated in Alzheimer’s Disease Neuroimaging Initiative (ADNI) participants with baseline mild cognitive impairment. Brain Imaging Behav. 2012, 6, 517–527. [Google Scholar] [CrossRef] [Green Version]
- Jack, C.R., Jr.; Petersen, R.C.; Xu, Y.C.; O’Brien, P.C.; Smith, G.E.; Ivnik, R.J.; Boeve, B.F.; Waring, S.C.; Tangalos, E.G.; Kokmen, E. Prediction of AD with MRI-based hippocampal volume in mild cognitive impairment. Neurology 1999, 52, 1397. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lee, H.W.; Kim, K. Magnetic resonance imaging texture predicts progression to dementia due to Alzheimer disease earlier than hippocampal volume. J. Psychiatry Neurosci. 2020, 45, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, L.; Aisen, P.S.; Petersen, R.C.; Donohue, M.C.; Gamst, A.; Raman, R.; Thomas, R.G.; Walter, S.; Trojanowski, J.Q.; Shaw, L.M.; et al. Early detection of Alzheimer’s disease using MRI hippocampal texture. Hum. Brain Mapp. 2016, 37, 1148–1161. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Leger, S.; Vallières, M.; Löck, S. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Group of Study | Total | MCIs | MCIp | p-Value |
|---|---|---|---|---|
| Subjects (males) | 40 (32) | 22 (18) | 18 (14) | 1.000 |
| Years of age | 75.3 ± 3.0 | 75.3 ± 3.2 | 75.2 ± 2.9 | 0.924 |
| Years of education | 15.7 ± 3.0 | 15.8 ± 3.1 | 15.6 ± 2.9 | 0.879 |
| Rank | Feature | Modality | Brain Region | p-Value |
|---|---|---|---|---|
| 1 | Value at 25% a | Difference | Superior frontal gyrus | 1.52 × 10−4 |
| 2 | Mass Scatter YY b | Difference | Hippocampus | 5.51 × 10−4 |
| 3 | σ at 90% central value a | Mean | Hippocampus | 0.001 |
| 4 | ICV at 90% central value a | Mean | Hippocampus | 0.002 |
| 5 | Probability of value being lower than 2σ a | Difference | Lateral ventricle, temporal horn | 0.002 |
| 6 | Entropy a | Mean | Hippocampus | 0.002 |
| 7 | Energy a | Mean | Hippocampus | 0.002 |
| 8 | Value at 75% a | Mean | Hippocampus | 0.003 |
| 9 | Skewness a | Mean | Subcallosal area | 0.004 |
| 10 | Energy a | Mean | Subcallosal area | 0.004 |
| 11 | Mass Scatter YY b | Difference | Cerebellum | 0.004 |
| 12 | Value at 5% a | Difference | Superior frontal gyrus | 0.004 |
| 13 | µ signal a | Mean | Hippocampus | 0.004 |
| 14 | µ at 90% central value a | Mean | Hippocampus | 0.005 |
| 15 | Entropy a | Mean | Subcallosal area | 0.005 |
| 16 | Value at 95% a | Mean | Hippocampus | 0.006 |
| 17 | Kurtosis a | Mean | Hippocampus | 0.006 |
| 18 | Precision range a | Mean | Hippocampus | 0.006 |
| 19 | Precision range a | Mean | Insula | 0.006 |
| 20 | Value at 99.99% a | Difference | Anterior orbital gyrus | 0.007 |
| 21 | ICV at 90% central value a | Mean | Lateral occipitotemporal gyrus, gyrus fusiformis | 0.008 |
| 22 | Probability of value being greater than 3σ a | Mean | Cingulate gyrus, posterior part | 0.008 |
| 23 | Energy a | Mean | Cingulate gyrus, posterior part | 0.008 |
| 24 | Value at 25% a | Difference | Putamen | 0.008 |
| 25 | Probability of value being greater than 3σ a | Difference | Lateral ventricles, temporal horn | 0.008 |
| Accuracy | ROC AUC | Specificity | Sensitivity | Balanced Error | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Technique | Mean | CI | Mean | CI | Mean | CI | Mean | CI | Mean | CI |
| BSWIMS | 0.500 | 0.338–0.662 | 0.558 | 0.380–0.736 | 0.273 | 0.107–0.502 | 0.778 | 0.524–0.936 | 0.475 | 0.341–0.613 |
| ENS | 0.650 | 0.483–0.794 | 0.649 | 0.472–0.826 | 0.636 | 0.407–0.828 | 0.667 | 0.410–0.867 | 0.347 | 0.198–0.513 |
| KNN | 0.625 | 0.458–0.773 | 0.674 | 0.504–0.845 | 0.500 | 0.282–0.718 | 0.778 | 0.524–0.936 | 0.361 | 0.225–0.509 |
| LASSO | 0.675 | 0.509–0.814 | 0.727 | 0.567–0.888 | 0.636 | 0.407–0.828 | 0.722 | 0.465–0.903 | 0.321 | 0.177–0.469 |
| RF | 0.650 | 0.483–0.794 | 0.657 | 0.507–0.806 | 0.591 | 0.364–0.793 | 0.722 | 0.465–0.903 | 0.343 | 0.200–0.494 |
| RPART | 0.650 | 0.483–0.794 | 0.638 | 0.483–0.793 | 0.682 | 0.451–0.861 | 0.611 | 0.357–0.827 | 0.353 | 0.208–0.506 |
| SVM | 0.650 | 0.483–0.794 | 0.652 | 0.499–0.804 | 0.636 | 0.407–0.828 | 0.667 | 0.410–0.867 | 0.350 | 0.201–0.504 |
| Accuracy | ROC AUC | Specificity | Sensitivity | Balanced Error | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Technique | Mean | CI | Mean | CI | Mean | CI | Mean | CI | Mean | CI |
| BSWIMS | 0.775 | 0.615–0.892 | 0.732 | 0.553–0.911 | 0.773 | 0.546–0.922 | 0.778 | 0.524–0.936 | 0.223 | 0.100–0.359 |
| ENS | 0.750 | 0.588–0.873 | 0.824 | 0.681–0.968 | 0.773 | 0.546–0.922 | 0.722 | 0.465–0.903 | 0.250 | 0.124–0.398 |
| KNN | 0.675 | 0.509–0.814 | 0.721 | 0.550–0.892 | 0.727 | 0.498–0.893 | 0.611 | 0.357–0.827 | 0.330 | 0.191–0.482 |
| LASSO | 0.675 | 0.509–0.814 | 0.773 | 0.610–0.936 | 0.636 | 0.407–0.828 | 0.722 | 0.465–0.903 | 0.321 | 0.177–0.477 |
| RF | 0.775 | 0.615–0.892 | 0.770 | 0.636–0.905 | 0.818 | 0.597–0.948 | 0.722 | 0.465–0.903 | 0.225 | 0.101–0.360 |
| RPART | 0.500 | 0.338–0.662 | 0.513 | 0.348–0.677 | 0.454 | 0.244–0.678 | 0.555 | 0.308–0.785 | 0.499 | 0.343–0.653 |
| SVM | 0.750 | 0.588–0.873 | 0.742 | 0.603–0.882 | 0.818 | 0.597–0.948 | 0.667 | 0.410–0.867 | 0.255 | 0.127–0.401 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trejo-Castro, A.I.; Caballero-Luna, R.A.; Garnica-López, J.A.; Vega-Lara, F.; Martinez-Torteya, A. Signal and Texture Features from T2 Maps for the Prediction of Mild Cognitive Impairment to Alzheimer’s Disease Progression. Healthcare 2021, 9, 941. https://doi.org/10.3390/healthcare9080941
Trejo-Castro AI, Caballero-Luna RA, Garnica-López JA, Vega-Lara F, Martinez-Torteya A. Signal and Texture Features from T2 Maps for the Prediction of Mild Cognitive Impairment to Alzheimer’s Disease Progression. Healthcare. 2021; 9(8):941. https://doi.org/10.3390/healthcare9080941
Chicago/Turabian StyleTrejo-Castro, Alejandro I., Ricardo A. Caballero-Luna, José A. Garnica-López, Fernando Vega-Lara, and Antonio Martinez-Torteya. 2021. "Signal and Texture Features from T2 Maps for the Prediction of Mild Cognitive Impairment to Alzheimer’s Disease Progression" Healthcare 9, no. 8: 941. https://doi.org/10.3390/healthcare9080941