
Effects of a Randomized Home-Based Quality of Movement Protocol on Function, Posture and Strength in Outpatients with Obesity


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Multidisciplinary Lifestyle Program
2.3. Procedures
Functional Parameters
2.4. Training Intervention
2.5. Ethical Considerations
2.6. Statistical Analysis
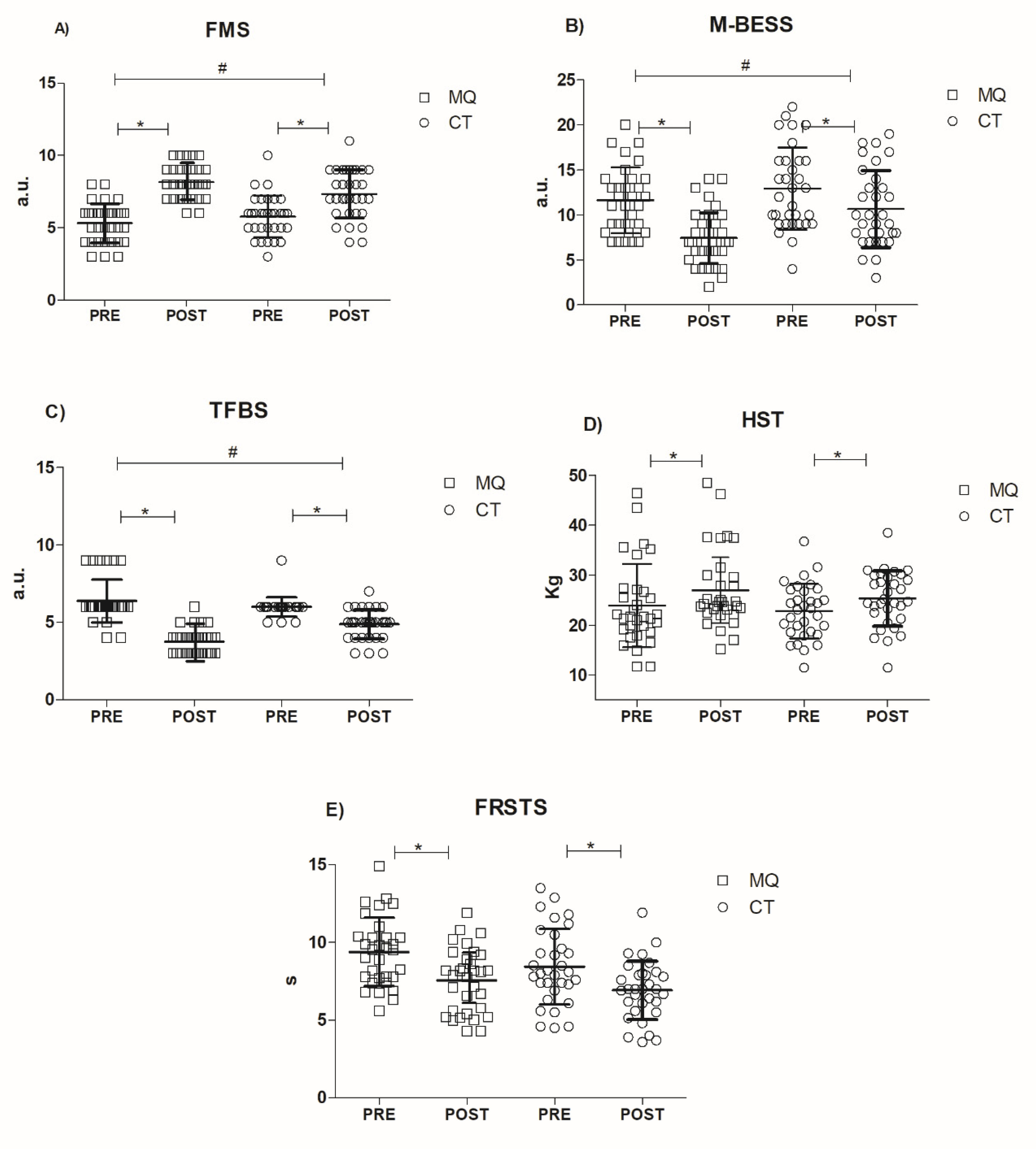
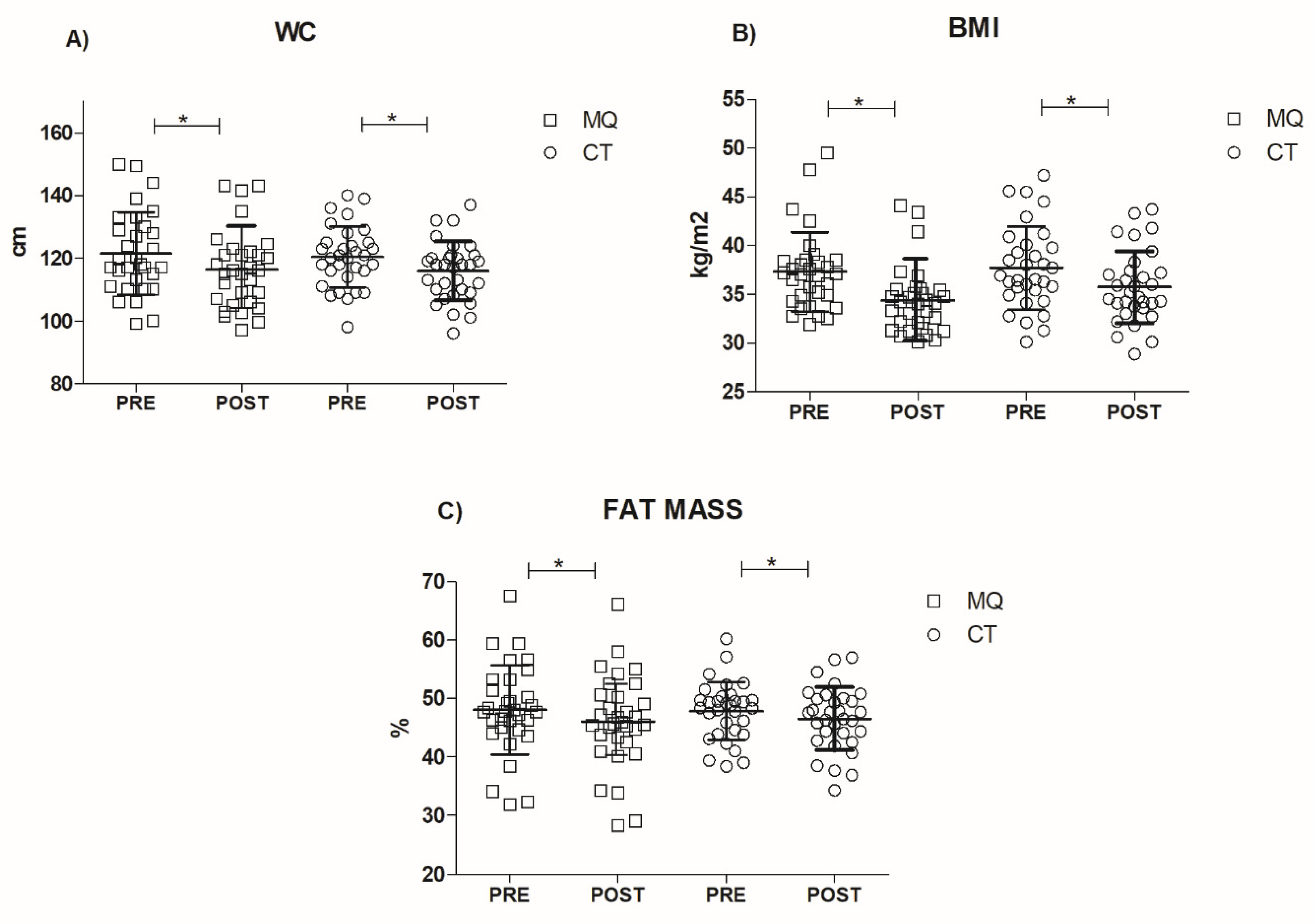
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knapik, J.J.; Sharp, M.A.; Canham-Chervak, M.; Hauret, K.; Patton, J.F.; Jones, B.H. Risk Factors for Training-Related Injuries among Men and Women in Basic Combat Training. Med. Sci. Sports Exerc. 2001, 33, 946–954. [Google Scholar] [CrossRef]
- Sallis, R.; Franklin, B.; Joy, L.; Ross, R.; Sabgir, D.; Stone, J. Strategies for Promoting Physical Activity in Clinical Practice. Prog. Cardiovasc. Dis. 2015, 57, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Yerrakalva, D.; Mullis, R.; Mant, J. The Associations of “Fatness,” “Fitness,” and Physical Activity with All-Cause Mortality in Older Adults: A Systematic Review. Obesity 2015, 23, 1944–1956. [Google Scholar] [CrossRef] [Green Version]
- Bray, G.A. Medical Consequences of Obesity. J. Clin. Endocrinol. Metab. 2004, 89, 2583–2589. [Google Scholar] [CrossRef] [Green Version]
- Haslam, D.W.; James, W.P.T. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar] [CrossRef]
- Capodaglio, P.; Cimolin, V.; Tacchini, E.; Parisio, C.; Galli, M. Balance Control and Balance Recovery in Obesity. Curr. Obes. Rep. 2012, 1, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Błaszczyk, J.W.; Cieślinska-Swider, J.; Plewa, M.; Zahorska-Markiewicz, B.; Markiewicz, A. Effects of Excessive Body Weight on Postural Control. J. Biomech. 2009, 42, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Gilleard, W.; Smith, T. Effect of Obesity on Posture and Hip Joint Moments during a Standing Task, and Trunk Forward Flexion Motion. Int. J. Obes (Lond.) 2007, 31, 267–271. [Google Scholar] [CrossRef]
- Molina-Garcia, P.; H Migueles, J.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Molina-Molina, A.; Garcia-Delgado, G.; D’Hondt, E.; et al. Fatness and Fitness in Relation to Functional Movement Quality in Overweight and Obese Children. J. Sports Sci. 2019, 37, 878–885. [Google Scholar] [CrossRef]
- Duncan, M.J.; Stanley, M.; Leddington Wright, S. The Association between Functional Movement and Overweight and Obesity in British Primary School Children. BMC Sports Sci. Med. Rehabil. 2013, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, D.J.; Erskine, R.M.; Morse, C.I.; Winwood, K.; Onambélé-Pearson, G. The Impact of Obesity on Skeletal Muscle Strength and Structure through Adolescence to Old Age. Biogerontology 2016, 17, 467–483. [Google Scholar] [CrossRef] [Green Version]
- Mafort, T.T.; Rufino, R.; Costa, C.H.; Lopes, A.J. Obesity: Systemic and Pulmonary Complications, Biochemical Abnormalities, and Impairment of Lung Function. Multidiscip. Respir. Med. 2016, 11, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frames, C.W.; Soangra, R.; Lockhart, T.E.; Lach, J.; Ha, D.S.; Roberto, K.A.; Lieberman, A. Dynamical Properties of Postural Control in Obese Community-Dwelling Older Adults. Sensors 2018, 18, 1692. [Google Scholar] [CrossRef] [Green Version]
- Maktouf, W.; Durand, S.; Boyas, S.; Pouliquen, C.; Beaune, B. Combined Effects of Aging and Obesity on Postural Control, Muscle Activity and Maximal Voluntary Force of Muscles Mobilizing Ankle Joint. J. Biomech. 2018, 79, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The Biomechanics of Restricted Movement in Adult Obesity. Obes. Rev. 2006, 7, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Gilardini, L.; Cancello, R.; Caffetto, K.; Cottafava, R.; Gironi, I.; Invitti, C. Nutrition Knowledge Is Associated with Greater Weight Loss in Obese Patients Following a Multidisciplinary Rehabilitaiton Program. Minerva Endocrinol. 2020, 46, 296–302. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports Medicine American College of Sports Medicine Position Stand. Appropriate Physical Activity Intervention Strategies for Weight Loss and Prevention of Weight Regain for Adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine American College of Sports Medicine Position Stand. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Bennett, H.; Arnold, J.; Martin, M.; Norton, K.; Davison, K. A Randomised Controlled Trial of Movement Quality-Focused Exercise versus Traditional Resistance Exercise for Improving Movement Quality and Physical Performance in Trained Adults. J. Sports Sci. 2019, 37, 2806–2817. [Google Scholar] [CrossRef]
- Frost, D.M.; Beach, T.A.C.; Callaghan, J.P.; McGill, S.M. Exercise-Based Performance Enhancement and Injury Prevention for Firefighters: Contrasting the Fitness- and Movement-Related Adaptations to Two Training Methodologies. J. Strength Cond. Res. 2015, 29, 2441–2459. [Google Scholar] [CrossRef] [PubMed]
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M. Functional Movement Screening: The Use of Fundamental Movements as an Assessment of Function—Part 1. Int J. Sports Phys. 2014, 9, 396–409. [Google Scholar]
- Cook, G.; Burton, L.; Hoogenboom, B.J.; Voight, M. Functional Movement Screening: The Use of Fundamental Movements as an Assessment of Function-Part 2. Int. J. Sports Phys. 2014, 9, 549–563. [Google Scholar]
- Iverson, G.L.; Koehle, M.S. Normative Data for the Modified Balance Error Scoring System in Adults. Brain Inj. 2013, 27, 596–599. [Google Scholar] [CrossRef]
- Mohan, V.; Perri, M.; Paungmali, A.; Sitilertpisan, P.; Joseph, L.H.; Jathin, R.; Mustafa, M.B.; Mohd Nasir, S.H.B. Intra-Rater and Inter-Rater Reliability of Total Faulty Breathing Scale Using Visual Observation and Videogrammetry Methods. J. Bodyw. Mov. 2017, 21, 694–698. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Kashman, N.; Volland, G.; Weber, K.; Dowe, M.; Rogers, S. Grip and Pinch Strength: Normative Data for Adults. Arch. Phys. Med. Rehabil 1985, 66, 69–74. [Google Scholar]
- Hamilton, G.F.; McDonald, C.; Chenier, T.C. Measurement of Grip Strength: Validity and Reliability of the Sphygmomanometer and Jamar Grip Dynamometer. J. Orthop. Sports Phys. 1992, 16, 215–219. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Bubela, D.J.; Magasi, S.R.; Wang, Y.-C.; Gershon, R.C. Sit-to-Stand Test: Performance and Determinants across the Age-Span. Isokinet Exerc. Sci. 2010, 18, 235–240. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Test-Retest Reliability of the Five-Repetition Sit-to-Stand Test: A Systematic Review of the Literature Involving Adults. J. Strength Cond. Res. 2011, 25, 3205–3207. [Google Scholar] [CrossRef]
- Cavaggioni, L.; Trecroci, A.; Tosin, M.; Iaia, F.M.; Alberti, G. Individualized Dry-Land Intervention Program for an Elite Paralympic Swimmer. J. Sports Med. Phys. Fit. 2019, 59, 82–86. [Google Scholar] [CrossRef]
- Stenger, L. What is Functional/Neuromotor Fitness? Acsm’s Health Fit. J. 2018, 22, 35–43. [Google Scholar] [CrossRef]
- Cavaggioni, L.; Ongaro, L.; Zannin, E.; Iaia, F.M.; Alberti, G. Effects of Different Core Exercises on Respiratory Parameters and Abdominal Strength. J. Phys. Sci. 2015, 27, 3249–3253. [Google Scholar] [CrossRef] [Green Version]
- Kobesova, A.; Kolar, P. Developmental Kinesiology: Three Levels of Motor Control in the Assessment and Treatment of the Motor System. J. Bodyw. Mov. 2014, 18, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S. Application of the TIDieR Checklist to Improve Understanding and Replicability of Studies in Physical and Rehabilitation Medicine. Eur. J. Phys. Rehabil. Med. 2015, 51, 667–668. [Google Scholar] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; ISBN 978-1-134-74277-6. [Google Scholar]
- Samsa, G.; Edelman, D.; Rothman, M.L.; Williams, G.R.; Lipscomb, J.; Matchar, D. Determining Clinically Important Differences in Health Status Measures: A General Approach with Illustration to the Health Utilities Index Mark II. Pharmacoeconomics 1999, 15, 141–155. [Google Scholar] [CrossRef]
- Mills, J.D.; Taunton, J.E.; Mills, W.A. The Effect of a 10-Week Training Regimen on Lumbo-Pelvic Stability and Athletic Performance in Female Athletes: A Randomized-Controlled Trial. Phys. Ther. Sport 2005, 6, 60–66. [Google Scholar] [CrossRef]
- Mitchell, U.H.; Johnson, A.W.; Vehrs, P.R.; Feland, J.B.; Hilton, S.C. Performance on the Functional Movement Screen in Older Active Adults. J. Sport Health Sci. 2016, 5, 119–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehling, W.E.; Gopisetty, V.; Daubenmier, J.; Price, C.J.; Hecht, F.M.; Stewart, A. Body Awareness: Construct and Self-Report Measures. PLoS ONE 2009, 4, e5614. [Google Scholar] [CrossRef] [Green Version]
- Behazin, N.; Jones, S.B.; Cohen, R.I.; Loring, S.H. Respiratory Restriction and Elevated Pleural and Esophageal Pressures in Morbid Obesity. J. Appl. Physiol. 2010, 108, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Sugerman, H.; Windsor, A.; Bessos, M.; Wolfe, L. Intra-Abdominal Pressure, Sagittal Abdominal Diameter and Obesity Comorbidity. J. Intern. Med. 1997, 241, 71–79. [Google Scholar] [CrossRef]
- Hills, A.P.; Hennig, E.M.; Byrne, N.M.; Steele, J.R. The Biomechanics of Adiposity--Structural and Functional Limitations of Obesity and Implications for Movement. Obes. Rev. 2002, 3, 35–43. [Google Scholar] [CrossRef]
- Massy-Westropp, N.M.; Gill, T.K.; Taylor, A.W.; Bohannon, R.W.; Hill, C.L. Hand Grip Strength: Age and Gender Stratified Normative Data in a Population-Based Study. BMC Res. Notes 2011, 4, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hergenroeder, A.L.; Brach, J.S.; Otto, A.D.; Sparto, P.J.; Jakicic, J.M. The Influence of Body Mass Index on Self-Report and Performance-Based Measures of Physical Function in Adult Women. Cardiopulm. Phys. J. 2011, 22, 11–20. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Volek, J.S.; Clark, K.L.; Gordon, S.E.; Puhl, S.M.; Koziris, L.P.; McBride, J.M.; Triplett-McBride, N.T.; Putukian, M.; Newton, R.U.; et al. Influence of Exercise Training on Physiological and Performance Changes with Weight Loss in Men. Med. Sci. Sports Exerc. 1999, 31, 1320–1329. [Google Scholar] [CrossRef]
- Seo, Y.-G.; Noh, H.-M.; Kim, S.Y. Weight Loss Effects of Circuit Training Interventions: A Systematic Review and Meta-Analysis. Obes. Rev. 2019, 20, 1642–1650. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Weeks | MQ | CT |
|---|---|---|
| Week 1 to 2 | Wall slide breathing with arms, rib-grab thoracic spine rotation from split stance, hip-airplane both feet on the ground, unilateral horizontal push with band in split squat position, goblet squat with dumbbell, side plank rotation with hands on the wall, unilateral horizontal pull with band in split squat position, in place standing cross-marching, pallof press from standing | Shoulder mobility circumduction, forward spine flexion from standing, quadriceps stretch, wall push-up, abdominal crunch, wall squat exercise, alternated biceps curl with dumbbells, abdominal oblique crunch, alternating forward lunge |
| Week 3 to 4 | Alternated wall slide breathing with arms, thoracic spine rotation with arm reach from split stance, hip-airplane with one foot raised, unilateral horizontal push with band with forward lunge, goblet squat to overhead press with dumbbell, tortional buttress with hands on table/wall, unilateral horizontal pull with band with backward lunge, in place standing cross-marching, stability lift with band in standing position | Shoulder flexion-extension mobility, forward spine flexion from standing with lower-legs abducted, quadriceps stretch, table push-up, abdominal crunch with slow eccentric phase, squat with dumbbells, symmetric biceps curl with dumbbells, abdominal oblique crunch, continuous forward lunge |
| Week 5 to 6 | Hip hinge with dowel, thoracic spine rotation with arm sweep from split stance, diaphragmatic breath with arms raised overhead, unilateral horizontal push with in monopodalic stance, squat with spine rotation and overhead press stability chop with band in standing position, unilateral horizontal pull in monopodalic stance, curl to press with dumbbells, stability lift with band in standing position | Shoulder adduction-abduction mobility, lateral spine flexion from standing with lower-legs abducted, quadriceps stretch, wall push-up with band around scapula, abdominal crunch with slow eccentric phase, squat with band under feet, symmetric biceps curl with band, abdominal oblique crunch, forward lunge with band under anterior foot |
| Characteristics | MQ | CT |
|---|---|---|
| Age (years) | 50.5 ± 10.4 | 50.4 ± 10.7 |
| Sex (Male/Female) | 6/26 | 5/27 |
| Weight (kg) | 100.6 ± 12.3 | 99.0 ± 14.9 |
| BMI (kg/m2) | 37.3 ± 4.0 | 37.7 ± 4.2 |
| Fat mass (%) | 37.3 ± 4.0 | 37.3 ± 4.0 |
| IPAQ (METS) | 552 ± 810 | 566 ± 1094 |
| Functional Movement ScreenTM (a.u.) | 5.3 ± 1.4 | 5.8 ± 1.4 |
| Modified Balance Error Scoring System (a.u.) | 11.6 ± 3.7 | 12.9 ± 4.6 |
| Total Faulty Breathing Scale (a.u.) | 6.4 ± 1.4 | 5.6 ± 1.6 |
| Handgrip Strength Test (kg) | 23.9 ± 8.3 | 22.8 ± 5.5 |
| Five repetition sit-to-stand | 9.4 ± 2.2 | 8.4 ± 2.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavaggioni, L.; Gilardini, L.; Redaelli, G.; Croci, M.; Capodaglio, P.; Gobbi, M.; Bertoli, S. Effects of a Randomized Home-Based Quality of Movement Protocol on Function, Posture and Strength in Outpatients with Obesity. Healthcare 2021, 9, 1451. https://doi.org/10.3390/healthcare9111451
Cavaggioni L, Gilardini L, Redaelli G, Croci M, Capodaglio P, Gobbi M, Bertoli S. Effects of a Randomized Home-Based Quality of Movement Protocol on Function, Posture and Strength in Outpatients with Obesity. Healthcare. 2021; 9(11):1451. https://doi.org/10.3390/healthcare9111451
Chicago/Turabian StyleCavaggioni, Luca, Luisa Gilardini, Gabriella Redaelli, Marina Croci, Paolo Capodaglio, Michele Gobbi, and Simona Bertoli. 2021. "Effects of a Randomized Home-Based Quality of Movement Protocol on Function, Posture and Strength in Outpatients with Obesity" Healthcare 9, no. 11: 1451. https://doi.org/10.3390/healthcare9111451