
Impact of Bariatric Surgery on the Healthy Eating Index, Binge Eating Behavior and Food Craving in a Middle Eastern Population: A Lebanese Experience

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Population
2.2. Tools
2.2.1. Healthy Eating Index
2.2.2. Binge Eating Scale
2.2.3. Food Craving Inventory
3. Ethical Considerations
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Food Item | Pre-Surgery N (%) | Post-Surgery N (%) | p Value | |
|---|---|---|---|---|
| Cake | 0 | 29 (48) | 31 (52) | 0.025 |
| 1 | 6 (10) | 12 (20) | ||
| 2 | 9 (15) | 11 (18) | ||
| 3 | 8 (13) | 3 (5) | ||
| 4 | 8 (13) | 3 (5) | ||
| Pizza | 0 | 38 (63) | 45 (75) | <0.01 |
| 1 | 2 (3) | 6 (10) | ||
| 2 | 6 (10) | 6 (10) | ||
| 3 | 3 (5) | 3 (5) | ||
| 4 | 11 (18) | 0 (0) | ||
| Fried Chicken | 0 | 38 (63) | 45 (76) | <0.01 |
| 1 | 2 (3) | 7 (12) | ||
| 2 | 6 (10) | 3 (5) | ||
| 3 | 6 (10) | 2 (3) | ||
| 4 | 8 (13) | 2 (3) | ||
| Sausages | 0 | 49 (82) | 54 (90) | 0.020 |
| 1 | 3 (5) | 4 (7) | ||
| 2 | 2 (3) | 1 (2) | ||
| 3 | 3 (5) | 1 (2) | ||
| 4 | 3 (5) | 0 (0) | ||
| Fries | 0 | 37 (62) | 47 (78) | <0.01 |
| 1 | 1 (2) | 1 (2) | ||
| 2 | 3 (5) | 4 (7) | ||
| 3 | 5 (8) | 4 (7) | ||
| 4 | 14 (23) | 4 (7) | ||
| Rice | 0 | 43 (72) | 46 (77) | 0.026 |
| 1 | 0 (0) | 4 (7) | ||
| 2 | 3 (5) | 5 (8) | ||
| 3 | 7 (12) | 3 (5) | ||
| 4 | 7 (12) | 2 (3) | ||
| Hotdogs | 0 | 55 (92) | 57 (95) | 0.275 |
| 1 | 1 (2) | 1 (2) | ||
| 2 | 2 (3) | 0 (0) | ||
| 3 | 0 (0) | 1 (2) | ||
| 4 | 2 (3) | 1 (2) | ||
| Hazelnuts | 0 | 35 (58) | 42 (70) | 0.014 |
| 1 | 3 (5) | 3 (5) | ||
| 2 | 8 (13) | 8 (13) | ||
| 3 | 4 (7) | 3 (5) | ||
| 4 | 10 (17) | 4 (7) | ||
| Burgers | 0 | 38 (63) | 43 (72) | 0.027 |
| 1 | 2 (3) | 4 (7) | ||
| 2 | 4 (7) | 6 (10) | ||
| 3 | 6 (10) | 3 (5) | ||
| 4 | 10 (17) | 4 (7) | ||
| Biscuits | 0 | 42 (70) | 45 (75) | 0.056 |
| 1 | 1 (2) | 2 (3) | ||
| 2 | 4 (7) | 7 (12) | ||
| 3 | 3 (5) | 4 (7) | ||
| 4 | 10 (17) | 2 (3) | ||
| Ice Cream | 0 | 27 (45) | 32 (53) | <0.01 |
| 1 | 2 (3) | 9 (15) | ||
| 2 | 2 (3) | 9 (15) | ||
| 3 | 11 (18) | 3 (5) | ||
| 4 | 18 (30) | 7 (12) | ||
| Pasta | 0 | 38 (63) | 41 (68) | 0.010 |
| 1 | 0 (0) | 2 (3) | ||
| 2 | 9 (15) | 9 (15) | ||
| 3 | 4 (7) | 3 (5) | ||
| 4 | 9 (15) | 5 (8) | ||
| Fried Fish | 0 | 46 (77) | 50 (83) | 0.096 |
| 1 | 2 (3) | 0 (0) | ||
| 2 | 5 (8) | 4 (7) | ||
| 3 | 1 (2) | 3 (5) | ||
| 4 | 6 (10) | 3 (5) | ||
| Cookies | 0 | 53 (88) | 56 (93) | 0.090 |
| 1 | 2 (3) | 2 (3) | ||
| 2 | 0 (0) | 1 (2) | ||
| 3 | 2 (3) | 0 (0) | ||
| 4 | 3 (5) | 1 (2) | ||
| Chocolate | 0 | 19 (32) | 21 (35) | 0.034 |
| 1 | 1 (2) | 5 (8) | ||
| 2 | 4 (7) | 8 (13) | ||
| 3 | 2 (3) | 5 (8) | ||
| 4 | 34 (57) | 21 (35) | ||
| Pancakes | 0 | 54 (90) | 58 (97) | 0.144 |
| 1 | 2 (3) | 0 (0) | ||
| 2 | 2 (3) | 0 (0) | ||
| 3 | 1 (2) | 2 (3) | ||
| 4 | 1 (2) | 0 (0) | ||
| Rolls | 0 | 56 (93) | 58 (97) | 0.050 |
| 2 | 1 (2) | 2 (3) | ||
| 3 | 2 (3) | 0 (0) | ||
| 4 | 1 (2) | 0 (0) | ||
| Donuts | 0 | 47 (78) | 49 (83) | 0.024 |
| 1 | 2 (3) | 4 (7) | ||
| 2 | 4 (7) | 5 (8) | ||
| 3 | 4 (7) | 1 (2) | ||
| 4 | 3 (5) | 0 (0) | ||
| Candies | 0 | 52 (87) | 52 (87) | 0.527 |
| 1 | 1 (2) | 1 (2) | ||
| 2 | 1 (2) | 2 (3) | ||
| 3 | 2 (3) | 4 (7) | ||
| 4 | 4 (7) | 1 (2) | ||
| Brownies | 0 | 36 (60) | 44 (73) | <0.01 |
| 1 | 2 (3) | 4 (7) | ||
| 2 | 5 (8) | 6 (10) | ||
| 3 | 6 (10) | 2 (3) | ||
| 4 | 11 (18) | 4 (7) | ||
| Bacon * | 0 | 59 (98) | 60 (100) | 1 |
| 2 | 1 (2) | 0 (0) | ||
| Croissants | 0 | 34 (57) | 41 (68) | <0.01 |
| 1 | 2 (3) | 9 (15) | ||
| 2 | 8 (13) | 6 (10) | ||
| 3 | 9 (15) | 3 (5) | ||
| 4 | 7 (12) | 1 (2) | ||
| Steak | 0 | 42 (70) | 45 (75) | 0.028 |
| 1 | 2 (3) | 5 (8) | ||
| 2 | 1 (2) | 2 (3) | ||
| 3 | 4 (7) | 2 (3) | ||
| 4 | 11 (18) | 6 (10) | ||
| Pie | 0 | 52 (87) | 56 (93) | 0.029 |
| 1 | 1 (2) | 2 (3) | ||
| 2 | 5 (8) | 0 (0) | ||
| 4 | 2 (3) | 2 (3) | ||
| Baked Potato | 0 | 55 (92) | 53 (88) | 0.194 |
| 1 | 1 (2) | 0 (0) | ||
| 2 | 3 (5) | 5 (8) | ||
| 3 | 1 (2) | 0 (0) | ||
| 4 | 0 (0) | 2 (3) | ||
| Barbecued Food | 0 | 34 (57) | 42 (70) | <0.01 |
| 1 | 2 (3) | 5 (8) | ||
| 2 | 4 (7) | 6 (10) | ||
| 3 | 6 (10) | 2 (3) | ||
| 4 | 14 (23) | 5 (8) | ||
| Mashed Potato | 0 | 58 (97) | 55 (92) | 0.102 |
| 1 | 1 (2) | 2 (3) | ||
| 2 | 1 (2) | 1 (2) | ||
| 3 | 0 (0) | 1 (2) | ||
| 4 | 0 (0) | 1 (2) | ||
| Bagels | 0 | 54 (90) | 57 (95) | 0.223 |
| 1 | 1 (2) | 1 (2) | ||
| 2 | 3 (5) | 2 (3) | ||
| 3 | 0 (0) | 0 (0) | ||
| 4 | 2 (3) | 0 (0) | ||
References
- Seidell, J.C.; Halberstadt, J. The Global Burden of Obesity and the Challenges of Prevention. Ann. Nutr. Metab. 2015, 66, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Alsumali, A.; Eguale, T.; Bairdain, S.; Samnaliev, M. Cost-effectiveness analysis of bariatric surgery for morbid obesity. Obes. Surg. 2018, 28, 2203–2214. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-H.; Stoll, C.R.; Song, J.; Varela, J.E.; Eagon, C.J.; Colditz, G.A. The effectiveness and risks of bariatric surgery: An updated systematic review and meta-analysis, 2003-2012. JAMA Surg. 2014, 149, 275–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.E.; Ghaferi, A.A. Understanding the Benefits of Bariatric Surgery: How Much Evidence Is Enough? JAMA Surg. 2018, 153, e183332. [Google Scholar] [CrossRef]
- Sjöström, L.; Lindroos, A.-K.; Peltonen, M.; Torgerson, J.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; Larsson, B.; Narbro, K.; Sjöström, C.D. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N. Engl. J. Med. 2004, 351, 2683–2693. [Google Scholar] [CrossRef]
- Singh, P.; Subramanian, A.; Adderley, N.; Gokhale, K.; Singhal, R.; Bellary, S.; Nirantharakumar, K.; Tahrani, A. Impact of bariatric surgery on cardiovascular outcomes and mortality: A population-based cohort study. Br. J. Surg. 2020, 107, 432–442. [Google Scholar] [CrossRef]
- Bond, D.S.; Phelan, S.; Leahey, T.M.; Hill, J.O.; Wing, R.R. Weight-loss maintenance in successful weight losers: Surgical vs non-surgical methods. Int. J. Obes. 2009, 33, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Christou, N.V.; Look, D.; MacLean, L.D. Weight gain after short-and long-limb gastric bypass in patients followed for longer than 10 years. Ann. Surg. 2006, 244, 734. [Google Scholar] [CrossRef]
- Dayyeh, B.K.A.; Lautz, D.B.; Thompson, C.C. Gastrojejunal stoma diameter predicts weight regain after Roux-en-Y gastric bypass. Clin. Gastroenterol. Hepatol. 2011, 9, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Gils Contreras, A.; Bonada Sanjaume, A.; Becerra-Tomás, N.; Salas-Salvadó, J. Adherence to Mediterranean Diet or Physical Activity After Bariatric Surgery and Its Effects on Weight Loss, Quality of Life, and Food Tolerance. Obes. Surg. 2020, 30, 687–696. [Google Scholar] [CrossRef]
- Da Silva, F.B.L.; Gomes, D.L.; de Carvalho, K.M.B. Poor diet quality and postoperative time are independent risk factors for weight regain after Roux-en-Y gastric bypass. Nutrition 2016, 32, 1250–1253. [Google Scholar] [CrossRef]
- Odom, J.; Zalesin, K.C.; Washington, T.L.; Miller, W.W.; Hakmeh, B.; Zaremba, D.L.; Altattan, M.; Balasubramaniam, M.; Gibbs, D.S.; Krause, K.R. Behavioral predictors of weight regain after bariatric surgery. Obes. Surg. 2010, 20, 349–356. [Google Scholar] [CrossRef]
- Rutledge, T.; Groesz, L.M.; Savu, M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes. Surg. 2011, 21, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Velapati, S.R.; Shah, M.; Kuchkuntla, A.R.; Abu-dayyeh, B.; Grothe, K.; Hurt, R.T.; Mundi, M.S. Weight Regain After Bariatric Surgery: Prevalence, Etiology, and Treatment. Curr. Nutr. Rep. 2018, 7, 329–334. [Google Scholar] [CrossRef]
- Papasavas, P.; Swede, H.; Stone, A.; Rawal, S.; Ng, J.; Tishler, D.; Duffy, V. Successful Weight Loss Post Bariatric Surgery Associates with Greater Affinity for Healthy Dietary and Activity Behaviors—Preliminary Support from A Case-Controlled Study. Surg. Obes. Relat. Dis. 2015, 11, S170–S171. [Google Scholar] [CrossRef]
- Tewksbury, C.; Wu, J.; Allison, K.C.; Gardiner, H.; Dumon, K.R.; Williams, N.N.; Sarwer, D.B. Prebariatric surgery care and postoperative outcomes: Increased number of visits associated with smaller weight losses over first 2 postoperative years. Surg. Obes. Relat. Dis. 2019, 15, 1548–1553. [Google Scholar] [CrossRef]
- Goldschmidt, A.B.; Conceição, E.M.; Thomas, J.G.; Mitchell, J.E.; Raynor, H.A.; Bond, D.S. Conceptualizing and studying binge and loss of control eating in bariatric surgery patients—time for a paradigm shift? Surg. Obes. Relat. Dis. 2016, 12, 1622–1625. [Google Scholar] [CrossRef] [Green Version]
- Cella, S.; Landino, F.; Rosa, D.A.; Giardiello, C.; Allaria, A.; Cotrufo, P. Binge eating disorder and related features in bariatric surgery candidates. Open Med. 2019, 14, 407–415. [Google Scholar] [CrossRef]
- Niego, S.H.; Kofman, M.D.; Weiss, J.J.; Geliebter, A. Binge eating in the bariatric surgery population: A review of the literature. Int. J. Eat. Disord. 2007, 40, 349–359. [Google Scholar] [CrossRef]
- Smith, K.E.; Orcutt, M.; Steffen, K.J.; Crosby, R.D.; Cao, L.; Garcia, L.; Mitchell, J.E. Loss of Control Eating and Binge Eating in the 7 Years Following Bariatric Surgery. Obes. Surg. 2019, 29, 1773–1780. [Google Scholar] [CrossRef]
- Fong, M. What, When and Why We Eat: Associations with Obesity in Adults. Ph.D. Thesis, The University of Sydney, Sydney, Australia, 2019. [Google Scholar]
- Surgenor, L.J. Commentary on disordered eating symptoms and bariatric/metabolic surgery. Australas Psychiatry 2020, 28, 153–155. [Google Scholar] [CrossRef]
- Freire, C.C.; Zanella, M.T.; Segal, A.; Arasaki, C.H.; Matos, M.I.R.; Carneiro, G. Associations between binge eating, depressive symptoms and anxiety and weight regain after Roux-en-Y gastric bypass surgery. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2020. [Google Scholar] [CrossRef]
- Utzinger, L.M.; Gowey, M.A.; Zeller, M.; Jenkins, T.M.; Engel, S.G.; Rofey, D.L.; Inge, T.H.; Mitchell, J.E. Teen Longitudinal Assessment of Bariatric Surgery (Teen-LABS) Consortium. Loss of control eating and eating disorders in adolescents before bariatric surgery. Int. J. Eat. Disord. 2016, 49, 947–952. [Google Scholar] [CrossRef] [Green Version]
- Koball, A.M.; Ames, G.; Goetze, R.E.; Grothe, K. Bariatric Surgery as a Treatment for Food Addiction? A Review of the Literature. Curr. Addict. Rep. 2020, 7, 1–8. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Food addiction: An examination of the diagnostic criteria for dependence. J. Addict. Med. 2009, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- White, M.A.; Grilo, C.M. Psychometric properties of the Food Craving Inventory among obese patients with binge eating disorder. Eat. Behav. 2005, 6, 239–245. [Google Scholar] [CrossRef]
- Ivezaj, V.; Wiedemann, A.A.; Grilo, C.M. Food addiction and bariatric surgery: A systematic review of the literature. Obes. Rev. 2017, 18, 1386–1397. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases Country Profiles (Lebanon) 2018. Available online: https://apps.who.int/iris/handle/10665/274512/ (accessed on 11 July 2021).
- Mansour, Z.; Said, R.; Dbaibo, H.; Mrad, P.; Torossian, L.; Rady, A.; Dufouil, C. Non-communicable diseases in Lebanon: Results from World Health Organization STEPS survey 2017. Public Health 2020, 187, 120–126. [Google Scholar] [CrossRef]
- Chamieh, M.C.; Moore, H.J.; Summerbell, C.; Tamim, H.; Sibai, A.M.; Hwalla, N. Diet, physical activity and socio-economic disparities of obesity in Lebanese adults: Findings from a national study. BMC Public Health 2015, 15, 279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohta, M.; Seki, Y.; Wong, S.K.-H.; Wang, C.; Huang, C.-K.; Aly, A.; Baijal, M.; Al-Sabah, S.; Udomsawaengsup, S.; Heo, Y.S.; et al. Bariatric/Metabolic Surgery in the Asia-Pacific Region: APMBSS 2018 Survey. Obes. Surg. 2019, 29, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Aridi, H.D.; Alami, R.; Tamim, H.; Shamseddine, G.; Fouani, T.; Safadi, B. Long-term outcomes of laparoscopic sleeve gastrectomy: A Lebanese center experience. Surg. Obes. Relat. Dis. 2016, 12, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, A.; Casamitjana, R.; Flores, L.; Viaplana, J.; Corcelles, R.; Lacy, A.; Vidal, J. Long-term effects of sleeve gastrectomy and Roux-en-Y gastric bypass surgery on type 2 diabetes mellitus in morbidly obese subjects. Ann. Surg. 2012, 256, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- El Ansari, W.; Elhag, W. Weight Regain and Insufficient Weight Loss After Bariatric Surgery: Definitions, Prevalence, Mechanisms, Predictors, Prevention and Management Strategies, and Knowledge Gaps—A Scoping Review. Obes. Surg. 2021, 31, 1755–1766. [Google Scholar] [CrossRef] [PubMed]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute Division of Cancer Control & Population Sciences. Overview of the Methods & Calculations. Available online: https://epi.grants.cancer.gov/hei/hei-methods-and-calculations.html (accessed on 3 January 2021).
- Grupski, A.E.; Hood, M.M.; Hall, B.J.; Azarbad, L.; Fitzpatrick, S.L.; Corsica, J.A. Examining the Binge Eating Scale in Screening for Binge Eating Disorder in Bariatric Surgery Candidates. Obes. Surg. 2013, 23, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- White, M.A.; Whisenhunt, B.L.; Williamson, D.A.; Greenway, F.L.; Netemeyer, R.G. Development and validation of the food-craving inventory. Obes. Res. 2002, 10, 107–114. [Google Scholar] [CrossRef]
- El Labban, S.; Safadi, B.; Olabi, A. The Effect of Roux-en-Y Gastric Bypass and Sleeve Gastrectomy Surgery on Dietary Intake, Food Preferences, and Gastrointestinal Symptoms in Post-Surgical Morbidly Obese Lebanese Subjects: A Cross-Sectional Pilot Study. Obes. Surg. 2015, 25, 2393–2399. [Google Scholar] [CrossRef]
- Zarshenas, N.; Tapsell, L.C.; Neale, E.P.; Batterham, M.; Talbot, M.L. The Relationship between Bariatric Surgery and Diet Quality: A Systematic Review. Obes. Surg. 2020, 30, 1768–1792. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Bradley, D.; Eagon, J.C.; Sullivan, S.; Abumrad, N.A.; Klein, S. Changes in taste perception and eating behavior after bariatric surgery-induced weight loss in women. Obesity 2014, 22, E13–E20. [Google Scholar] [CrossRef]
- Kasim, A.; Penney, N.; Darzi, A.; Purkayastha, S. Taste Changes after Bariatric Surgery: A Systematic Review. Obes. Surg. 2018, 28, 3321–3332. [Google Scholar] [CrossRef] [Green Version]
- Coluzzi, I.; Raparelli, L.; Guarnacci, L.; Paone, E.; Del Genio, G.; Le Roux, C.W.; Silecchia, G. Food intake and changes in eating behavior after laparoscopic sleeve gastrectomy. Obes. Surg. 2016, 26, 2059–2067. [Google Scholar] [CrossRef]
- Leahey, T.M.; Bond, D.S.; Raynor, H.; Roye, D.; Vithiananthan, S.; Ryder, B.A.; Sax, H.C.; Wing, R.R. Effects of bariatric surgery on food cravings: Do food cravings and the consumption of craved foods “normalize” after surgery? Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2012, 8, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Chou, J.-J.; Lee, W.-J.; Almalki, O.; Chen, J.-C.; Tsai, P.-L.; Yang, S.-H. Dietary Intake and Weight Changes 5 Years After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2017, 27, 3240–3246. [Google Scholar] [CrossRef]
- Ivezaj, V.; Barnes, R.D.; Cooper, Z.; Grilo, C.M. Loss-of-control eating after bariatric/sleeve gastrectomy surgery: Similar to binge-eating disorder despite differences in quantities. Gen. Hosp. Psychiatry 2018, 54, 25–30. [Google Scholar] [CrossRef]
- Kops, N.L.; Vivan, M.A.; de Castro, M.L.D.; Horvath, J.D.C.; Costa, F.S.; Friedman, R. Binge eating scores pre-bariatric surgery and subsequent weight loss: A prospective, 5 years follow-up study. Clin. Nutr. ESPEN 2020, 38, 146–152. [Google Scholar] [CrossRef]
- Bianciardi, E.; Gentileschi, P.; Niolu, C.; Innamorati, M.; Fabbricatore, M.; Contini, L.M.; Procenesi, L.; Siracusano, A.; Imperatori, C. Assessing psychopathology in bariatric surgery candidates: Discriminant validity of the SCL-90-R and SCL-K-9 in a large sample of patients. Eat. Weight Disord. 2021, 26, 2211–2218. [Google Scholar] [CrossRef]
- Nasirzadeh, Y.; Kantarovich, K.; Wnuk, S.; Okrainec, A.; Cassin, S.E.; Hawa, R.; Sockalingam, S. Binge Eating, Loss of Control over Eating, Emotional Eating, and Night Eating After Bariatric Surgery: Results from the Toronto Bari-PSYCH Cohort Study. Obes. Surg. 2018, 28, 2032–2039. [Google Scholar] [CrossRef]
- King, W.C.; Hinerman, A.S.; Belle, S.H.; Wahed, A.S.; Courcoulas, A.P. Comparison of the Performance of Common Measures of Weight Regain After Bariatric Surgery for Association with Clinical Outcomes. JAMA 2018, 320, 1560–1569. [Google Scholar] [CrossRef]
- Clapp, B.; Wynn, M.; Martyn, C.; Foster, C.; O’Dell, M.; Tyroch, A. Long term (7 or more years) outcomes of the sleeve gastrectomy: A meta-analysis. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2018, 14, 741–747. [Google Scholar] [CrossRef]
- Freire, R.H.; Borges, M.C.; Alvarez-Leite, J.I.; Correia, M.I.T.D. Food quality, physical activity, and nutritional follow-up as determinant of weight regain after Roux-en-Y gastric bypass. Nutrition 2012, 28, 53–58. [Google Scholar] [CrossRef]
- Baig, S.J.; Pallawi, P.; Mahawar, K.K.; Shah, S. Weight Regain After Bariatric Surgery—A Multicentre Study of 9617 Patients from Indian Bariatric Surgery Outcome Reporting Group. Obes. Surg. 2019, 29, 1583–1592. [Google Scholar] [CrossRef]
- Fried, M.; Hainer, V.; Basdevant, A.; Buchwald, H.; Deitel, M.; Finer, N.; Greve, J.; Horber, F.; Mathus-Vliegen, E.; Scopinaro, N. Inter-disciplinary European guidelines on surgery of severe obesity. Int. J. Obes. 2007, 31, 569–577. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Richard, L.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines For The Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored By American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society For Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists *. Endocr. Pract. 2019, 25, 1–75. [Google Scholar] [CrossRef]
- Bianciardi, E.; Imperatori, C.; Innamorati, M.; Fabbricatore, M.; Monacelli, A.M.; Pelle, M.; Siracusano, A.; Niolu, C.; Gentileschi, P. Measuring Knowledge, Attitudes, and Barriers to Medication Adherence in Potential Bariatric Surgery Patients. Obes. Surg. 2021, 31, 4045–4054. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Kushner, R.F.; Sugerman, H.J.; Gonzalez-Campoy, J.M.; Collazo-Clavell, M.L.; Guven, S.; Spitz, A.F.; Apovian, C.M.; Livingston, E.H.; Brolin, R. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2010, 6, 112. [Google Scholar]
- Van Zyl, N.; Andrews, L.; Williamson, H.; Meyrick, J. The effectiveness of psychosocial interventions to support psychological well-being in post-operative bariatric patients: A systematic review of evidence. Obes. Res. Clin. Pract. 2020, 14, 404–420. [Google Scholar] [CrossRef]
- World Health Organization. WHO Country Cooperation Strategy at A Glance: Lebanon. Available online: https://www.who.int/publications/i/item/WHO-CCU-18.02-Lebanon (accessed on 13 October 2021).

| Variable | Result (N = 60) | |
|---|---|---|
| Gender, n (%) | male | 9 (15) |
| female | 51 (85) | |
| Age (years), mean ± SD | 35.5 ± 11 | |
| Educational Level, n (%) | primary | 16 (27) |
| secondary | 12 (20) | |
| tertiary | 32 (53) | |
| Occupation status, n (%) | unemployed | 24 (40) |
| student | 10 (17) | |
| employed | 26 (43) | |
| Surgery Type, n (%) | bypass | 6 (10) |
| sleeve | 54 (90) | |
| Time since surgery (years) | 2.4 ± 1.8 | |
| Time since surgery (years) | 0.5–1 | 9 (23) |
| 1–3 | 21 (53) | |
| 3–5 | 8 (20) | |
| >5 | 2 (5) | |
| Pre-surgery BMI (Kg/m2) | 43.3 ± 8.0 | |
| Post-surgery BMI (Kg/m2) | 29.3 ± 5.3 | |
| Weight Regain, n (%) | 24 (40) | |
| Variable | Pre-Surgery | Post-Surgery | p Value |
|---|---|---|---|
| Energy Intake (Kcal/day) | 4002 ± 1898 | 1142 ± 556 | <0.01 |
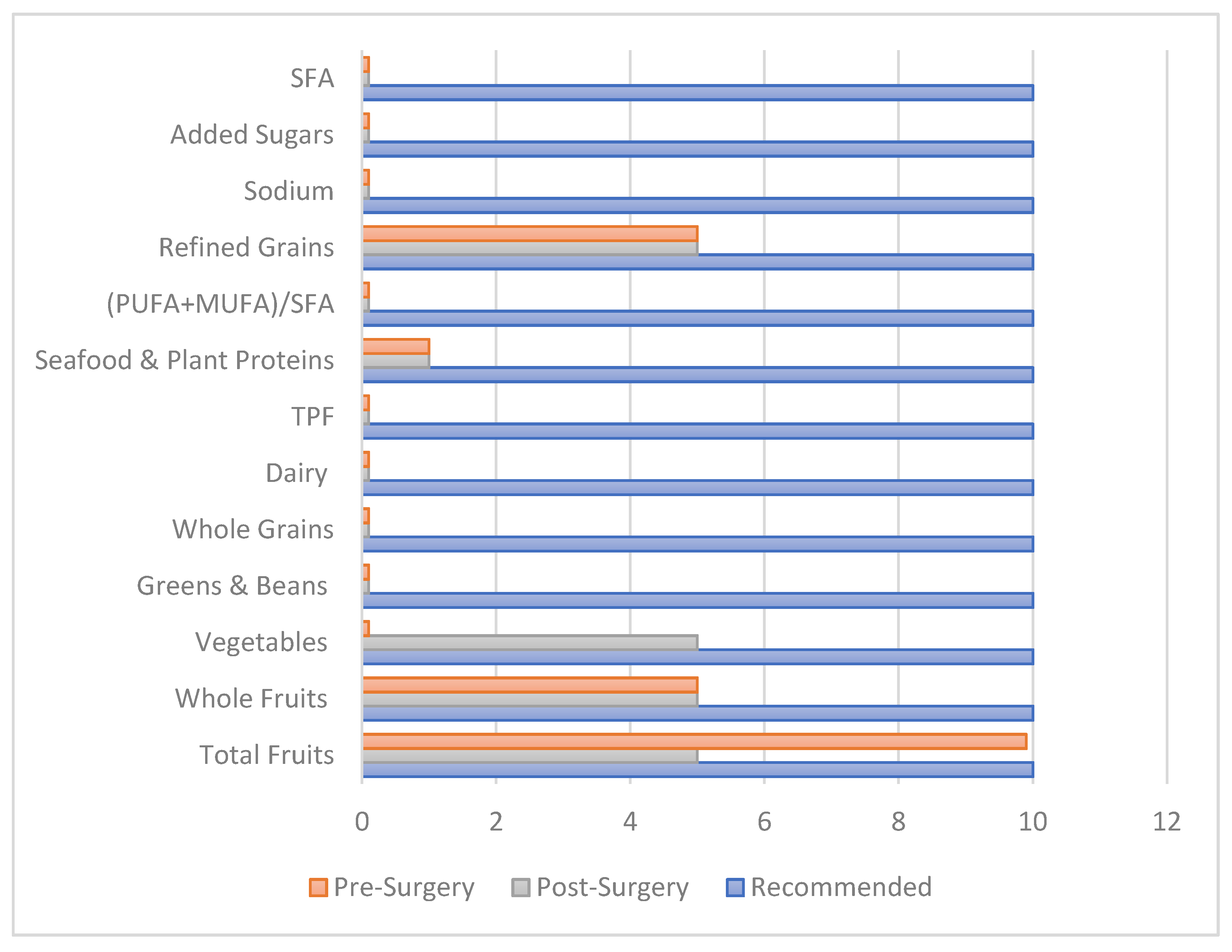
| Healthy Eating Index | 27 ± 8.6 | 36 ± 13 | <0.01 |
| Total Fruits (cups/1000 Kcal) | 0.54 ± 0.83 | 0.98 ± 1.2 | 0.015 |
| Whole Fruits (cups/1000 Kcal) | 0.53 ± 0.83 | 0.92 ± 1.2 | 0.032 |
| Vegetables (cups/1000 Kcal) | 0.64 ± 0.57 | 1.1 ± 1.5 | 0.025 |
| Greens & Beans (cups/1000 Kcal) | 0.06 ± 0.15 | 0.06 ± 0.17 | 0.844 |
| Whole Grains (oz/1000 Kcal) | 0.05 ± 0.14 | 0.64 ± 1.0 | <0.01 |
| Dairy (cups/1000 Kcal) | 0.26 ± 0.25 | 0.71 ± 1.2 | <0.01 |
| TPF (oz/day) | 1.6 ± 0.86 | 2.0 ± 1.4 | 0.105 |
| Seafood and Plant Proteins (oz/1000 Kcal) | 0.88 ± 0.87 | 1.0 ± 1.7 | 0.504 |
| 0.67 ± 0.46 | 0.87 ± 0.83 | 0.096 | |
| Refined Grains (oz/day) | 3.3 ± 1.1 | 2.5 ± 1.4 | <0.01 |
| Sodium (grams/1000 Kcal) | 2.1 ± 0.48 | 3.1 ± 2.1 | <0.01 |
| Added Sugars (% of energy) | 13 ± 8.0 | 7.1 ± 7.1 | <0.01 |
| Saturated Fatty Acids (% of energy) | 28 ± 30 | 24 ± 8.2 | 0.285 |
| Group Comparison | Within Groups | Between Groups | ||||||
|---|---|---|---|---|---|---|---|---|
| Variable/Weight Regain Categories | No Weight Regain 36 (60%) | Weight Regain 24 (40%) | p-Value Baseline | p-Value % Change | ||||
| Pre-Surgery | Post-Surgery | % Change | Pre-Surgery | Post-Surgery | % Change | |||
| Daily Energy intake (Kcal) | 4010 ± 2100 | 981 ± 439 | 71 ± 17 | 3990 ± 1589 | 1383 ± 630 | 60 ± 24 | 0.968 | 0.039 |
| HEI score | 27 ± 9.0 | 37 ± 13 | −50 ± 65 | 27 ± 8.3 | 35 ± 13 | −40 ± 68 | 0.995 | 0.536 |
| Total Fruits servings/1000 Kcal | 0.53 ± 0.88 | 1.2 ± 1.4 | −141 ± 308 | 0.55 ± 0.78 | 0.67 ± 0.78 | −31 ± 149 | 0.903 | 0.213 |
| Whole Fruits (cups/1000 Kcal) | 0.52 ± 0.88 | 1.1 ± 1.4 | −145 ± 306 | 0.54 ± 0.76 | 0.61 ± 0.78 | −17 ± 151 | 0.912 | 0.148 |
| Vegetables exchanges, servings/1000 Kcal | 0.60 ± 0.56 | 1.1 ± 1.8 | −139 ± 328 | 0.70 ± 0.58 | 1.1 ± 1.0 | −93 ± 200 | 0.479 | 0.560 |
| Greens & Beans (cups/1000 Kcal) | 0.08 ± 0.17 | 0.05 ± 0.19 | 38 ± 183 | 0.04 ± 0.13 | 0.07 ± 0.14 | 100 ± 0 | 0.375 | 0.583 |
| Whole Grains servings/1000 Kcal | 0.02 ± 0.09 | 0.50 ± 0.91 | 100 ± 0 | 0.08 ± 0.18 | 0.85 ± 1.18 | −100 ± 246 | 0.077 | 0.143 |
| Dairy (cups/1000 Kcal) | 0.22 ± 0.22 | 0.63 ± 0.89 | −236 ± 533 | 0.32 ± 0.29 | 0.83 ± 1.62 | −151 ± 294 | 0.135 | 0.514 |
| TPF (oz/day) | 1.69 ± 0.83 | 2.04 ± 1.53 | −58 ± 171 | 1.5 ± 0.92 | 1.8 ± 1.13 | −27 ± 106 | 0.471 | 0.445 |
| Seafood & Plant Protein servings (oz/1000 Kcal) | 0.93 ± 0.93 | 0.89 ± 1.33 | −61 ± 341 | 0.79 ± 0.77 | 1.2 ± 2.1 | −34 ± 234 | 0.547 | 0.402 |
| 0.64 ± 0.45 | 1.1 ± 0.99 | −150 ± 269 | 0.72 ± 0.49 | 0.60 ± 0.41 | −32 ± 202 | 0.550 | 0.780 | |
| Refined Grains (oz/day) | 3.1 ± 1.1 | 2.4 ± 1.4 | 9.4 ± 68 | 3.6 ± 1.13 | 2.8 ± 1.5 | 8.3 ± 77 | 0.062 | 0.058 |
| Sodium (grams/1000 Kcal) | 2.2 ± 0.44 | 3.46 ± 2.41 | −67 ± 135 | 2.1 ± 0.54 | 2.6 ± 1.5 | −34 ± 104 | 0.536 | 0.316 |
| Added Sugars (% of energy) | 13.4 ± 7.87 | 6.21 ± 6.38 | 50 ± 67 | 12 ± 7. 6 | 8.5 ± 8.1 | 6.0 ± 134 | 0.463 | 0.103 |
| Saturated Fatty Acids (% of energy) | 25 ± 7.7 | 23 ± 10 | −4.7 ± 61 | 33 ± 46 | 25 ± 5.8 | −11 ± 55 | 0.281 | 0.698 |
| Variable | Pre-Surgery | Post-Surgery | p Value | |
|---|---|---|---|---|
| BES score, mean ± SD | 31 ± 7.1 | 10 ± 7.2 | <0.01 | |
| BES category | None | 3 (5) | 48 (80) | <0.01 |
| Moderate | 10 (17) | 9 (15) | ||
| Severe | 47 (78) | 3 (5) | ||
| Food Craving Score, mean ± SD | 50 ± 36 | 30 ± 25 | <0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabbour, J.; Awada, D.; Naim, N.; Al-Jawaldeh, A.; Haidar Ahmad, H.; Mortada, H.; Hoteit, M. Impact of Bariatric Surgery on the Healthy Eating Index, Binge Eating Behavior and Food Craving in a Middle Eastern Population: A Lebanese Experience. Healthcare 2021, 9, 1416. https://doi.org/10.3390/healthcare9111416
Jabbour J, Awada D, Naim N, Al-Jawaldeh A, Haidar Ahmad H, Mortada H, Hoteit M. Impact of Bariatric Surgery on the Healthy Eating Index, Binge Eating Behavior and Food Craving in a Middle Eastern Population: A Lebanese Experience. Healthcare. 2021; 9(11):1416. https://doi.org/10.3390/healthcare9111416
Chicago/Turabian StyleJabbour, Jana, Dalia Awada, Nour Naim, Ayoub Al-Jawaldeh, Houssein Haidar Ahmad, Hussein Mortada, and Maha Hoteit. 2021. "Impact of Bariatric Surgery on the Healthy Eating Index, Binge Eating Behavior and Food Craving in a Middle Eastern Population: A Lebanese Experience" Healthcare 9, no. 11: 1416. https://doi.org/10.3390/healthcare9111416