United States County-level COVID-19 Death Rates and Case Fatality Rates Vary by Region and Urban Status



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
4. Discussion
4.1. Null versus Full Models
4.2. Population Mortality Rates
4.3. Case Fatality Rate
4.4. State Maps
4.5. Other Factors
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lai, C.C.; Wang, C.Y.; Wang, Y.H.; Hsueh, S.C.; Ko, W.C.; Hsueh, P.R. Global epidemiology of coronavirus disease 2019 (COVID-19): Disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status. Int. J. Antimicrob. Agents 2020, 55, 105946. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, S. Comprehensive review of coronavirus disease 2019 (COVID-19). Biomed. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease (COVID-19) Situation Report 171; World Health Organization: Genevaa Switzerland, 2020. [Google Scholar]
- Gold, J.A.W.; Wong, K.K.; Szablewski, C.M.; Patel, P.R.; Rossow, J.; da Silva, J.; Natarajan, P.; Morris, S.B. Characteristics and Clinical Outcomes of Adult Patients Hospitalized with COVID-19—Georgia, March 2020. Morb. Mortal. Wkl. Rep. 2020, 69, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Suleyman, G.; Fadel, R.A.; Malette, K.M.; Hammond, C.; Abdulla, H.; Entz, A.; Demertzis, Z.; Hanna, Z.; Failla, A.; Dagher, C.; et al. Clinical Characteristics and Morbidity Associated With Coronavirus Disease 2019 in a Series of Patients in Metropolitan Detroit. JAMA Netw. Open 2020, 3, e2012270. [Google Scholar] [CrossRef]
- Price-Haywood, E.G.; Burton, J.; Fort, D.; Seoane, L. Hospitalization and Mortality among Black Patients and White Patients with Covid-19. N. Engl. J. Med. 2020, 382, 2534–2543. [Google Scholar] [CrossRef] [PubMed]
- Raisi-Estabragh, Z.; McCracken, C.; Bethell, M.S.; Cooper, J.; Cooper, C.; Caulfield, M.J.; Munroe, P.B.; Harvey, N.C.; Petersen, S.E. Greater risk of severe COVID-19 in Black, Asian and Minority Ethnic populations is not explained by cardiometabolic, socioeconomic or behavioural factors, or by 25(OH)-vitamin D status: Study of 1326 cases from the UK Biobank. J. Public Health (Oxf.) 2020, 42, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Lan, L.; Xu, D.; Ye, G.; Xia, C.; Wang, S.; Li, Y.; Xu, H. Positive RT-PCR Test Results in Patients Recovered From COVID-19. JAMA 2020, 323, 1502–1503. [Google Scholar] [CrossRef] [Green Version]
- Deng, X.; Yang, J.; Wang, W.; Wang, X.; Zhou, J.; Chen, Z.; Li, J.; Chen, Y.; Yan, H.; Zhang, J.; et al. Case fatality risk of the first pandemic wave of novel coronavirus disease 2019 (COVID-19) in China. Clin. Infect. Dis. 2020, in press. [Google Scholar] [CrossRef]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Salj, H.; Kiem, C.T.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; Hoze, N.; Richet, J.; Dubost, C.L.; et al. Estimating the burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef]
- Rajgor, D.D.; Lee, M.H.; Archuleta, S.; Bagdasarian, N.; Quek, S.C. The many estimates of the COVID-19 case fatality rate. Lancet Infect. Dis. 2020, 20, 776–777. [Google Scholar] [CrossRef] [Green Version]
- Basu, A. Estimating The Infection Fatality Rate Among Symptomatic COVID-19 Cases In The United States. Health Aff. (Millwood) 2020, 39. [Google Scholar] [CrossRef] [PubMed]
- Paul, R.; Arif, A.A.; Adeyemi, O.; Ghosh, S.; Han, D. Progression of COVID-19 From Urban to Rural Areas in the United States: A Spatiotemporal Analysis of Prevalence Rates. J. Rural Health 2020. [Google Scholar] [CrossRef] [PubMed]
- CDC. About Rural Health. 2017. Available online: https://www.cdc.gov/ruralhealth/about (accessed on 8 September 2020).
- Souch, J.M.; Cossman, J.S. A Commentary on Rural-Urban Disparities in COVID-19 Testing Rates per 100,000 and Risk Factors. J. Rural Health 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, K.M. An Older Population Increases Estimated COVID-19 Death Rates in Rural America; University of New Hampshire; Carsey School of Public Policy: Durham, NH, USA, 2020. [Google Scholar]
- Lakhani, H.V.; Pillai, S.S.; Zehra, M.; Sharma, I.; Sodhi, K. Systematic Review of Clinical Insights into Novel Coronavirus (CoVID-19) Pandemic: Persisting Challenges in U.S. Rural Population. Int J. Environ. Res. Public Health 2020, 17, 4279. [Google Scholar] [CrossRef]
- Zhang, C.H.; Schwartz, G.G. Spatial Disparities in Coronavirus Incidence and Mortality in the United States: An Ecological Analysis as of May 2020. J. Rural Health 2020, 36, 433–445. [Google Scholar] [CrossRef]
- Khan, S.; McCabe, M.; Krefman, A.; Petito, L.C.; Yang, X.; Kershaw, K.; Pool, L.; Allen, N.B. A County-Level Susceptibility Index and Coronavirus Disease 2019 Mortality in the United States: A Socioecological Study. medRxiv 2020. [Google Scholar] [CrossRef]
- New York Times COVID-19 Data. Available online: https://github.com/nytimes/covid-19-data (accessed on 8 September 2020).
- USDA Rural Urban Continuum Codes. Available online: https://www.ers.usda.gov/data-products/rural-urban-continuum-codes.aspx (accessed on 8 September 2020).
- American Community Survey. 2018. Available online: https://www.census.gov/programs-surveys/acs (accessed on 8 September 2020).
- Definitive Healthcare USA Hospital Beds. Available online: https://coronavirus-resources.esri.com/datasets/definitivehc::definitive-healthcare-usa-hospital-beds?geometry=13.007%2C-16.820%2C-37.969%2C72.123 (accessed on 8 September 2020).
- Sng, J.; Koh, D.; Siong, W.C.; Choo, T.B. Skin cancer trends among Asians living in Singapore from 1968 to 2006. J. Am. Acad. Dermatol. 2009, 61, 426–432. [Google Scholar] [CrossRef]
- Lawless, J.F. Negative Binomial and Mixed Poisson Regression. Can. J. Stat. 1987, 15, 209–225. [Google Scholar] [CrossRef]
- Hoef, J.M.V.; Boveng, P.L. Quasi-Poisson vs. Negative Binomial Regression: How Should We Model Overdispersed Data? Ecology 2007, 88, 2766–2772. [Google Scholar] [CrossRef] [Green Version]
- Olson, D.R.; Huynh, M.; Fine, A.; Baumgartner, J.; Castro, A.; Chan, H.T.; Daskalakis, D.; Devinney, K.; Guerra, K.; Harper, S.; et al. Preliminary Estimate of Excess Mortality During the COVID-19 Outbreak—New York City, 11 March–2 May. Morb. Mortal. Wkl. Rep. 2020, 69, 6303–6305. [Google Scholar]
- Alsan, M.; Stantcheva, S.; Yang, D.; Cutler, D. Disparities in Coronavirus 2019 Reported Incidence, Knowledge, and Behavior Among US Adults. JAMA Netw. Open 2020, 3, e2012403. [Google Scholar] [CrossRef]
- Wu, X.; Nethery, R.C.; Sabath, B.M.; Braun, D.; Dominici, F. Exposure to air pollution and COVID-19 mortality in the United States: A nationwide cross-sectional study. medRxiv. 2020. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Zhao, Y.; Liu, J.; He, X.; Wang, B.; Fu, S.; Yan, J.; Niu, J.; Zhou, J.; Luo, B. Effects of temperature variation and humidity on the death of COVID-19 in Wuhan, China. Sci. Total Environ. 2020, 724, 138226. [Google Scholar] [CrossRef]
- Benedetti, F.; Pachetti, M.; Marini, B.; Ippodrino, R.; Gallo, R.C.; Ciccozzi, M.; Zella, D. Inverse correlation between average monthly high temperatures and COVID-19-related death rates in different geographical areas. J. Transl. Med. 2020, 18, 251. [Google Scholar] [CrossRef] [PubMed]
- Mathews, J.D.; McBryde, E.S.; McVernon, J.; Pallaghy, P.K.; McCaw, J.M. Prior immunity helps to explain wave-like behaviour of pandemic influenza in 1918–9. BMC Infect. Dis. 2010, 10, 128. [Google Scholar] [CrossRef] [Green Version]
- Le Bert, N.; Tan, A.T.; Kunasegaran, K.; Tham, C.Y.L.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 2020, 584, 457–462. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total US | Midwest | Northeast | Southeast | Southwest | West | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Mean | Median | Mean | Median | Mean | Median | Mean | Median | Mean | Median | |
| Demographic | ||||||||||||
| % White | 83.1 | 89.7 | 91.4 | 94.7 | 85.3 | 91.2 | 74.8 | 78.8 | 81.3 | 83.5 | 83.9 | 89.8 |
| % Black | 9.1 | 2.3 | 2.6 | 0.9 | 7.1 | 3.3 | 20.3 | 14.2 | 5.2 | 2.9 | 1.3 | 0.7 |
| % Hispanic | 9.3 | 4.1 | 4.6 | 2.8 | 6.8 | 3.8 | 5.0 | 3.2 | 30.6 | 23.5 | 14.4 | 9.4 |
| Sex ratio | 100.9 | 98.5 | 100.9 | 99.7 | 99.1 | 97.1 | 98.8 | 96.2 | 103.8 | 99.4 | 104.8 | 101.6 |
| Age | 41.3 | 41.2 | 42.0 | 41.9 | 42.5 | 42.5 | 41.1 | 41.0 | 39.4 | 39.0 | 41.1 | 40.2 |
| Socioeconomic | ||||||||||||
| Family size | 3.1 | 3.0 | 3.0 | 2.9 | 3.0 | 3.0 | 3.1 | 3.1 | 3.3 | 3.2 | 3.2 | 3.1 |
| Income | 51,557 | 49,886 | 53,508 | 52,558 | 63,285 | 59,114 | 45,620 | 42,621 | 49,727 | 48,331 | 56,827 | 53,311 |
| % insured | 89.9 | 90.8 | 92.2 | 93.3 | 94.0 | 94.5 | 89.1 | 89.2 | 83.9 | 84.3 | 89.3 | 90.5 |
| % in poverty | 11.2 | 10.3 | 8.8 | 8.2 | 8.2 | 8.0 | 14.5 | 13.7 | 12.5 | 11.8 | 9.5 | 9.0 |
| Hospital | ||||||||||||
| Bed number | 305.2 | 42.0 | 205.7 | 25.0 | 813.4 | 237.0 | 251.9 | 55.0 | 314.9 | 25.0 | 389.5 | 30.0 |
| Bed utilization | 0.3 | 0.3 | 0.3 | 0.3 | 0.5 | 0.5 | 0.3 | 0.3 | 0.2 | 0.2 | 0.3 | 0.3 |
| Ventilator number | 2.0 | 2.0 | 1.5 | 1.0 | 3.7 | 3.0 | 2.3 | 2.0 | 1.4 | 1.0 | 1.7 | 1.5 |
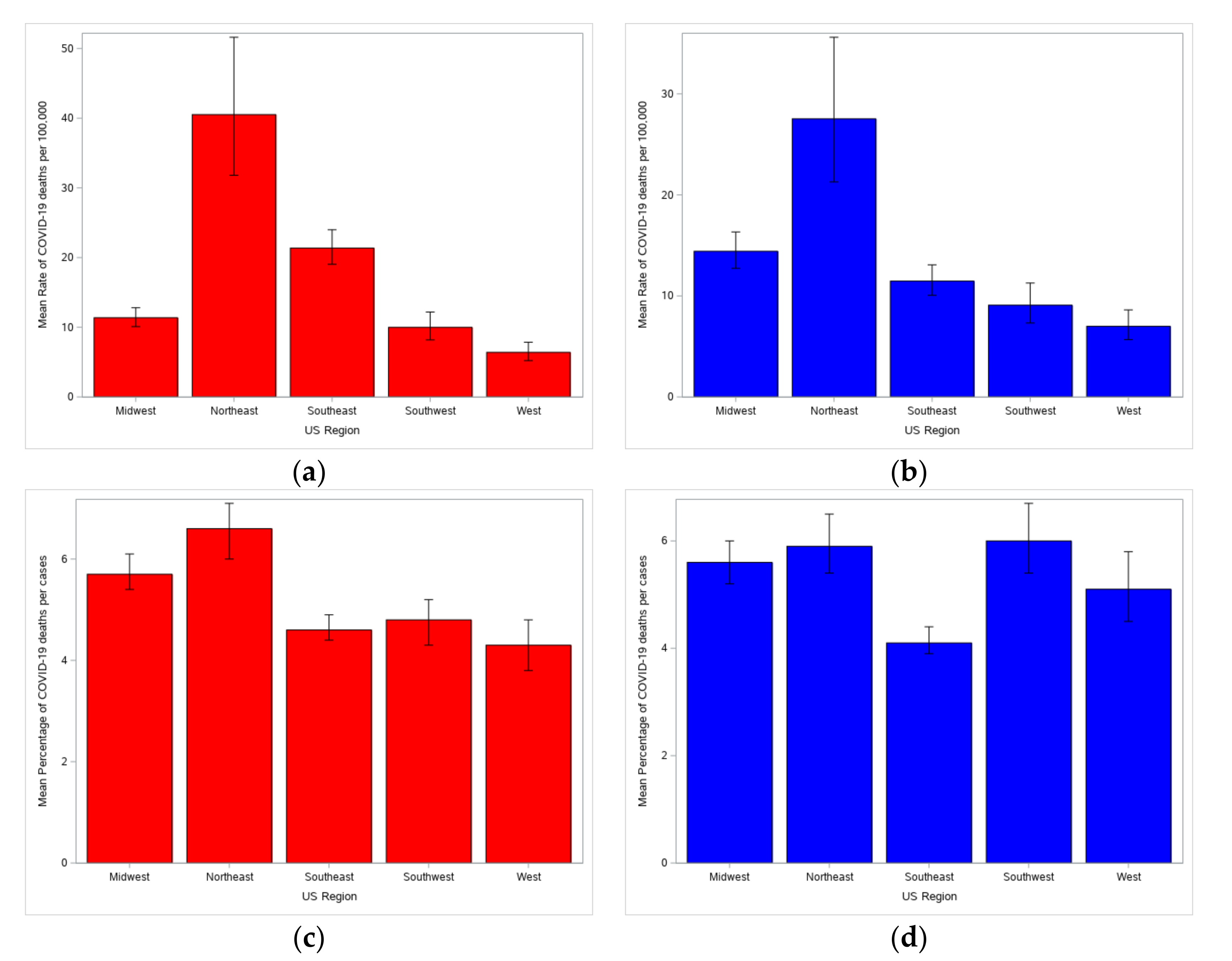
| a. Model-corrected mean mortality rate per 100,000 mean and case fatality rate percentage (CFR %) by US region. Confidence Intervals (CI) are 95%. | ||||||
| Predictor Variable | Mean Mortality Rate per 100,000 | CFR % | ||||
| US Region | Estimate | Lower CI | Upper CI | Estimate | Lower CI | Upper CI |
| Midwest | 14.4 | 12.7 | 16.3 | 5.6% | 5.2 | 6.0 |
| Northeast | 27.5 | 21.3 | 35.6 | 5.9% | 5.4 | 6.5 |
| Southeast | 11.5 | 10.1 | 13.1 | 4.1% | 3.9 | 4.1 |
| Southwest | 9.1 | 7.3 | 11.3 | 6.0% | 5.4 | 6.7 |
| West | 7.0 | 5.7 | 8.6 | 5.1% | 4.5 | 5.8 |
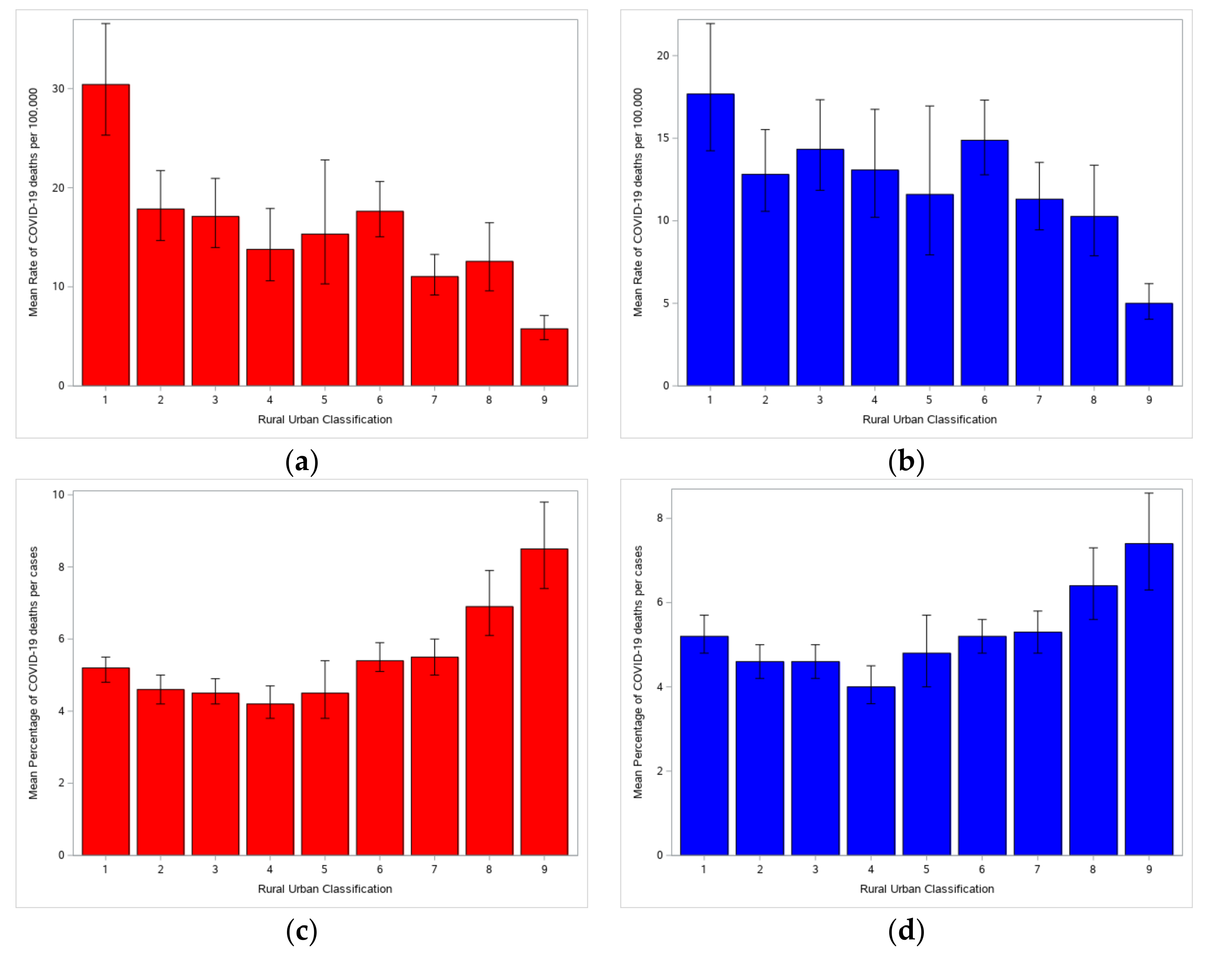
| b. Model-corrected mean mortality rate per 100,000 mean and case fatality rate percentage (CFR %) by Rural-Urban Classification. Confidence Intervals (CI) are 95%. | ||||||
| Predictor Variable | Mean Mortality Rate per 100,000 | CFR % | ||||
| Rural-Urban Code | Estimate | Lower CI | Upper CI | Estimate | Lower CI | Upper CI |
| 1 | 17.7 | 14.2 | 21.9 | 5.2% | 4.8 | 5.7 |
| 2 | 12.8 | 10.6 | 15.5 | 4.6% | 4.2 | 5.0 |
| 3 | 14.3 | 11.8 | 17.3 | 4.6% | 4.2 | 5.0 |
| 4 | 13.1 | 10.2 | 16.7 | 4.0% | 3.6 | 4.5 |
| 5 | 11.6 | 7.9 | 17.0 | 4.8% | 4.0 | 5.7 |
| 6 | 14.9 | 12.8 | 17.3 | 5.2% | 4.8 | 5.6 |
| 7 | 11.3 | 9.5 | 13.5 | 5.3% | 4.8 | 5.8 |
| 8 | 10.3 | 7.9 | 13.4 | 6.4% | 5.6 | 7.3 |
| 9 | 5.0 | 4.0 | 6.2 | 7.4% | 6.3 | 8.76). |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, R.; Williamson, M.; Hamid, M.A.; Ashraf, N. United States County-level COVID-19 Death Rates and Case Fatality Rates Vary by Region and Urban Status. Healthcare 2020, 8, 330. https://doi.org/10.3390/healthcare8030330
Ahmed R, Williamson M, Hamid MA, Ashraf N. United States County-level COVID-19 Death Rates and Case Fatality Rates Vary by Region and Urban Status. Healthcare. 2020; 8(3):330. https://doi.org/10.3390/healthcare8030330
Chicago/Turabian StyleAhmed, Rashid, Mark Williamson, Muhammad Akhter Hamid, and Naila Ashraf. 2020. "United States County-level COVID-19 Death Rates and Case Fatality Rates Vary by Region and Urban Status" Healthcare 8, no. 3: 330. https://doi.org/10.3390/healthcare8030330