Personality, Healthcare Use and Costs—A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Analysis
2.3. Quality Assessment
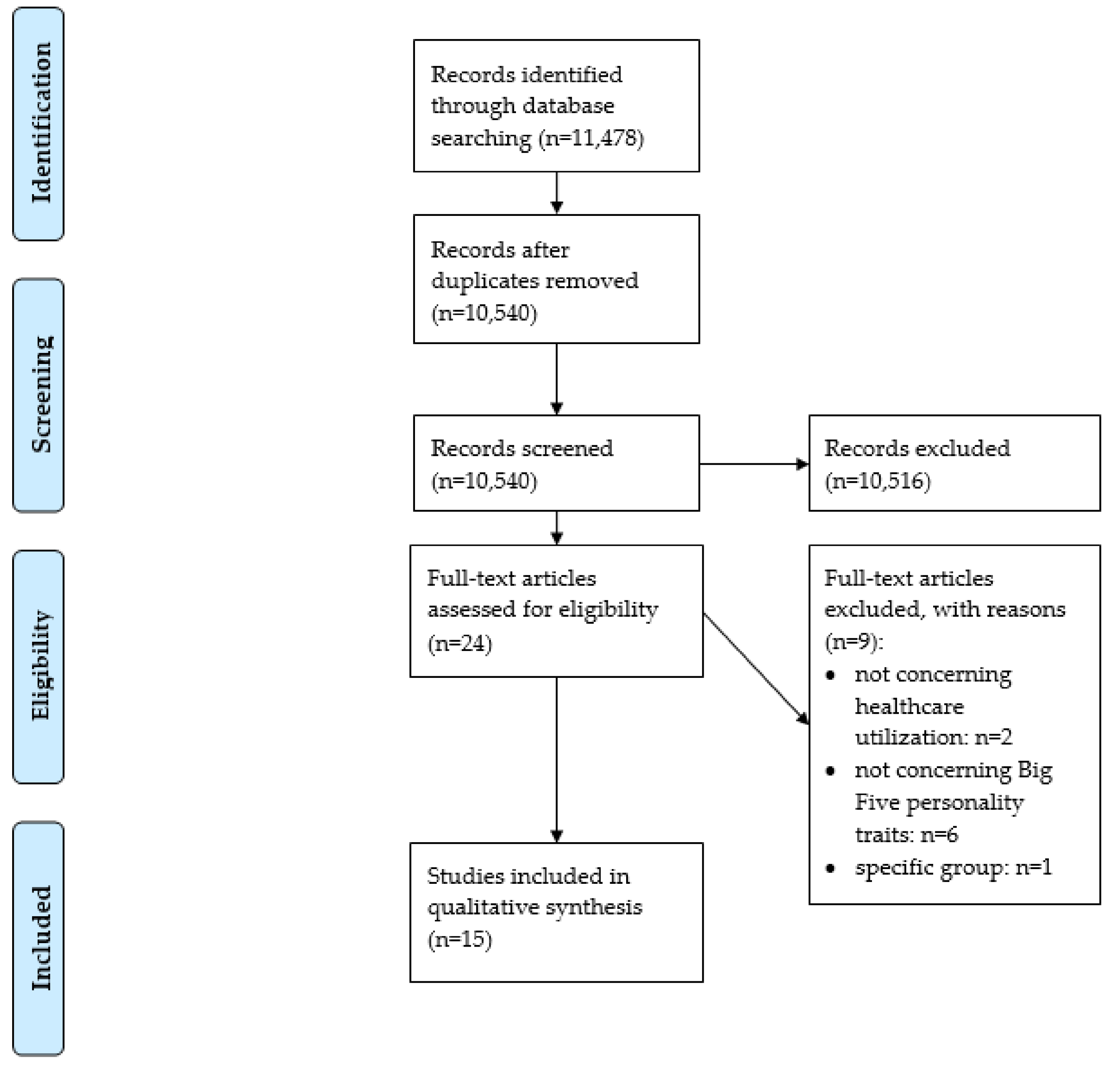
3. Results
3.1. Overview: Included Studies
3.2. Extraversion and HCU
3.3. Agreeableness and HCU
3.4. Conscientiousness and HCU
3.5. Neuroticism and HCU or Costs
3.6. Openness to Experience and HCU
3.7. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethics Statement
References
- Andersen, R.; Newman, J.F. Societal and Individual Determinants of Medical Care Utilization in the United States. Milbank Mem. Fund Q. Health Soc. 1973, 51, 95–124. [Google Scholar] [CrossRef] [Green Version]
- Flennert, M.; König, H.-H.; Hajek, A. The Association between Voluntary Work and Health Care Use among Older Adults in Germany. BMC Health Serv. Res. 2019, 19, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajek, A.; König, H.-H. Meaning in Life and Health Care Use: Findings from a Nationally Representative Study of Older Adults in Germany. BMC Geriatr. 2019, 19, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Babitsch, B.; Gohl, D.; Von Lengerke, T. Re-Revisiting Andersen’s Behavioral Model of Health Services Use: A Systematic Review of Studies from 1998–2011. GMS Psycho Soc. Med. 2012, 9, 9. [Google Scholar]
- Welzel, F.D.; Stein, J.; Hajek, A.; König, H.-H.; Riedel-Heller, S.G. Frequent Attenders in Late Life in Primary Care: A Systematic Review of European Studies. BMC Fam. Pract. 2017, 18, 104. [Google Scholar] [CrossRef]
- Friedman, B.; Veazie, P.J.; Chapman, B.P.; Manning, W.G.; Duberstein, P. Is Personality Associated with Health Care Use by Older Adults? Milbank Q. 2013, 91, 491–527. [Google Scholar] [CrossRef] [Green Version]
- Hajek, A.; Bock, J.-O.; König, H.-H. The Role of Personality in Health Care Use: Results of a Population-Based Longitudinal Study in Germany. PLoS ONE 2017, 12, e0181716. [Google Scholar] [CrossRef] [Green Version]
- Ashton, M.C.; Lee, K.; Perugini, M.; Szarota, P.; De Vries, R.E.; Di Blas, L.; Boies, K.; De Raad, B. A Six-Factor Structure of Personality-Descriptive Adjectives: Solutions from Psycholexical Studies in Seven Languages. J. Pers. Soc. Psychol. 2004, 86, 356–366. [Google Scholar] [CrossRef]
- Goldberg, L.R. The Structure of Phenotypic Personality Traits. Am. Psychol. 1993, 48, 26–34. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.J.; Ghersi, D.; Liberati, A.; Petticrew, M.P.; Shekelle, P.; Stewart, L.; the PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Stuhldreher, N.; König, H.-H.; Konnopka, A.; Wild, B.; Herzog, W.; Zipfel, S.; Löwe, B. Cost-of-illness studies and cost?effectiveness analyses in eating disorders: A systematic review. Int. J. Eat. Disord. 2012, 45, 476–491. [Google Scholar] [CrossRef] [PubMed]
- Hohls, J.K.; König, H.-H.; Raynik, Y.I.; Hajek, A. A Systematic Review of the Association of Anxiety with Health Care Utilization and Costs in People Aged 65 Years and Older. J. Affect. Disord. 2018, 232, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, U.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, B.P.; Shah, M.; Friedman, B.; Drayer, R.; Duberstein, P.; Lyness, J.M. Personality Traits Predict Emergency Department Utilization Over 3 Years in Older Patients. Am. J. Geriatr. Psychiatry 2009, 17, 526–535. [Google Scholar] [CrossRef] [Green Version]
- Honda, K.; Jacobson, J.S. Use of Complementary and Alternative Medicine among United States Adults: The Influences of Personality, Coping Strategies, and Social Support. Prev. Med. 2005, 40, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Boeft, M.D.; Twisk, J.W.R.; Terluin, B.; Penninx, B.W.J.H.; Van Marwijk, H.; Numans, M.E.; Van Der Wouden, J.C.; Van Der Horst, H. The Association between Medically Unexplained Physical Symptoms and Health Care Use over Two Years and the Influence of Depressive and Anxiety Disorders and Personality Traits: A Longitudinal Study. BMC Health Serv. Res. 2016, 16, 100. [Google Scholar] [CrossRef] [Green Version]
- Sirois, F.M.; Purc-Stephenson, R.J. Personality and Consultations with Complementary and Alternative Medicine Practitioners: A Five-Factor Model Investigation of the Degree of Use and Motives. J. Altern. Complement. Med. 2008, 14, 1151–1158. [Google Scholar] [CrossRef]
- Westhead, J. Frequent Attenders in General Practice: Medical, Psychological and Social Characteristics. J. R. Coll. Gen. Pract. 1985, 35, 337–340. [Google Scholar]
- Tomenson, B.; McBeth, J.; Chew-Graham, C.A.; Macfarlane, G.J.; Davies, I.; Jackson, J.; Littlewood, A.; Creed, F.H. Somatization and Health Anxiety as Predictors of Health Care Use. Psychosom. Med. 2012, 74, 656–664. [Google Scholar] [CrossRef]
- Kennedy, B.D.; Aldwin, C.M.; Bossé, R.; Douglass, C.W.; Chauncey, H.H. Special Concern: Personality and Dental Care Utilization: Findings from the VA Longitudinal Study. Spéc. Care Dent. 1990, 10, 102–106. [Google Scholar] [CrossRef]
- Van Hemert, A.M.; Bakker, C.H.; Vandenbroucke, J.P.; Valkenburg, H.A. Psychologic Distress as a Longterm Predictor of Medical Utilisation. Int. J. Psychiatry Med. 1993, 23, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Wikehult, B.; Willebrand, M.; Kildal, M.; Lannerstam, K.; Fugl-Meyer, A.; Ekselius, L.; Gerdin, B. Use of Healthcare a Long Time after Severe Burn Injury; Relation to Perceived Health and Personality Characteristics. Disabil. Rehabil. 2005, 27, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Smit, F.; Penninx, B.W.J.H.; De Graaf, R.; Have, M.T.; Beekman, A.T.F. Economic Costs of Neuroticism. Arch. Gen. Psychiatry 2010, 67, 1086–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metin, Z.G.; Karadas, C.; Ozdemir, L. Usage and Attitudes Related to Complementary and Alternative Medicine among Turkish Academicians on the Basis of the Five-Factor Model of Personality: A Multi-centered Study. Complement. Ther. Med. 2019, 44, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Hakulinen, C.; Elovainio, M.; Batty, G.D.; Virtanen, M.; Kivimäki, M.; Jokela, M. Personality and Alcohol Consumption: Pooled Analysis of 72,949 Adults from Eight Cohort Studies. Drug Alcohol Depend. 2015, 151, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Hakulinen, C.; Hintsanen, M.; Munafo, M.R.; Virtanen, M.; Kivimäki, M.; Batty, G.D.; Jokela, M. Personality and Smoking: Individual-Participant Meta-Analysis of Nine Cohort Studies. Addiction 2015, 110, 1844–1852. [Google Scholar] [CrossRef]
- Marusic, M.; Musek, M.; Marusic, A.; Musek, J.; Gudjonsson, G. Injury Proneness and Personality. Nord. J. Psychiatry 2001, 55, 157–161. [Google Scholar] [CrossRef]
- Takahashi, Y.; Edmonds, G.W.; Jackson, J.J.; Roberts, B.W. Longitudinal Correlated Changes in Conscientiousness, Preventative Health-Related Behaviors, and Self-Perceived Physical Health. J. Pers. 2013, 81, 417–427. [Google Scholar] [CrossRef] [Green Version]
- Aschwanden, D.; Gerend, M.A.; Luchetti, M.; Stephan, Y.; Sutin, A.R.; Terracciano, A. Personality Traits and Preventive Cancer Screenings in the Health Retirement Study. Prev. Med. 2019, 126, 105763. [Google Scholar] [CrossRef]
- Bogg, T.; Roberts, B.W. Conscientiousness and Health-Related Behaviors: A Meta-Analysis of the Leading Behavioral Contributors to Mortality. Psychol. Bull. 2004, 130, 887–919. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, R.D.; Hoven, C.W.; Lyons, J.S.; Stein, M.B. Mental Health Service Utilization in the United States. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Hopwood, C.J.; Quigley, B.D.; Grilo, C.M.; Sanislow, C.A.; McGlashan, T.H.; Yen, S.; Shea, M.T.; Zanarini, M.C.; Gunderson, J.G.; Skodol, A.E.; et al. Personality Traits and Mental Health Treatment Utilization. Pers. Ment. Health 2008, 2, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhandari, A.; Wagner, T. Self-Reported Utilization of Health Care Services: Improving Measurement and Accuracy. Med. Care Res. Rev. 2006, 63, 217–235. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M. Systematic Reviews of Observational Studies. Syst. Rev. Health Care 2008, 211–227. [Google Scholar] [CrossRef]
- Mueller, M.; D’Addario, M.; Egger, M.; Cevallos, M.; Dekkers, O.M.; Mugglin, C.; Scott, P. Methods to Systematically Review and Meta-Analyse Observational Studies: A Systematic Scoping Review of Recommendations. Bmc Med. Res. Methodol. 2018, 18, 44. [Google Scholar] [CrossRef] [Green Version]
- Hajek, A.; König, H.-H. Locus of Control and Frequency of Physician Visits: Results of a Population-Based Longitudinal Study in Germany. Br. J. Health Psychol. 2017, 22, 414–428. [Google Scholar] [CrossRef]


{kind=link}
| # | Search Term |
|---|---|
| #1 | Personality [Title/Abstract] |
| #2 | Big five [Title/Abstract] |
| #3 | #1 OR #2 |
| #4 | Health care |
| #5 | Health service * |
| #6 | #4 OR #5 |
| #7 | Use |
| #8 | Utili * |
| #9 | #7 OR #8 |
| #10 | #6 AND #9 |
| #11 | cost |
| #12 | Expense * |
| #13 | Expenditure * |
| #14 | Economic * |
| #15 | #11 OR #12 OR #13 OR #14 |
| #16 | #10 OR #15 |
| #17 | #3 AND #16 |
| First Author | Country | Assessment of Personality | Assessment of Healthcare Utilization | Study Type | Sample Description | Sample Size | Age | Proportion of Women (in %) | Results |
|---|---|---|---|---|---|---|---|---|---|
| Andersen (2012) | Denmark | Neuroticism: Mini International Personality Item Pool—Five-Factor Model measure (five items) | Visits to the general practitioner (duration: 1.5 years) | Cross-sectional | Representative (not specified) population | n = 5068 | 17–65 | 55.5% | Ordinal logistic regression revealed that people with neuroticism had more visits (OR = 1.2, 95% CI: 1.0–1.4) to the general practitioner. |
| M = 46.1 | |||||||||
| SD = 12.9 | |||||||||
| Chapman (2009) | United States of America | NEO Five-Factor Inventory (60 items) | Emergency department utilization (duration: three years) | Longitudinal | Recruited in primary care clinics | Baseline | 65–94 | 63.8% | Generalized linear mixed models revealed that a one sample deviation * (which means 50th versus 83rd population percentile) increase in extroversion increased the odds of emergency department utilization by 51% (OR = 1.51, 95% CI: 1.03–2.21). An equal decrease in agreeableness (which means 50th versus 17th population percentile) increased the odds by 54% (OR = 1.54, 95% CI: 1.05–2.22). |
| n = 747 | M = 75.2 | ||||||||
| SD = 6.6 | |||||||||
| Cuijpers (2010) | Netherlands | Neuroticism scale from the Amsterdam Biographic Inventory (14 items) | Costs: health service uptake in primary and secondary mental healthcare, out-of-pocket costs, and production losses | Cross-sectional | Netherlands Mental Health Survey and Incidence Study | n = 5504 | 18–65 | 49.1% | Total per capita excess costs were $12,362 per year (reference year: 2007) in the 5% highest scorers of neuroticism (top 10%: $8243; top 25%: $5572). Total excess costs of neuroticism per 1 million inhabitants resulting from the 25% highest scorers was $1.393 billion (top 10%: $824.3 million; top 5%: $618.1 million). |
| M = 41.1 | |||||||||
| SD = 11.9 | |||||||||
| den Boeft (2016) | Netherlands | NEO Five-Factor Inventory (60 items) | Trimbos and iMTA (instituut voor Medische Technology Assessment) questionnaire on costs associated with psychiatric illness | Longitudinal | Netherlands Study of Anxiety and Depression | Baseline | 18–65 | 66.4% | Generalized estimating equations showed that all five personality traits (neuroticism: RR = 1.01, 95% CI: 1.01–1.02; extraversion: RR = 1.02, 95% CI: 1.02–1.02; openness: RR = 1.02, 95% CI: 1.02–1.02; agreeableness: RR = 1.02, 95% CI: 1.02–1.02; conscientiousness: RR = 1.02, 95% CI: 1.02–1.02) are significantly associated with healthcare use. |
| n = 2981 | M = 41.9 | ||||||||
| SD = 13.1 | |||||||||
| Friedman (2013) | United States of America | NEO Five-Factor Inventory (number of items not specified) | Daily use of thirty different services (duration not specified) | Cross-sectional | Recruited for the Medicare Primary and Consumer-Directed Care Demonstration | n = 1074 | 65–100 | 72.7% | Controlling for various need variables from the Andersen Behavioral Model, neuroticism increased the use of any emergency department (β = 0.03, p < 0.001), and any custodial nursing home (β = 0.04, p < 0.05). Agreeableness (β = 0.03, p < 0.05) and conscientiousness (β = −0.05, p < 0.01) were associated with using any custodial nursing home as well. Openness to experience was associated with any custodial home care (β = 0.02, p < 0.05). |
| M = 79.7 | |||||||||
| SD = 7.5 | |||||||||
| Hajek (2017) | Germany | Short version of the Big Five Inventory (15 items) | Hospital stays for at least one night and number of physician visits (duration: three months) | Longitudinal | German Socioeconomic Panel | Baseline | 17–103 | 54.3% | FE Poisson regressions showed that neuroticism was associated with physician visits (β = 0.01, p < 0.001). Furthermore, conditional FE logistic regressions showed that extraversion was associated with the risk of hospitalization (OR = 1.02, p < 0.05). |
| M = 51.6 | |||||||||
| n = 37,185 | SD = 16.7 | ||||||||
| Honda (2005) | United States of America | Big five factor model (25 items) | Use of acupuncture, biofeedback, chiropractic, energy healing, exercise/movement therapy, herbal medicine, high-dose megavitamins, homeopathy, hypnosis, imagery techniques, massage, prayer/spiritual practice, relaxation/mediation, and special diet (duration: twelve months) | Cross-sectional | Midlife development in the United States Survey | n = 3032 | 25–74 | 50.2% among non-users of complementary and alternative medicine; | Logistic regression stated that openness (OR = 1.65, 95% CI: 1.18–2.31) and extraversion (OR = 0.65, 95% CI: 0.46–0.91) were associated with the use of any alternative medicine. |
| (mean age and SD for the total sample not specified) | 62.5% among users of complementary and alternative medicine | ||||||||
| Kennedy (1990) | United States of America | EPI-Q (Eysenck Personality Inventory Questionnaire) (18 items) | Dental utilization as measured by percent restored | Cross-sectional | VA (Veterans Affairs) Dental Longitudinal Study | n = 593 | 28–80 | 0.0% | A plot of neuroticism versus utilization stated that there was a curvilinear association: those scoring lowest and highest on this scale sought less treatment. Linear regressions showed that neuroticism squared was significantly associated with dental utilization (β = −0.3, p = 0.03). |
| M = 47.8 | |||||||||
| SD = 8.1 | |||||||||
| Metin (2019) | Turkey | Ten-Item Personality Inventory (10 items) | Holistic Complementary and Alternative Health Questionnaire | Cross-sectional | Academicians working for three leading universities in Turkey | n = 227 | M = 38.9 SD = 10.4 (age range not specified) | 65.6% | t-tests revealed that openness was positively associated with the use of complementary and alternative healthcare utilization (p = 0.02). |
| Reber (2018) | Germany | Short version of the Big Five Inventory (15 items) | Number of physician visits (duration: three months) | Longitudinal | German Socioeconomic Panel | n = 2140 | In men: | 31.0% | Poisson fixed effects regressions did not show any association for all big five personality domains and the number of physician visits. |
| M = 48.3 years | |||||||||
| SD = 9.4 | |||||||||
| In women: | |||||||||
| M = 46.2 | |||||||||
| SD = 9.3 | |||||||||
| (age range not specified) | |||||||||
| Sirois (2008) | Canada | Big Five Factor Inventory (44 items) | Seven domains of complementary and alternative medicine (duration: one year) | Cross-sectional | Clients of complementary and alternative medicine | n = 184 | 15–86 | 83.2% | Hierarchical multiple regression revealed that agreeableness was associated with a higher use of complementary and alternative medicine (β = 0.21, p < 0.01). |
| M = 41.4 | |||||||||
| SD = 13.7 | |||||||||
| Tomenson (2012) | United Kingdom | Revised NEO Personality Inventory for neuroticism (number of items not specified) | Number of primary care consultations (duration: one year) | Cross-sectional | Random sample of the U.K. adult population | n = 961 | 25–65 | 54.0% | According to the Spearman correlation coefficient, there is a significant positive correlation between neuroticism and primary care consultations (year before baseline: ρ = 0.17, p < 0.001; year after baseline: ρ = 0.12, p = 0.003). |
| M = 47.4 | |||||||||
| SD = 11.6 | |||||||||
| van Hemert (1993) | Netherlands | Dutch Personality Inventory (132 items) | Using any medication daily (duration not specified) | Longitudinal | Data from the Epidemiological Preventive Investigation at Zoetermeer | n = 1167 | 45–64 | 100.0% | Controlling for age and education, logistic regressions showed that the upper quintile concerning neuroticism had higher chances than the lower quintile to use medication (OR = 2.8, 95% CI: 1.8–4.5). |
| M = 53.2 | |||||||||
| SD = 5.7 | |||||||||
| Wikehult (2005) | Sweden | Swedish universities Scales of Personality (91 items) | Receiving healthcare (duration: “currently”) | Cross-sectional | Victims of burn injury | n = 69 | N = 46.1 | 23.2% | Mann–Whitney U tests stated a significant correlation between neuroticism and currently receiving healthcare (p = 0.022). |
| SD = 15.5 | |||||||||
| (range not specified) | |||||||||
| Westhead (1985) | United Kingdom | Eysenck Personality Questionnaire (number of items not specified) | Being a frequent attender (ten percent most frequent attenders in each decade age group for each sex) | Cross-sectional | Practice population | n = 1491 | Mean age, SD, and range not specified | 50.9% | Chi-square tests revealed that mean scores for neuroticism were higher among frequent attenders, both among men (p < 0.05) and women (p < 0.01). |
| First Author (Year) | Type of Study (HCU/COI) | Study Objective | Inclusion and Exclusion Criteria | Cost Description | Comparison Group- or Disorder-Specific Costs | HCU Description | Comparison Group- or Disorder-Specific HCU | Currency | Reference Year | Perspective | Costs from More than One Category | Data Source | Valuation of Costs | Discounting |
| Cuijpers (2010) | COI | ✓ | ✓ | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Andersen (2012) | HCU | ✓ | X | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Chapman (2009) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| den Boeft (2016) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Friedman (2013) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Hajek (2017) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Honda (2005) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Kennedy (1990) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Metin (2019) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Reber (2018) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Sirois (2008) | HCU | ✓ | X | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Tomenson (2012) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| van Hemert (1993) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Westhead (1985) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| Wikehult (2005) | HCU | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | n.a. | n.a. | n.a. | n.a. | ✓ | n.a. | n.a. |
| % of criteria fulfilled by studies | 100 | 86.7 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | |
| First Author (Year) | Missing Data | Statistics | Consideration of Confounders | Sensitivity Analysis | Sample Size (Sub-group) | Demographics | Arithmetic Mean Costs | SD (SE) or CI | Results Discussed with Respect to Other Studies | Results Discussed Regarding Generalizability | Limitations | Conclusion Supported by Data | Conflict of interest/funders | % of Criteria Fulfilled by Study |
| Cuijpers (2010) | X | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 95.8 |
| Andersen (2012) | X | ✓ | ✓ | ✓ | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 87.5 |
| Chapman (2009) | ✓ | ✓ | ✓ | X | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 93.8 |
| den Boeft (2016) | X | ✓ | ✓ | X | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 87.5 |
| Friedman (2013) | X | ✓ | ✓ | ✓ | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 93.8 |
| Hajek (2017) | X | ✓ | ✓ | ✓ | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 93.8 |
| Honda (2005) | X | ✓ | ✓ | X | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 87.5 |
| Kennedy (1990) | X | ✓ | ✓ | X | ✓ | ✓ | n.a. | n.a. | ✓ | X | ✓ | ✓ | ✓ | 81.3 |
| Metin (2019) | X | ✓ | X | X | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 81.3 |
| Reber (2018) | X | ✓ | ✓ | ✓ | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 93.8 |
| Sirois (2008) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 93.8 |
| Tomenson (2012) | X | ✓ | ✓ | X | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | ✓ | ✓ | ✓ | 87.5 |
| van Hemert (1993) | X | ✓ | ✓ | X | ✓ | ✓ | n.a. | n.a. | ✓ | X | ✓ | ✓ | ✓ | 81.3 |
| Westhead (1985) | X | ✓ | ✓ | X | ✓ | X | n.a. | n.a. | ✓ | X | X | ✓ | X | 62.5 |
| Wikehult (2005) | X | ✓ | ✓ | X | ✓ | ✓ | n.a. | n.a. | ✓ | ✓ | X | ✓ | ✓ | 81.3 |
| % of criteria fulfilled by studies | 13.3 | 100 | 93.3 | 40 | 100 | 93.3 | 100 | 100 | 100 | 80 | 86.7 | 100 | 93.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hajek, A.; Kretzler, B.; König, H.-H. Personality, Healthcare Use and Costs—A Systematic Review. Healthcare 2020, 8, 329. https://doi.org/10.3390/healthcare8030329
Hajek A, Kretzler B, König H-H. Personality, Healthcare Use and Costs—A Systematic Review. Healthcare. 2020; 8(3):329. https://doi.org/10.3390/healthcare8030329
Chicago/Turabian StyleHajek, André, Benedikt Kretzler, and Hans-Helmut König. 2020. "Personality, Healthcare Use and Costs—A Systematic Review" Healthcare 8, no. 3: 329. https://doi.org/10.3390/healthcare8030329