
Neurological Implications of Vitamin B12 Deficiency in Diet: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Employed
2.2. Review Hypotheses
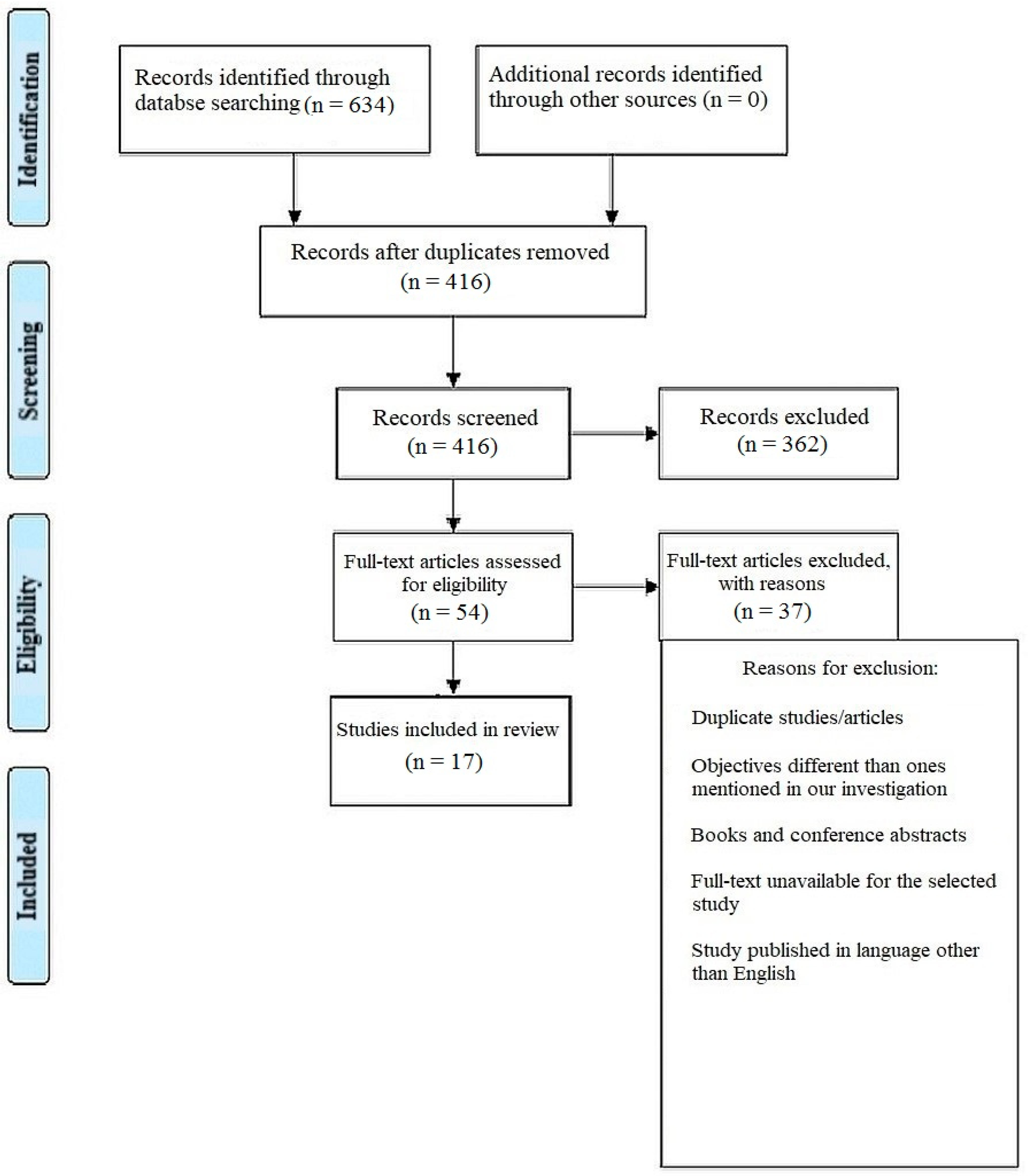
2.3. Study Selection Process
2.4. Inclusion Criterion
2.5. Exclusion Criteria
2.6. Search Strategy
2.7. Data Selection and Coding
2.8. Risk of Bias Assessment
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allen, L.H. Folate and Vitamin B12 status in the Americas. Nutr. Rev. 2004, 62, S29–S33. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.B.F.; Madsen, M.; Storm, T.; Moestrup, S.K.; Andersen, G.R. Structural basis for receptor recognition of Vitamin-B 12–intrinsic factor complexes. Nature 2010, 464, 445. [Google Scholar] [CrossRef] [PubMed]
- Selhub, J.; Jacques, P.F.; Dallal, G.; Choumenkovitch, S.; Rogers, G. The use of blood concentrations of Vitamins and their respective functional indicators to define folate and Vitamin B12 status. Food Nutr. Bull. 2008, 29 (Suppl. S1), S67–S73. [Google Scholar] [CrossRef] [Green Version]
- Black, M.M. Effects of Vitamin B12 and folate deficiency on brain development in children. Food Nutr. Bull. 2008, 29 (Suppl. S1), S126–S131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagnelie, P.C.; van Staveren, W.A.; Vergote, F.J.; Dingjan, P.G.; Van Den Berg, H.; Hautvast, J. Increased risk of Vitamin B-12 and iron deficiency in infants on macrobiotic diets. Am. J. Clin. Nutr. 1989, 50, 818–824. [Google Scholar] [CrossRef]
- Kozyraki, R.; Fyfe, J.; Kristiansen, M.; Gerdes, C.; Jacobsen, C.; Cui, S.; Christensen, E.I.; Aminoff, M.; De La Chapelle, A.; Krahe, R.; et al. The intrinsic factor–Vitamin B 12 receptor, cubilin, is a high-affinity apolipoprotein AI receptor facilitating endocytosis of high-density lipoprotein. Nat. Med. 1999, 5, 656. [Google Scholar] [CrossRef]
- Fyfe, J.C.; Madsen, M.; Højrup, P.; Christensen, E.I.; Tanner, S.M.; de la Chapelle AMoestrup, S.K. The functional cobalamin (Vitamin B12)–intrinsic factor receptor is a novel complex of cubilin and amnionless. Blood 2004, 103, 1573–1579. [Google Scholar] [CrossRef]
- Briani, C.; Dalla Torre, C.; Citton, V.; Manara, R.; Pompanin, S.; Binotto, G.; Adami, F. Cobalamin deficiency: Clinical picture and radiological findings. Nutrients 2013, 5, 4521–4539. [Google Scholar] [CrossRef] [Green Version]
- Nykjaer, A.; Fyfe, J.C.; Kozyraki, R.; Leheste, J.-R.; Jacobsen, C.; Nielsen, M.S.; Moestrup, S.K. Cubilin dysfunction causes abnormal metabolism of the steroid hormone 25 (OH) Vitamin D3. Proc. Natl. Acad. Sci. USA 2001, 98, 13895–13900. [Google Scholar] [CrossRef] [Green Version]
- de Benoist, B. Conclusions of a WHO Technical Consultation on folate and Vitamin B12 deficiencies. Food Nutr. Bull. 2008, 29 (Suppl. S1), S238–S244. [Google Scholar] [CrossRef]
- de Jager, C.A. Critical levels of brain atrophy associated with homocysteine and cognitive decline. Neurobiol. Aging 2014, 35, S35–S39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arya, S.; Kaji, A.H.; Boermeester, M.A. PRISMA Reporting Guidelines for Meta-analyses and Systematic Reviews. JAMA Surg. 2021, 156, 789–790. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arıcan, P.; Bozkurt, O.; Cavusoglu, D.; Gencpınar, P.; Haspolat, S.; Duman, O.; Olgac Dundar, N. Various Neurological Symptoms with Vitamin B12 Deficiency and Posttreatment Evaluation. J. Pediatr. Neurosci. 2020, 15, 365–369. [Google Scholar] [CrossRef]
- Bolaman, Z.; Kadikoylu, G.; Yukselen, V.; Yavasoglu, I.; Barutca, S.; Senturk, T. Oral versus intramuscular cobalamin treatment in megaloblastic anemia: A single-center, prospective, randomized, open-label study. Clin. Ther. 2003, 25, 3124–3134. [Google Scholar] [CrossRef]
- Dangour, A.D.; Allen, E.; Clarke, R.; Elbourne, D.; Fasey, N.; Fletcher, A.E.; Letley, L.; Richards, M.; Whyte, K.; Mills, K.; et al. A randomised controlled trial investigating the effect of Vitamin B12 supplementation on neurological function in healthy older people: The Older People and Enhanced Neurological function (OPEN) study protocol [ISRCTN54195799]. Nutr. J. 2011, 10, 22. [Google Scholar] [CrossRef] [Green Version]
- Dangour, A.D.; Allen, E.; Clarke, R.; Elbourne, D.; Fletcher, A.E.; Letley, L.; Richards, M.; Whyte, K.; Uauy, R.; Mills, K. Effects of Vitamin B-12 supplementation on neurologic and cognitive function in older people: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 102, 639–647. [Google Scholar] [CrossRef] [Green Version]
- de Koning, E.J.; van der Zwaluw, N.L.; van Wijngaarden, J.P.; Sohl, E.; Brouwer-Brolsma, E.M.; van Marwijk, H.W.; Enneman, A.W.; Swart, K.M.; van Dijk, S.C.; Ham, A.C.; et al. Effects of Two-Year Vitamin B12 and Folic Acid Supplementation on Depressive Symptoms and Quality of Life in Older Adults with Elevated Homocysteine Concentrations: Additional Results from the B-PROOF Study, an RCT. Nutrients 2016, 8, 748. [Google Scholar] [CrossRef] [Green Version]
- Eussen, S.J.; de Groot, L.C.; Joosten, L.W.; Bloo, R.J.; Clarke, R.; Ueland, P.M.; Schneede, J.; Blom, H.J.; Hoefnagels, W.H.; van Staveren, W.A. Effect of oral Vitamin B-12 with or without folic acid on cognitive function in older people with mild Vitamin B-12 deficiency: A randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2006, 84, 361–370. [Google Scholar] [CrossRef]
- Farvid, M.S.; Homayouni, F.; Amiri, Z.; Adelmanesh, F. Improving neuropathy scores in type 2 diabetic patients using micronutrients supplementation. Diabetes Res. Clin. Pract. 2011, 93, 86–94. [Google Scholar] [CrossRef]
- Fonseca, V.A.; Lavery, L.A.; Thethi, T.K.; Daoud, Y.; DeSouza, C.; Ovalle, F.; Denham, D.S.; Bottiglieri, T.; Sheehan, P.; Rosenstock, J. Metanx in type 2 diabetes with peripheral neuropathy: A randomized trial. Am. J. Med. 2013, 126, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Franques, J.; Chiche, L.; De Paula, A.M.; Grapperon, A.M.; Attarian, S.; Pouget, J.; Mathis, S. Characteristics of patients with Vitamin B12-responsive neuropathy: A case series with systematic repeated electrophysiological assessment. Neurol. Res. 2019, 41, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Ghumare, S.S.; Chandanwale, A.S.; Jadhav, P.; Arya, S.; Rawat, S.S.; Sankar, S. A study of relationship between Vitamin b12 levels and neurological function in patients with cervical spondylotic myelopathy. Int. J. Orthop. Sci. 2020, 6, 611–617. [Google Scholar] [CrossRef]
- Warendorf, J.K.; van Doormaal, P.T.; Vrancken, A.F.; Verhoeven-Duif, N.M.; van Eijk, R.P.; van den Berg, L.H.; Notermans, N.C. Notermans Clinical relevance of testing for metabolic Vitamin B12 deficiency in patients with polyneuropathy. Nutr. Neurosci. 2022, 25, 2536–2546. [Google Scholar] [CrossRef]
- Lata Kanyal, M.T.; Mujawar, A. Status of Vitamin b12 in type 2 diabetes mellitus patients taking metformin based oral hypoglycemic agent-a cross sectional study. Indian J. Basic Appl. Med. Res. 2019, 1, 18–26. [Google Scholar]
- Kuzminski, A.M.; Del Giacco, E.J.; Allen, R.H.; Stabler, S.P.; Lindenbaum, J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood 1998, 92, 1191–1198. [Google Scholar] [CrossRef]
- Kwok, T.; Wu, Y.; Lee, J.; Lee, R.; Yung, C.Y.; Choi, G.; Lee, V.; Harrison, J.; Lam, L.; Mok, V. A randomized placebo-controlled trial of using B Vitamins to prevent cognitive decline in older mild cognitive impairment patients. Clin. Nutr. 2020, 39, 2399–2405. [Google Scholar] [CrossRef] [Green Version]
- Markun, S.; Gravestock, I.; Jäger, L.; Rosemann, T.; Pichierri, G.; Burgstaller, J.M. Effects of Vitamin B12 Supplementation on Cognitive Function, Depressive Symptoms, and Fatigue: A Systematic Review, Meta-Analysis, and Meta-Regression. Nutrients 2021, 13, 923. [Google Scholar] [CrossRef]
- Nawaz, A.; Khattak, N.N.; Khan, M.S.; Nangyal, H.; Sabri, S.; Shakir, M. Deficiency of Vitamin B12 and its relation with neurological disorders: A critical review. J. Basic Appl. Zool. 2020, 81, 10. [Google Scholar] [CrossRef]
- Serin, H.M.; Arslan, E.A. Neurological symptoms of Vitamin B12 deficiency: Analysis of pediatric patients. Acta Clin. Croat. 2019, 58, 295–302. [Google Scholar] [CrossRef]
- Yuan, S.; Mason, A.M.; Carter, P.; Burgess, S.; Larsson, S.C. Homocysteine, B Vitamins, and cardiovascular disease: A Mendelian randomization study. BMC Med. 2021, 19, 97. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, S.; Ge, B.; Zhou, D.; Li, M.; Li, W.; Ma, F.; Liu, Z.; Ji, Y.; Huang, G. Effects of Folic Acid and Vitamin B12 Supplementation on Cognitive Impairment and Inflammation in Patients with Alzheimer’s Disease: A Randomized, Single-Blinded, Placebo-Controlled Trial. J. Prev. Alzheimers Dis. 2021, 8, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Reischl-Hajiabadi, A.T.; Garbade, S.F.; Feyh, P.; Weiss, K.H.; Mütze, U.; Kölker, S.; Hoffmann, G.F.; Gramer, G. Maternal Vitamin B12 Deficiency Detected by Newborn Screening—Evaluation of Causes and Characteristics. Nutrients 2022, 14, 3767. [Google Scholar] [CrossRef] [PubMed]
- Kurpad, A.V.; Ghosh, S.; Thomas, T.; Bandyopadhyay, S.; Goswami, R.; Gupta, A.; Gupta, P.; John, A.T.; Kapil, U.; Kulkarni, B.; et al. Perspective: When the cure might become the malady: The layering of multiple interventions with mandatory micronutrient fortification of foods in India. Am. J. Clin. Nutr. 2021, 114, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Campana, M.; Löhrs, L.; Strauß, J.; Münz, S.; Oviedo-Salcedo, T.; Fernando, P.; Maurus, I.; Raabe, F.; Moussiopoulou, J.; Eichhorn, P.; et al. Blood-brain-barrier dysfunction and folate and Vitamin B12 levels in first-episode psychosis. Eur. Arch. Psychiatry Clin. Neurosci. 2022; preprint. [Google Scholar] [CrossRef]
- Song, Y.; Quan, M.; Li, T.; Jia, J. Serum Homocysteine, Vitamin B 12, Folate, and Their Association with Mild Cognitive Impairment and Subtypes of Dementia. J. Alzheimers Dis. 2022, 681–691. [Google Scholar] [CrossRef]
- Kimura, J. Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practice, 4th ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Olaso-Gonzalez, G.; Inzitari, M.; Bellelli, G.; Morandi, A.; Barcons, N.; Viña, J. Impact of supplementation with Vitamins B6, B12, and/or folic acid on the reduction of homocysteine levels in patients with mild cognitive impairment: A systematic review. IUBMB Life 2022, 74, 74–84. [Google Scholar] [CrossRef]
- Brenowitz, W.D.; Robbins, N.M.; Strotmeyer, E.S.; Yaffe, K. Associations of Lower Extremity Peripheral Nerve Impairment and Risk of Dementia in Black and White Older Adults. Neurology 2022, 98, e1837–e1845. [Google Scholar] [CrossRef]
- Acharya, M.; Jena, S.K. Reference values of dorsal sural sensory nerve action potential: A useful tool to diagnose peripheral neuropathy. Muller J. Med. Sci. Res. 2021, 12, 13–16. [Google Scholar]
- Balk, E.M.; Raman, G.; Tatsioni, A.; Chung, M.; Lau, J.; Rosenberg, I.H. Vitamin B6, B12, and folic acid supplementation and cognitive function: A systematic review of randomized trials. Arch. Intern. Med. 2007, 167, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Macaron, T.; Giudici, K.V.; Bowman, G.L.; Sinclair, A.; Stephan, E.; Vellas, B.; de Souto Barreto, P. Associations of Omega-3 fatty acids with brain morphology and volume in cognitively healthy older adults: A narrative review. Ageing Res. Rev. 2021, 67, 101300. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Bennett, D.; Parish, S.; Lewington, S.; Skeaff, M.; Eussen, S.J.; Lewerin, C.; Stott, D.J.; Armitage, J.; Hankey, G.J.; et al. Effects of homocysteine lowering with B Vitamins on cognitive aging: Meta-analysis of 11 trials with cognitive data on 22,000 individuals. Am. J. Clin. Nutr. 2014, 100, 657–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies Selected | Question and Inclusion | Protocol | Study Design | Comprehensive Search | Study Selection | Data Extraction | Excluded Studies Justification | Included Study Details | Risk of Bias | Funding Sources | Statistical Methods | Risk of Bias in Meta-Analysis | Risk of Bias in Individual Studies | Explanation of Heterogeneity | Publication Bias | Conflict of Interest |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ancan et al., 2020 [14] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Bolaman et al., 2003 [15] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Dangour et al., 2011 [16] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | N/A | Yes | Yes | Yes | Yes |
| Dangour et al., 2015 [17] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| De Koning et al., 2016 [18] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Eussen et al., 2006 [19] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Farvid et al., 2011 [20] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Fonseca et al., 2013 [21] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Franques et al., 2019 [22] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | N/A | Yes | Yes | Yes | Yes |
| Ghumare et al., 2020 [23] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | |
| Janna et al., 2022 [24] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | |
| Kanyal et al., 2019 [25] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Kuzminski et al., 1998 [26] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Kwok et al., 2019 [27] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Markun et al., 2021 [28] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Nawaz et al., 2020 [29] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes | Yes |
| Serin et al., 2019 [30] | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | N/A | Yes | Yes | Yes | Yes | Yes |
| Author and Year of Study | Sample Size; Mean Age | Study Design | Male:Female Ratio | Study Description/Intervention | Study Outcome/Inference |
|---|---|---|---|---|---|
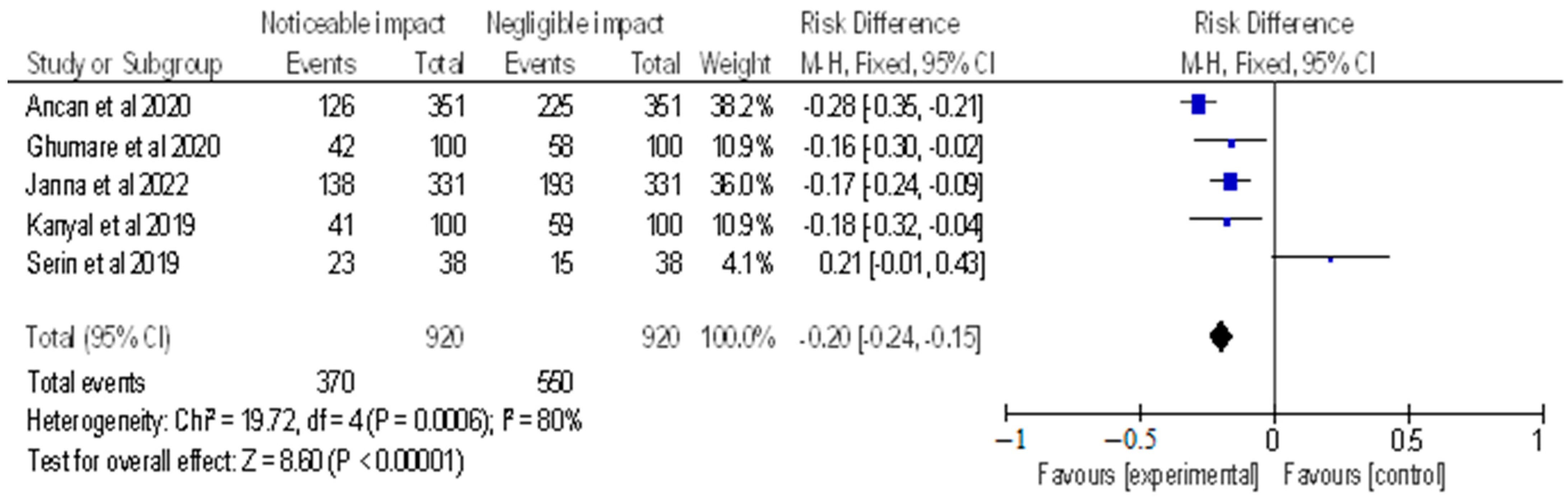
| Ancan et al., 2020 [14] | 351 children; 11.8 years | Retrospective study | 122:229 | The purpose of this study was to assess the clinical response to Vitamin B12 treatment and to report the Vitamin B12 status of patients who were admitted with neurological symptoms. From January 2014 to October 2016, this study focused on children who had Vitamin B12 insufficiency and neurological symptoms. Treatment with intramuscular or oral Vitamin B12 was given to patients whose serum Vitamin B12 levels were less than 300 pg/mL. | To prevent long-term harm, early diagnosis and Vitamin B12 treatment were encouraged. According to the study, those who received Vitamin B12 treatment and had serum Vitamin B12 levels lower than 300 pg/mL experienced a clinical improvement in their neurological symptoms. |
| Bolaman et al., 2003 [15] | 60 patients; ≥16 years | Randomised control trial | 61.5:38.5 | This was a 90-day prospective, randomised, open-label trial carried out at the Adnan Menderes University Research and Practice Hospital’s Division of Hematology and Department of Internal Medicine (Aydin, Turkey). Patients under the age of 16 with megaloblastic anaemia brought on by cobalamin deficiency were randomised to receive either 1000 g of cobalamin PO or 1000 g of cobalamin IM once day for 10 days (IM group). Both treatments were given after 10 days once a week for 4 weeks, and then once a month going forward. Between days 5 and 10 of treatment, patients were checked for the existence of reticulocytosis until it was found. Hematologic parameters were measured on days 0, 10, 30, and 90, and blood Vitamin B12 concentration was measured on days 0 and 90 to determine the success of the treatment. | Treatment with PO cobalamin was equally efficacious as treatment with IM cobalamin in this trial of patients with megaloblastic anaemia brought on by cobalamin deficiency. In addition, PO medication was less expensive and more tolerated as compared to IM treatment. To ascertain the effectiveness of PO cobalamin treatment, the authors felt that additional long-term studies were required due to the limited sample size and short duration of this investigation. |
| Dangour et al., 2011 [16] | 200 individuals; ≥75 years | Randomised double blind control trial | - | The study’s objective was to determine whether crystalline Vitamin B12 dietary supplements would have improved electrophysiological measures of neurological function in elderly individuals who had biochemical evidence of Vitamin B12 deficiency without anaemia. 200 seniors aged 75 years or over who were randomly assigned to receive either a daily oral tablet containing 1 mg of Vitamin B12 or a corresponding placebo tablet participated in a randomised double-blind placebo-controlled experiment. | Observable improvements in electrophysiological markers of peripheral and central neurosensory responses necessary for movement and sensory function were the main outcome evaluated after 12 months. |
| Dangour et al., 2015 [17] | 201 individuals; 80 years | Randomised control trial | 94:107 | A double-blind, randomised, placebo-controlled trial was carried out by the authors in South East England’s seven general practices. Participants in the study received 1 mg of crystalline Vitamin B12 or a corresponding placebo as an oral tablet daily for 12 months if they were older than 80 years old and had a mild Vitamin B12 deficiency (serum Vitamin B12 concentrations: 107–210 pmol/L) without anaemia. Prior to and following treatment, peripheral motor and sensory nerve conduction, central motor conduction, a clinical neurologic examination, and cognitive function were evaluated. | A 177% rise in blood Vitamin B12 concentration (641 pmol/L vs. 231 pmol/L), a 331% increase in serum holotranscobalamin (240 vs. 56 pmol/L), and a 17% decrease in serum homocysteine (14.2 vs. 17.1 mol/L) were all linked with allocation to Vitamin B12 when compared to baseline. The trial’s findings did not corroborate the idea that correcting a mild Vitamin B12 deficiency would have positive impacts on later-life neurologic or cognitive function, even in the absence of anaemia and neurologic or cognitive signs or symptoms. |
| De Koning et al., 2016 [18] | 2919 individuals; ≥65 years | Randomised control trial | 50:50 | This study’s randomised controlled experiment was designed to examine this idea. For two years, participants either received daily doses of Vitamin B12 and folic acid or a placebo. Vitamin D3 was present in both pills. The Geriatric Depression Scale-15 was used to assess depressive symptoms (GDS-15). The SF-12 Mental and Physical component summary scores, the EQ-5D Index score, and the Visual Analogue Scale were used to evaluate health-related quality of life (HR-QoL). | In conclusion, lowering homocysteine concentrations did not reduce depressive symptoms, but it may have had a small positive impact on HR-QoL in older adults with hyperhomocysteinemia who received Vitamin B12 and folic acid supplements for two years. |
| Eussen et al., 2006 [19] | 195 individuals; ≥70 years | Randomised double blind control trial | - | A total of 195 participants in this double-blind, placebo-controlled experiment were randomised to receive Vitamin B12, folic acid, or a placebo for a period of 24 weeks. Methylmalonic acid, total homocysteine (tHcy), and holotranscobalamin (holoTC) concentrations were measured before and after 12 and 24 weeks of treatment to determine the Vitamin B12 status. An thorough neuropsychological test battery that covered the domains of attention, construction, sensomotor speed, memory, and executive function was used to compare cognitive function before and after 24 weeks of treatment. | After receiving treatment, the placebo group’s Vitamin B12 status did not significantly change; however, oral Vitamin B12 supplementation was able to treat mild Vitamin B12 deficiency. Supplementation with Vitamin B12 and folic acid raised red blood cell folate levels and decreased tHcy levels by 36%. The placebo group showed a greater improvement in memory than the group receiving just Vitamin B12. No improvement in other cognitive domains was observed with either Vitamin B12 supplementation alone or in conjunction with folic acid. |
| Farvid et al., 2011 [20] | 67 patients | Randomised double blind control trial | - | Some 75 patients with type 2 diabetes were divided into three treatment groups in this randomised, double-blind, placebo-controlled clinical research. Each group received one of the following daily supplements for four months: Group MVB contains both of the aforementioned mineral and Vitamin supplements along with Vitamin B1 (10 mg), B2 (10 mg), B6 (10 mg), biotin (200 g), B12 (10 g), and folic acid (1 mg); Group P contains a placebo. Group MV contains zinc (20 mg), magnesium (250 mg), Vitamin C (200 mg), and Vitamin E (100 mg). | After 4 months, neuropathic symptoms as measured by the MNSI questionnaire decreased in the group MVB from 3.45 to 0.64, the group MV from 3.96 to 1.0, and the placebo group from 2.54 to 1.95. After four months of supplementation, there was no discernible difference between the three treatment groups on MNSI exams. Patients in the MV and MVB groups did not exhibit any differences in electrophysiological measurements, capillary blood flow, or glycemic management during the course of the 4-month treatment period in comparison to the placebo group. |
| Fonseca et al., 2013 [21] | 214 patients | Randomised double blind control trial | A total of 214 patients with type 2 diabetes and neuropathy (baseline vibration perception threshold [VPT]: 25–45 volts) participated in this multicentre, randomised, double-blind, placebo-controlled trial. Patients were randomised to receive either L-methylfolate calcium 3 mg, methylcobalamin 2 mg, and pyridoxal-5′-phosphate 35 mg for 24 weeks of treatment, or a placebo. The effect on VPT was the main outcome. Other secondary endpoints were plasma levels of folate, Vitamins B(6) and B(12), methylmalonic acid (MMA), homocysteine, and the Neuropathy Total Symptom Score (NTSS-6) and Short Form 36 (SF-36). | In the short term, L-methylfolate, methylcobalamin, and pyridoxal-5′-phosphate (LMF-MC-PLP; brand name Metanx; Pamlab LLC, Covington, La) appears to be a safe and efficient treatment for reducing peripheral neuropathy symptoms. The trial period may have been too brief to demonstrate an effect on VPT, hence the authors argued for more extensive long-term trials. | |
| Franques et al., 2019 [22] | 9 patients | Randomised control trial | - | At a hospital, a 3-year retrospective analysis of patients with B12-responsive neuropathy was carried out. The inclusion criteria were electrophysiological research (nerve conduction study) confirmation of neuropathy and improvement of at least 1 point on the overall Overall Neuropathy Limitations Scale following Vitamin B12 therapy. | There were nine patients found. Only four people had low serum B12 levels. Five patients had only sensory neuronopathy, compared to four who had sensorimotor (predominantly sensory) axonal polyneuropathy. Six improved after taking B12 supplements in less than a month. |
| Ghumare et al., 2020 [23] | 100 individuals; 59.32 years | Observational cross-sectional study | 61:39 | The goal of the current investigation was to determine whether cervical spondylotic myelopathy (CSM) and VB12 insufficiency are related. In our study, 100 CSM patients were examined for VB12 deficiency co-relation. To determine a correlation between VB12 insufficiency and severity of symptoms, demographic data, clinical, radiographic, and laboratory examinations were conducted. | The C5-C6 level (42%) had the highest level of participation, followed by the C4-C5 level (28%) and the C6-C7 level (20%). Motor weakness was noted in 50% of cases, whereas sensory abnormalities were present in 61%. In 47% of instances, VB12 insufficiency was found to be prevalent. 40% of level 1 cord compression cases and 54.1% and 53.8% of level 2 and 3 cord compression cases, respectively, were found to have VB12 deficiencies. |
| Janna et al., 2022 [24] | 331 patients; 63 years | Retrospective cohort study | 71:29 | Measurements were made of Vitamin B12, methylmalonic acid (MMA), and homocysteine (Hcy) in a retrospective cohort analysis of patients with polyneuropathy. To determine which was most closely associated with Vitamin B12, Hcy or MMA were examined as covariates in linear regression models with Vitamin B12 as the dependent variable. Using logistic regression with elevated metabolites as the dependent variable and Vitamin B12 as the covariate, the threshold Vitamin B12 values for metabolic insufficiency (characterised as elevated metabolites) were established. 42 patients underwent a structured interview to gauge their reaction to Vitamin B12 administration. | B12 was the best Vitamin to link to MMA., and the authors discovered 90% sensitivity at a Vitamin B12 threshold level of 264 pmol/L (358 pg/mL) and 95% sensitivity at 304 pmol/L (412 pg/mL) using increased MMA as a marker for metabolic deficit. Patients reported stabilisation after supplementation in 24% of cases and improvements in 19%. A metabolic or absolute deficit (elevated MMA and Vitamin B12 148 pmol/L) was seen in 88% of patients who improved and 90% of patients who stabilised. |
| Kanyal et al., 2019 [25] | 100 patients; ≥30 years | Cross-sectional study | 62:38 | This study’s goal was to determine the Vitamin B12 status of T2DM patients using metformin. 100 T2DM patients in total are present at the Dr. Prabhakar Kore Charitable Hospital at KLE. HbA1c and serum Vitamin B12 levels were both calculated. | According to the findings of the current investigation, metformin-induced Vitamin B12 deficiency caused neurologic impairment with symptoms of peripheral neuropathy that may also be classified as diabetic neuropathy. The researchers also found that screening for a subclinical diagnosis of Vitamin B12 insufficiency would be needed at six months or yearly in diabetic patients on metformin therapy. |
| Kuzminski et al., 1998 [26] | 33 patients; 43–92 years | Randomised control trial | 2:1 | Some 38 patients with recently discovered cobalamin deficiency were randomly randomised to receive cyanocobalamin as either 1 mg intramuscularly on days 1, 3, 7, 10, 14, 21, 30, 60, and 90, or 2 mg orally once day for 120 days. Hematologic and neurologic improvement as well as changes in serum levels of cobalamin (normal, 200 to 900 pg/mL), methylmalonic acid (normal, 73 to 271 nmol/L), and homocysteine (normal, 5.1 to 13.9 mmol/L) were used to assess the efficacy of the treatment. | When treating cobalamin deficiency, 2 mg of cyanocobalamin taken orally once a day was just as beneficial as 1 mg given intramuscularly once a month—and may even be more so. |
| Kwok et al., 2019 [27] | 279 individuals; ≥65 years | Randomised control trial | 59.5:40.5 | A total of 279 outpatients with moderate cognitive impairment (MCI) who were 65 years old and had serum homocysteine levels of 10.0 mmol/L were randomly randomised to consume two placebo tablets for 24 months or methylcobalamin 500 mg and folic acid 400 mg once daily. Every subject underwent follow-up at intervals of 12 months. The main result was cognitive decline as measured by a rise in the sum of boxes on the clinical dementia rating scale (CDR) (CDR SOB). Global CDR, memory Z score, executive function Z score, and Hamilton Depression Rating Scale (HDRS) score were the secondary outcomes. | Even though the cognitive impairment over the course of two years in the placebo group was minimal, Vitamin B12 and folic acid treatment did not slow cognitive decline in older persons with MCI and increased serum homocysteine. At month 12, the supplement significantly reduced depression symptoms; however, this effect was not long-lasting. The use of aspirin exhibited a detrimental impact on cognitive performance upon interaction with B supplements. |
| Markun et al., 2021 [28] | 16 studies; 66–82 years | Systematic review and meta-analysis | - | This study sought to evaluate the effects of Vitamin B12 alone (B12 alone), along with Vitamin B12 and folic acid with or without Vitamin B6 (B complex), on cognitive function, depressive symptoms, and idiopathic fatigue in patients without advanced neurological disorders or overt Vitamin B12 deficiency. | The clinicians did not discover any proof that supplementing with B12 or B complex had any impact on any subdomain of cognitive function results. Meta-regression also revealed no meaningful correlations between treatment outcomes and any of the putative predictors. Additionally, there was no overall impact of Vitamin supplementation on depression-related indicators. Additionally, because there was just one trial that revealed effects on idiopathic fatigue, no analysis could be done. In patients without advanced neurological problems, Vitamin B12 administration was discovered to be probably useless for enhancing cognitive performance and depressive symptoms. |
| Nawaz et al., 2020 [29] | - | Literature review | - | This review sought to examine some of the contributing factors to Vitamin B12 (B12) deficiency and its relationship to neurological diseases. The portals that were searched for literature retrieval included PubMed, Google Scholar, the Directory of Open Access Journals (DOAJ), Pak MediNet, and Science Direct. | A review of the literature found that inadequate food intake was the primary cause of this Vitamin’s deficiency, which led to a range of neurological symptoms in both adults and children. Apathy, anorexia, irritability, growth retardation, and developmental regression were among these neurological conditions. Additionally, it could have played a role in the delayed myelination or demyelination of neurons. B12 was found to be an essential micronutrient for young children’s and elders’ healthy brains. |
| Serin et al., 2019 [30] | 38 patients; 0–18 years | Retrospective study | 20:18 | In view of the characteristics of the patients included, the aim of this study was to stress the significance of early detection of Vitamin B12 deficiency. A total of 38 kids with Vitamin B12 deficiency-related neurological symptoms participated in this retrospective clinical investigation. | After receiving Vitamin B12 supplements, every patient with Vitamin B12 deficiency-related neurological symptoms made a full recovery within a month. In conclusion, anaemia and an increase in mean corpuscular volume are not necessarily connected with the clinical features of Vitamin B12 deficiency, which are general and generic. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alruwaili, M.; Basri, R.; AlRuwaili, R.; Albarrak, A.M.; Ali, N.H. Neurological Implications of Vitamin B12 Deficiency in Diet: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 958. https://doi.org/10.3390/healthcare11070958
Alruwaili M, Basri R, AlRuwaili R, Albarrak AM, Ali NH. Neurological Implications of Vitamin B12 Deficiency in Diet: A Systematic Review and Meta-Analysis. Healthcare. 2023; 11(7):958. https://doi.org/10.3390/healthcare11070958
Chicago/Turabian StyleAlruwaili, Mubarak, Rehana Basri, Raed AlRuwaili, Anas Mohammad Albarrak, and Naif H. Ali. 2023. "Neurological Implications of Vitamin B12 Deficiency in Diet: A Systematic Review and Meta-Analysis" Healthcare 11, no. 7: 958. https://doi.org/10.3390/healthcare11070958