
Comparison of Hemodynamic and Cerebral Oxygenation Responses during Exercise between Normal-Weight and Overweight Men

Abstract
:1. Introduction
2. Materials and Methods
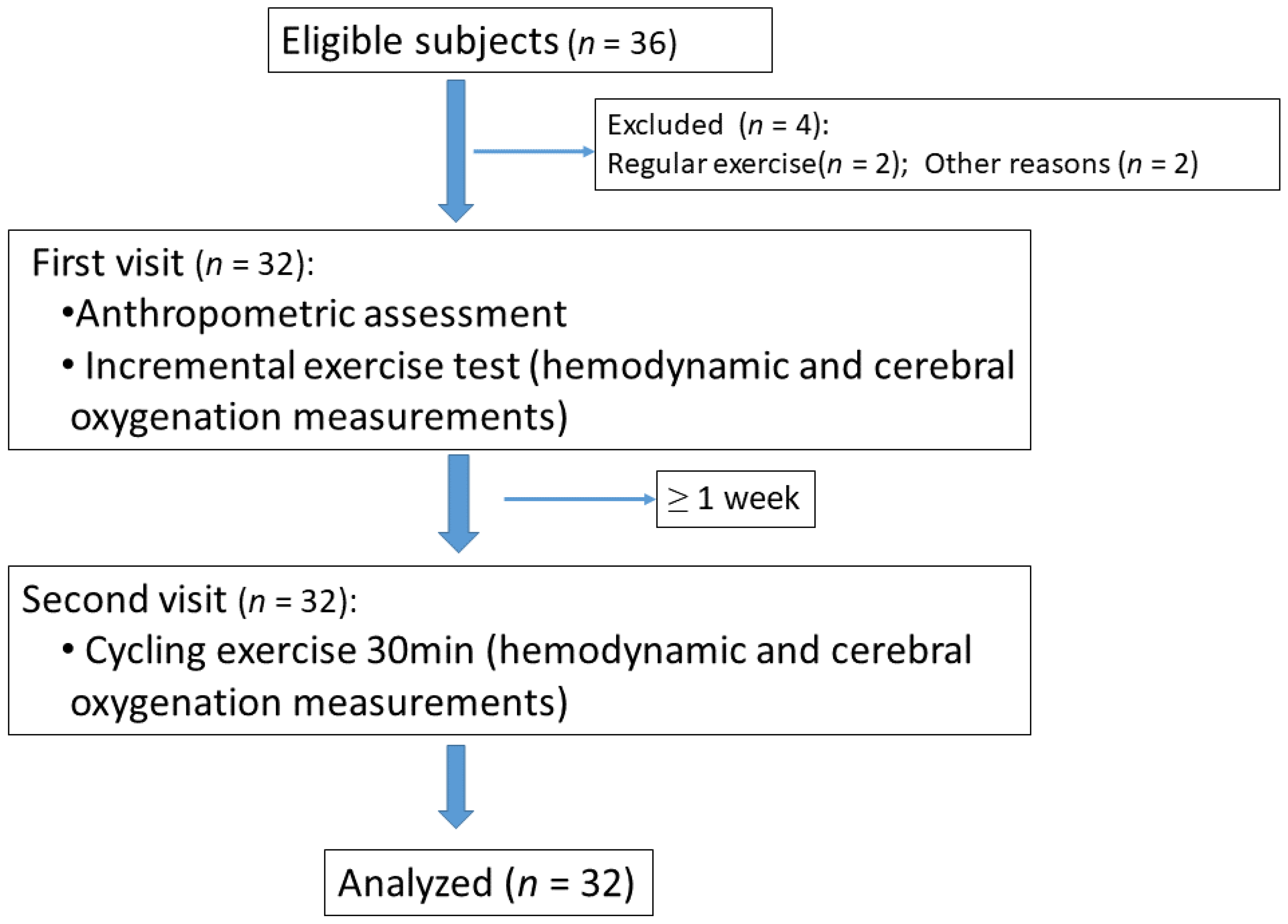
2.1. Participants
2.2. Procedures
2.3. Measurement
2.3.1. Central Hemodynamic Measurements
2.3.2. Cerebral Oxygenation Measurements
2.4. Statistical Analysis
3. Results
3.1. Clinical and Anthropometric Characteristics
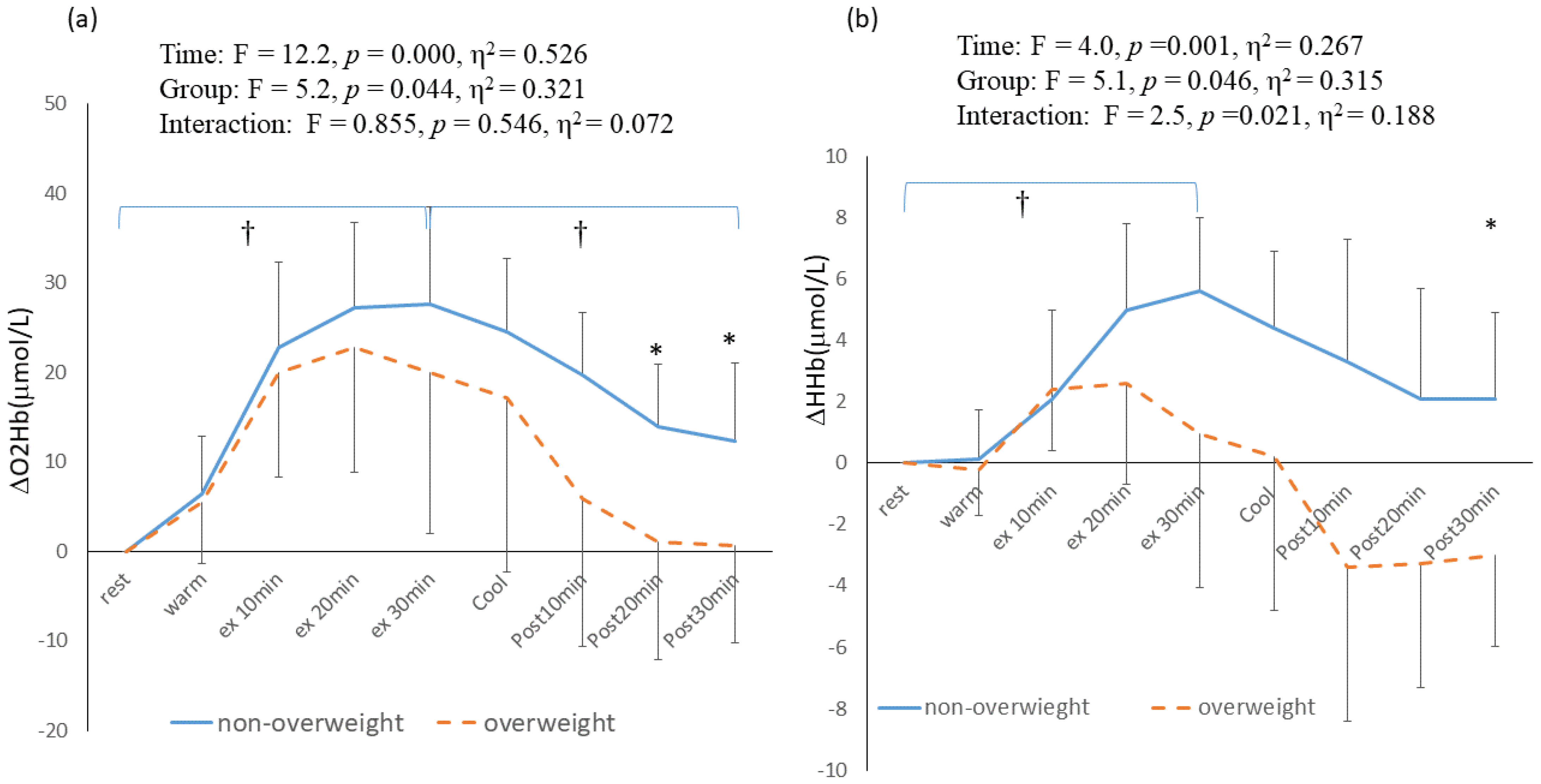
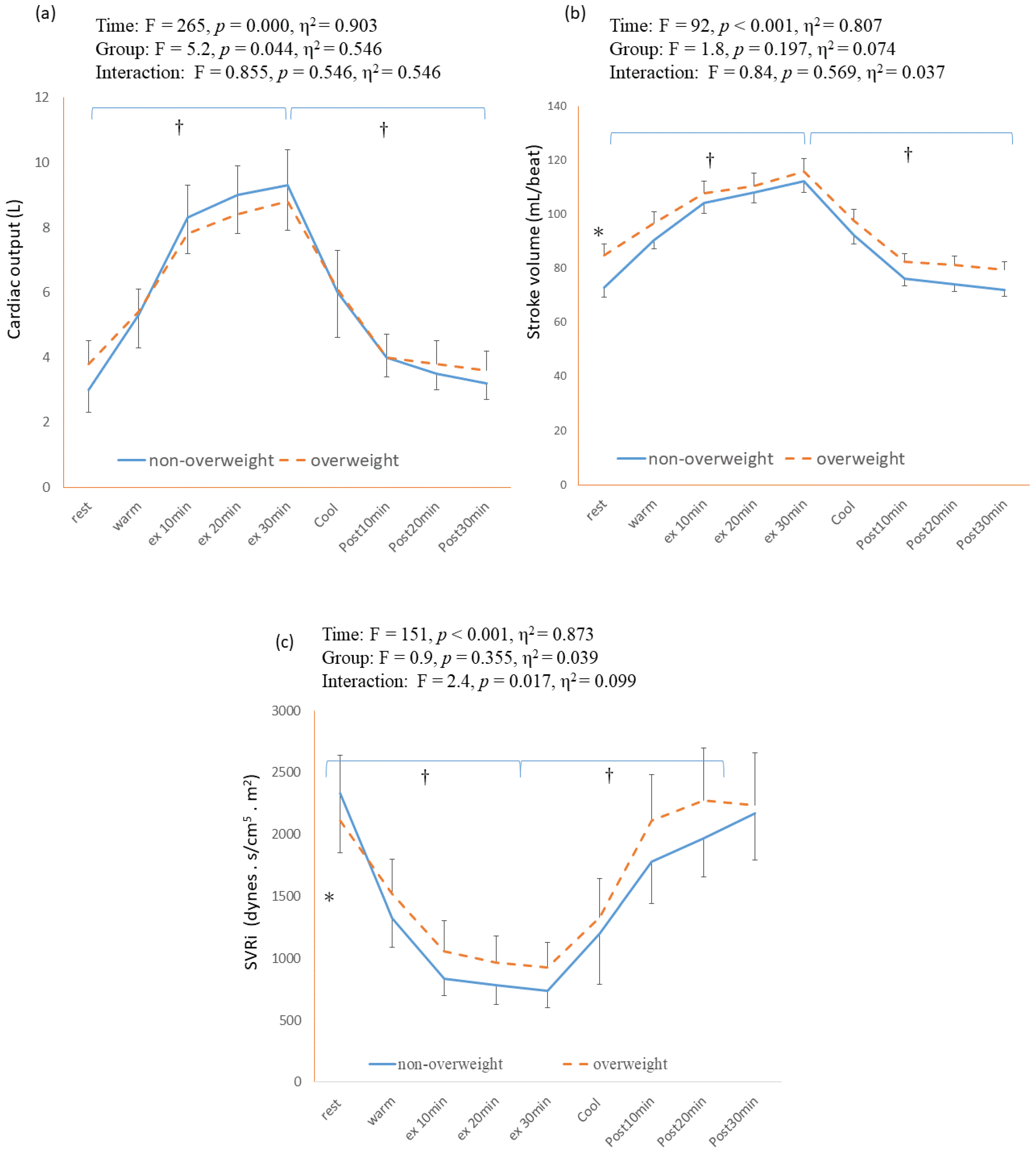
3.2. Cardiovascular and Cerebral Hemodynamics Response during 30 min Continuous Exercise
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lakhan, S.E.; Kirchgessner, A. The emerging role of dietary fructose in obesity and cognitive decline. Nutr. J. 2013, 12, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, W.; McLerran, D.F.; Rolland, B.; Zhang, X.; Inoue, M.; Matsuo, K.; He, J.; He, J.; Gupta, P.C.; Ramadas, K.; et al. Association between body-mass index and risk of death in more than 1 million Asians. N. Engl. J. Med. 2011, 364, 719–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Alpert, M.A.; Omran, J.; Bostick, B.P. Effects of obesity on cardiovascular hemodynamics, cardiac morphology, and ventricular function. Curr. Obes. Rep. 2016, 5, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Vella, C.A.; Ontiveros, D.; Zubia, R.Y. Cardiac function and arteriovenous oxygen difference during exercise in obese adults. Eur. J. Appl. Physiol. 2011, 111, 915–923. [Google Scholar] [CrossRef]
- Claassen, J.A.H.R.; Thijssen, D.H.J.; Panerai, R.B.; Faraci, F.M. Regulation of cerebral blood flow in humans: Physiology and clinical implications of autoregulation. Physiol. Rev. 2021, 101, 1487–1559. [Google Scholar] [CrossRef]
- Tchistiakova, E.; Anderson, N.D.; Greenwood, C.E.; MacIntosh, B.J. Combined effects of type 2 diabetes and hypertension associated with cortical thinning and impaired cerebrovascular reactivity relative to hypertension alone in older adults. NeuroImage Clin. 2014, 5, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Chiesa, S.; Masi, S.; Shipley, M.J.; A Ellins, E.; Fraser, A.G.; Hughes, A.; Patel, R.S.; Khir, A.W.; Halcox, J.P.; Singh-Manoux, A.; et al. Carotid artery wave intensity in mid- to late-life predicts cognitive decline: The Whitehall II study. Eur. Hearth J. 2019, 40, 2300–2309. [Google Scholar] [CrossRef]
- Giudici, A.; Palombo, C.; Kozakova, M.; Morizzo, C.; Losso, L.; Nannipieri, M.; Berta, R.; Hughes, A.D.; Cruickshank, J.K.; Khir, A.W. Weight Loss After Bariatric Surgery Significantly Improves Carotid and Cardiac Function in Apparently Healthy People with Morbid Obesity. Obes. Surg. 2020, 30, 3776–3783. [Google Scholar] [CrossRef]
- Kintiraki, E.; Dipla, K.; Triantafyllou, A.; Koletsos, N.; Grigoriadou, I.; Poulakos, P.; Sachpekidis, V.; Vrabas, I.S.; Zafeiridis, A.; Bili, E.; et al. Blunted cerebral oxygenation during exercise in women with gestational diabetes mellitus: Associations with macrovascular function and cardiovascular risk factors. Metabolism 2018, 83, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Strangman, G.; Boas, D.A.; Sutton, J.P. Non-invasive neuroimaging using near-infrared light. Biol. Psychiatry 2002, 52, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Perrey, S. Non-invasive NIR spectroscopy of human brain function during exercise. Methods 2008, 45, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine. American college of sports medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults, guidance for prescribing exercise. Med. Sci. Sports. Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Franco, R.L.; Fallow, B.A.; Huang, C.J.; Acevedo, E.O.; Arrowood, J.A.; Evans, R.K. Forearm blood flow response to acute exercise in obese and non-obese males. Eur. J. Appl. Physiol. 2013, 113, 2015–2023. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Cahalin, L.P. Evaluation of cardiorespiratory fitness and respiratory muscle function in the obese population. Prog. Cardiovasc. Dis. 2014, 56, 457–464. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International physical activity questionnaire, 12-country reliability and validity. Med. Sci. Sports. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports Medicine. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sport. Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Charloux, A.; Lonsdorfer-Wolf, E.; Richard, R.; Lampert, E.; Oswald-Mammosser, M.; Mettauer, B.; Geny, B.; Lonsdorfer, J. A new impedance cardiograph device for the non-invasive evaluation of cardiac output at rest and during exercise: Comparison with the “direct” Fick method. Eur. J. Appl. Physiol. 2000, 82, 313–320. [Google Scholar] [CrossRef]
- Richard, R.; Lonsdorfer-Wolf, E.; Charloux, A.; Doutreleau, S.; Buchheit, M.; Oswald-Mammosser, M.; Lampert, E.; Mettauer, B.; Geny, B.; Lonsdorfer, J. Non-invasive cardiac output evaluation during a maximal progressive exercise test, using a new impedance cardiograph device. Eur. J. Appl. Physiol. 2001, 85, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N.; Abbiss, C.R.; Maiorana, A.J.; Marston, K.J.; Peiffer, J.J. Intrarater reliability and agreement of the physioflow bioimpedance cardiography device during rest, moderate and high-intensity exercise. Kinesiology 2018, 50 (Suppl. S1), 140–149. [Google Scholar]
- Billaut, F.; Davis, J.M.; Smith, K.J.; Marino, F.E.; Noakes, T.D. Cerebral oxygenation decreases but does not impair performance during self-paced, strenuous exercise. Acta Physiol. 2010, 198, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Messerli, F.H.; Ventura, H.O.; Reisin, E.; Dreslinski, G.R.; Dunn, F.G.; MacPhee, A.A.; Frohlich, E.D. Borderline hypertension and obesity: Two prehypertensive states with elevated cardiac output. Circulation 1982, 66, 55–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvadori, A.; Fanari, P.; Fontana, M.; Buontempi, L.; Saezza, A.; Baudo, S.; Miserocchi, G.; Longhini, E. Oxygen uptake and cardiac performance in obese and normal subjects during exercise. Respiration 1999, 66, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Myung, J.H.; Kim, B.R.M.; Yoon, S.H.; Kwon, Y.K.M.; Park, S.S.M.; Pyun, S.B.M. Relationship between cardiorespiratory fitness and preoperative evaluation findings in patients with morbid obesity undergoing sleeve gastrectomy: A cross-sectional study. Medicine 2021, 100, e27263. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, M.J.; Baweja, P. Obesity: The ‘huge’ problem in cardiovascular diseases. Mo. Med. 2013, 110, 499–504. [Google Scholar]
- Ren, J.; Wu, N.N.; Wang, S.; Sowers, J.R.; Zhang, Y. Obesity cardiomyopathy: Evidence, mechanisms, and therapeutic implications. Physiol. Rev. 2021, 101, 1745–1807. [Google Scholar] [CrossRef]
- Zeigler, Z.S.; Swan, P.D.; Buman, M.P.; Mookadam, F.; Gaesser, G.A.; Angadi, S.S. Postexercise hemodynamic responses in lean and obese men. Med. Sci. Sport. Exerc. 2018, 50, 2292–2300. [Google Scholar] [CrossRef]
- Cavuoto, L.A.; Maikala, R.V. Obesity and the role of short duration submaximal work on cardiovascular and cerebral hemodynamics. PLoS ONE 2016, 11, e0153826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiura, M.; Nariai, T.; Takahashi, K.; Muta, A.; Sakata, M.; Ishibashi, K.; Toyohara, J.; Wagatsuma, K.; Tago, T.; Ishii, K.; et al. Dynamic exercise elicits dissociated changes between tissue oxygenation and cerebral blood flow in the prefrontal cortex: A Study Using NIRS and PET. Adv. Exp. Med. Biol. 2018, 1072, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Cavuoto, L.A.; Maikala, R.V. Role of obesity on cerebral hemodynamics and cardiorespiratory responses in healthy men during repetitive incremental lifting. Eur. J. Appl. Physiol. 2015, 115, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Hallmark, R.; Patrie, J.T.; Liu, Z.; Gaesser, G.A.; Barrett, E.J.; Weltman, A. The effect of exercise intensity on endothelial function in physically inactive lean and obese adults. PLoS ONE 2014, 9, e85450–e85551. [Google Scholar] [CrossRef] [PubMed]
- Silverman, A.; Petersen, N.H. Physiology, Cerebral Autoregulation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Csige, I.; Ujvárosy, D.; Szabó, Z.; Lőrincz, I.; Paragh, G.; Harangi, M.; Somodi, S. The Impact of Obesity on the Cardiovascular System. J. Diabetes Res. 2018, 2018, 3407306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.J.; Sherwood, A.; Hinderliter, A.L.; Mabe, S.; Tyson, C.; Avorgbedor, F.; Watkins, L.L.; Lin, P.H.; Kraus, W.E.; Blumenthal, J.A. Cerebrovascular function, vascular risk and lifestyle patterns in resistant hypertension. J. Alzheimers. Dis. 2022, 87, 345–357. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | NW Group (n = 18) | OW Group (n = 14) | p |
|---|---|---|---|
| Age (year) | 21.6 ± 0.7 | 21.8 ± 1.0 | 0.543 |
| Gender (Males) (n) | 18 | 14 | |
| Body height (cm) | 174.8 ± 5.2 | 169.3 ± 6.8 | 0.021 * |
| Body weight (kg) | 68.5 ± 4.0 | 83.3 ± 17.5 | 0.010 * |
| BMI (kg/m2) | 22.4 ± 1.4 | 29.0 ± 5.4 | 0.001 ** |
| Waist circumference (cm) | 82.7 ± 3.3 | 100.3 ± 13.8 | 0.002 ** |
| Hip circumference (cm) | 99.6 ± 4.5 | 108.3 ± 13.8 | 0.006 ** |
| Waist/hip ratio | 0.84 ± 0.03 | 0.92 ± 0.7 | 0.001 ** |
| Muscle mass (kg) | 31.1 ± 1.9 | 32.0 ± 4.4 | 0.475 |
| Fat mass (kg) | 13.4 ± 3.8 | 26.5 ± 12.5 | 0.003 ** |
| Body fat (%) | 19.3 ± 4.8 | 30.6 ± 7.8 | 0.000 ** |
| NW Group | OW Group | p | |
|---|---|---|---|
| Rest | |||
| HR (bpm) | 76.0 ± 12.1 | 82.6 ± 9.8 | 0.174 |
| SBP(mmHg) | 121.2 ± 9.7 | 128.7 ± 12.4 | 0.130 |
| DBP (mmHg) | 76.2 ± 8.3 | 88.4 ± 9.1 | 0.004 ** |
| At anaerobic threshold (AT) | |||
| Powers (watt) | 87.2 ± 26.8 | 64.7 ± 20.1 | 0.032 * |
| VO2 (mL/min) | 1274.5 ± 283.4 | 1043.1 ± 254.6 | 0.049 * |
| VO2/predicted (%) | 47.6 ± 6.1 | 47.3 ± 11.4 | 0.933 |
| At peak effort | |||
| HR (bpm) | 178.6 ± 5.2 | 167.9 ± 7.0 | 0.000 ** |
| RPE | 18.5 ± 0.51 | 18.5 ± 0.51 | 0.864 |
| Powers (watt) | 186.0 ± 26.6 | 153.4 ± 19.6 | 0.003 ** |
| VO2peak (mL/min) | 2773.5 ± 410.4 | 2451.8 ± 283.6 | 0.019 * |
| VO2peak (mL/min/kg) | 41.3 ± 5.7 | 30.0 ± 5.0 | 0.000 ** |
| %VO2peak predicted (%) | 80.1 ± 14.3 | 66.0 ± 7.5 | 0.008 ** |
| Power (Peak) | VO2peak | VO2peak/kg | ||
|---|---|---|---|---|
| TSI peak | r | 0.095 | 0.041 | 0.052 |
| p | 0.659 | 0.851 | 0.808 | |
| O2Hb peak | r | 0.353 | 0.390 * | 0.295 |
| p | 0.071 | 0.044 | 0.135 | |
| HHb peak | r | 0.508 ** | 0.469 * | 0.468 * |
| p | 0.007 | 0.014 | 0.014 | |
| tHb peak | r | 0.429 * | 0.442 * | 0.374 |
| p | 0.026 | 0.021 | 0.055 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.-H.; Lin, H.-L.; Huang, C.-C.; Chen, Y.-H. Comparison of Hemodynamic and Cerebral Oxygenation Responses during Exercise between Normal-Weight and Overweight Men. Healthcare 2023, 11, 923. https://doi.org/10.3390/healthcare11060923
Wang S-H, Lin H-L, Huang C-C, Chen Y-H. Comparison of Hemodynamic and Cerebral Oxygenation Responses during Exercise between Normal-Weight and Overweight Men. Healthcare. 2023; 11(6):923. https://doi.org/10.3390/healthcare11060923
Chicago/Turabian StyleWang, Szu-Hui, Hui-Ling Lin, Chung-Chi Huang, and Yen-Huey Chen. 2023. "Comparison of Hemodynamic and Cerebral Oxygenation Responses during Exercise between Normal-Weight and Overweight Men" Healthcare 11, no. 6: 923. https://doi.org/10.3390/healthcare11060923