
Depression in Central and Eastern Europe: How Much It Costs? Cost of Depression in Romania
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size and Participants
2.2. Definition of Cost Variables
2.3. Direct Costs
2.3.1. Primary Care Consultations
2.3.2. Outpatient System: Psychiatric Consultations and Psychotherapy
2.3.3. Hospitalization
2.3.4. Medication
2.4. Indirect Costs
Morbidity Cost
2.5. Statistical Analysis
3. Results
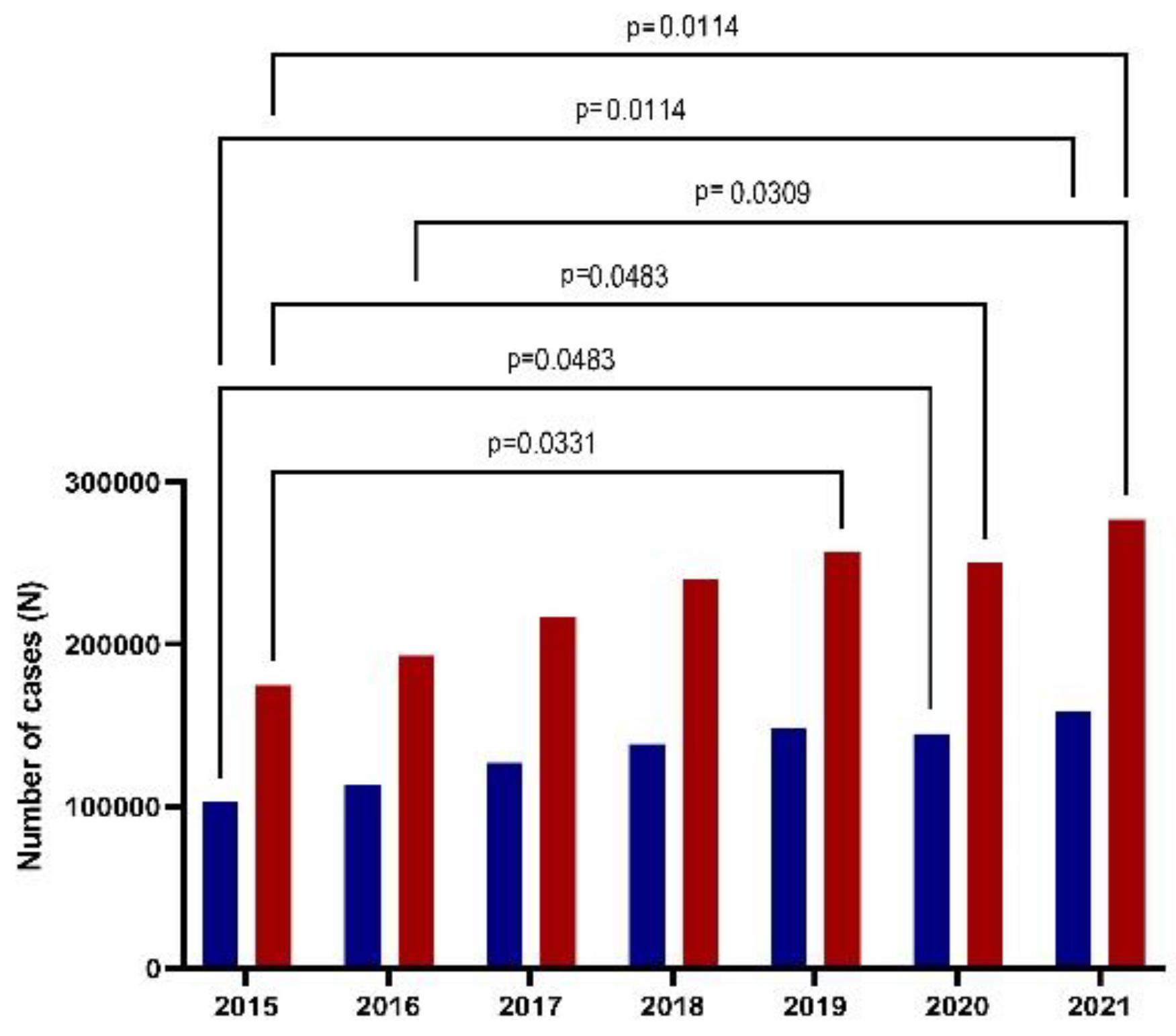
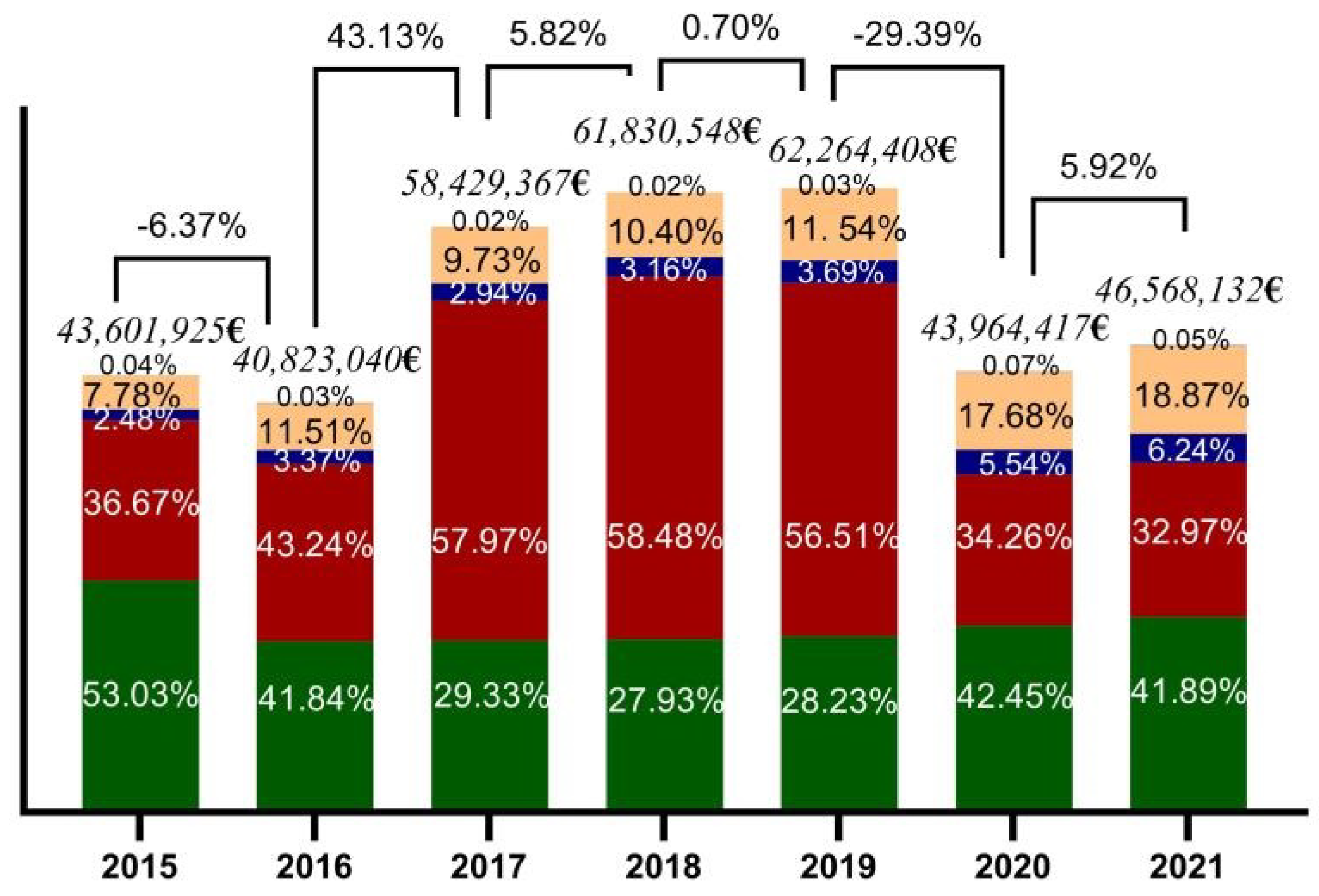
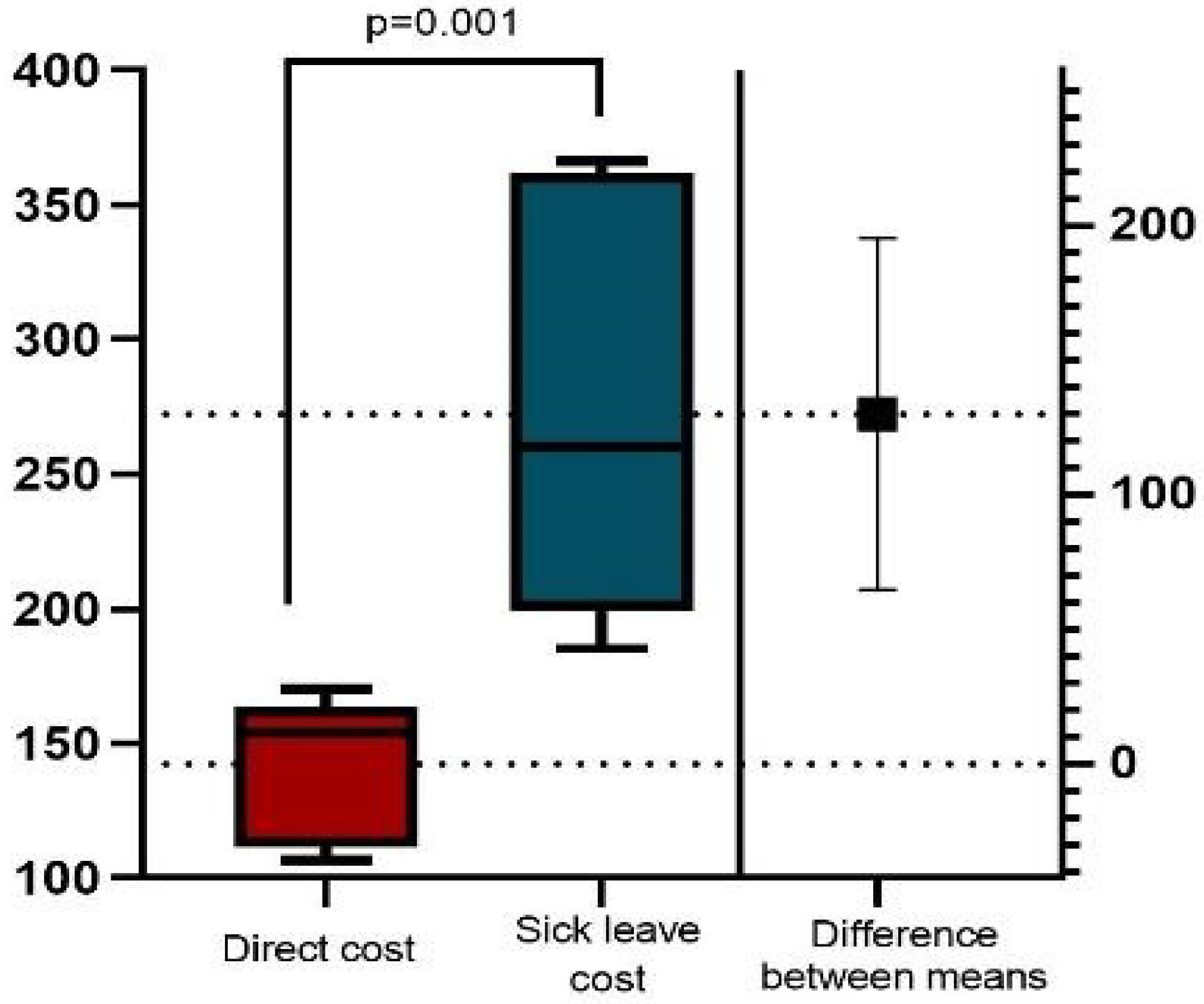
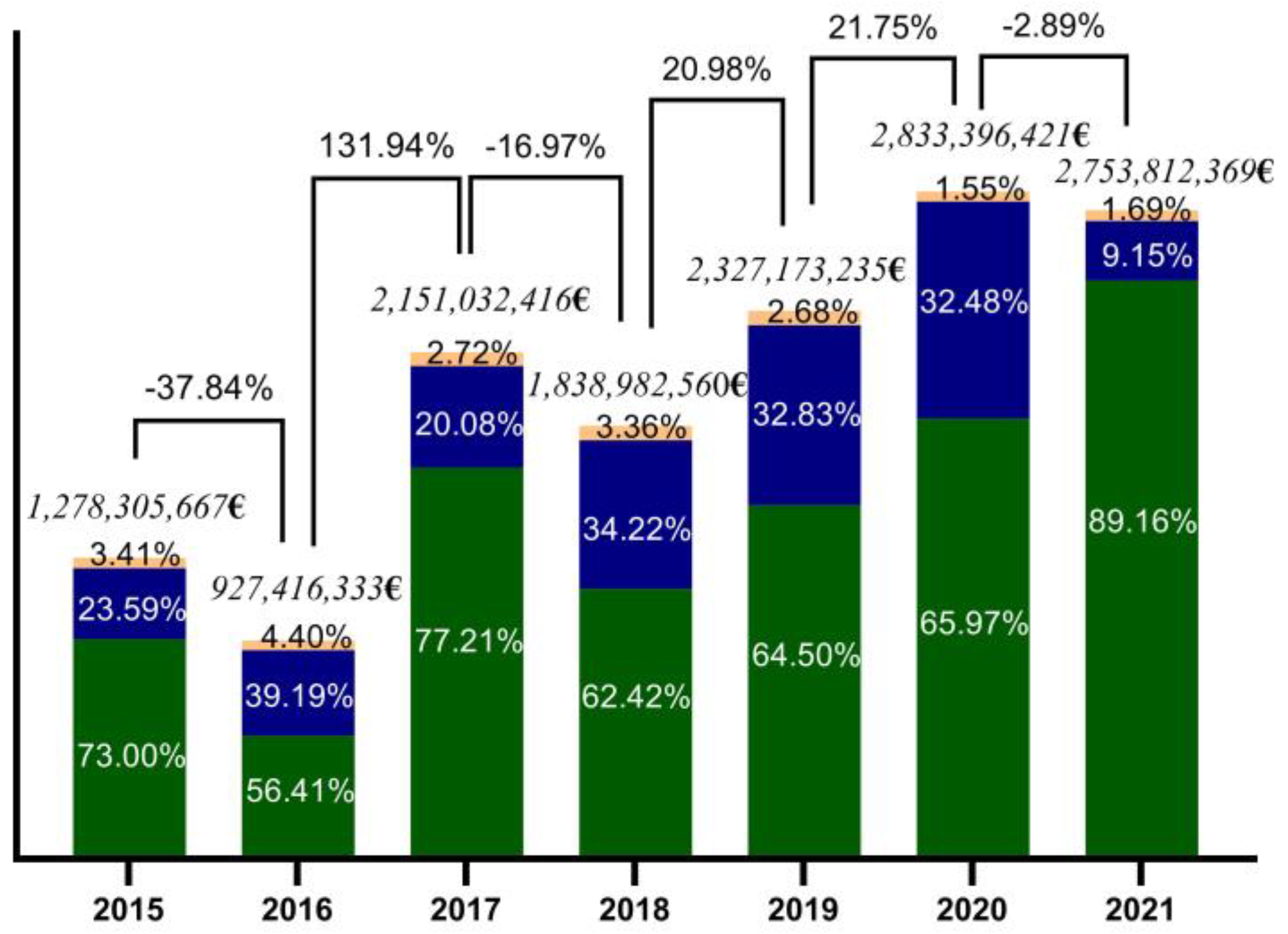
3.1. Descriptive Analysis
3.2. Correlations
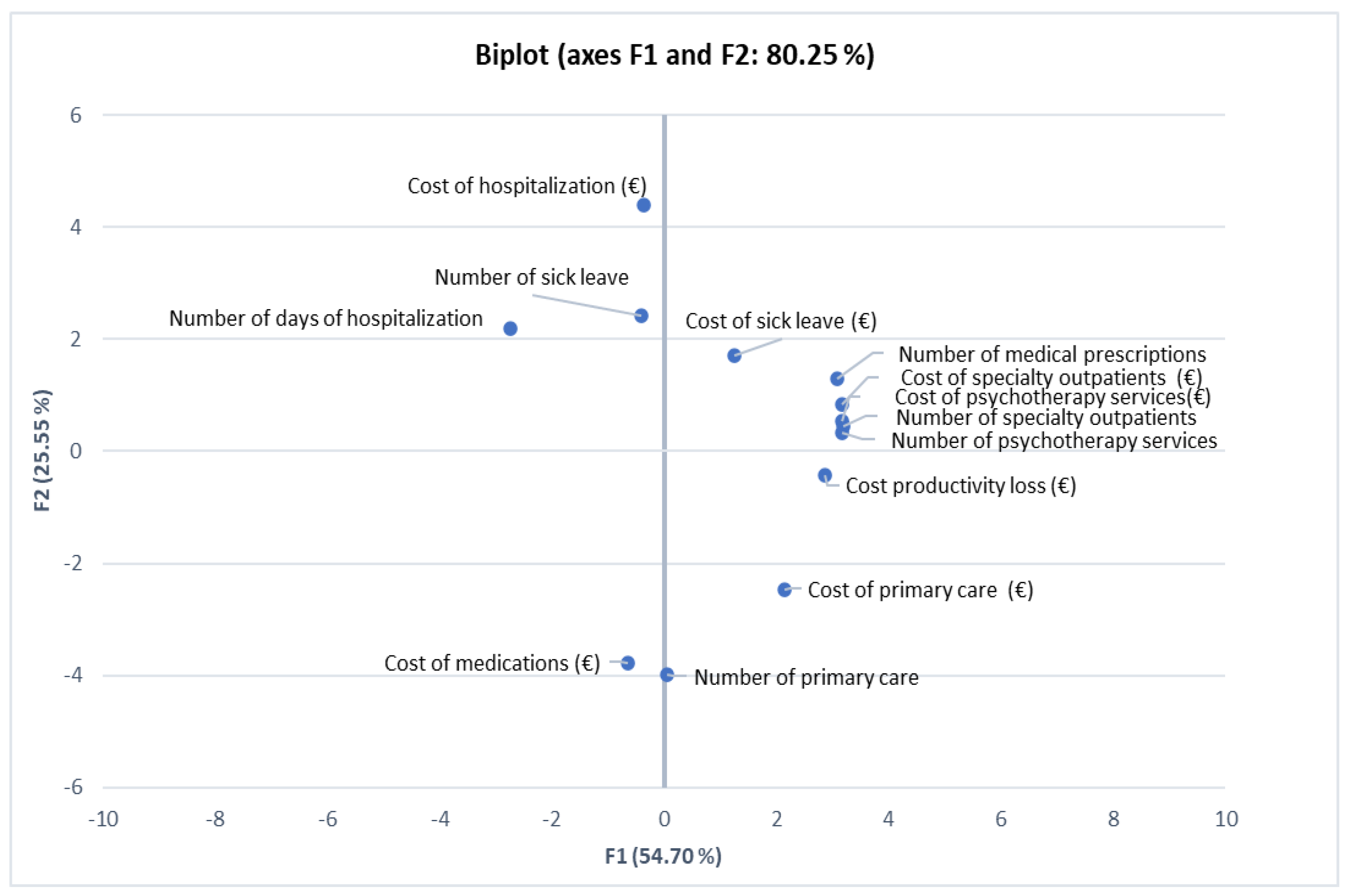
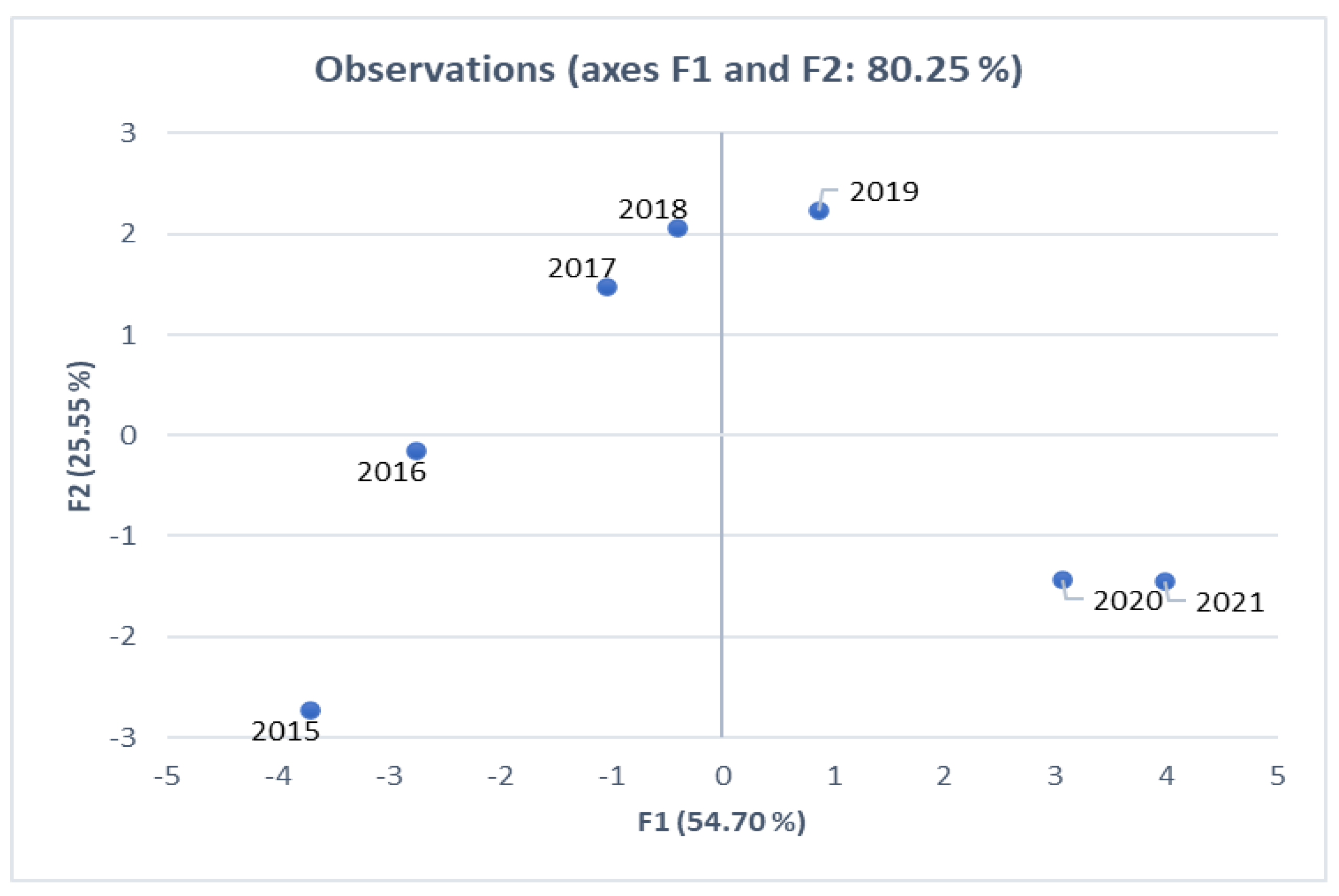
Principal Component Analysis
- −
- the years 2015 and 2016, located on the same side relative to the first factorial axis, are characterized by the same pattern;
- −
- the years 2017, 2018, and 2019 present values closest to the analyzed period’s mean levels;
- −
- 2020 and 2021, marked by the COVID-19 pandemic, have similar values for all the analyzed indicators.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Mental-Health-Strengthening-Our-Response. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-respons (accessed on 18 July 2022).
- World Health Organization. Depression and Other Common Mental Disorders Global Health Estimates. 2017. Available online: http://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf;sessionid=F8EA4E7FFF9B38B407D395EF9DEE295E?sequence=1 (accessed on 18 July 2022).
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Strawbridge, R.; McCrone, P.; Ulrichsen, A.; Zahn, R.; Eberhard, J.; Wasserman, D.; Brambilla, P.; Schiena, G.; Hegerl, U.; Balazs, J.; et al. Care pathways for people with major depressive disorder: A European Brain Council Value of Treatment study. Eur. Psychiatry 2022, 65, e36. [Google Scholar] [CrossRef] [PubMed]
- Mekonen, T.; Chan, G.C.; Connor, J.P.; Hides, L.; Leung, J. Estimating the global treatment rates for depression: A systematic review and meta-analysis. J. Affect. Disord. 2021, 295, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Global Health. Mental health matters. Lancet Glob. Health 2020, 8, e1352. [Google Scholar] [CrossRef]
- ESEMeD/MHEDEA 2000 Investigators; Alonso, J.; Angermeyer, M.C.; Bernert, S.; Bruffaerts, R.; Brugha, T.S.; Bryson, H.; de Girolamo, G.; De Graaf, R.; Demyttenaere, K.; et al. Prevalence of mental disorders in Europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr. Scand. Suppl. 2004, 109, 21–27. [Google Scholar] [CrossRef]
- Arias-de la Torre, J.; Vilagut, G.; Ronaldson, A.; Serrano-Blanco, A.; Martín, V.; Peters, M.; Valderas, J.M.; Dregan, A.; Alonso, J. Prevalence and variability of current depressive disorder in 27 European countries: A population-based study. Lancet Public Health 2021, 6, e729–e738. [Google Scholar] [CrossRef]
- Vieta, E.; Alonso, J.; Pérez-Sola, V.; Roca, M.; Hernando, T.; Sicras-Mainar, A.; Sicras-Navarro, A.; Herrera, B.; Gabilondo, A. Epidemiology and costs of depressive disorder in Spain: The EPICO study. Eur. Neuropsychopharmacol. 2021, 50, 93–103. [Google Scholar] [CrossRef]
- Thomas, C.; Morris, S. Cost of depression among adults in England in 2000. Br. J. Psychiatry 2003, 183, 514–519. [Google Scholar] [CrossRef] [Green Version]
- Kleine-Budde, K.M. The cost of depression–a cost analysis from a large database. J. Affect. Disord. 2013, 147, 137–143. [Google Scholar] [CrossRef]
- Salvador-Carulla, L.; Bendeck, M.; Fernández, A.; Alberti, C.; Sabes-Figuera, R.; Molina, C.; Knapp, M. Costs of depression in Catalonia (Spain). J. Affect. Disord. 2011, 132, 130–138. [Google Scholar] [CrossRef]
- Sobocki, P.; Jönsson, B.; Angst, J.; Rehnberg, C. Cost of depression in Europe. J. Ment. Health Policy Econ. 2006, 9, 87–98. [Google Scholar] [PubMed]
- Krupchanka, D.; Winkler, P. State of mental healthcare systems in Eastern Europe: Do we really understand what is going on? BJPsych Int. 2016, 13, 96–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Observatory on Health Systems; Policies, O. România: Profilul de țară din 2021 în ceea ce privește sănătatea; Paris/European Observatory on Health Systems and Policies: Bruxelles Paris; State of Health in the EU, OECD Publishing: Paris, France, 2021. [Google Scholar] [CrossRef]
- World Health Organizatio. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Luppa, M.; Heinrich, S.; Angermeyer, M.C.; König, H.-H.; Riedel-Heller, S.G. Cost-of-illness studies of depression: A systematic review. J. Affect. Disord. 2007, 98, 29–43. [Google Scholar] [CrossRef] [PubMed]
- DECISION No. 696/2021 for the Approval the Service Packages and of the Framework Contract Regulating the Conditions of Providing Medical Assistance, Medicines and Medical Devices, Technologies, and Assistive Devices within. and Assistive Devices within the Social Health Insurance System for the Years 2021–2022. Available online: https://legislatie.just.ro/Public/DetaliiDocument/243847 (accessed on 15 March 2023).
- Rumisha, S.F.; George, J.; Bwana, V.M.; Mboera, L.E. Years of potential life lost and productivity costs due to premature mortality from six priority diseases in Tanzania, 2006–2015. PLoS ONE 2020, 15, e0234300. [Google Scholar] [CrossRef] [PubMed]
- Gardner, J.W.; Sanborn, J.S. Years of potential life lost (YPLL)—What does it measure? Epidemiology 1990, 1, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Addinsoft. (n.d.). A Limited liability Company Registered at the Registre du Commerce et des Sociétés de Paris under number 429 102 767; Having Its Principal Office: Paris, France, 2020. [Google Scholar]
- Microsoft Office 365. Microsoft Corporation. One Microsoft Way: Redmond, WA, USA, 2017. [Google Scholar]
- Katon, W.J. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin. Neurosci. 2022, 13, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Knapp, M. Economics and mental health: The current scenario. World Psychiatry Off. J. World Psychiatr. Assoc. 2020, 19, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Brietzke, E.; Cao, B.; Chen, Y.; Linnaranta, O.; Mansur, R.B.; McIntyre, R.S. Development and implementation of guidelines for the management of depression: A systematic review. Bull. World Health Organ. 2020, 98, 683. [Google Scholar] [CrossRef]
- McDaid, D.K. Barriers in the mind: Promoting an economic case for mental health in low-and middle-income countries. World Psychiatry 2008, 7, 79. [Google Scholar] [CrossRef] [Green Version]
- Eurostat. Sourse Dataset: Hlth_Ehis_Cd1e: Eurostat. 2019. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20210910-1 (accessed on 18 July 2022).
- Shoukai, Y. Uncovering the hidden impacts of inequality on mental health: A global study. Transl. Psychiatry 2018, 8, 98. [Google Scholar]
- Kleiboer, A.S. European COMPARative Effectiveness research on blended Depression treatment versus treatment-as-usual (E-COMPARED): Study protocol for a randomized control’led, non-inferiority trial in eight European countries. Trials 2016, 17, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gili, M.; Castro, A.; García-Palacios, A.; Garcia-Campayo, J.; Mayoral-Cleries, F.; Botella, C.; Roca, M.; Barceló-Soler, A.; Hurtado, M.M.; Navarro, M.; et al. Efficacy of three low-intensity, internet-based psychological interventions for the treatment of depression in primary care: Randomized controlled trial. J. Med. Internet Res. 2020, 22, e15845. [Google Scholar] [CrossRef] [PubMed]
- Roy, T.L. Prevalence of comorbid depression in outpatients with type 2 diabetes mellitus in Bangladesh. BMC Psychiatry 2012, 12, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katon, W.M. Depression and Diabetes; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Szigethy, E.M.-N. Mental health costs of inflammatory bowel diseases. Inflamm. Bowel Dis. 2021, 27, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Iordache, M.M.; Tocia, C.; Aschie, M.; Dumitru, A.; Manea, M.; Cozaru, G.C.; Petcu, L.; Vlad, S.E.; Dumitru, E.; Chisoi, A. Intestinal Permeability and Depression in Patients with Inflammatory Bowel Disease. J. Clin. Med. 2022, 11, 5121. [Google Scholar] [CrossRef]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Brugha, T.S. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Morris, S.; Sutton, M.; Gravelle, H. Inequity and inequality in the use of health care in England: An empirical investigation. Soc. Sci. Med. 2005, 60, 1251–1266. [Google Scholar] [CrossRef]
- Issue Monitoring. Available online: https://www.issuemonitoring.ro/sistemul-de-sanatate-din-romania-politici-publice/ (accessed on 15 March 2023).
- Ordin 622/2012, Ministerul Sanatatii Hotararea nr 196/139/2017. Available online: http://www.casan.ro/castr/media/postFiles/Ordin%20Norme%20metodologice%20Contract%20Cadru%20MS-CNAS%20196-139_2017.pdf (accessed on 15 March 2023).
- Ordin 388/186/2015 Ministerul Sanatatii. Available online: https://lege5.ro (accessed on 15 March 2023).
- Ordin 1728/2017Ministerul Sanatatii. Available online: https://cas.cnas.ro (accessed on 15 March 2023).
- Proiect Consultare. Available online: https://www.formaremedicala.ro/wp-content/uploads/2023/02/PROIECT-CONTRACT-CADRU-2023-CNAS.pdf (accessed on 15 March 2023).
- Krieger, N. Theories for social epidemiology in the 21st century: An ecosocial perspective. Int. J. Epidemiol. 2001, 30, 668–677. [Google Scholar] [CrossRef]
- Cubillos, L.B.-R. The effectiveness and cost-effectiveness of integrating mental health services in primary care in low-and middle-income countries: Systematic review. BJPsych Bull. 2021, 45, 40–52. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Cardinal, R.N. Accessibility and efficiency of mental health services, United Kingdom of Great Britain and Northern Ireland. Bull. World Health Organ. 2021, 99, 674. [Google Scholar] [CrossRef]
- Hafner, J.; Schönfeld, S.; Tokgöz, P.; Choroschun, K.; Schlubach, A.; Dockweiler, C. Digital Health Interventions in Depression Care—A Survey on Acceptance from the Perspective of Patients, Their Relatives and Health Professionals. Healthcare 2022, 10, 2019. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.M.; Canvin, L.; Green, J.; Layard, R.; Pilling, S.; Janecka, M. Transparency about the outcomes of mental health services (IAPT approach): An analysis of public data. Lancet 2018, 91, 679–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of cases ≥18 years | 2,540,792 | ||
| Number of deaths ≥18 years | 143,340 | 5.64% | |
| Depression costs EUR (2015–2021) | Mean/year patient | Cost components | % |
| Direct costs | 142.30 | 357,481,837 | 2.83 |
| Primary care | 0.05 | 131,420 | 0.04 |
| Specialty outpatients | 16.96 | 43,953,075 | 12.30 |
| Psychotherapy | 5.42 | 13,767,622 | 3.85 |
| Hospitalization | 67.12 | 169,274,345 | 47.35 |
| Medications | 52.88 | 130,355,375 | 36.46 |
| Indirect costs | 13,752,637,164 | 97.17 | |
| Sick leaves | 272.33 | 3,662,215,236 | 27.36 |
| Cost of productivity loss (CPL) | - | 10,090,421,928 | 69.81 |
| Total costs | 5553.4 | 14,110,119,001 | - |
| Component | Initial Eigenvalues | Extraction Sums of Squared Loadings | ||||
|---|---|---|---|---|---|---|
| Total | % of Variance | Cumulative % | Total | % of Variance | Cumulative % | |
| 1 | 7.112 | 54.707 | 54.707 | 7.112 | 54.707 | 54.707 |
| 2 | 3.322 | 25.552 | 80.259 | 3.322 | 25.552 | 80.259 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iordache, M.M.; Sorici, C.O.; Aivaz, K.A.; Lupu, E.C.; Dumitru, A.; Tocia, C.; Dumitru, E. Depression in Central and Eastern Europe: How Much It Costs? Cost of Depression in Romania. Healthcare 2023, 11, 921. https://doi.org/10.3390/healthcare11060921
Iordache MM, Sorici CO, Aivaz KA, Lupu EC, Dumitru A, Tocia C, Dumitru E. Depression in Central and Eastern Europe: How Much It Costs? Cost of Depression in Romania. Healthcare. 2023; 11(6):921. https://doi.org/10.3390/healthcare11060921
Chicago/Turabian StyleIordache, Miorita Melina, Costin Octavian Sorici, Kamer Ainur Aivaz, Elena Carmen Lupu, Andrei Dumitru, Cristina Tocia, and Eugen Dumitru. 2023. "Depression in Central and Eastern Europe: How Much It Costs? Cost of Depression in Romania" Healthcare 11, no. 6: 921. https://doi.org/10.3390/healthcare11060921