
The Impact of Event Scale-Revised: Examining Its Cutoff Scores among Arab Psychiatric Patients and Healthy Adults within the Context of COVID-19 as a Collective Traumatic Event

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, and Procedure
2.2. Study Instruments
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
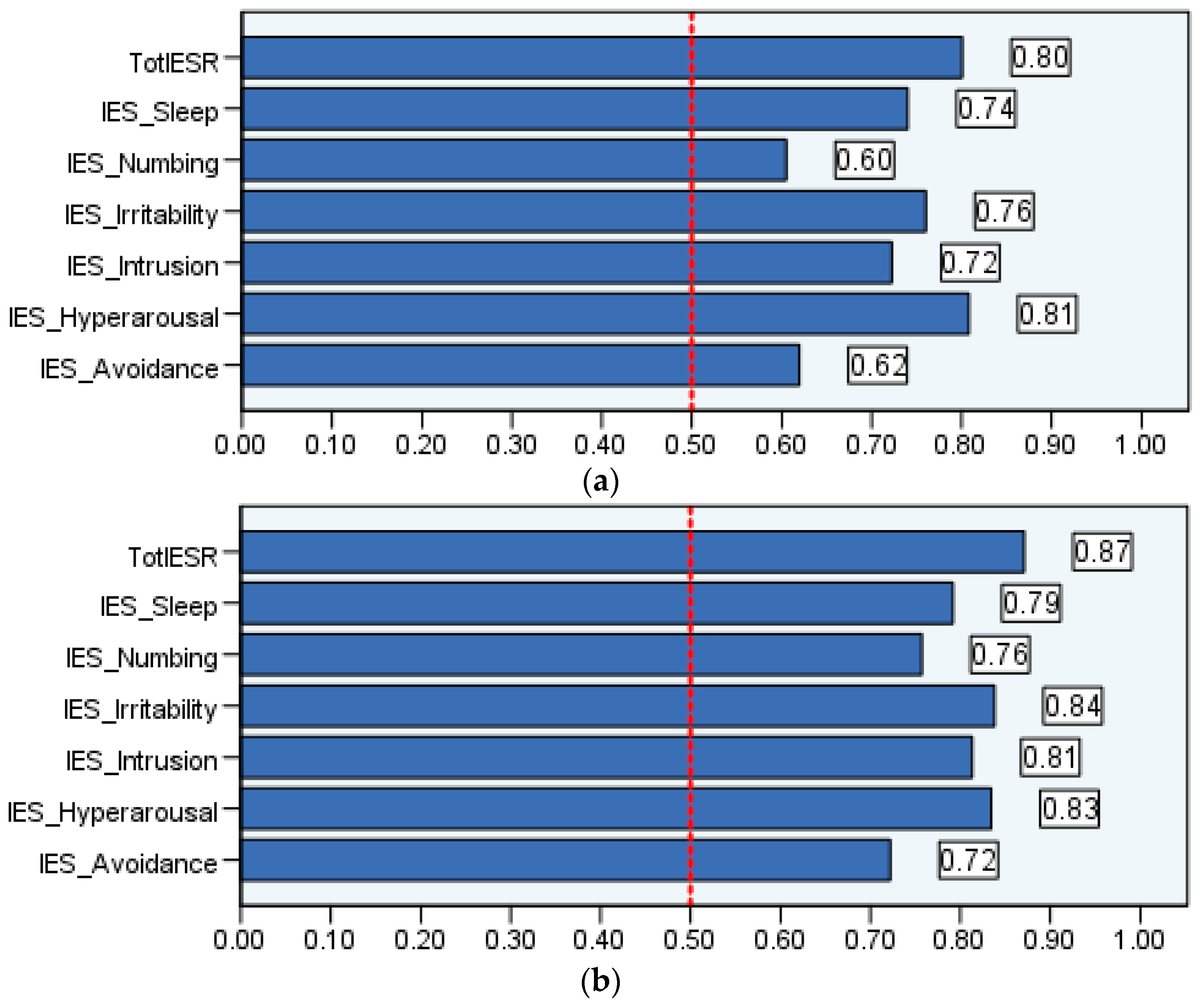
3.2. Receiver-Operating Characteristic (ROC) Analysis Determining the Cutoff of the Arabic Version of the Impact of Event Scale-Revised (IES-R)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatr. 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, R.; Krishnamoorthy, Y.; Basavarachar, V.; Dakshinamoorthy, R. Prevalence of post-traumatic stress disorder among survivors of severe COVID-19 infections: A systematic review and meta-analysis. J. Affect. Disord. 2022, 299, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Al-Amer, R.; Malak, M.Z.; Burqan, H.M.R.; Stănculescu, E.; Nalubega, S.; Alkhamees, A.A.; Hendawy, A.O.; Ali, A.M. Emotional Reaction to the First Dose of COVID-19 Vaccine: Postvaccination Decline in Anxiety and Stress among Anxious Individuals and Increase among Individuals with Normal Prevaccination Anxiety Levels. J. Pers. Med. 2022, 12, 912. [Google Scholar] [CrossRef]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreaks in the general population: Practical considerations for the COVID-19 pandemic. Singap. Med. J. 2020, 61, 350. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef]
- Karbasi, Z.; Eslami, P. Prevalence of post-traumatic stress disorder during the COVID-19 pandemic in children: A review and suggested solutions. Middle East Curr. Psychiatry 2022, 29, 74. [Google Scholar] [CrossRef]
- Ali, A.M.; Hendawy, A.O.; Almarwani, A.M.; Alzahrani, N.; Ibrahim, N.; Alkhamees, A.A.; Kunugi, H. The Six-item Version of the Internet Addiction Test: Its development, psychometric properties, and measurement invariance among women with eating disorders and healthy school and university students. Int. J. Environ. Res. Public Health 2021, 18, 12341. [Google Scholar] [CrossRef]
- Ali, A.M.; Hori, H.; Kim, Y.; Kunugi, H. Predictors of nutritional status, depression, internet addiction, Facebook addiction, and tobacco smoking among women with eating disorders in Spain. Front. Psychiatry 2021, 12, 2001. [Google Scholar] [CrossRef] [PubMed]
- Trnka, R.; Lorencova, R. Fear, anger, and media-induced trauma during the outbreak of COVID-19 in the Czech Republic. Psychol. Trauma 2020, 12, 546–549. [Google Scholar] [CrossRef]
- Ali, A.M.; Alkhamees, A.A.; Elhay, E.S.A.; Taha, S.M.; Hendawy, A.O. COVID-19-related psychological trauma and psychological distress among community-dwelling psychiatric patients: People struck by depression and sleep disorders endure the greatest burden. Front. Public Health 2022, 9, 2141. [Google Scholar] [CrossRef] [PubMed]
- Andhavarapu, S.; Yardi, I.; Bzhilyanskaya, V.; Lurie, T.; Bhinder, M.; Patel, P.; Pourmand, A.; Tran, Q.K. Post-traumatic stress in healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2022, 317, 114890. [Google Scholar] [CrossRef]
- Li, W.; Zhao, N.; Yan, X.; Xu, X.; Zou, S.; Wang, H.; Li, Y.; Du, X.; Zhang, L.; Zhang, Q.; et al. Network Analysis of Depression, Anxiety, Posttraumatic Stress Symptoms, Insomnia, Pain, and Fatigue in Clinically Stable Older Patients With Psychiatric Disorders During the COVID-19 Outbreak. J. Geriatr. Psychiatry Neurol. 2022, 35, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Idoiaga, N.; Legorburu, I.; Ozamiz-Etxebarria, N.; Lipnicki, D.M.; Villagrasa, B.; Santabárbara, J. Prevalence of Post-Traumatic Stress Disorder (PTSD) in University Students during the COVID-19 Pandemic: A Meta-Analysis Attending SDG 3 and 4 of the 2030 Agenda. Sustainability 2022, 14, 7914. [Google Scholar] [CrossRef]
- Sun, R.; Zhou, X. Differences in posttraumatic stress disorder networks between young adults and adolescents during the COVID-19 pandemic. Psychol. Trauma 2022. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR; American Psychiatric Association Publishing: Washington, DC, USA, 2022. [Google Scholar]
- Chamaa, F.; Bahmad, H.F.; Darwish, B.; Kobeissi, J.M.; Hoballah, M.; Nassif, S.B.; Ghandour, Y.; Saliba, J.-P.; Lawand, N.; Abou-Kheir, W. PTSD in the COVID-19 Era. Curr. Neuropharmacol. 2021, 19, 2164–2179. [Google Scholar] [CrossRef]
- Dong, F.; Liu, H.-L.; Dai, N.; Yang, M.; Liu, J.-P. A living systematic review of the psychological problems in people suffering from COVID-19. J. Affect. Disord. 2021, 292, 172–188. [Google Scholar] [CrossRef]
- d’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-Traumatic Stress Symptoms in Healthcare Workers Dealing with the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 601. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Gong, Y.-M.; Liu, L.; Sun, Y.-K.; Tian, S.-S.; Wang, Y.-J.; Zhong, Y.; Zhang, A.-Y.; Su, S.-Z.; Liu, X.-X.; et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: A meta-analysis and systematic review. Mol. Psychiatry 2021, 26, 4982–4998. [Google Scholar] [CrossRef]
- Mueller-Pfeiffer, C.; Martin-Soelch, C.; Blair, J.R.; Carnier, A.; Kaiser, N.; Rufer, M.; Schnyder, U.; Hasler, G. Impact of emotion on cognition in trauma survivors: What is the role of posttraumatic stress disorder? J. Affect. Disord. 2010, 126, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Kaseda, E.T.; Levine, A.J. Post-traumatic stress disorder: A differential diagnostic consideration for COVID-19 survivors. Clin. Neuropsychol. 2020, 34, 1498–1514. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A. Post-traumatic stress disorder as moderator of other mental health conditions. World Psychiatry 2022, 21, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Chung, M.C.; Zhang, J.; Fang, S. Network analysis on the relationship between posttraumatic stress disorder, psychiatric co-morbidity and posttraumatic growth among Chinese adolescents. J. Affect. Disord. 2022, 309, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Ge, F.; Zhang, D.; Wu, L.; Mu, H. Predicting Psychological State Among Chinese Undergraduate Students in the COVID-19 Epidemic: A Longitudinal Study Using a Machine Learning. Neuropsychiatr. Dis. Treat. 2020, 16, 2111–2118. [Google Scholar] [CrossRef] [PubMed]
- Debowska, A.; Horeczy, B.; Boduszek, D.; Dolinski, D. A repeated cross-sectional survey assessing university students’ stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol. Med. 2022, 52, 3744–3747. [Google Scholar] [CrossRef]
- Kim, M.-J.; Paek, S.-H.; Kwon, J.-H.; Park, S.-H.; Chung, H.-J.; Byun, Y.-H. Changes in Suicide Rate and Characteristics According to Age of Suicide Attempters before and after COVID-19. Children 2022, 9, 151. [Google Scholar] [CrossRef]
- Ali, A.M.; Al-Amer, R.; Atout, M.; Ali, T.S.; Mansour, A.M.H.; Khatatbeh, H.; Alkhamees, A.A.; Hendawy, A.O. The Nine-Item Internet Gaming Disorder Scale (IGDS9-SF): Its Psychometric Properties among Sri Lankan Students and Measurement Invariance across Sri Lanka, Turkey, Australia, and the USA. Healthcare 2022, 10, 490. [Google Scholar] [CrossRef]
- Beck, J.G.; Grant, D.M.; Read, J.P.; Clapp, J.D.; Coffey, S.F.; Miller, L.M.; Palyo, S.A. The impact of event scale-revised: Psychometric properties in a sample of motor vehicle accident survivors. J. Anxiety Disord. 2008, 22, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Craparo, G.; Faraci, P.; Rotondo, G.; Gori, A. The Impact of Event Scale—Revised: Psychometric properties of the Italian version in a sample of flood victims. Neuropsychiatr. Dis. Treat. 2013, 9, 1427–1432. [Google Scholar] [CrossRef] [Green Version]
- Eid, J.; Larsson, G.; Johnsen, B.H.; Laberg, J.C.; Bartone, P.T.; Carlstedt, B. Psychometric properties of the Norwegian Impact of Event Scale-revised in a non-clinical sample. Nord. J. Psychiatry 2009, 63, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Asukai, N.; Kato, H.; Kawamura, N.; Kim, Y.; Yamamoto, K.; Kishimoto, J.; Miyake, Y.; Nishizono-Maher, A. Reliability and validity of the Japanese-language version of the impact of event scale-revised (IES-R-J): Four studies of different traumatic events. J. Nerv. Ment. Dis. 2002, 190, 175–182. [Google Scholar] [CrossRef]
- Gargurevich, R.; Luyten, P.; Fils, J.F.; Corveleyn, J. Factor structure of the Impact of Event Scale-Revised in two different Peruvian samples. Depress. Anxiety 2009, 26, E91–E98. [Google Scholar] [CrossRef] [PubMed]
- Morina, N.; Böhme, H.F.; Ajdukovic, D.; Bogic, M.; Franciskovic, T.; Galeazzi, G.M.; Kucukalic, A.; Lecic-Tosevski, D.; Popovski, M.; Schützwohl, M.; et al. The structure of post-traumatic stress symptoms in survivors of war: Confirmatory factor analyses of the Impact of Event Scale—Revised. J. Anxiety Disord. 2010, 24, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Davey, C.; Heard, R.; Lennings, C. Development of the Arabic versions of the Impact of Events Scale-Revised and the Posttraumatic Growth Inventory to assess trauma and growth in Middle Eastern refugees in Australia. Clin. Psychol. 2015, 19, 131–139. [Google Scholar] [CrossRef]
- Ali, A.M.; Al-Amer, R.; Kunugi, H.; Stănculescu, E.; Taha, S.M.; Saleh, M.Y.; Alkhamees, A.A.; Hendawy, A.O. The Arabic version of the Impact of Event Scale—Revised: Psychometric evaluation in psychiatric patients and the general public within the context of COVID-19 outbreak and quaran-tine as collective traumatic events. J. Pers. Med. 2022, 12, 681. [Google Scholar] [CrossRef]
- Ali, A.M.; Ahmed, A.H.; Smail, L. Psychological Climacteric Symptoms and Attitudes toward Menopause among Emirati Women. Int. J. Environ. Res. Public Health 2020, 17, 5028. [Google Scholar] [CrossRef]
- Ali, A.M.; Hori, H.; Kim, Y.; Kunugi, H. The Depression Anxiety Stress Scale 8-items expresses robust psychometric properties as an ideal shorter version of the Depression Anxiety Stress Scale 21 among healthy respondents from three continents. Front. Psychol. 2022, 13, 799769. [Google Scholar] [CrossRef]
- Ali, A.M.; Alkhamees, A.A.; Hori, H.; Kim, Y.; Kunugi, H. The Depression Anxiety Stress Scale 21: Development and Validation of the Depression Anxiety Stress Scale 8-item in Psychiatric Patients and the General Public for Easier Mental Health Measurement in a Post-COVID-19 World. Int. J. Environ. Res. Public Health 2021, 18, 10142. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Taylor, S. Garbage in, garbage out: The tenuous state of research on PTSD in the context of the COVID-19 pandemic and infodemic. J. Anxiety Disord. 2021, 78, 102368. [Google Scholar] [CrossRef]
- Van Overmeire, R. The Methodological Problem of Identifying Criterion A Traumatic Events During the COVID-19 Era: A Commentary on Karatzias et al. (2020). J. Trauma. Stress 2020, 33, 864–865. [Google Scholar] [CrossRef] [PubMed]
- Norrholm, S.D.; Zalta, A.; Zoellner, L.; Powers, A.; Tull, M.T.; Reist, C.; Schnurr, P.P.; Weathers, F.; Friedman, M.J. Does COVID-19 count?: Defining Criterion A trauma for diagnosing PTSD during a global crisis. Depress. Anxiety 2021, 38, 882–885. [Google Scholar] [CrossRef]
- Husky, M.M.; Pietrzak, R.H.; Marx, B.P.; Mazure, C.M. Research on Posttraumatic Stress Disorder in the Context of the COVID-19 Pandemic: A Review of Methods and Implications in General Population Samples. Chronic Stress 2021, 5, 24705470211051327. [Google Scholar] [CrossRef]
- Ali, A.M.; Hendawy, A.O.; Al-Amer, R.; Shahrour, G.; Ali, E.M.; Alkhamees, A.A.; Ibrahim, N.; Lamadah, S.M.T.; Ahmed, A.H. Psychometric evaluation of the Depression Anxiety Stress Scale 8 among women with chronic non-cancer pelvic pain. Sci. Rep. 2022, 12, 20693. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Alameri, R.A.; Brooks, T.; Ali, T.S.; Ibrahim, N.; Khatatbeh, H.; Alkhamees, A.A.; A1-Dossary, S.A.; Hassan, B.H. The Depression Anxiety Stress Scale-8: Investigating Its Cutoff Score among Women with Chronic Pelvic Pain for Better Pain Management Outcomes. BMC Nurs. 2023. under review. [Google Scholar]
- Ali, A.M.; Alkhamees, A.A.; Al-Dwaikat, T.N.; Khatatbeh, H.; A1-Dossary, S.A. The Depression Anxiety Stress Scale 8: Determining its cutoff scores among family caregivers of patients with dementia. Front. Public Health 2023. under review. [Google Scholar]
- Ali, A.M.; Kunugi, H. Approaches to nutritional screening in patients with Coronavirus Disease 2019 (COVID-19). Int. J. Environ. Res. Public Health 2021, 18, 2772. [Google Scholar] [CrossRef]
- King, D.W.; Orazem, R.J.; Lauterbach, D.; King, L.A.; Hebenstreit, C.L.; Shalev, A.Y. Factor structure of posttraumatic stress disorder as measured by the Impact of Event Scale–Revised: Stability across cultures and time. Psychol. Trauma 2009, 1, 173–187. [Google Scholar] [CrossRef]
- Yuan, G.F.; Shi, W.; Elhai, J.D.; Montag, C.; Chang, K.; Jackson, T.; Hall, B.J. Gaming to cope: Applying network analysis to understand the relationship between posttraumatic stress symptoms and internet gaming disorder symptoms among disaster-exposed Chinese young adults. Addict. Behav. 2022, 124, 107096. [Google Scholar] [CrossRef]
- Flory, J.D.; Yehuda, R. Comorbidity between post-traumatic stress disorder and major depressive disorder: Alternative explanations and treatment considerations. Dialogues Clin. Neurosci. 2015, 17, 141–150. [Google Scholar] [CrossRef]
- Morina, N.; Ehring, T.; Priebe, S. Diagnostic utility of the impact of event scale-revised in two samples of survivors of war. PLoS ONE 2013, 8, e83916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawamura, N.; Kim, Y.; Asukai, N. Suppression of cellular immunity in men with a past history of posttraumatic stress disorder. Am. J. Psychiatry 2001, 158, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Hendawy, A.O.; Elhay, E.S.A.; Ali, E.M.; Alkhamees, A.A.; Kunugi, H.; Hassan, N.I. The Bergen Facebook Addiction Scale: Its psychometric properties and invariance among women with eating disorders. BMC Women’s Health 2022, 22, 99. [Google Scholar] [CrossRef] [PubMed]
- Dalgleish, T.; Power, M.J. Emotion-specific and emotion-non-specific components of posttraumatic stress disorder (PTSD): Implications for a taxonomy of related psychopathology. Behav. Res. Ther. 2004, 42, 1069–1088. [Google Scholar] [CrossRef]
- Salehinejad, M.A.; Azarkolah, A.; Ghanavati, E.; Nitsche, M.A. Circadian disturbances, sleep difficulties and the COVID-19 pandemic. Sleep Med. 2021, 91, 246–252. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Psychiatric Patients (N = 168) No (%) | Healthy Adults (N = 992) No (%) | |
|---|---|---|
| Gender | ||
| Females | 119 (70.8) | 622 (62.7) |
| Males | 49 (29.2) | 370 (37.3) |
| Age (years) | ||
| 18–30 | 87 (51.8) | 448 (45.2) |
| >31 | 81 (48.2) | 544 (54.8) |
| Marital status | ||
| Married | 77 (45.8) | 553 (55.7) |
| Single/widowed/divorced | 91 (54.2) | 439 (44.3) |
| Education | ||
| School degree | 51 (30.4) | 263 (26.5) |
| University degree | 105 (62.5) | 605 (61.0) |
| Post-graduate degree | 12 (7.1) | 124 (12.5) |
| DASS-8 MD (IQR) | 9 (2.0–17.0) | 2 (0.0–7.0) |
| IES-R MD (IQR) | 30.0 (14.0–43.0) | 18.0 (7.0–29.0) |
| Avoidance MD (IQR) | 8.0 (4.0–12.0) | 6.0 (1.0–10.0) |
| Intrusion MD (IQR) | 5.0 (2.0–9.0) | 3.0 (1.0–6.0) |
| Numbing MD (IQR) | 4.0 (2.0–7.0) | 3.0 (0–6.0) |
| Hyperarousal MD (IQR) | 4.0 (2.0–8.0) | 2.0 (0–4.0) |
| Sleep disturbance MD (IQR) | 2.0 (0–5.0) | 0 (0–2.0) |
| Irritability MD (IQR) | 3.0 (0–4.0) | 1.0 (0–3.0) |
| Sample | AUC | SE | AUC 95% CI | Cutoff | Sensitivity | Specificity | Youden Index | |
|---|---|---|---|---|---|---|---|---|
| IES-R | Sample 1 | 0.86 | 0.03 | 0.80 to 0.92 | 39.5 | 0.85 | 0.73 | 0.58 |
| Sample 2 | 0.91 | 0.02 | 0.87 to 0.94 | 30.5 | 0.87 | 0.83 | 0.70 | |
| Avoidance | Sample 1 | 0.70 | 0.04 | 0.62 to 0.79 | 7.5 | 0.74 | 0.58 | 0.32 |
| Sample 2 | 0.77 | 0.02 | 0.72 to 0.82 | 8.5 | 0.69 | 0.72 | 0.41 | |
| Intrusion | Sample 1 | 0.80 | 0.04 | 0.72 to 0.87 | 6.5 | 0.72 | 0.78 | 0.50 |
| Sample 2 | 0.85 | 0.02 | 0.81 to 0.89 | 5.5 | 0.86 | 0.74 | 0.60 | |
| Numbing | Sample 1 | 0.69 | 0.04 | 0.60 to 0.78 | 5.5 | 0.56 | 0.75 | 0.31 |
| Sample 2 | 0.80 | 0.02 | 0.76 to 0.85 | 5.5 | 0.70 | 0.77 | 0.47 | |
| Hyperarousal | Sample 1 | 0.87 | 0.03 | 0.81 to 0.93 | 5.5 | 0.80 | 0.83 | 0.63 |
| Sample 2 | 0.88 | 0.02 | 0.83 to 0.92 | 4.5 | 0.83 | 0.81 | 0.64 | |
| Sleep | Sample 1 | 0.81 | 0.04 | 0.74 to 0.88 | 3.5 | 0.74 | 0.79 | 0.53 |
| Sample 2 | 0.84 | 0.02 | 0.79 to 0.88 | 2.5 | 0.72 | 0.83 | 0.55 | |
| Irritability | Sample 1 | 0.83 | 0.03 | 0.76 to 0.89 | 1.5 | 0.96 | 0.54 | 0.50 |
| Sample 2 | 0.87 | 0.02 | 0.84 to 0.91 | 3.5 | 0.77 | 0.83 | 0.60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, A.M.; Al-Dossary, S.A.; Almarwani, A.M.; Atout, M.; Al-Amer, R.; Alkhamees, A.A. The Impact of Event Scale-Revised: Examining Its Cutoff Scores among Arab Psychiatric Patients and Healthy Adults within the Context of COVID-19 as a Collective Traumatic Event. Healthcare 2023, 11, 892. https://doi.org/10.3390/healthcare11060892
Ali AM, Al-Dossary SA, Almarwani AM, Atout M, Al-Amer R, Alkhamees AA. The Impact of Event Scale-Revised: Examining Its Cutoff Scores among Arab Psychiatric Patients and Healthy Adults within the Context of COVID-19 as a Collective Traumatic Event. Healthcare. 2023; 11(6):892. https://doi.org/10.3390/healthcare11060892
Chicago/Turabian StyleAli, Amira Mohammed, Saeed A. Al-Dossary, Abdulaziz Mofdy Almarwani, Maha Atout, Rasmieh Al-Amer, and Abdulmajeed A. Alkhamees. 2023. "The Impact of Event Scale-Revised: Examining Its Cutoff Scores among Arab Psychiatric Patients and Healthy Adults within the Context of COVID-19 as a Collective Traumatic Event" Healthcare 11, no. 6: 892. https://doi.org/10.3390/healthcare11060892