
An Approach to Improve the Effectiveness of the Video-Assisted Intubating Stylet Technique for Tracheal Intubation: A Case Series Report

Abstract
:1. Introduction
2. Case Series Presentation
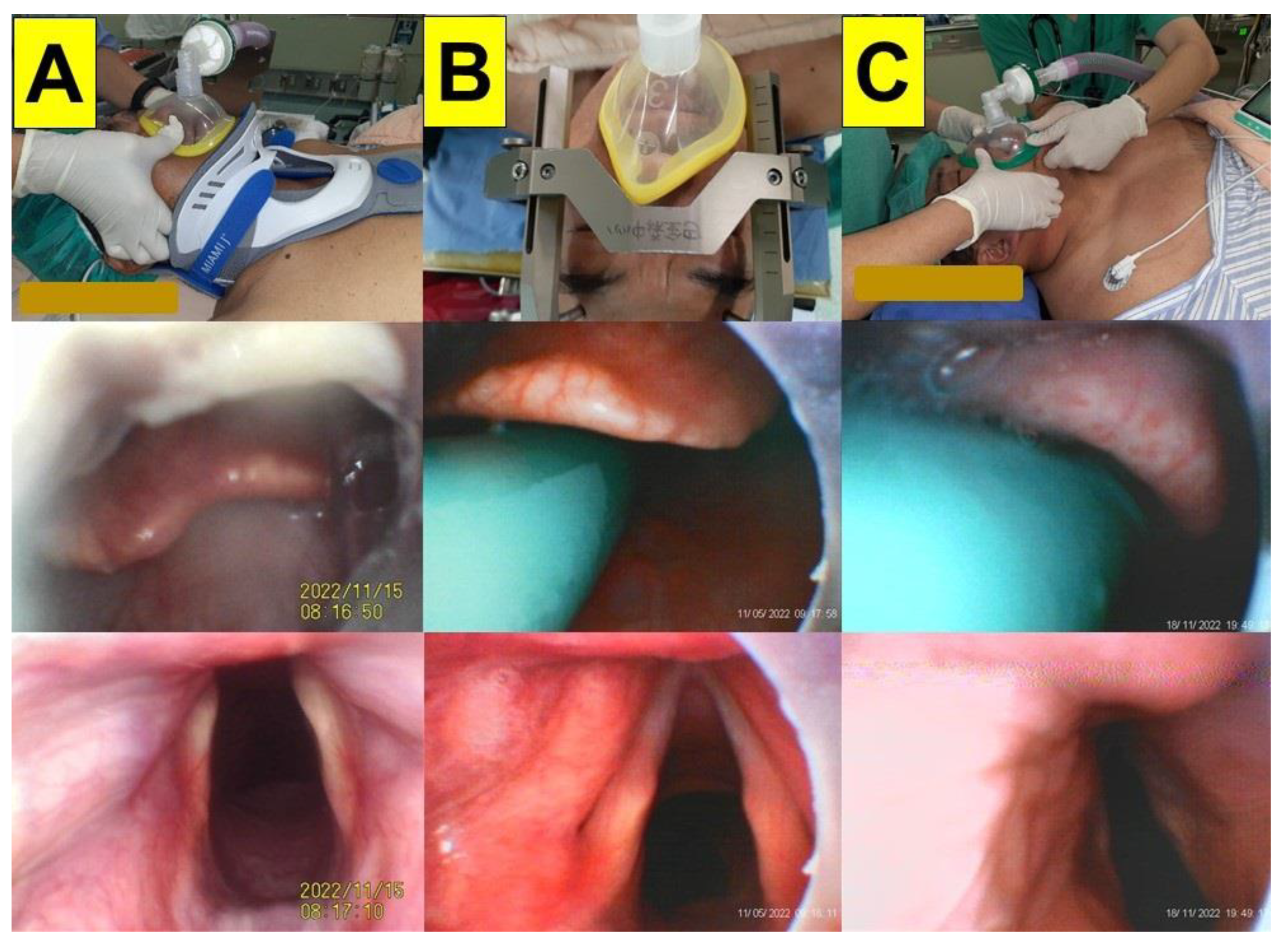
2.1. Case 1 (Limited Cervical Spine Mobility Due to Neck Collar)
2.2. Case 2 (Limited Cervical Spine Mobility Due to Headframe)
2.3. Case 3 (Morbid Obesity)
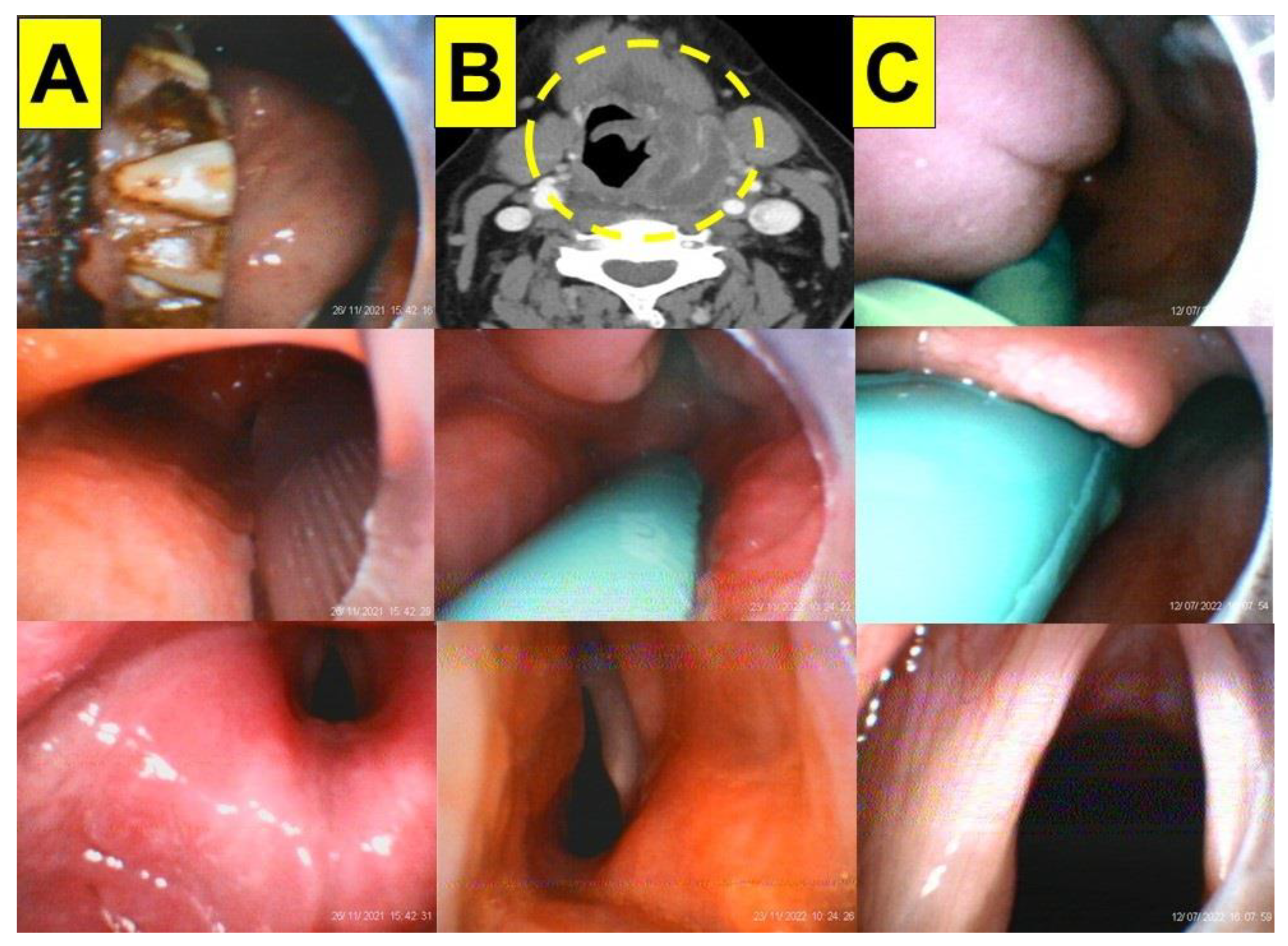
2.4. Case 4 (Morbid Obesity with Enlarged Tonsils)
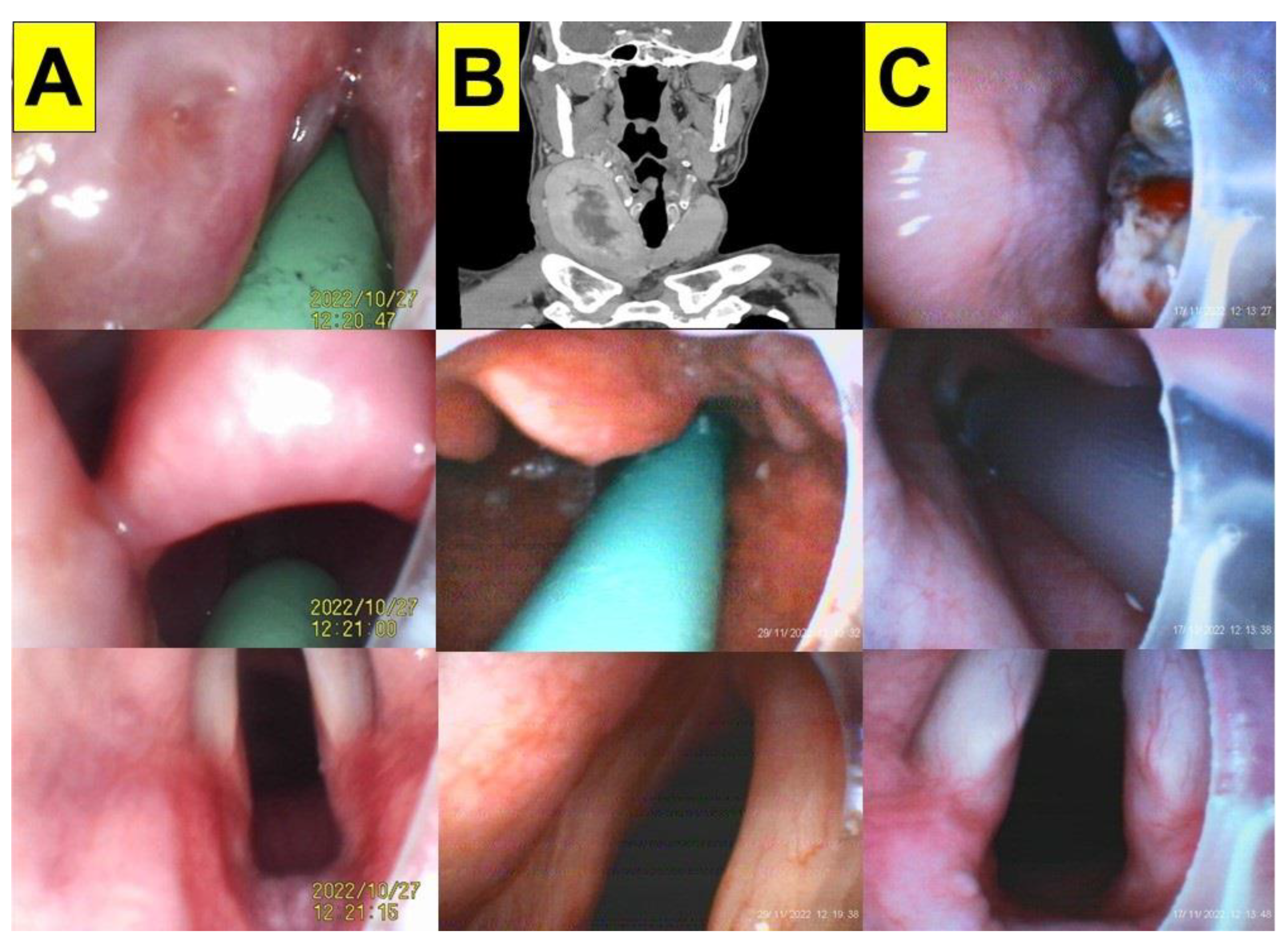
2.5. Case 5 (Enlarged Thyroid Glands)
2.6. Case 6 (Oral Cancer)
2.7. Case 7 (Facial Trauma)
2.8. Case 8 (Deep Neck Infection)
2.9. Case 9 (Rapid Sequence Induction and Intubation)
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, R.M. Use of a new videolaryngoscope (GlideScope) in the management of a difficult airway. Can. J. Anesth. 2003, 50, 611–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, R.M.; Pacey, J.A.; Bishop, M.J.; McCluskey, S.A. Early clinical experience with a new videolaryngoscope (GlideScope) in 728 patients. Can. J. Anesth. 2005, 52, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matek, J.; Kolek, F.; Klementova, O.; Michalek, P.; Vymazal, T. Optical devices in tracheal intubation-State of the art in 2020. Diagnostics 2021, 11, 575. [Google Scholar] [CrossRef] [PubMed]
- Nouruzi-Sedeh, P.; Schumann, M.; Groeben, H. Laryngoscopy via Macintosh blade versus GlideScope: Success rate and time for endotracheal intubation in untrained medical personnel. Anesthesiology 2009, 110, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: A multicentre randomized controlled trial. Br. J. Anesth. 2016, 116, 670–679. [Google Scholar] [CrossRef] [Green Version]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst. Rev. 2022, 4, CD011136. [Google Scholar] [CrossRef]
- Liem, E.B.; Bjoraker, D.G.; Gravenstein, D. New options for airway management: Intubating fibreoptic stylets. Br. J. Anesth. 2003, 91, 408–418. [Google Scholar] [CrossRef] [Green Version]
- Agrò, F.; Hung, O.R.; Cataldo, R.; Carassiti, M.; Gherardi, S. Lightwand intubation using the Trachlight: A brief review of current knowledge. Can. J. Anesth. 2001, 48, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Shikani, A.H. New “seeing” stylet-scope and method for the management of the difficult airway. Otolaryngol. Head Neck Surg. 1999, 120, 113–116. [Google Scholar] [CrossRef]
- Luk, H.N.; Luk, H.N.; Qu, J.Z.; Shikani, A. A paradigm shift of airway management: The role of video-assisted intubating stylet technique. In Advances in Tracheal Intubation [Working Title]; Jessica, L.-S., Ed.; IntechOpen [Internet]: London, UK, 2022. [Google Scholar] [CrossRef]
- Lee, A.R.; Yang, S.; Shin, Y.H.; Kim, J.A.; Chung, I.S.; Cho, H.S.; Lee, J.J. A comparison of the BURP and conventional and modified jaw thrust manoeuvres for orotracheal intubation using the Clarus Video System. Anaesthesia 2013, 68, 931–937. [Google Scholar] [CrossRef]
- Hsu, H.T.; Chou, S.H.; Chen, C.L.; Tseng, K.Y.; Kuo, Y.W.; Chen, M.K.; Cheng, K.I. Left endobronchial intubation with a double-lumen tube using direct laryngoscopy or the Trachway® video stylet. Anaesthesia 2013, 68, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.C.; Tseng, K.Y.; Shen, Y.C.; Lin, C.H.; Hsu, C.W.; Hsu, H.J.; Lu, I.C.; Cheng, K.I. Nasotracheal intubation in patients with limited mouth opening: A comparison between fibreoptic intubation and the Trachway®. Anaesthesia 2016, 71, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.C.; Cho, A.H.; Lin, J.R.; Chung, Y.T. The Clarus Video System (Trachway) and direct laryngoscope for endotracheal intubation with cricoid pressure in simulated rapid sequence induction intubation: A prospective randomized controlled trial. BMC Anesthesiol. 2019, 19, 33. [Google Scholar] [CrossRef]
- Yang, Y.L.; Huang, C.H.; Luk, H.N.; Tsai, P.B. Adaptation to the plastic barrier sheet to facilitate intubation during the COVID-19 pandemic. Anesth. Analg. 2020, 131, e97–e99. [Google Scholar] [CrossRef]
- Tsai, P.B.; Luk, H.N. Plastic sheet and video intubating stylet: A technical note. Asian J. Anesthesiol. 2021, 59, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.B.; Luk, H.-N. Sheet Barrier and Intubating Stylet. Encyclopedia 2021, 1, 1058–1075. [Google Scholar] [CrossRef]
- Luk, H.N.; Yang, Y.L.; Tsai, P.B. Application of plastic sheet barrier and video intubating stylet to protect tracheal intubators during Coronavirus Disease 2019 pandemic: A Taiwan experience. Cell Transplant. 2021, 30, 963689720987527, Erratum in Cell Transplant. 2021, 30, 9636897211027078. [Google Scholar] [CrossRef] [PubMed]
- Tsay, P.J.; Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted intubating stylet technique for difficult intubation: A case series report. Healthcare 2022, 10, 741. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of a video-assisted intubating stylet technique in a critically ill and contagious COVID-19 patient. Healthcare 2022, 10, 388. [Google Scholar] [CrossRef]
- Huang, C.H.; Su, I.M.; Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted stylet intubation with a plastic sheet barrier, a safe and simple technique for tracheal intubation of COVID-19 patients. Healthcare 2022, 10, 1105. [Google Scholar] [CrossRef]
- Shih, T.L.; Koay, K.P.; Hu, C.Y.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of the Shikani video-assisted intubating stylet technique in patients with restricted neck mobility. Healthcare 2022, 10, 1688. [Google Scholar] [CrossRef] [PubMed]
- Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-twin technique for airway management, combining video-intubating stylet with videolaryngoscope: A case Series report and review of the literature. Healthcare 2022, 10, 2175. [Google Scholar] [CrossRef] [PubMed]
- Thong, S.Y.; Wong, T.G. Clinical uses of the Bonfils retromolar intubation fiberscope: A review. Anesth. Analg. 2012, 115, 855–866. [Google Scholar] [CrossRef]
- Theiler, L.; Greif, R.; Bütikofer, L.; Arheart, K.; Kleine-Brueggeney, M. The skill of tracheal intubation with rigid scopes—A randomised controlled trial comparing learning curves in 740 intubations. BMC Anesthesiol. 2020, 20, 263. [Google Scholar] [CrossRef]
- Cook, T.; Kristensen, M. Core Topics in Airway Management, 3rd ed.; Cambridge University Press: Cambridge, UK, 2020. [Google Scholar] [CrossRef]
- Artime, C.A.; Hagberg, C.A. Airway management in the adult. In Miller’s Anesthesia, 9th ed.; Gropper, M.A., Eriksson, L., Fleisher, L., Wiener-Kronish, J., Cohen, N., Leslie, K., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; Chapter 44; pp. 1373–1412.e7. ISBN 9780323612647. [Google Scholar]
- Nørskov, A.K.; Rosenstock, C.V.; Wetterslev, J.; Astrup, G.; Afshari, A.; Lundstrøm, L.H. Diagnostic accuracy of anaesthesiologists’ prediction of difficult airway management in daily clinical practice: A cohort study of 188 064 patients registered in the Danish Anaesthesia Database. Anaesthesia 2015, 70, 272–281. [Google Scholar] [CrossRef]
- Heidegger, T. Management of the difficult airway. N. Engl. J. Med. 2021, 384, 1836–1847. [Google Scholar] [CrossRef]
- Law, J.A.; Duggan, L.V.; Asselin, M.; Baker, P.; Crosby, E.; Downey, A.; Hung, O.R.; Kovacs, G.; Lemay, F.; Noppens, R.; et al. Canadian Airway Focus Group. Canadian Airway Focus Group updated consensus-based recommendations for management of the difficult airway: Part 2. Planning and implementing safe management of the patient with an anticipated difficult airway. Can. J. Anaesth. 2021, 68, 1405–1436. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef]
- Yoon, H.K.; Lee, H.C.; Park, J.B.; Oh, H.; Park, H.P. McGrath MAC videolaryngoscope versus Optiscope Video Stylet for tracheal intubation in patients with manual inline cervical stabilization: A randomized trial. Anesth. Analg. 2020, 130, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Bathory, I.; Granges, J.C.; Frascarolo, P.; Magnusson, L. Evaluation of the Video Intubation Unit in morbid obese patients. Acta Anaesthesiol. Scand. 2010, 54, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Van Zundert, A.A.; Pieters, B.M. Combined technique using videolaryngoscopy and Bonfils for a difficult airway intubation. Br. J. Anaesth. 2012, 108, 327–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieters, B.M.; Theunissen, M.; van Zundert, A.A. Macintosh blade videolaryngoscopy combined with rigid Bonfils intubation endoscope offers a suitable alternative for patients with difficult airways. Anesth. Analg. 2018, 126, 988–994. [Google Scholar] [CrossRef] [PubMed]
- van Zundert, A.; van Zundert, T.; Brimacombe, J. Downfolding of the epiglottis during intubation. Anesth. Analg. 2010, 110, 1246–1247. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Y.; Lin, C.; Chen, C.C.; Teng, W.N.; Chen, K.H.; Lo, M.T.; Ting, C.K. Improvement in vocal-cord visualization with Trachway video intubating stylet using direct oxygen flow and effective analysis of the fraction of inspired oxygen: A bench study. J. Clin. Monit. Comput. 2022, 36, 1723–1730. [Google Scholar] [CrossRef]
- Fiore, M.P.; Marmer, S.L.; Steuerwald, M.T.; Thompson, R.J.; Galgon, R.E. Three airway management techniques for airway decontamination in massive emesis: A manikin study. West. J. Emerg. Med. 2019, 20, 784–790. [Google Scholar] [CrossRef]
- Root, C.W.; Mitchell, O.J.L.; Brown, R.; Evers, C.B.; Boyle, J.; Griffin, C.; West, F.M.; Gomm, E.; Miles, E.; McGuire, B.; et al. Suction assisted laryngoscopy and airway decontamination (SALAD): A technique for improved emergency airway management. Resusc. Plus 2020, 1–2, 100005. [Google Scholar] [CrossRef]
- Pirotte, A.; Panchananam, V.; Finley, M.; Petz, A.; Herrmann, T. Current considerations in emergency airway management. Curr. Emerg. Hosp. Med. Rep. 2022, 10, 73–86. [Google Scholar] [CrossRef]
- Tseng, K.Y.; Chau, S.W.; Su, M.P.; Shih, C.K.; Lu, I.C.; Cheng, K.I. A comparison of Trachway intubating stylet and Airway Scope for tracheal intubation by novice operators: A manikin study. Kaohsiung J. Med. Sci. 2012, 28, 448–451. [Google Scholar] [CrossRef] [Green Version]
- Hung, K.C.; Tan, P.H.; Lin, V.C.; Wang, H.K.; Chen, H.S. A comparison of the Trachway intubating stylet and the Macintosh laryngoscope in tracheal intubation: A manikin study. J. Anesth. 2013, 27, 205–210. [Google Scholar] [CrossRef]
- Ong, J.; Lee, C.L.; Huang, S.J.; Shyr, M.H. Comparison between the Trachway video intubating stylet and Macintosh laryngoscope in four simulated difficult tracheal intubations: A manikin study. Ci Ji Yi Xue Za Zhi 2016, 28, 109–112. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, A.; Kekec, A. Endotracheal intubation with optical stylet vs Macintosh laryngoscope performed on a manikin by medical students: A prospective manikin trial. J. Pak. Med. Assoc. 2019, 69, 1651–1656. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; An, S.; Park, S.; Nahm, F.S.; Han, S.H.; Kim, J.H. Comparison of a new video intubation stylet and McGrath® MAC video laryngoscope for intubation in an airway manikin with normal airway and cervical spine immobilization scenarios by novice personnel: A randomized crossover study. BioMed Res. Int. 2021, 2021, 4288367. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Yiang, G.T.; Ke, J.Y.; Chen, C.S.; Lin, P.C.; Chen, Y.L. Role of Trachway versus conventional modes of intubation in difficult airway management in COVID-19 setups. Emerg. Med. Int. 2021, 2021, 6614523. [Google Scholar] [CrossRef]
- Fu, D.; Li, W.; Li, W.; Han, Y. Improved skill for tracheal intubation using optical stylets through remote training model: A before and after interventional study. BMC Med. Educ. 2022, 22, 668. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 | Case 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Age/Gender | 56/M | 58/M | 25/M | 27/F | 47/M | 63/F | 45/M | 68/F | 18/F |
| BMI (kg/m2) | 23.4 | 36.4 | 44.7 | 42.2 | 23.8 | 25.6 | 27.6 | 30.8 | 23.4 |
| ASA Physical Status | II | III | II | III | I | I | I | III | II |
| Comorbidity | Hypertension | Hypertension, type II diabetes mellitus, and gout | Morbid obesity | Exotropia, benign intracranial hypertension, Foster Kennedy syndrome, morbid obesity, and obstructive sleep apnea syndrome. | Type II diabetes mellitus, hypertension, gall stones, lumbar spine disc herniation, gastroesophageal reflux disease, and esophagitis. | Systemic lupus erythematosus | |||
| Diagnosis | Cervical HIVD | Parkinson’s disease | Exotropia | Pituitary cyst | Thyroid goiter | Gum tumor | Facial trauma | Deep neck infection | Acute appendicitis |
| Surgery | ACDF | DBS | Recession and myectomy | Transsphenoidal removal | Thyroidectomy | Wide excision maxillectomy | Open reduction, graft, and wound debridement | Incision, drainage, and tracheostomy | Laparoscopic appendectomy |
| Induction | MDZ, FEN, PPF, and ROC | FEN, PPF, and ROC | FEN, PPF, and ROC | MDZ, FEN, PPF, and ROC | FEN, PPF, and ROC | FEN, PPF, ROC, and SCC | FEN, PPF, ROC, and SCC | MDZ, FEN, PPF, and SCC | FEN, PPF, ROC, and SCC |
| Maintenance | Desflurane | Sevoflurane | Sevoflurane | Sevoflurane | Sevoflurane | Sevoflurane | Sevoflurane | Sevoflurane | Sevoflurane |
| Airway Evaluation | Cervical collar | Stereotactic frame | Thick neck | Enlarged tonsils | Neck mass | Gum tumor mass | Blood in the oral cavity | Neck erythema, swelling | Normal |
| LQS Grading | Grade 2 | Grade 2 | Grade 2 | Grade 2 | Grade 1 | Grade 2 | Grade 1 | Grade 2 | Grade 1 |
| View of Glottis | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent |
| Success on First Attempt | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Intubation Time | 58 s | 21 s | 20 s | 42 s | 15 s | 23 s | 20 s | 19 s | 9 s |
| Complications | Nil | Nil | Nil | Nil | Nil | Nil | Nil | Nil | Nil |
| Subjective Satisfaction | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent | Excellent |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lan, C.-H.; Luk, H.-N.; Qu, J.Z.; Shikani, A. An Approach to Improve the Effectiveness of the Video-Assisted Intubating Stylet Technique for Tracheal Intubation: A Case Series Report. Healthcare 2023, 11, 891. https://doi.org/10.3390/healthcare11060891
Lan C-H, Luk H-N, Qu JZ, Shikani A. An Approach to Improve the Effectiveness of the Video-Assisted Intubating Stylet Technique for Tracheal Intubation: A Case Series Report. Healthcare. 2023; 11(6):891. https://doi.org/10.3390/healthcare11060891
Chicago/Turabian StyleLan, Cing-Hong, Hsiang-Ning Luk, Jason Zhensheng Qu, and Alan Shikani. 2023. "An Approach to Improve the Effectiveness of the Video-Assisted Intubating Stylet Technique for Tracheal Intubation: A Case Series Report" Healthcare 11, no. 6: 891. https://doi.org/10.3390/healthcare11060891