
Motor-Sparing Effect of Adductor Canal Block for Knee Analgesia: An Updated Review and a Subgroup Analysis of Randomized Controlled Trials Based on a Corrected Classification System
 , , ,
, , ,
Abstract
:1. Introduction
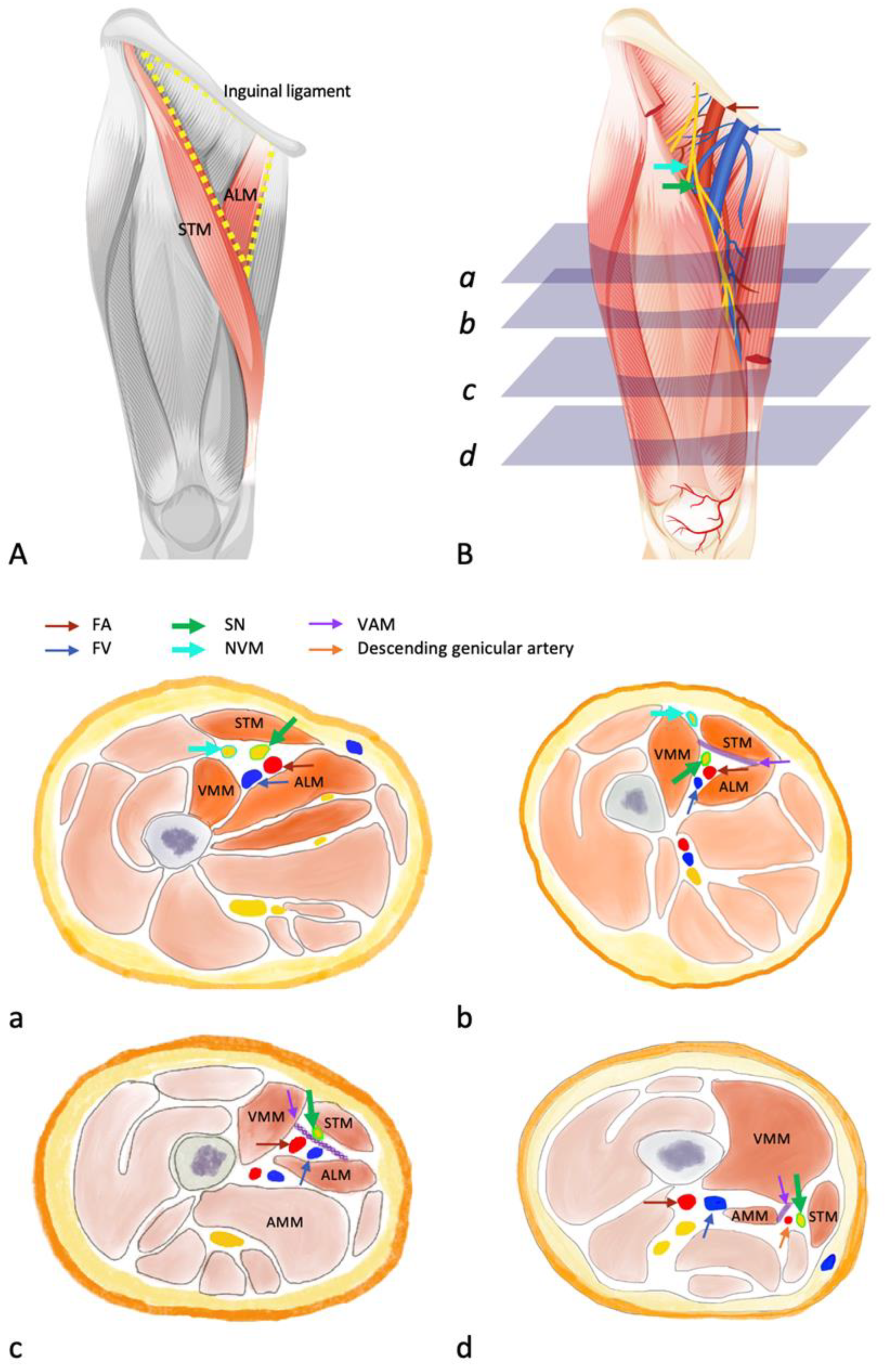
1.1. Applied Anatomy
1.1.1. Femoral Triangle (FT, Scarpa’s Triangle)
1.1.2. Adductor Canal (Hunter’s Canal)
1.1.3. Knee Sensory Innervation
1.2. Corrected Classification System
1.3. Femoral Triangle Block (FTB)
1.4. Proximal ACB (p-ACB)
1.5. Distal ACB (d-ACB)
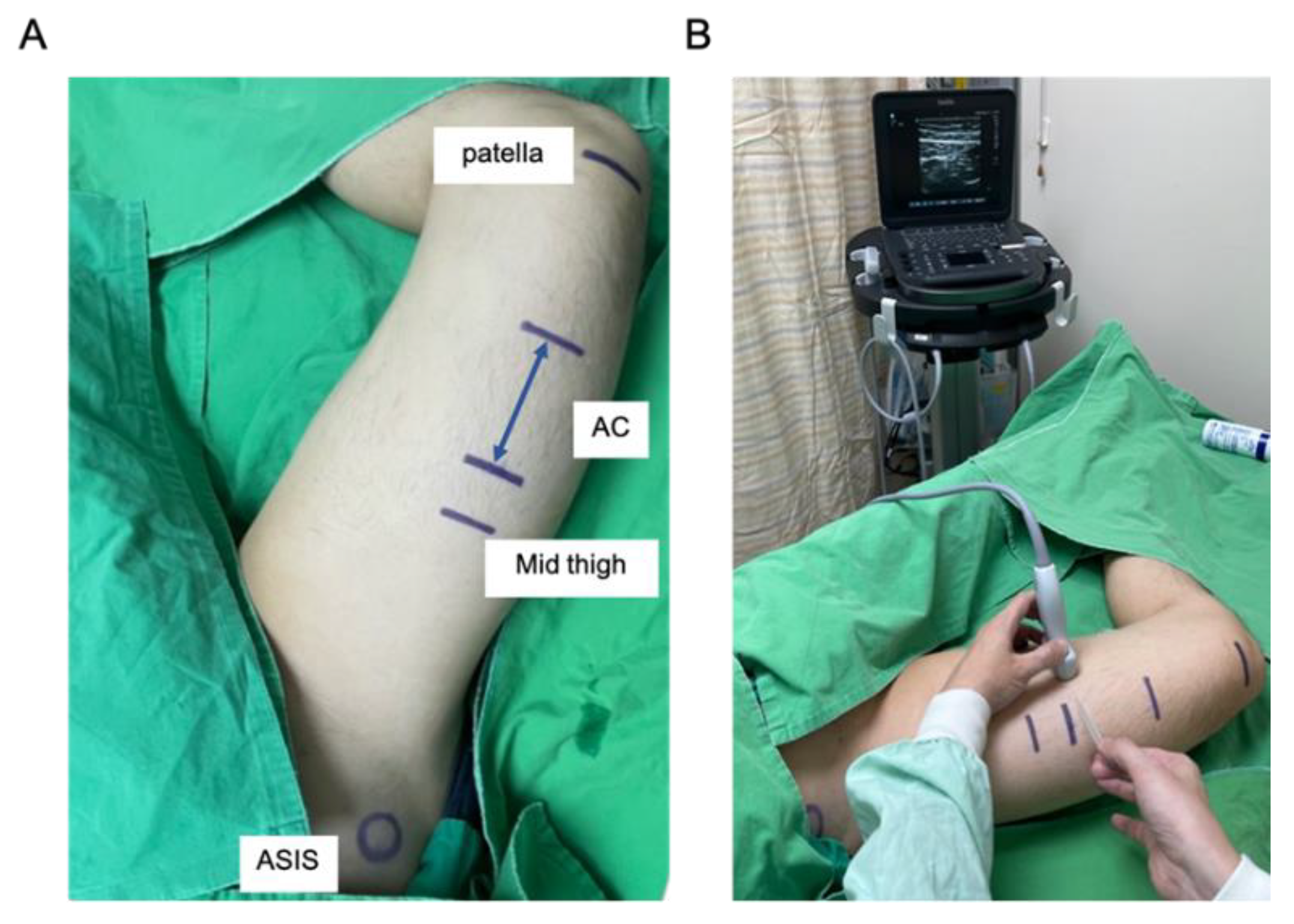
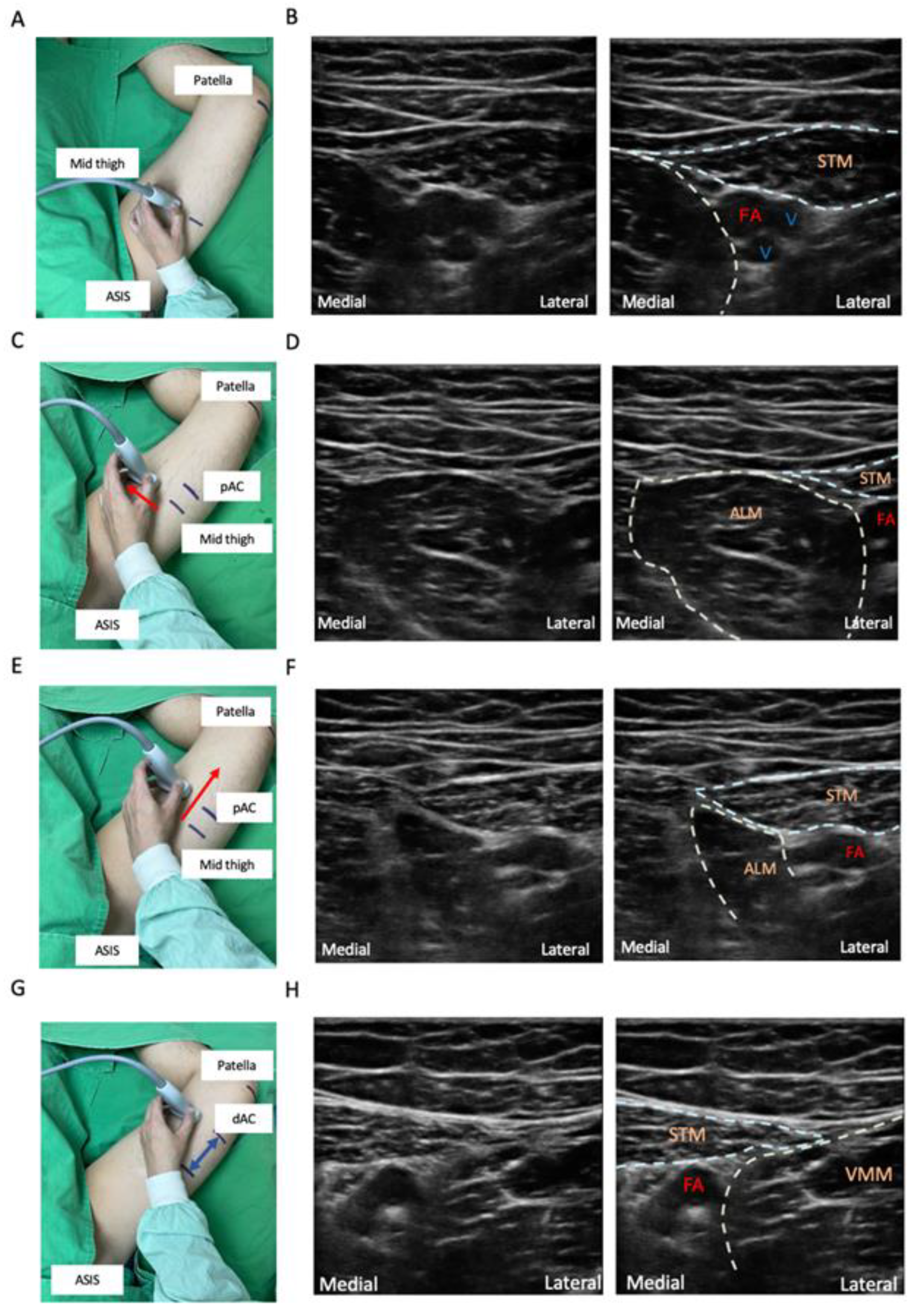
1.6. ACB Techniques
- Mark the location midway between the anterior superior iliac spine (ASIS) and the base of the patella. Place the transducer transversely on the marker of the thigh to obtain a short-axis view. The femoral vessels will be identified beneath the sartorius muscle. The artery can be distinguished by color doppler flow imaging or by compression sign (Figure 3A,B).
- Slide the probe along the medial border of the sartorius muscle to visualize the intersection of the medial borders of the sartorius muscle and the adductor longus muscle. This point means the start of the AC (Figure 3C–F).
- Slide the probe caudally until the femoral artery goes deep into the echogenic adductor magnus tendon and then passes through the adductor hiatus. This point is the end of the AC (Figure 3G,H).
1.7. Ultrasound-Guided FTB
- After identifying the AC, place the probe halfway between the base of the patella and the ASIS for a transverse view. The superficial femoral artery (SFA) is identified underneath the sartorius muscle. The SN is usually visible as a hyperechoic structure anterolateral to the artery typically [7,65].
- Once the neurovascular bundle is seen, adjust the probe so that the bundle is on the medial side of the ultrasound screen. The needle is placed lateral to the SN and femoral artery using an in-plane technique. A periarterial injection of local anesthetics is performed at this level, involving the SN, NVM, and medial and intermediate femoral cutaneous nerves [41]. It may also affect the motor branches of the femoral nerve [7].
1.8. Ultrasound-Guided p-ACB
- At the distal FT, move the probe caudally about 1–2 cm beyond the apex of the FT. At this level, SN can usually be visualized laterally to the SFA with the thigh in external rotation, and injection between the SFA and SN helps achieve a successful ACB with 2–5 mL of local anesthetics.
1.9. Ultrasound-Guided d-ACB
1.10. Systematic Review of RCTs on the Divergent Definition of ACB
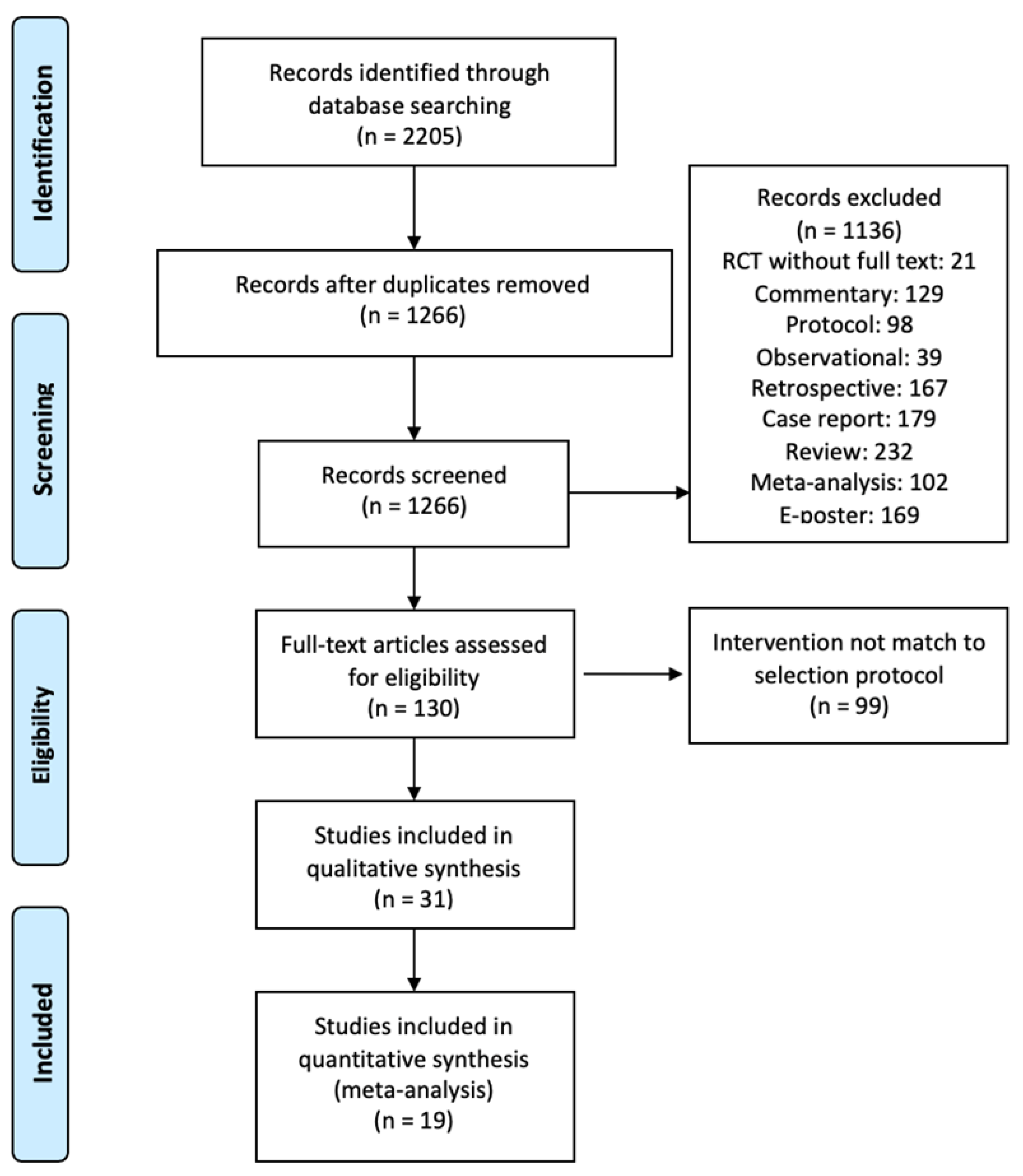
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- (1)
- Study type: clinical RCTs
- (2)
- Subjects: patients who underwent knee surgeries without limitations
- (3)
- Interventions: comparison of ACB with other methods for knee surgeries, including local infiltration, periarticular local anesthetic infiltration, FNB, interspace between the popliteal artery and the capsule of the posterior knee block, and epidural analgesia, after knee surgery.
- (1)
- Non-English articles
- (2)
- No full text available
3. Results
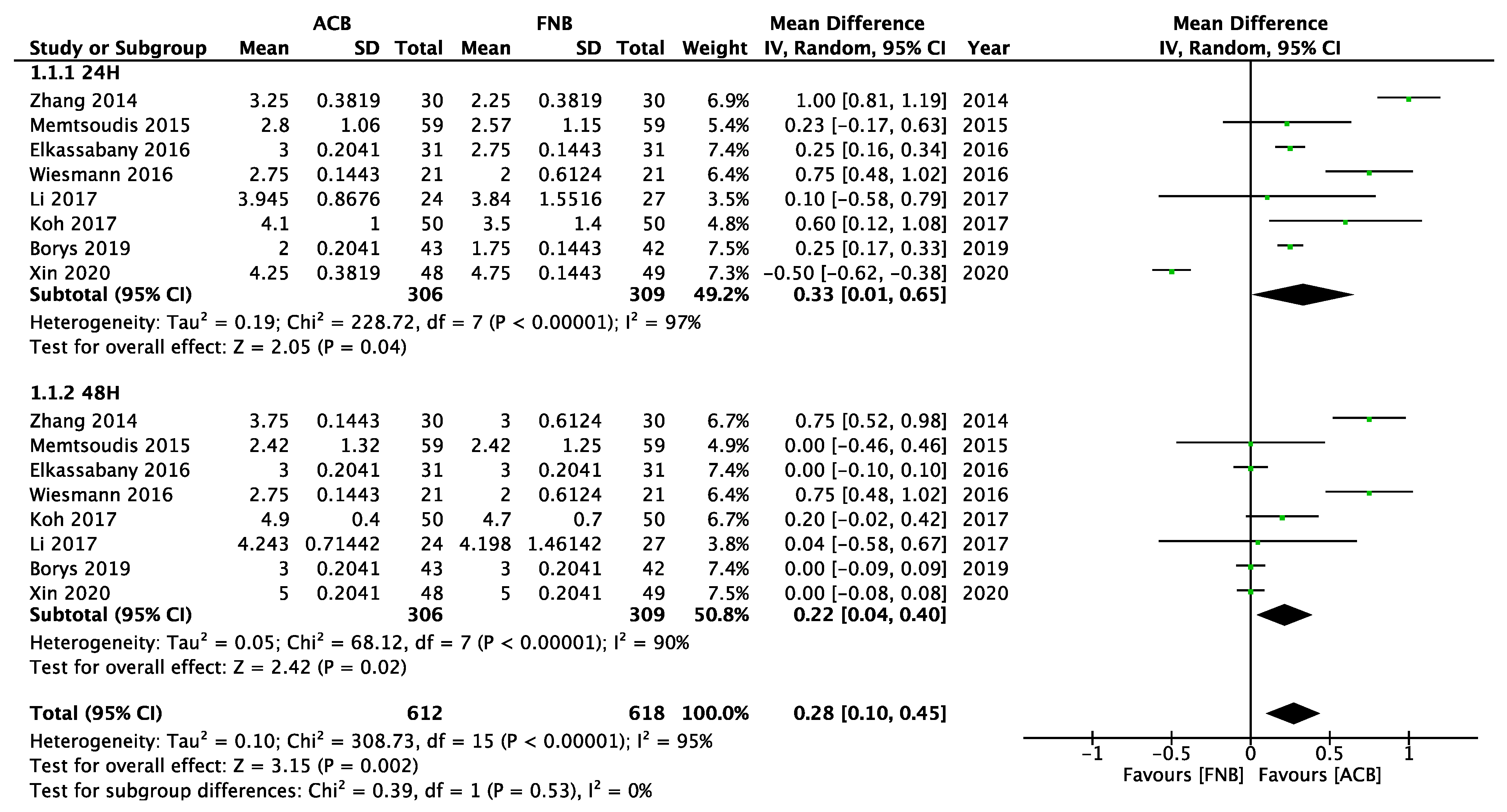
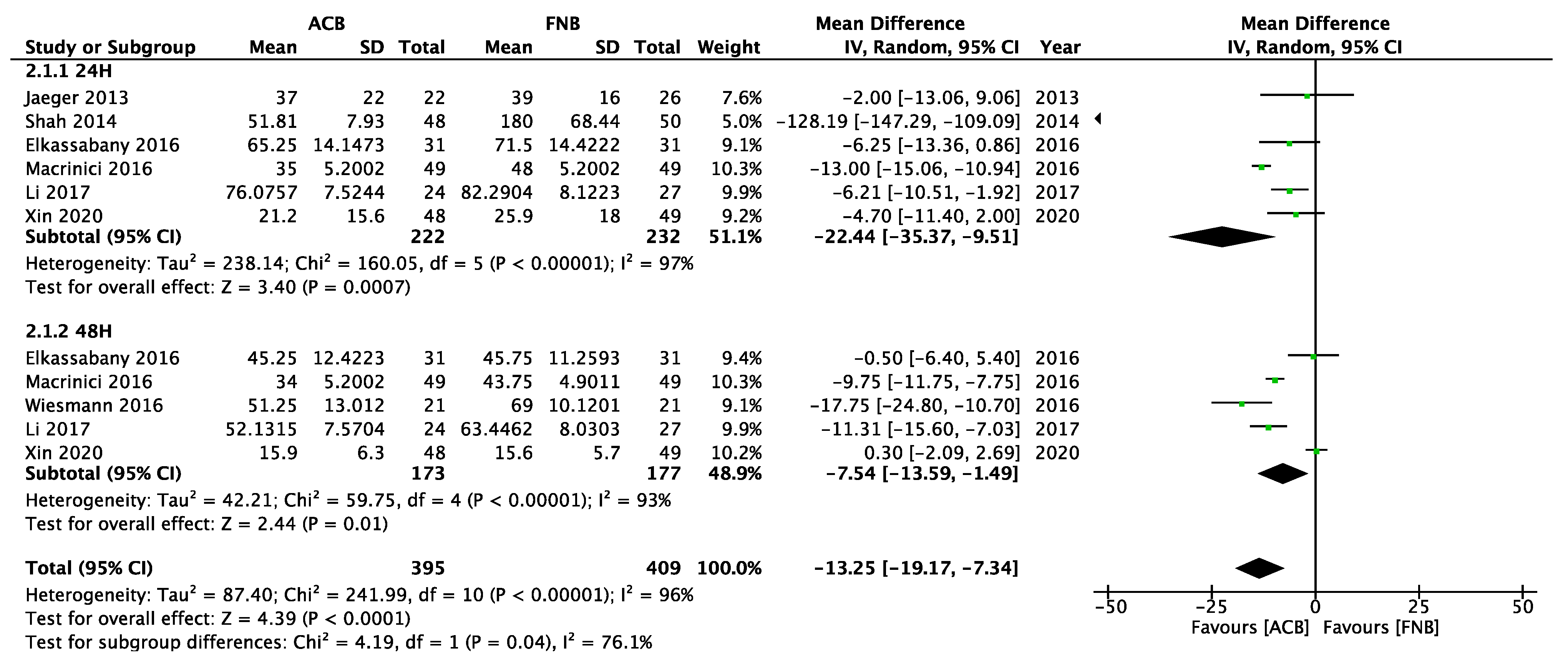
3.1. The Clinical Effect of Mixed ACB versus FNB
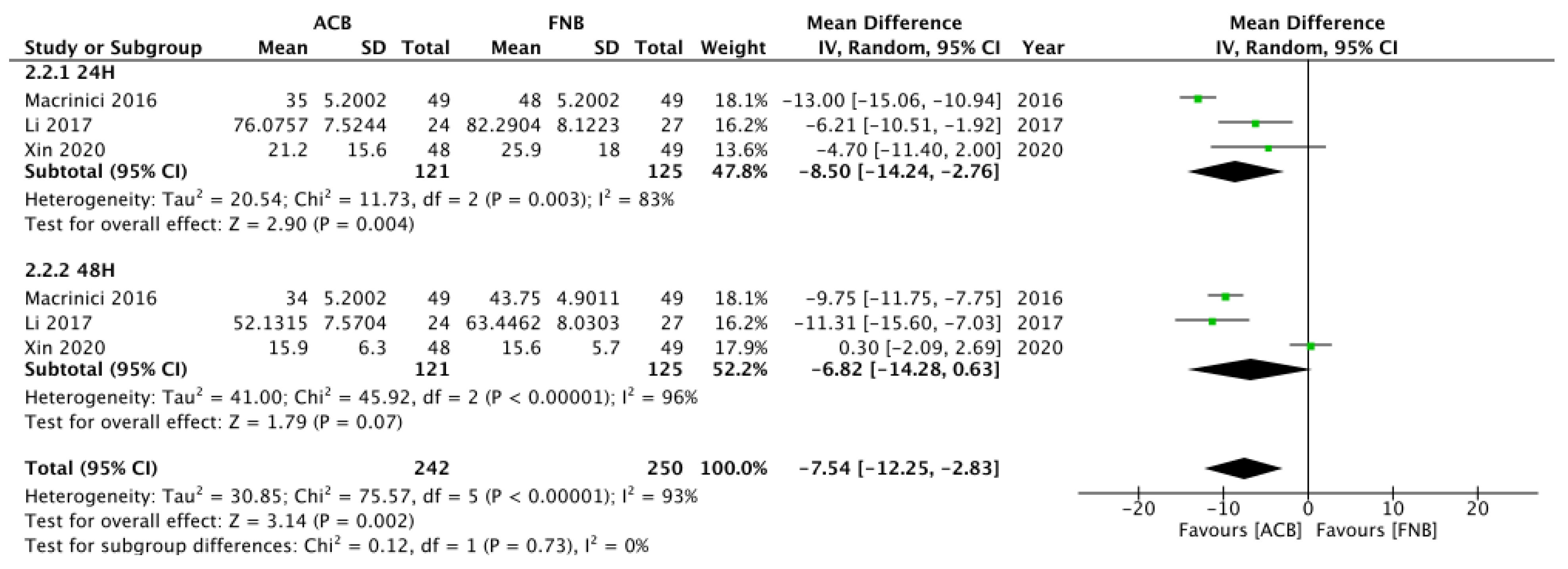
3.2. The Effect of p-ACB versus d-ACB
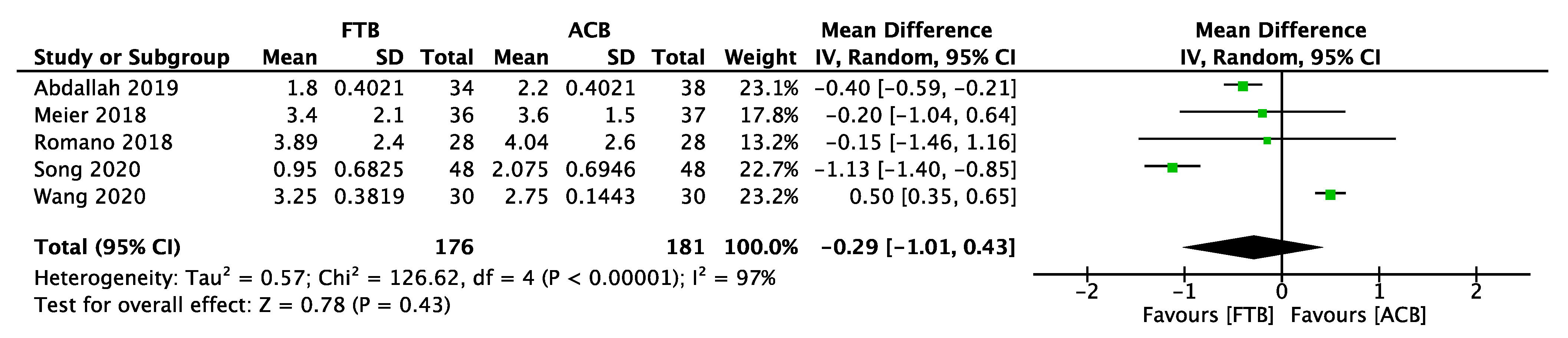
3.3. The Effect of True ACB versus FTB
4. Other Considerations
4.1. Complications
4.2. Local Anesthetic Volume and Concentration
4.3. Continuous versus Single-Shot ACB
4.4. Perineural Adjuvant of FTB
4.5. ACB for Anterior Cruciate Ligament (ACL) Surgery
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paul, J.E.; Arya, A.; Hurlburt, L.; Cheng, J.; Thabane, L.; Tidy, A.; Murthy, Y. Femoral Nerve Block Improves Analgesia Outcomes after Total Knee Arthroplasty: A Meta-analysis of Randomized Controlled Trials. Anesthesiology 2010, 113, 1144–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, M.; Wang, L.; Onibonoje, O.K.; Parrett, C.; Sessler, D.I.; Mounir-Soliman, L.; Zaky, S.; Krebs, V.; Buller, L.T.; Donohue, M.C. Continuous femoral nerve blocks: Decreasing local anesthetic concentration to minimize quadriceps femoris weakness. J. Am. Soc. Anesthesiol. 2012, 116, 665–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.V.; Thiayagarajan, M.K.; Venkatesh, S. An Exact Localization of Adductor Canal and Its Clinical Significance: A Cadaveric Study. Anesth. Essays Res. 2019, 13, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Jaeger, P.; Nielsen, Z.J.; Henningsen, M.H.; Hilsted, K.L.; Mathiesen, O.; Dahl, J.B. Adductor canal block versus femoral nerve block and quadriceps strength: A randomized, double-blind, placebo-controlled, crossover study in healthy volunteers. Anesthesiology 2013, 118, 409–415. [Google Scholar] [CrossRef]
- Kwofie, M.K.; Shastri, U.D.; Gadsden, J.C.; Sinha, S.K.; Abrams, J.H.; Xu, D.; Salviz, E.A. The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk: A blinded, randomized trial of volunteers. Reg. Anesth. Pain Med. 2013, 38, 321–325. [Google Scholar] [CrossRef]
- Grevstad, U.; Mathiesen, O.; Valentiner, L.S.; Jaeger, P.; Hilsted, K.L.; Dahl, J.B. Effect of adductor canal block versus femoral nerve block on quadriceps strength, mobilization, and pain after total knee arthroplasty: A randomized, blinded study. Reg. Anesth. Pain Med. 2015, 40, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Vora, M.U.; Nicholas, T.A.; Kassel, C.A.; Grant, S.A. Adductor canal block for knee surgical procedures: Review article. J. Clin. Anesth. 2016, 35, 295–303. [Google Scholar] [CrossRef]
- Lund, J.; Jenstrup, M.T.; Jaeger, P.; Sørensen, A.M.; Dahl, J.B. Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: Preliminary results. Acta Anaesthesiol. Scand. 2010, 55, 14–19. [Google Scholar] [CrossRef]
- Jenstrup, M.T.; Jæger, P.; Lund, J.; Fomsgaard, J.S.; Bache, S.; Mathiesen, O.; Larsen, T.K.; Dahl, J.B. Effects of adductor-canal-blockade on pain and ambulation after total knee arthroplasty: A randomized study. Acta Anaesthesiol. Scand. 2012, 56, 357–364. [Google Scholar] [CrossRef]
- Van Der Wal, M.; Lang, S.A.; Yip, R.W. Transsartorial approach for saphenous nerve block. Can. J. Anaesth. 1993, 40, 542–546. [Google Scholar] [CrossRef]
- Horn, J.L.; Pitsch, T.; Salinas, F.; Benninger, B. Anatomic basis to the ultrasound-guided approach for saphenous nerve blockade. Reg. Anesth. Pain Med. 2009, 34, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krombach, J.; Gray, A.T. Sonography for saphenous nerve block near the adductor canal. Reg. Anesth. Pain Med. 2007, 32, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Manickam, B.; Perlas, A.; Duggan, E.; Brull, R.; Chan, V.W.; Ramlogan, R. Feasibility and efficacy of ultrasound-guided block of the saphenous nerve in the adductor canal. Reg. Anesth. Pain Med. 2009, 34, 578–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdallah, F.W.; Whelan, D.B.; Chan, V.W.; Prasad, G.A.; Endersby, R.V.; Theodoropolous, J.; Oldfield, S.; Oh, J.; Brull, R. Adductor Canal Block Provides Noninferior Analgesia and Superior Quadriceps Strength Compared with Femoral Nerve Block in Anterior Cruciate Ligament Reconstruction. Anesthesiology 2016, 124, 1053–1064. [Google Scholar] [CrossRef] [PubMed]
- Jæger, P.; Koscielniak-Nielsen, Z.J.; Schrøder, H.M.; Mathiesen, O.; Henningsen, M.H.; Lund, J.; Jenstrup, M.T.; Dahl, J.B. Adductor canal block for postoperative pain treatment after revision knee arthroplasty: A blinded, randomized, placebo-controlled study. PLoS ONE 2014, 9, e111951. [Google Scholar] [CrossRef] [PubMed]
- Thacher, R.R.; Hickernell, T.R.; Grosso, M.J.; Shah, R.; Cooper, H.J.; Maniker, R.; Brown, A.R.; Geller, J. Decreased risk of knee buckling with adductor canal block versus femoral nerve block in total knee arthroplasty: A retrospective cohort study. Arthroplast. Today 2017, 3, 281–285. [Google Scholar] [CrossRef] [Green Version]
- Elkassabany, N.M.; Antosh, S.; Ahmed, M.; Nelson, C.; Israelite, C.; Badiola, I.; Cai, L.F.; Williams, R.; Hughes, C.; Mariano, E.R.; et al. The Risk of Falls After Total Knee Arthroplasty with the Use of a Femoral Nerve Block Versus an Adductor Canal Block: A Double-Blinded Randomized Controlled Study. Anesth Analg 2016, 122, 1696–1703. [Google Scholar] [CrossRef]
- Bolarinwa, S.A.; Novicoff, W.; Cui, Q. Reducing costly falls after total knee arthroplasty. World J. Orthop. 2018, 9, 198–202. [Google Scholar] [CrossRef]
- Rahimzadeh, P.; Faiz, H.R.; Imani, F.; Hobika, G.G.; Abbasi, A.; Nader, N.D. Relieving Pain After Arthroscopic Knee Surgery: Ultrasound-Guided Femoral Nerve Block or Adductor Canal Block? Turk. J. Anaesthesiol. Reani. 2017, 45, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Runner, R.P.; Boden, S.A.; Godfrey, W.S.; Premkumar, A.; Samady, H.; Gottschalk, M.B.; Xerogeanes, J.W. Quadriceps Strength Deficits After a Femoral Nerve Block Versus Adductor Canal Block for Anterior Cruciate Ligament Reconstruction: A Prospective, Single-Blinded, Randomized Trial. Orthop. J. Sports Med. 2018, 6, 2325967118797990. [Google Scholar] [CrossRef]
- Lim, Y.C.; Quek, H.Y.K.; Phoo, W.H.J.; Mah, C.L.; Tan, S. A randomised controlled trial comparing adductor canal block and femoral nerve block for knee arthroplasty. Singap. Med. J. 2019, 60, 145–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deloach, J.K.; Boezaart, A.P. Is an adductor canal block simply an indirect femoral nerve block? Anesthesiology 2014, 121, 1349–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sztain, J.F.; Khatibi, B.; Monahan, A.M.; Said, E.T.; Abramson, W.B.; Gabriel, R.A.; Finneran, J.J.t.; Bellars, R.H.; Nguyen, P.L.; Ball, S.T.; et al. Proximal Versus Distal Continuous Adductor Canal Blocks: Does Varying Perineural Catheter Location Influence Analgesia? A Randomized, Subject-Masked. Control. Clin. Trial. Anesth. Analg. 2018, 127, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Romano, C.; Lloyd, A.; Nair, S.; Wang, J.Y.; Viswanathan, S.; Vydyanathan, A.; Gritsenko, K.; Shaparin, N.; Kosharskyy, B. A Randomized Comparison of Pain Control and Functional Mobility between Proximal and Distal Adductor Canal Blocks for Total Knee Replacement. Anesth. Essays Res. 2018, 12, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Tulgar, S.; Selvi, O. Ultrasound guided distal adductor canal block provides effective postoperative analgesia in lower leg surgery. J. Clin. Anesth. 2018, 45, 51. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, T.F.; Moriggl, B.; Chan, V.; Pedersen, E.M.; Børglum, J. Redefining the adductor canal block. Reg. Anesth. Pain Med. 2014, 39, 442–443. [Google Scholar] [CrossRef]
- Panchamia, J.K.; Niesen, A.D.; Amundson, A.W. Adductor Canal Versus Femoral Triangle: Let Us All Get on the Same Page. Anesth. Analg. 2018, 127, e50. [Google Scholar] [CrossRef]
- Grevstad, U.; Jæger, P.; Sørensen, J.K.; Gottschau, B.; Ilfeld, B.; Ballegaard, M.; Hagelskjaer, M.; Dahl, J.B. The Effect of Local Anesthetic Volume within the Adductor Canal on Quadriceps Femoris Function Evaluated by Electromyography: A Randomized, Observer- and Subject-Blinded, Placebo-Controlled Study in Volunteers. Anesth. Analg. 2016, 123, 493–500. [Google Scholar] [CrossRef]
- Sørensen, J.K.; Jæger, P.; Dahl, J.B.; Gottschau, B.; Stephensen, S.L.; Grevstad, U. The Isolated Effect of Adductor Canal Block on Quadriceps Femoris Muscle Strength After Total Knee Arthroplasty: A Triple-Blinded, Randomized, Placebo-Controlled Trial with Individual Patient Analysis. Anesth. Analg. 2016, 122, 553–558. [Google Scholar] [CrossRef]
- Grevstad, U.; Mathiesen, O.; Lind, T.; Dahl, J.B. Effect of adductor canal block on pain in patients with severe pain after total knee arthroplasty: A randomized study with individual patient analysis. Br. J. Anaesth. 2014, 112, 912–919. [Google Scholar] [CrossRef]
- Henningsen, M.H.; Jaeger, P.; Hilsted, K.L.; Dahl, J.B. Prevalence of saphenous nerve injury after adductor-canal-blockade in patients receiving total knee arthroplasty. Acta Anaesthesiol. Scand. 2013, 57, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Jæger, P.; Zaric, D.; Fomsgaard, J.S.; Hilsted, K.L.; Bjerregaard, J.; Gyrn, J.; Mathiesen, O.; Larsen, T.K.; Dahl, J.B. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: A randomized, double-blind study. Reg. Anesth. Pain. Med. 2013, 38, 526–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mudumbai, S.C.; Kim, T.E.; Howard, S.K.; Workman, J.J.; Giori, N.; Woolson, S.; Ganaway, T.; King, R.; Mariano, E.R. Continuous adductor canal blocks are superior to continuous femoral nerve blocks in promoting early ambulation after TKA. Clin. Orthop. Relat. Res. 2014, 472, 1377–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, N.A.; Jain, N.P. Is continuous adductor canal block better than continuous femoral nerve block after total knee arthroplasty? Effect on ambulation ability, early functional recovery and pain control: A randomized controlled trial. J. Arthroplast. 2014, 29, 2224–2229. [Google Scholar] [CrossRef]
- Shah, N.A.; Jain, N.P.; Panchal, K.A. Adductor Canal Blockade Following Total Knee Arthroplasty-Continuous or Single Shot Technique? Role in Postoperative Analgesia, Ambulation Ability and Early Functional Recovery: A Randomized Controlled Trial. J. Arthroplast. 2015, 30, 1476–1481. [Google Scholar] [CrossRef]
- Wong, W.Y.; Bjørn, S.; Strid, J.M.; Børglum, J.; Bendtsen, T.F. Defining the Location of the Adductor Canal Using Ultrasound. Reg. Anesth. Pain Med. 2017, 42, 241–245. [Google Scholar] [CrossRef] [Green Version]
- Pascarella, G.; Costa, F.; Del Buono, R.; Agrò, F.E. Adductor canal and femoral triangle: Two different rooms with the same door. Saudi. J. Anaesth. 2019, 13, 276–277. [Google Scholar] [CrossRef]
- Pascarella, G.; Costa, F.; Del Buono, R.; Strumia, A.; Agrò, F.E. Adductor canal or femoral triangle block: Not a conundrum but a continuum. Br. J. Anaesth. 2020, 125, e233–e234, Comment on Br. J. Anaesth. 2020, 124, e194–e195. [Google Scholar] [CrossRef]
- Sondekoppam, R.V.; Johnston, D.F.; Ranganath, Y.S.; Parra, M.C.; Marian, A.A. Adductor canal or femoral triangle block: The continuity conundrum. Br. J. Anaesth. 2020, 124, e194–e195. [Google Scholar] [CrossRef]
- Basinger, H.; Hogg, J.P. Anatomy, Abdomen and Pelvis, Femoral Triangle; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2020. [Google Scholar]
- Bendtsen, T.F.; Moriggl, B.; Chan, V.; Børglum, J. The Optimal Analgesic Block for Total Knee Arthroplasty. Reg. Anesth. Pain Med. 2016, 41, 711–719. [Google Scholar] [CrossRef]
- Refai, N.A.; Tadi, P. Anatomy, Bony Pelvis and Lower Limb, Thigh Femoral Nerve; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2020. [Google Scholar]
- Bendtsen, T.F.; Moriggl, B.; Chan, V.; Pedersen, E.M.; Børglum, J. Defining adductor canal block. Reg. Anesth. Pain Med. 2014, 39, 253–254. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, T.F.; Moriggl, B.; Chan, V.; Børglum, J. Basic Topography of the Saphenous Nerve in the Femoral Triangle and the Adductor Canal. Reg. Anesth. Pain Med. 2015, 40, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Tubbs, R.S.; Loukas, M.; Shoja, M.M.; Apaydin, N.; Oakes, W.J.; Salter, E.G. Anatomy and potential clinical significance of the vastoadductor membrane. Surg. Radiol. Anat. 2007, 29, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Burckett-St Laurant, D.; Peng, P.; Girón Arango, L.; Niazi, A.U.; Chan, V.W.; Agur, A.; Perlas, A. The Nerves of the Adductor Canal and the Innervation of the Knee: An Anatomic Study. Reg. Anesth. Pain. Med. 2016, 41, 321–327. [Google Scholar] [CrossRef]
- Mathew, K.; Varacallo, M. Anatomy, Bony Pelvis and Lower Limb, Saphenous Nerve, Artery, and Vein; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2020. [Google Scholar]
- Migirov, A.; Vilella, R.C. Anatomy, Abdomen and Pelvis, Adductor Canal (Subsartorial, Hunter’s Canal); StatPearls Publishing LLC.: Treasure Island, FL, USA, 2020. [Google Scholar]
- Horner, G.; Dellon, A.L. Innervation of the human knee joint and implications for surgery. Clin. Orthop. Relat. Res. 1994, 301, 221–226. [Google Scholar] [CrossRef]
- Andersen, H.L.; Andersen, S.L.; Tranum-Jensen, J. The spread of injectate during saphenous nerve block at the adductor canal: A cadaver study. Acta Anaesthesiol. Scand. 2015, 59, 238–245. [Google Scholar] [CrossRef]
- Ozer, H.; Tekdemir, I.; Elhan, A.; Turanli, S.; Engebretsen, L. A clinical case and anatomical study of the innervation supply of the vastus medialis muscle. Knee. Surg. Sport. Traumatol. Arthrosc. 2004, 12, 119–122. [Google Scholar] [CrossRef]
- Johnston, D.F.; Black, N.D.; Cowden, R.; Turbitt, L.; Taylor, S. Spread of dye injectate in the distal femoral triangle versus the distal adductor canal: A cadaveric study. Reg. Anesth. Pain Med. 2019, 44, 39–45. [Google Scholar] [CrossRef]
- Orduña Valls, J.M.; Vallejo, R.; López Pais, P.; Soto, E.; Torres Rodríguez, D.; Cedeño, D.L.; Tornero Tornero, C.; Quintáns Rodríguez, M.; Baluja González, A.; Álvarez Escudero, J. Anatomic and Ultrasonographic Evaluation of the Knee Sensory Innervation: A Cadaveric Study to Determine Anatomic Targets in the Treatment of Chronic Knee Pain. Reg. Anesth. Pain Med. 2017, 42, 90–98. [Google Scholar] [CrossRef]
- Tran, J.; Peng, P.W.H.; Lam, K.; Baig, E.; Agur, A.M.R.; Gofeld, M. Anatomical Study of the Innervation of Anterior Knee Joint Capsule: Implication for Image-Guided Intervention. Reg. Anesth. Pain Med. 2018, 43, 407–414. [Google Scholar] [CrossRef]
- Tran, J.; Peng, P.W.H.; Gofeld, M.; Chan, V.; Agur, A.M.R. Anatomical study of the innervation of posterior knee joint capsule: Implication for image-guided intervention. Reg. Anesth. Pain Med. 2019, 44, 234–238. [Google Scholar] [CrossRef]
- Vloka, J.D.; Hadzić, A.; Drobnik, L.; Ernest, A.; Reiss, W.; Thys, D.M. Anatomical landmarks for femoral nerve block: A comparison of four needle insertion sites. Anesth. Analg. 1999, 89, 1467–1470. [Google Scholar] [PubMed]
- Jæger, P.; Lund, J.; Jenstrup, M.T.; Brøndum, V.; Dahl, J.B. Reply to Dr Bendtsen. Reg. Anesth. Pain Med. 2014, 39, p. 254–255. [Google Scholar] [CrossRef]
- Runge, C.; Moriggl, B.; Børglum, J.; Bendtsen, T.F. The Spread of Ultrasound-Guided Injectate From the Adductor Canal to the Genicular Branch of the Posterior Obturator Nerve and the Popliteal Plexus: A Cadaveric Study. Reg. Anesth. Pain Med. 2017, 42, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Chan, V.W.S.; Peng, P.W.H.; Agur, A.M.R. Evaluation of the proximal adductor canal block injectate spread: A cadaveric study. Reg. Anesth. Pain Med. 2019, 45, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Goffin, P.; Lecoq, J.P.; Ninane, V.; Brichant, J.F.; Sala-Blanch, X.; Gautier, P.E.; Bonnet, P.; Carlier, A.; Hadzic, A. Interfascial Spread of Injectate After Adductor Canal Injection in Fresh Human Cadavers. Anesth. Analg. 2016, 123, 501–503. [Google Scholar] [CrossRef] [PubMed]
- Gautier, P.E.; Hadzic, A.; Lecoq, J.P.; Brichant, J.F.; Kuroda, M.M.; Vandepitte, C. Distribution of Injectate and Sensory-Motor Blockade After Adductor Canal Block. Anesth. Analg. 2016, 122, 279–282. [Google Scholar] [CrossRef]
- Hopkins, P.M. Ultrasound guidance as a gold standard in regional anaesthesia. Br. J. Anaesth. 2007, 98, 299–301. [Google Scholar] [CrossRef] [Green Version]
- Fathil, S.M.; Ghani, M.R.A.; Chen, K.-Y.; Lee, P.; Hou, J.-D.; Lin, J.-A. Physical Ergonomics in Peripheral Nerve Block. Appl. Sci. 2021, 11, 9736. [Google Scholar] [CrossRef]
- Karmakar, M. Atlas of Sonoanatomy for Regional Anesthesia and Pain Medicine; McGraw Hill Professional: New York, NY, USA, 2017. [Google Scholar]
- Kapoor, R.; Adhikary, S.D.; Siefring, C.; McQuillan, P.M. The saphenous nerve and its relationship to the nerve to the vastus medialis in and around the adductor canal: An anatomical study. Acta Anaesthesiol. Scand. 2012, 56, 365–367. [Google Scholar] [CrossRef]
- Karkhur, Y.; Mahajan, R.; Kakralia, A.; Pandey, A.P.; Kapoor, M.C. A comparative analysis of femoral nerve block with adductor canal block following total knee arthroplasty: A systematic literature review. J. Anaesthesiol. Clin. Pharmacol. 2018, 34, 433–438. [Google Scholar] [PubMed]
- Kuang, M.J.; Ma, J.X.; Fu, L.; He, W.W.; Zhao, J.; Ma, X.L. Is Adductor Canal Block Better Than Femoral Nerve Block in Primary Total Knee Arthroplasty? A GRADE Analysis of the Evidence Through a Systematic Review and Meta-Analysis. J. Arthroplast. 2017, 32, 3238–3248.e3. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Ma, J.; Sun, W.; Guo, W.; Li, Z.; Wang, W. Adductor Canal Block Versus Femoral Nerve Block for Analgesia After Total Knee Arthroplasty: A Systematic Review and Meta-analysis. Clin. J. Pain 2017, 33, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Yang, Y.; Li, Q.; Tang, S.L.; Zeng, W.N.; Xu, J.; Xie, T.H.; Pei, F.X.; Yang, L.; Li, L.L.; et al. Adductor canal block versus femoral nerve block for total knee arthroplasty: A meta-analysis of randomized controlled trials. Sci. Rep. 2017, 7, 40721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, C.C.; Dong, S.L.; He, F.C. Comparison of Adductor Canal Block and Femoral Nerve Block for Postoperative Pain in Total Knee Arthroplasty: A Systematic Review and Meta-analysis. Medicine 2016, 95, e2983. [Google Scholar] [CrossRef]
- Li, D.; Ma, G.-G. Analgesic efficacy and quadriceps strength of adductor canal block versus femoral nerve block following total knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2614–2619. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, Y.; Liu, Y. Effectiveness of continuous adductor canal block versus continuous femoral nerve block in patients with total knee arthroplasty: A PRISMA guided systematic review and meta-analysis. Medicine 2019, 98, e18056. [Google Scholar] [CrossRef]
- Zhao, X.Q.; Jiang, N.; Yuan, F.F.; Wang, L.; Yu, B. The comparison of adductor canal block with femoral nerve block following total knee arthroplasty: A systematic review with meta-analysis. J. Anesth. 2016, 30, 745–754. [Google Scholar] [CrossRef]
- Jiang, X.; Wang, Q.Q.; Wu, C.A.; Tian, W. Analgesic Efficacy of Adductor Canal Block in Total Knee Arthroplasty: A Meta-analysis and Systematic Review. Orthop. Surg. 2016, 8, 294–300. [Google Scholar] [CrossRef]
- Schnabel, A.; Reichl, S.U.; Weibel, S.; Zahn, P.K.; Kranke, P.; Pogatzki-Zahn, E.; Meyer-Frießem, C.H. Adductor canal blocks for postoperative pain treatment in adults undergoing knee surgery. Cochrane Database Syst. Rev. 2019, 2019. [Google Scholar] [CrossRef]
- Edwards, M.D.; Bethea, J.P.; Hunnicutt, J.L.; Slone, H.S.; Woolf, S.K. Effect of Adductor Canal Block Versus Femoral Nerve Block on Quadriceps Strength, Function, and Postoperative Pain After Anterior Cruciate Ligament Reconstruction: A Systematic Review of Level 1 Studies. Am. J. Sports Med. 2020, 48, 2305–2313. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.H.; Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Scillia, A.J.; McCarty, E.C. Adductor Canal Versus Femoral Nerve Block after Anterior Cruciate Ligament Reconstruction: A Systematic Review of Level I Randomized Controlled Trials Comparing Early Postoperative Pain, Opioid Requirements, and Quadriceps Strength. Arthroscopy 2020, 36, 1973–1980. [Google Scholar] [CrossRef] [PubMed]
- Memtsoudis, S.G.; Yoo, D.; Stundner, O.; Danninger, T.; Ma, Y.; Poultsides, L.; Kim, D.; Chisholm, M.; Jules-Elysee, K.; Valle, A.G.; et al. Subsartorial adductor canal vs femoral nerve block for analgesia after total knee replacement. Int. Orthop. 2015, 39, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Wiesmann, T.; Piechowiak, K.; Duderstadt, S.; Haupt, D.; Schmitt, J.; Eschbach, D.; Feldmann, C.; Wulf, H.; Zoremba, M.; Steinfeldt, T. Continuous adductor canal block versus continuous femoral nerve block after total knee arthroplasty for mobilisation capability and pain treatment: A randomised and blinded clinical trial. Arch. Orthop. Trauma. Surg. 2016, 136, 397–406. [Google Scholar] [CrossRef]
- Zhao, M.W.; Wang, N.; Zeng, L.; Li, M.; Zhao, Z.K.; Zhang, H.; Tian, H. Comparision for clinical efficiency of continuous adductor canal block and femoral nerve block in total knee arthroplasty. Beijing Da Xue Xue Bao Yi Xue Ban 2017, 49, 142–147. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Jaeger, P.; Baggesgaard, J.; Sørensen, J.K.; Ilfeld, B.M.; Gottschau, B.; Graungaard, B.; Dahl, J.B.; Odgaard, A.; Grevstad, U. Adductor Canal Block With Continuous Infusion Versus Intermittent Boluses and Morphine Consumption: A Randomized, Blinded, Controlled Clinical Trial. Anesth. Analg. 2018, 126, 2069–2077. [Google Scholar] [CrossRef]
- Hanson, N.A.; Derby, R.E.; Auyong, D.B.; Salinas, F.V.; Delucca, C.; Nagy, R.; Yu, Z.; Slee, A.E. Ultrasound-guided adductor canal block for arthroscopic medial meniscectomy: A randomized, double-blind trial. Can. J. Anaesth. 2013, 60, 874–880. [Google Scholar] [CrossRef] [Green Version]
- Hanson, N.A.; Allen, C.J.; Hostetter, L.S.; Nagy, R.; Derby, R.E.; Slee, A.E.; Arslan, A.; Auyong, D.B. Continuous ultrasound-guided adductor canal block for total knee arthroplasty: A randomized, double-blind trial. Anesth. Analg. 2014, 118, 1370–1377. [Google Scholar] [CrossRef]
- Jaeger, P.; Grevstad, U.; Henningsen, M.H.; Gottschau, B.; Mathiesen, O.; Dahl, J.B. Effect of adductor-canal-blockade on established, severe post-operative pain after total knee arthroplasty: A randomised study. Acta Anaesthesiol. Scand. 2012, 56, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Lin, Y.; Goytizolo, E.A.; Kahn, R.L.; Maalouf, D.B.; Manohar, A.; Patt, M.L.; Goon, A.K.; Lee, Y.Y.; Ma, Y.; et al. Adductor canal block versus femoral nerve block for total knee arthroplasty: A prospective, randomized, controlled trial. Anesthesiology 2014, 120, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Mariano, E.R.; Kim, T.E.; Wagner, M.J.; Funck, N.; Harrison, T.K.; Walters, T.; Giori, N.; Woolson, S.; Ganaway, T.; Howard, S.K. A randomized comparison of proximal and distal ultrasound-guided adductor canal catheter insertion sites for knee arthroplasty. J. Ultrasound Med. 2014, 33, 1653–1662. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Hu, Y.; Tao, Y.; Liu, X.; Wang, G. Ultrasound-guided continuous adductor canal block for analgesia after total knee replacement. Chin. Med, J. 2014, 127, 4077–4081. [Google Scholar] [PubMed]
- Ishiguro, S.; Yokochi, A.; Yoshioka, K.; Asano, N.; Deguchi, A.; Iwasaki, Y.; Sudo, A.; Maruyama, K. Technical communication: Anatomy and clinical implications of ultrasound-guided selective femoral nerve block. Anesth. Analg. 2012, 115, 1467–1470. [Google Scholar] [CrossRef] [PubMed]
- Meier, A.W.; Auyong, D.B.; Yuan, S.C.; Lin, S.E.; Flaherty, J.M.; Hanson, N.A. Comparison of Continuous Proximal Versus Distal Adductor Canal Blocks for Total Knee Arthroplasty: A Randomized, Double-Blind, Noninferiority Trial. Reg. Anesth. Pain Med. 2018, 43, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Marian, A.A.; Ranganath, Y.; Bayman, E.O.; Senasu, J.; Brennan, T.J. A Comparison of 2 Ultrasound-Guided Approaches to the Saphenous Nerve Block: Adductor Canal Versus Distal Transsartorial: A Prospective, Randomized, Blinded, Noninferiority Trial. Reg. Anesth. Pain. Med. 2015, 40, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Macrinici, G.I.; Murphy, C.; Christman, L.; Drescher, M.; Hughes, B.; Macrinici, V.; Diab, G. Prospective, Double-Blind, Randomized Study to Evaluate Single-Injection Adductor Canal Nerve Block Versus Femoral Nerve Block: Postoperative Functional Outcomes After Total Knee Arthroplasty. Reg. Anesth. Pain Med. 2017, 42, 10–16. [Google Scholar] [CrossRef]
- Messeha, M.M. Real-time ultrasound-guided comparison of adductor canal block and psoas compartment block combined with sciatic nerve block in laparoscopic knee surgeries. Anesth. Essays Res. 2016, 10, 305–311. [Google Scholar] [CrossRef] [Green Version]
- Thapa, D.; Ahuja, V.; Verma, P.; Gombar, S.; Gupta, R.; Dhiman, D. Post-operative analgesia using intermittent vs. continuous adductor canal block technique: A randomized controlled trial. Acta Anaesthesiol. Scand. 2016, 60, 1379–1385. [Google Scholar] [CrossRef]
- Thapa, D.; Ahuja, V.; Pandey, K.; Gombar, S.; Gupta, R. Evaluation of analgesic efficacy of dexmedetomidine as adjuvant with ropivacaine in ultrasound-guided adductor canal block in patients following anterior cruciate ligament reconstruction surgeries. Br. J. Pain 2019, 13, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.H.; Jaeger, P.; Sonne, T.L.; Dahl, J.B.; Mathiesen, O.; Grevstad, U. Clonidine used as a perineural adjuvant to ropivacaine, does not prolong the duration of sensory block when controlling for systemic effects: A paired, blinded, randomized trial in healthy volunteers. PLoS ONE 2017, 12, e0181351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, J.H.; Grevstad, U.; Siegel, H.; Dahl, J.B.; Mathiesen, O.; Jæger, P. Does Dexmedetomidine Have a Perineural Mechanism of Action When Used as an Adjuvant to Ropivacaine?: A Paired, Blinded, Randomized Trial in Healthy Volunteers. Anesthesiology 2017, 126, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R.; Mittal, G.; Yadav, A.K.; Sethi, R.; Chattopadhyay, A. Adductor canal block for post-operative analgesia after simultaneous bilateral total knee replacement: A randomised controlled trial to study the effect of addition of dexmedetomidine to ropivacaine. Indian J. Anaesth. 2017, 61, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Koh, H.J.; Koh, I.J.; Kim, M.S.; Choi, K.Y.; Jo, H.U.; In, Y. Does Patient Perception Differ Following Adductor Canal Block and Femoral Nerve Block in Total Knee Arthroplasty? A Simultaneous Bilateral Randomized Study. J. Arthroplast. 2017, 32, 1856–1861. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Tan, Z.; Kang, P.; Shen, B.; Pei, F. Effects of multi-site infiltration analgesia on pain management and early rehabilitation compared with femoral nerve or adductor canal block for patients undergoing total knee arthroplasty: A prospective randomized controlled trial. Int. Orthop. 2017, 41, 75–83. [Google Scholar] [CrossRef]
- Li, D.; Alqwbani, M.; Wang, Q.; Liao, R.; Yang, J.; Kang, P. Efficacy of Adductor Canal Block Combined with Additional Analgesic Methods for Postoperative Analgesia in Total Knee Arthroplasty: A Prospective, Double-Blind, Randomized Controlled Study. J. Arthroplast. 2020, 35, 3554–3562. [Google Scholar] [CrossRef]
- Shalu, P.S.; Ghodki, P.S.; Sardesai, S.P. Ultrasound-guided adductor canal block versus femoral nerve block for arthroscopic anterior cruciate ligament repair under general anesthesia. J. Anaesthesiol. Clin. Pharmacol. 2018, 34, 242–246. [Google Scholar] [CrossRef]
- Grosso, M.J.; Murtaugh, T.; Lakra, A.; Brown, A.R.; Maniker, R.B.; Cooper, H.J.; Macaulay, W.; Shah, R.P.; Geller, J.A. Adductor Canal Block Compared with Periarticular Bupivacaine Injection for Total Knee Arthroplasty: A Prospective Randomized Trial. J. Bone. Joint. Surg. Am. 2018, 100, 1141–1146. [Google Scholar] [CrossRef]
- Kampitak, W.; Tanavalee, A.; Ngarmukos, S.; Amarase, C.; Songthamwat, B.; Boonshua, A. Comparison of Adductor Canal Block Versus Local Infiltration Analgesia on Postoperative Pain and Functional Outcome after Total Knee Arthroplasty: A Randomized Controlled Trial. Malays. Orthop. J. 2018, 12, 7–14. [Google Scholar]
- Kampitak, W.; Tanavalee, A.; Ngarmukos, S.; Amarase, C.; Apihansakorn, R.; Vorapalux, P. Does Adductor Canal Block Have a Synergistic Effect with Local Infiltration Analgesia for Enhancing Ambulation and Improving Analgesia after Total Knee Arthroplasty? Knee Surg. Relat. Res. 2018, 30, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousseau-Saine, N.; Williams, S.R.; Girard, F.; Hébert, L.J.; Robin, F.; Duchesne, L.; Lavoie, F.; Ruel, M. The Effect of Adductor Canal Block on Knee Extensor Muscle Strength 6 Weeks After Total Knee Arthroplasty: A Randomized, Controlled Trial. Anesth. Analg. 2018, 126, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Tong, Q.J.; Lim, Y.C.; Tham, H.M. Comparing adductor canal block with local infiltration analgesia in total knee arthroplasty: A prospective, blinded and randomized clinical trial. J. Clin. Anesth. 2018, 46, 39–43. [Google Scholar] [CrossRef]
- Turner, J.D.; Dobson, S.W.; Henshaw, D.S.; Edwards, C.J.; Weller, R.S.; Reynolds, J.W.; Russell, G.B.; Jaffe, J.D. Single-Injection Adductor Canal Block with Multiple Adjuvants Provides Equivalent Analgesia When Compared with Continuous Adductor Canal Blockade for Primary Total Knee Arthroplasty: A Double-Blinded, Randomized, Controlled, Equivalency Trial. J. Arthroplast. 2018, 33, 3160–3166.e1. [Google Scholar] [CrossRef]
- Turner, J.D.; Henshaw, D.S.; Weller, R.S.; Jaffe, J.D.; Edwards, C.J.; Reynolds, J.W.; Russell, G.B.; Dobson, S.W. Perineural dexamethasone successfully prolongs adductor canal block when assessed by objective pinprick sensory testing: A prospective, randomized, dose-dependent, placebo-controlled equivalency trial. J. Clin. Anesth. 2018, 48, 51–57. [Google Scholar] [CrossRef]
- Abdallah, F.W.; Mejia, J.; Prasad, G.A.; Moga, R.; Chahal, J.; Theodoropulos, J.; Dwyer, T.; Brull, R. Opioid- and Motor-sparing with Proximal, Mid-, and Distal Locations for Adductor Canal Block in Anterior Cruciate Ligament Reconstruction: A Randomized Clinical Trial. Anesthesiology 2019, 131, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Canbek, U.; Akgun, U.; Aydogan, N.H.; Kilinc, C.Y.; Uysal, A.I. Continuous adductor canal block following total knee arthroplasty provides a better analgesia compared to single shot: A prospective randomized controlled trial. Acta Orthop. Traumatol. Turc. 2019, 53, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Cicekci, F.; Yildirim, A.; Önal, Ö.; Celik, J.B.; Kara, I. Ultrasound-guided adductor canal block using levobupivacaine versus periarticular levobupivacaine infiltration after totalknee arthroplasty: A randomized clinical trial. Sao Paulo Med. J. 2019, 137, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Elkassabany, N.M.; Cai, L.F.; Badiola, I.; Kase, B.; Liu, J.; Hughes, C.; Israelite, C.L.; Nelson, C.L. A prospective randomized open-label study of single injection versus continuous adductor canal block for postoperative analgesia after total knee arthroplasty. Bone Jt. J. 2019, 101, 340–347. [Google Scholar] [CrossRef]
- Faiaz, A.; Kamath, S. Randomised Controlled Trial between Ultrasound Guided Femoral Nerve Block and Adductor Canal Block for Postoperative Pain and Functional Outcome in Anterior Cruciate Ligament Reconstruction. J. Clin. Diagn. Res. 2019, 13, 11–14. [Google Scholar] [CrossRef]
- Goytizolo, E.A.; Lin, Y.; Kim, D.H.; Ranawat, A.S.; Westrich, G.H.; Mayman, D.J.; Su, E.P.; Padgett, D.E.; Alexiades, M.M.; Soeters, R.; et al. Addition of Adductor Canal Block to Periarticular Injection for Total Knee Replacement: A Randomized Trial. J. Bone. Joint. Surg. Am. 2019, 101, 812–820. [Google Scholar] [CrossRef]
- Ibrahim, A.S.; Aly, M.G.; Farrag, W.S.; Gad El-Rab, N.A.; Said, H.G.; Saad, A.H. Ultrasound-guided adductor canal block after arthroscopic anterior cruciate ligament reconstruction: Effect of adding dexamethasone to bupivacaine, a randomized controlled trial. Eur. J. Pain 2019, 23, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Lyngeraa, T.S.; Jaeger, P.; Gottschau, B.; Graungaard, B.; Rossen-Jørgensen, A.M.; Toftegaard, I.; Grevstad, U. Comparison of the analgesic effect of an adductor canal block using a new suture-method catheter vs. standard perineural catheter vs. single-injection: A randomised, blinded, controlled study. Anaesthesia 2019, 74, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Kastelik, J.; Fuchs, M.; Krämer, M.; Trauzeddel, R.F.; Ertmer, M.; von Roth, P.; Perka, C.; Kirschbaum, S.M.; Tafelski, S.; Treskatsch, S. Local infiltration anaesthesia versus sciatic nerve and adductor canal block for fast-track knee arthroplasty: A randomised controlled clinical trial. Eur. J. Anaesthesiol. 2019, 36, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Kukreja, P.; Bevinetto, C.; Brooks, B.; McKissack, H.; Montgomery, T.P.; Alexander, B.; Shah, A. Comparison of Adductor Canal Block and Femoral Nerve Block for Early Ambulation After Primary Total Knee Arthroplasty: A Randomized Controlled Trial. Cureus 2019, 11, e6331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, M.M.; Dadheech, A.N.; Wakankar, H.M.; Ganjewar, N.V.; Hedgire, S.S.; Pandit, H.G. Randomized Prospective Comparative Study of Adductor Canal Block vs Periarticular Infiltration on Early Functional Outcome After Unilateral Total Knee Arthroplasty. J. Arthroplast. 2019, 34, 2360–2364. [Google Scholar] [CrossRef]
- Lan, F.; Shen, Y.; Ma, Y.; Cao, G.; Philips, N.; Zhang, T.; Wang, T. Continuous Adductor Canal Block used for postoperative pain relief after medial Unicondylar Knee Arthroplasty: A randomized, double-blind, placebo-controlled trial. BMC Anesthesiol. 2019, 19, 114. [Google Scholar] [CrossRef]
- Lynch, J.R.; Okoroha, K.R.; Lizzio, V.; Yu, C.C.; Jildeh, T.R.; Moutzouros, V. Adductor Canal Block Versus Femoral Nerve Block for Pain Control After Anterior Cruciate Ligament Reconstruction: A Prospective Randomized Trial. Am. J. Sports Med. 2019, 47, 355–363. [Google Scholar] [CrossRef]
- Stebler, K.; Martin, R.; Kirkham, K.R.; Lambert, J.; De Sede, A.; Albrecht, E. Adductor canal block versus local infiltration analgesia for postoperative pain after anterior cruciate ligament reconstruction: A single centre randomised controlled triple-blinded trial. Br. J. Anaesth. 2019, 123, e343–e349. [Google Scholar] [CrossRef]
- Wang, Q.; Yue, Y.; Li, D.; Yang, Z.; Yeersheng, R.; Kang, P. Efficacy of Single-Shot Adductor Canal Block Combined with Posterior Capsular Infiltration on Postoperative Pain and Functional Outcome After Total Knee Arthroplasty: A Prospective, Double-Blind, Randomized Controlled Study. J. Arthroplast. 2019, 34, 1650–1655. [Google Scholar] [CrossRef]
- Gadsden, J.C.; Sata, S.; Bullock, W.M.; Kumar, A.H.; Grant, S.A.; Dooley, J.R. The relative analgesic value of a femoral nerve block versus adductor canal block following total knee arthroplasty: A randomized, controlled, double-blinded study. Korean J. Anesthesiol. 2020, 73, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Kavak Akelma, F.; Baran Akkuş, I.; Altinsoy, S.; Özkan, D.; Ergil, J. The effects of pregabalin and adductor canal block on postoperative pain in arthroscopic anterior cruciate ligament reconstruction. Turk. J. Med. Sci. 2020, 50, 195–204. [Google Scholar] [PubMed]
- Kertkiatkachorn, W.; Kampitak, W.; Tanavalee, A.; Ngarmukos, S. Adductor Canal Block Combined with iPACK (Interspace Between the Popliteal Artery and the Capsule of the Posterior Knee) Block vs Periarticular Injection for Analgesia After Total Knee Arthroplasty: A Randomized Noninferiority Trial. J. Arthroplast. 2020, 36, 122–129.e1. [Google Scholar] [CrossRef]
- Song, L.; Li, Y.; Xu, Z.; Geng, Z.Y.; Wang, D.X. Comparison of the ultrasound-guided single-injection femoral triangle block versus adductor canal block for analgesia following total knee arthroplasty: A randomized, double-blind trial. J. Anesth. 2020, 34, 702–711. [Google Scholar] [CrossRef]
- Wang, C.G.; Ding, Y.L.; Wang, Y.Y.; Liu, J.Y.; Zhang, Q. Comparison of Adductor Canal Block and Femoral Triangle Block for Total Knee Arthroplasty. Clin. J. Pain. 2020, 36, 558–561. [Google Scholar] [CrossRef]
- Xin, J.; Zhang, Y.; Li, Q.; Cheng, X.; Lin, Y.; Liu, B.; Zhou, L. Adductor canal block is similar to femoral nerve block for the quality of rehabilitation after arthroscopic partial meniscectomy. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 2334–2342. [Google Scholar] [CrossRef]
- Greenky, M.R.; McGrath, M.E.; Levicoff, E.A.; Good, R.P.; Nguyen, J.; Makhdom, A.M.; Lonner, J.H. Intraoperative Surgeon Administered Adductor Canal Blockade Is Not Inferior to Anesthesiologist Administered Adductor Canal Blockade: A Prospective Randomized Trial. J. Arthroplast. 2020, 35, 1228–1232. [Google Scholar] [CrossRef]
- Kampitak, W.; Tanavalee, A.; Ngarmukos, S.; Tantavisut, S. Motor-sparing effect of iPACK (interspace between the popliteal artery and capsule of the posterior knee) block versus tibial nerve block after total knee arthroplasty: A randomized controlled trial. Reg. Anesth. Pain Med. 2020, 45, 267–276. [Google Scholar] [CrossRef]
- Raddaoui, K.; Radhouani, M.; Bargaoui, A.; Nasri, O.; Zoghlami, K.; Trigui, E.; Kaabachi, O. Adductor canal block: Effect of volume of injectate on sciatic extension. Saudi. J. Anaesth. 2020, 14, 33–37. [Google Scholar]
- Mittal, S.; Mehrotra, S.; Asthana, V.; Agarwal, A. Ultrasound Guided Adductor Canal Block vs Intra Articular Analgesia for Post-operative Pain Relief after Arthroscopic Knee Surgeries: A Comparative Evaluation. Anesth. Essays Res. 2021, 15, 138–142. [Google Scholar] [PubMed]
- Rambhia, M.; Chen, A.; Kumar, A.H.; Bullock, W.M.; Bolognesi, M.; Gadsden, J. Ultrasound-guided genicular nerve blocks following total knee arthroplasty: A randomized, double-blind, placebo-controlled trial. Reg. Anesth. Pain Med. 2021, 46, 862–866. [Google Scholar] [CrossRef]
- Saini, S.; Khattar, N.; Gautam, D.; Agrawal, N.; Gupta, A. Comparison of combined adductor canal block with peri-hamstring infiltration versus adductor canal block for postoperative analgesia in arthroscopic anterior cruciate ligament reconstruction surgery. J. Arthrosc. Jt. Surg. 2021, 8, 282–287. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, Z.; Ma, W.; Liu, R.; Li, Q.; Li, Y. Perineural Dexmedetomidine Reduces the Median Effective Concentration of Ropivacaine for Adductor Canal Block. Med. Sci. Monit. 2021, 27, e929857. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Hu, J.; Zeng, Y.; Li, D.; Yang, J.; Kang, P. Efficacy of Two Unique Combinations of Nerve Blocks on Postoperative Pain and Functional Outcome After Total Knee Arthroplasty: A Prospective, Double-Blind, Randomized Controlled Study. J. Arthroplast. 2021, 36, 3421–3431. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.Y.; Liu, Y.B.; Huang, H.; Xu, S.; Ma, X.J.; Liu, Y.Z.; Chu, H.C. The impact of IPACK combined with adductor canal block under ultrasound guidance on early motor function after total knee arthroplasty. Braz. J. Anesthesiol. 2022, 72, 110–114. [Google Scholar] [CrossRef]
- Borys, M.; Domagała, M.; Wencław, K.; Jarczyńska-Domagała, J.; Czuczwar, M. Continuous femoral nerve block is more effective than continuous adductor canal block for treating pain after total knee arthroplasty: A randomized, double-blind, controlled trial. Medicine 2019, 98, e17358. [Google Scholar] [CrossRef]
- Chuan, A.; Lansdown, A.; Brick, K.L.; Bourgeois, A.J.G.; Pencheva, L.B.; Hue, B.; Goddard, S.; Lennon, M.J.; Walters, A.; Auyong, D. Adductor canal versus femoral triangle anatomical locations for continuous catheter analgesia after total knee arthroplasty: A multicentre randomised controlled study. Br. J. Anaesth. 2019, 123, 360–367. [Google Scholar] [CrossRef]
- Johnston, D.F.; Sondekoppam, R.V.; Giffin, R.; Litchfield, R.; Ganapathy, S. Determination of ED50 and ED95 of 0.5% Ropivacaine in Adductor Canal Block to Produce Quadriceps Weakness: A Dose-Finding Study. Reg. Anesth. Pain Med. 2017, 42, 731–736. [Google Scholar] [CrossRef]
- Zhang, L.-K.; Chen, C.; Du, W.-B.; Zhou, H.-T.; Quan, R.-F.; Liu, J.-S. Is the proximal adductor canal block a better choice than the distal adductor canal block for primary total knee arthroplasty?: A meta-analysis of randomized controlled trials. Medicine 2020, 99, e22667. [Google Scholar] [CrossRef]
- Gautier, P.E.; Lecoq, J.P.; Vandepitte, C.; Harstein, G.; Brichant, J.F. Impairment of sciatic nerve function during adductor canal block. Reg. Anesth. Pain Med. 2015, 40, 85–89. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Arnold, C.; Alvarado, A.C.; Brady, M.F. Saphenous Nerve Block; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2020. [Google Scholar]
- Hamilton, D.L. Increasing patient safety during adductor canal block. Reg. Anesth. Pain Med. 2020, 45, 394. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.-C.; Yoshida, T.; Chuang, T.-Y.; Yang, S.-F.; Chang, C.-C.; Yao, H.-Y.; Tai, Y.-T.; Lin, J.-A.; Chen, K.-Y. Transversus Abdominis Plane Block: An Updated Review of Anatomy and Techniques. BioMed Res. Int. 2017, 2017, 8284363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.-A.; Lu, H.-T. A convenient alternative for monitoring opening pressure during multiple needle redirection. Br. J. Anaesth. 2014, 112, 771–772. [Google Scholar] [CrossRef] [PubMed]
- Veal, C.; Auyong, D.B.; Hanson, N.A.; Allen, C.J.; Strodtbeck, W. Delayed quadriceps weakness after continuous adductor canal block for total knee arthroplasty: A case report. Acta Anaesthesiol. Scand. 2014, 58, 362–364. [Google Scholar] [CrossRef]
- Chen, J.; Lesser, J.B.; Hadzic, A.; Reiss, W.; Resta-Flarer, F. Adductor canal block can result in motor block of the quadriceps muscle. Reg. Anesth. Pain Med. 2014, 39, 170–171. [Google Scholar] [CrossRef]
- Chen, J.; Kim, J.H.; Rosenblatt, M.A.; Lesser, J.B.; Lai, Y.H. Delayed onset of foot drop after the insertion of a mid-thigh adductor canal catheter. J. Clin. Anesth. 2019, 54, 59–60. [Google Scholar] [CrossRef]
- Yee, E.J.; Gapinski, Z.A.; Ziemba-Davis, M.; Nielson, M.; Meneghini, R.M. Quadriceps Weakness After Single-Shot Adductor Canal Block: A Multivariate Analysis of 1,083 Primary Total Knee Arthroplasties. J. Bone. Joint. Surg. Am. 2020, 103, 30–36. [Google Scholar] [CrossRef]
- Joshi, G.; Gandhi, K.; Shah, N.; Gadsden, J.; Corman, S.L. Peripheral nerve blocks in the management of postoperative pain: Challenges and opportunities. J. Clin. Anesth. 2016, 35, 524–529. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Chen, Z.; Ma, X. Continuous adductor canal block is a better choice compared to single shot after primary total knee arthroplasty: A meta-analysis of randomized controlled trials. Int. J. Surg. 2019, 72, 16–24. [Google Scholar] [CrossRef]
- Zhang, L.K.; Zhang, B.Y.; Quan, R.F.; Xu, H.; Sun, Y.J.; Zhou, J.H. Single shot versus continuous technique adductor canal block for analgesia following total knee arthroplasty: A PRISMA-compliant meta-analysis. Medicine 2019, 98, e15539. [Google Scholar] [CrossRef]
- Sun, C.; Zhang, X.; Song, F.; Zhao, Z.; Du, R.; Wu, S.; Ma, Q.; Cai, X. Is continuous catheter adductor canal block better than single-shot canal adductor canal block in primary total knee arthroplasty?: A GRADE analysis of the evidence through a systematic review and meta-analysis. Medicine 2020, 99, e20320. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Wang, H.; Zhuo, Y.; Liu, D.; Wu, C.; Zhang, Y. Continuous adductor canal block provides better performance after total knee arthroplasty compared with the single-shot adductor canal block?: An updated meta-analysis of randomized controlled trials. Medicine 2020, 99, e22762. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Long, F.Y.; Yang, L.Q.; Shen, Y.J.; Guo, F.; Huang, T.F.; Gao, J. Efficacy of perineural dexamethasone with ropivacaine in adductor canal block for post-operative analgesia in patients undergoing total knee arthroplasty: A randomized controlled trial. Exp. Ther. Med. 2017, 14, 3942–3946. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.H.; Gilbert, L.A.; Ghoddoussi, F.; Applefield, D.J.; Kassab, S.S.; Ellis, T.A., 2nd. Addition of buprenorphine to local anesthetic in adductor canal blocks after total knee arthroplasty improves postoperative pain relief: A randomized controlled trial. J. Clin. Anesth. 2016, 33, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Kirksey, M.A.; Haskins, S.C.; Cheng, J.; Liu, S.S. Local Anesthetic Peripheral Nerve Block Adjuvants for Prolongation of Analgesia: A Systematic Qualitative Review. PLoS ONE 2015, 10, e0137312. [Google Scholar] [CrossRef]
- Sehmbi, H.; Brull, R.; Shah, U.J.; El-Boghdadly, K.; Nguyen, D.; Joshi, G.P.; Abdallah, F.W. Evidence Basis for Regional Anesthesia in Ambulatory Arthroscopic Knee Surgery and Anterior Cruciate Ligament Reconstruction: Part II: Adductor Canal Nerve Block-A Systematic Review and Meta-analysis. Anesth. Analg. 2019, 128, 223–238. [Google Scholar] [CrossRef]
- Abdallah, F.W.; Brull, R.; Joshi, G.P. Pain Management for Ambulatory Arthroscopic Anterior Cruciate Ligament Reconstruction: Evidence-Based Recommendations From the Society for Ambulatory Anesthesia. Anesth. Analg. 2019, 128, 631–640. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description Regarding the Needle (Catheter) Tip Position | Corrected Classification | Rationale | Number |
|---|---|---|---|
| Approach by surface landmarks | |||
| Halfway between ASIS and patella | FTB | This position has been proven to be proximal to the adductor canal [36]. | 27 |
| Halfway between greater trochanter to patella | ACB (not sure proximal or distal) | Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter [26]. | 4 |
| Halfway between inguinal ligament and patella | ACB (not sure proximal or distal) | 1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter [26]. 2. The lower border of greater trochanter approximates the level of inguinal crease [56]. | 12 |
| Halfway between inguinal ligament and medial condyle | ACB (not sure proximal or distal) | 1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the inguinal crease. 2. Medial condyles of femur articulate with the tibia and the patella. Medial condyles are distal than the base of the patella. | 2 |
| Approach by ultrasound guidance | |||
| SFA covered by the medial border of sartorius muscles | FTB | Based on the representative image, the medial border of sartorius did not meet the medial border of adductor longus yet. | 5 |
| FA covered by the midpoint of sartorius muscles | FTB or proximal ACB | Whether the medial borders of sartorius and adductor longus meet could not be identified in the representative image. | 4 |
| FA underneath the sartorius muscles | FTB or ACB (not sure proximal or distal) | Depends on whether the medial borders of sartorius and adductor longus meet in the representative image. | 10 |
| Cavity surrounded by medial femoris, ALM, and sartorius muscles | FTB or proximal ACB | 1. Depends on whether the medial borders of sartorius and adductor longus meet in the representative image. 2. Mid-adductor canal can be defined as ”distal to the proximal adductor canal, where the ALM is replaced by AMM posteromedially”. | 5 |
| 2–3 cm proximal to femoral artery diving deep | Distal ACB | Using corrected classification system. | 5 |
| Numbers of inconsistent approaches of ACB related studies | 66 * | ||
| Study | Original Grouping in the Study | Description Regarding the Needle (Catheter) Tip Position /Further Evidence in the Study | Corrected Classification /Rationale |
|---|---|---|---|
| Jæger 2013, 2014, 2018 [15,32,83] | ACB | Halfway between the ASIS and the patella; the catheter was advanced 1–2 cm beyond the tip of the needle. | FTB /This position has been proven to proximal to the adductor canal [36]. |
| Kwofie 2013 [5] | ACB | The midpoint between the inguinal crease and the medial condyle. /Under ultrasound guidance, the femoral artery in short axis deep to the sartorius muscle can be visualized. | FTB or proximal ACB /The medial border of sartorius muscle didn’t meet the medial border of ALM in the representative image. |
| Hanson 2013, 2014 [84,85] | ACB | Mid-thigh, half the distance between the inguinal crease and the patella. | Proximal ACB /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter [26]. 2. The lower border of greater trochanter approximates the level of inguinal crease. 3. FA is not diving in the representative image [56]. |
| Grevstad 2014, 2015 [6,30] | ACB | Mid-thigh level, as described by Jæger 2012 [86] (with the FA, femoral vein, and the saphenous nerve deep to the sartorius muscle between the vastus medialis muscle and the ALM). | FTB or proximal ACB /No ultrasound image can be referred to. Whether the medial borders of sartorius and adductor longus meet could not be identified |
| Kim 2014 [87] | ACB | Mid-thigh level, as described by Manickam 2009 [13]. /By techniques of Manickam 2009, the injection site is 2–3 cm proximal to where the femoral artery diving deep. | Distal ACB /No ultrasound image can be referred to. |
| Mariano 2014 [88] | Proximal ACB | Where the medial border of sartorius first covers the superficial femoral artery; the catheter was advanced 1 to 3 cm beyond the needle tip posterior to the nerve. | FTB /1. Obviously, the medial border of sartorius did not meet the medial border of adductor longus yet. 2. The so-called distal ACB in the study should also be anatomically classified as FTB, not to mention the proximal one |
| Distal ACB | Approximately halfway between the anterior superior iliac spine and the patella; the catheter was advanced 1 to 3 cm beyond the needle tip posterior to the nerve. | FTB /This position has been proven to be proximal to the adductor canal [36]. | |
| Shah 2014 [34] | ACB | Halfway between ASIS and the patella; a catheter was inserted 5–8 cm through the cannula. | FTB /This position has been proven to proximal to the adductor canal. |
| Zhang 2014 [89] | ACB | Approximately 8–12 cm below the inguinal crease; a catheter was placed 5 cm beyond the tip of the needle. /The authors used the definition by Ishiguro 2012, in the discussion section [90]. The site is where SFA passes beneath the medial border of the sartorius muscle. | FTB /Whether the medial borders of sartorius and adductor longus meet could not be identified in the representative image. By the Mariano 2014 [88] and Meier 2018 [91], the medial border of sartorius did not meet the medial border of adductor longus yet in this level. |
| Marian 2015 [92] | ACB | Mid-thigh level, the femoral artery was visualized in the short axis below the sartorius muscle. | FTB or proximal ACB /Whether the medial borders of sartorius and adductor longus meet could not be identified in the representative image. |
| Shah 2015 [35] | ACB | Halfway between the ASIS and the patella; a catheter was inserted 5–8 cm through the cannula. | FTB /This position has been proven to proximal to the adductor canal. |
| Abdallah 2016 [14] | ACB | Mid-thigh level. /The authors used the definitions by Manickam 2009 [13] in the method section. By techniques of Manickam 2009, the injection site is 2–3 cm proximal to where the femoral artery diving deep. | Distal ACB /No ultrasound image can be referred to. |
| Elkassabany 2016 [17] | ACB | Where the femoral artery was underneath the midpoint of the sartorius muscle with the vein just inferior to the artery; the catheter was advanced 2–3 cm beyond the tip of the needle. /The authors used the definitions by Ishiguro 2012 [90] and Mariano 2014 [88], but the injection site was more distal. | FTB or proximal ACB /There is no ultrasound image for reference. |
| Macrinici 2016 [93] | ACB | Where the femoral artery in short axis deep to the sartorius muscle. /The authors used the definitions by Manickam 2009 in the method section. | Distal ACB /There is no ultrasound image for reference. By techniques of Manickam 2009, the injection site is 2–3 cm proximal to where the femoral artery diving deep [13]. |
| Messeha 2016 [94] | ACB | Mid-point between the inguinal crease and medial condyle. | ACB (not sure proximal or distal) /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the inguinal crease. 2. Medial condyles of femur articulate with the tibia and the patella. Medial condyles are distal than the base of the patella. |
| Thapa 2016 [95,96] | ACB | Halfway between ASIS and the patella. | FTB /This position has been proven to be proximal to the adductor canal. |
| Wiesmann 2016 [79] | ACB | Where the femoral artery posterior to the sartorius muscle; the insertion point was 20 cm proximal to the cranial margin of the patella as measured by a ruler. A catheter wad inserted 3–5 cm over the needle. | FTB or proximal ACB /1. There is no ultrasound image or cited articles for reference. 2. Based on Wong 2016 [36], 20 cm proximal to the patella may be located in the femoral triangle. |
| Andersen 2017 [97,98] | ACB | Mid-thigh level, the femoral artery was visualized in the short axis below the sartorius muscle. | FTB or proximal ACB /There is no ultrasound image for reference. |
| Goyal 2017 [99] | ACB | Mid-thigh level. Use ultrasound proof to visualize sartorius muscle and femoral vessels. Target anterolateral to the femoral artery and below the sartorius. | FTB /From the ultrasound image, the medial border of sartorius muscle didn’t meet the medial border of ALM yet. |
| Koh 2017 [100] | ACB | Where the femoral artery was underneath the sartorius muscle; the needle was placed to the space bordered by vastus medialis, sartorius muscle, and femoral artery. | FTB or ACB (not sure proximal or distal) /No ultrasound image can be referred to. Whether the medial borders of sartorius and adductor longus meet could not be identified by the description. |
| Li 2017, 2020 [101,102] | ACB | Find a cavity surrounded by the sartorius muscle, medial femoral muscle, and the adductor muscles. | FTB or ACB (not sure proximal or distal) /There is no ultrasound image for reference. Whether the medial borders of sartorius and adductor longus meet could not be identified by the description. |
| Ghodki 2018 [103] | ACB | Halfway between ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Grosso 2018 [104] | ACB | Halfway between ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Kampitak 2018 [105] | ACB | Halfway between the inguinal crease and the patella. | ACB (not sure proximal or distal) /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the inguinal crease. 2. Medial condyles of femur articulate with the tibia and the patella. Medial condyles are distal than the base of the patella. |
| Kampitak 2018 [106] | ACB | Mid-thigh level. /Based on the reference of Jaeger 2012 [86], Jenstrup 2012 [9], and Lund 2011 [8] from the introduction section, these articles defined mid-thigh level as halfway between ASIS and patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Meier 2018 [91] | Proximal ACB | Where SFA existed underneath the medial third of sartorius (ultrasound image); a catheter was advanced 1 to 2 cm into the adductor canal. /The authors used the definitions by Mariano 2014 in the introduction section. | FTB /Obviously, the medial border of sartorius did not meet the medial border of adductor longus yet. |
| Distal ACB | Where SFA was underneath the midpoint of the sartorius muscle. | FTB or proximal ACB /Whether the medial borders of sartorius and adductor longus meet could not be identified in the representative image. | |
| Romano 2018 [24] | Proximal ACB | Where SFA passed beneath the medial border of sartorius. /The authors agreed with the definitions by Mariano 2014 and Meier 2018 when comparing the results of proximal and distal ACB in the discussion section. | FTB /The medial border of sartorius did not meet the medial border of adductor longus yet |
| Distal ACB | Half of the distance between the inguinal crease and top of patella. | ACB (but not sure of proximal or distal) /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter [26]. 2. The lower border of greater trochanter approximates the level of inguinal crease [56]. | |
| Rousseau-Saine 2018 [107] | ACB | Halfway between the ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Runner 2018 [20] | ACB | The adductor canal was located by visualizing the FA on the short axis bordered by the sartorius muscle, the vastus medialis muscle, and the ALM. | FTB or proximal ACB /No ultrasound image can be referred to. Whether the medial borders of sartorius and adductor longus meet could not be identified. |
| Sztain 2018 [23] | Proximal ACB | Halfway between the ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Distal ACB | 2–3 cm proximal to the adductor hiatus. | Distal ACB | |
| Tong 2018 [108] | ACB | Mid-thigh approach based on Jæger 2013 [32], halfway between the ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Turner 2018 [109] | ACB | Midpoint between the patella and inguinal crease. | ACB (but not sure of proximal or distal) /As explained above, adductor canal is located at the middle one-third of the distance from the patella and inguinal crease. |
| Turner 2018 [110] | ACB | Halfway between the ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Abdallah 2019 [111] | Proximal ACB | Femoral artery medial to sartorius. | FTB /The medial border of sartorius did not reach the medial border of adductor longus in the representative image. |
| Mid-ACB | Femoral artery inferior to sartorius. | FTB or proximal ACB /Whether the medial borders of sartorius and adductor longus meet could not be identified in the representative image. | |
| Distal ACB | Femoral artery lateral to sartorius. | Distal ACB /Femoral artery is diving in the representative image. | |
| Canbek 2019 [112] | ACB | Mid-thigh level (halfway between the anterior superior iliac spine and the patella). | FTB /This position has been proven to proximal to the adductor canal. |
| Cicekci 2019 [113] | ACB | Midway between the inguinal ligament and the medial condyle. /An ultrasonographic image of the saphenous nerve was captured in the adductor canal, laterally to the femoral artery under the sartorius muscle. | ACB (not sure proximal or distal) /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the inguinal crease. 2. Medial condyles of femur articulate with the tibia and the patella. Medial condyles are distal than the base of the patella. |
| Elkassabany 2019 [114] | ACB | Halfway between the ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Faiaz 2019 [115] | ACB | Mid-thigh level. /Based on the citation of Jæger 2013 [4], mid-thigh level is at halfway between ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Goytizolo 2019 [116] | ACB | Mid-thigh level. /The femoral artery was visualized under the sartorius muscle. | FTB or ACB (not sure proximal or distal) /No ultrasound image can be referred to. Whether the medial borders of sartorius and adductor longus meet could not be identified. |
| Ibrahim 2019 [117] | ACB | Midway between the ASIS and patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Lim 2019 [21] | ACB | Mid-thigh, midway between the ASIS and patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Lyngeraa 2019 [118] | ACB | Mid-thigh, midway between the ASIS and patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Kastelik 2019 [119] | ACB | Identify the SFA below the sartorius muscle. | FTB or ACB (not sure proximal or distal) /No ultrasound image can be referred to. Whether the medial borders of sartorius and adductor longus meet could not be identified. |
| Kukreja 2019 [120] | ACB | Mid-thigh level. /Based on the citation of Jæger 2013 [32], mid-thigh level is at halfway between ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Kulkarni 2019 [121] | ACB | Mid-thigh, halfway between the inguinal crease and patella. | ACB /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. 2. The lower border of greater trochanter approximates the level of inguinal crease. |
| Lan 2019 [122] | ACB | Mid-thigh level. /Based on the citation of Lund 2011 [8], mid-thigh level at halfway between ASIS and the patella. | FTB /This position has been proven to proximal to the adductor canal. |
| Lynch 2019 [123] | ACB | Target the saphenous nerve at the adductor hiatus. | Distal ACB |
| Stebler 2019 [124] | ACB | Mid-thigh site; target the triangular hyperechoic region lateral to the artery, bounded by the sartorius muscle superiorly, and the vastus medialis laterally. | FTB or ACB (not sure proximal or distal) /There is no ultrasound image for reference. Whether the medial borders of sartorius and adductor longus meet could not be identified from the paragraph. |
| Wang 2019 [125] | ACB | Half the distance between the inguinal crease and the patella. | ACB (but not sure of proximal or distal) /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. 2. The lower border of greater trochanter approximates the level of inguinal crease. |
| Gadsden 2020 [126] | ACB | The midpoint between the inguinal crease and the proximal aspect of patella. | ACB (but not sure of proximal or distal) /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. 2. The lower border of greater trochanter approximates the level of inguinal crease. |
| KAVAK AKELMA 2020 [127] | ACB | Halfway between the ASIS and the patella; visualize femoral artery under the sartorius muscle. | FTB /This position has been proven to proximal to the adductor canal. |
| Kertkiatkachorn 2020 [128] | ACB | Identify the sartorius muscle, ALM, vastus medialis muscles, and the femoral artery. Position the needle tip between the superficial femoral artery and the posterior region of the sartorius muscle. | FTB or proximal ACB /1. No sonographic image can be referred to. Whether the medial borders of sartorius and adductor longus meet cannot be identified. 2. Mid-adductor canal can be defined as “distal to the proximal adductor canal, where the ALM is replaced by AMM posteromedially”. |
| Song 2020 [129] | FTB | 5 cm proximal to the apex of femoral triangle, identified as the intersection of the medial borders of the sartorius and adductor longus muscles. | FTB |
| ACB | 5 cm distal to the apex of femoral triangle. | Almost mid-adductor ACB /1. The femoral artery was underneath the sartorius muscle, not diving deep in the representative image. 2. Mid-adductor canal can be defined as ”distal to the proximal adductor canal, where the ALM is replaced by AMM posteromedially”. The ALM was almost replaced by AMM from the representative image. | |
| Wang 2020 [130] | FTB | Halfway between the ASIS and the base of the patella; a catheter was inserted 3 cm past the needle tip. | FTB |
| ACB | The midpoint between the greater trochanter of the femur and the base of the patella. | Proximal ACB /1. Adductor canal surrounded by the sartorius muscle, the vastus medialis muscle, and the adductor longus muscle was identified clearly from the representative image. 2. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter [26]. | |
| Xin 2020 [131] | ACB | The probe was placed on the middle of the thigh. A catheter was inserted 3 cm past the needle tip. /The authors use the techniques described by Manickam 2009. | Distal ACB /There is no ultrasound image for reference. By techniques of Manickam 2009, the injection site is 2–3 cm proximal to where the femoral artery diving deep [13]. |
| Greenky 2020 [132] | ACB | The probe was placed anteromedially on the middle and distal third of the thigh. /The femoral artery and sartorius muscle formed the roof of the adductor canal. | FTB or proximal ACB /Whether the medial borders of sartorius and adductor longus meet cannot be identified from the sonographic image. |
| Kampitak 2020 [133] | ACB | Halfway between the ASIS and the base of the patella. | FTB |
| Raddaoui 2020 [134] | ACB | The probe was positioned transversely midway from the patella and the inguinal ligament. | ACB /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. 2. The lower border of greater trochanter approximates the level of inguinal crease. |
| Mittal 2021 [135] | ACB | Halfway between the ASIS and the base of the patella. | FTB |
| Rambhia 2021 [136] | ACB | The adductor canal catheter was placed as per our standard technique, at the mid-point between the inguinal crease and the superior pole of the patella. | ACB /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. 2. The lower border of greater trochanter approximates the level of inguinal crease. |
| Saini 2021 [137] | ACB | Probe was placed transversely on medial aspect of mid-thigh; midway between ASIS and base of patella. | FTB |
| Wang 2021 [138] | ACB | Probe was placed on the anteromedial part of the thigh at the level of the midpoint, between the greater trochanter of the femur and the proximal edge of patella. | ACB /Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. |
| Wang 2021 [139] | ACB | Probe was used to scan the middle of the thigh (half the distance between the inguinal crease and the patella) | ACB /1. Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. 2. The lower border of greater trochanter approximates the level of inguinal crease. |
| Zheng 2022 [140] | ACB | Probe was placed at the midpoint of the connecting line between the greater trochanter of the femur and the upper edge of the patella. | ACB /Adductor canal is located at the middle one-third of the distance from the base of the patella to the lower border of the greater trochanter. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan Chiang, Y.-H.; Wang, M.-T.; Chan, S.-M.; Chen, S.-Y.; Wang, M.-L.; Hou, J.-D.; Tsai, H.-C.; Lin, J.-A. Motor-Sparing Effect of Adductor Canal Block for Knee Analgesia: An Updated Review and a Subgroup Analysis of Randomized Controlled Trials Based on a Corrected Classification System. Healthcare 2023, 11, 210. https://doi.org/10.3390/healthcare11020210
Fan Chiang Y-H, Wang M-T, Chan S-M, Chen S-Y, Wang M-L, Hou J-D, Tsai H-C, Lin J-A. Motor-Sparing Effect of Adductor Canal Block for Knee Analgesia: An Updated Review and a Subgroup Analysis of Randomized Controlled Trials Based on a Corrected Classification System. Healthcare. 2023; 11(2):210. https://doi.org/10.3390/healthcare11020210
Chicago/Turabian StyleFan Chiang, Yu-Hsuan, Ming-Tse Wang, Shun-Ming Chan, Se-Yi Chen, Man-Ling Wang, Jin-De Hou, Hsiao-Chien Tsai, and Jui-An Lin. 2023. "Motor-Sparing Effect of Adductor Canal Block for Knee Analgesia: An Updated Review and a Subgroup Analysis of Randomized Controlled Trials Based on a Corrected Classification System" Healthcare 11, no. 2: 210. https://doi.org/10.3390/healthcare11020210