
The Educational Needs of Adolescent and Young Adult Renal Transplant Recipients—A Scoping Review



{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy
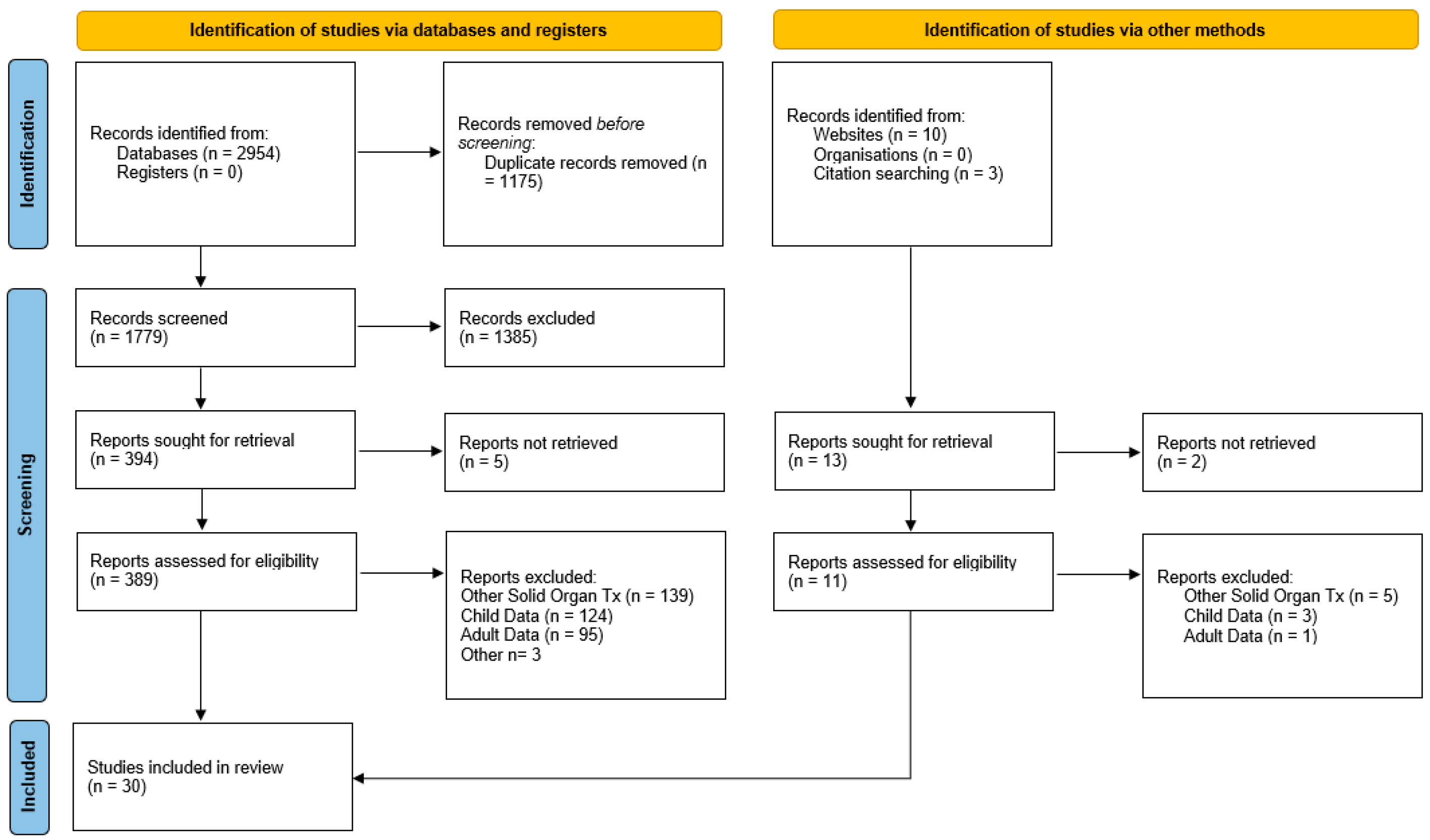
2.3. Study Selection and Data Extraction
- Study characteristics: author, year of publication, country, design, sample size, clinical setting, number studied
- Population characteristics: adolescent vs. young adult, transplant function
- Study design: methods used to investigate educational needs
- Key findings
2.4. Data Analysis
3. Results
3.1. Qualitative Analysis of Selected Studies
- The needs of the disrupted youth
- The needs of the disorganized youth
- The needs of the distressed youth
3.2. The Needs of the Disrupted Youth
3.3. The Needs of the Disorganised Youth
3.4. The Needs of the Distressed Youth
4. Discussion
- (1)
- There is a paucity of research on how certain young people are successful and cope/adapt following transplantation which may help in developing tools to help other patients.
- (2)
- Educational needs of racial, ethnic, and religious minority groups and those from immigrant or socially deprived backgrounds need further exploration as these may be different from the general population.
- (3)
- An in-depth qualitative analysis of young transplant recipients, which fully explores the contextual factors such as healthcare setting, background, and resources, may help further our understanding of their experiences and requirements.
- (4)
- Future studies that are designed and carried out with adolescent or young adult transplant recipients as equal partners may improve the quality and validity of the results.
4.1. Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Authors (Reference), Country | Aim of Study | Number of Participants | Adolescents or Young Adults | Study Design | Length of Study | Methodology of Assessment | Key Findings | Limitations |
| Aasebø [30] Norway | Describe the life situation, lifestyle, and common activities of daily life in young adult kidney transplant recipients aged 18–35 years. In addition, compared their HRQoL with a general population sample, adjusting for age, sex, and education. | 131 | Both | Cross sectional study. Questionnaire. Short Form 36 (SF-36). Comparison made with matched general population. | Retrospective-snapshot | Short Form 36 (SF-36) questionnaire. compared groups using a two-sample t-test or Fisher’s exact test, or the Mann–Whitney U-test. | Recipients reported high participation rates in cultural and sports activities. Majority were working and satisfied. 25% of the total group were not integrated in professional life. The transplant recipients scored lower than the general population on seven of the eight SF-36 scales and the two summary scales after adjusting for age, sex and education. 70% stated had delayed education. 6% were happy with physical appearance-77% reported-ve change since transplant. Higher pain scores than general population. | Self-reported Questionnaire. 47% return rate. Predominance for females to return. Data of clinical status and transplant function not collected. |
| Akchurin [48] USA | Was there a difference in immunosuppression adherence in groups transitioning to adult services? | 27 | Adolescents | Retrospective Case control study | 2 years | Measured tacrolimus levels. Statistical analyses including t-Test and multivariate analyses. | Transition not associated with changes in medication adherence. | Tacrolimus levels less than ideal to measure adherence. single centre didn’t cover those lost to follow-up |
| Anthony [11] Canada | To measure quality of life in adolescent transplant recipients and impact on their families. | 12 | Adolescents | Retrospective pilot study. Case control. Questionnaire. | 3 years post transplant. Single study, | VAQOL and General Health, the PedsQL 4.0, PedsQL End Stage Renal Disease Module, and Impact on Family Module | High level of fatigue. Concerns about physical appearance. Reported difficulties in interactions with peer and family. Despite good outcomes family reported negative emotional outcomes, stress and worry. Education delay. Turbulent relationships both peer and family. | Small study. Self reported. |
| Ashoor [49] USA | To assess the prevalence and types of sexually transmitted infections in paediatric renal transplant patients | 49 | Adolescents and young adults. | Retrospective cohort observational study. | 4 years | Observation | 15% of men sexually active. 45% of women. 75% off sexually active women on contraception. 36% sexually active had at least one STI. Most patients rely on nephrologist for preventive care -important to raise awareness of this issue in the transplant community | Small study. Self reporting by patients, |
| Boucquemont [37] Canada/USA | If day of the week affected teen or young adult adherence to medications | 138 | Both | Post-hoc analysis of a prospective randomised control trial | 15 months | Logistic regression with generalized estimating equations to estimate the association between week- ends/weekdays and each of perfect taking. | Weekends are disruptive to normal routine and patients have reduced adherence to medication at the weekends. | Post-hoc analysis. Small sample. |
| Bullington [50] USA | Understand opinions of adolescent transplant patients on why not taking medications | 12 | A | Qualitative | One interview and follow-up | Q-methodology | Three themes- medication issues. Deliberate non-adherence and “troubled adherence”. | Self-reported. Small sample. |
| Chaturvedi [51] Australia | Assess graft stability and patient satisfaction after transition from children to adult services. | 11 | Both | Cohort observational. Retrospective review of clinical notes | Over course of two year | Patient evaluations. | 1 acute episode of antibody mediated rejection. Inadequate involvement of young people in transition planning. Lack of preparation for transition to adult services. | Small numbers, self reported. |
| Dobbels [10] Netherlands | assess HRQOL, depressive symptoms, side effect experience and treatment adherence in a sample of adolescent kidney transplant patients, using self-report and parent-report. | 26 | A | Cross-sectional study | Single episode | Self-reported questionnaires. KIDSCREEN-27 (QOL), a treatment adherence interview, the MTSOSD-59R (side effects) and the Beck Depression Inventory (depression) | Patients reported good QOL. Depressive symptoms occurred in 17.4%, and 75% were non-adherent with their medications. Many show problematic health behaviours. Side effects were increased appetite, fatigue and headache; the most distressing ones were hair loss or thinning of hair, warts on hands or feet, and sores in the mouth or on the lips. | Small. Cross-sectional design. |
| Hamilton [32] UK | wellbeing and medication adherence are associated with psychosocial factors using data from the Surveying Patients Experiencing Young Adult Kidney Failure (SPEAK) study | 417 | Both | Survey | Once off survey | multivariable linear regression to examine psychosocial associations with scores on the Warwick–Edinburgh Mental Wellbeing Scale and the eight-item Morisky Medication Adherence Scale. | Wellbeing was positively associated with extraversion, openness, independence, and social support, and negatively associated with neuroticism, negative body image, stigma, psychologic morbidity, and dialysis. Higher medication adherence was associated with living with parents, conscientiousness, physician access satisfaction, patient activation, age, and male sex, and lower adherence was associated with comorbidity, dialysis, education, ethnicity, and psychologic morbidity. | Cross-sectional design limits changes on outcome can not be tracked, directionability between variables could not be assessed. |
| Jakubowska-Winecka [38] Poland | To determine parental attitudes affect on adolescent medication adherence | 197 | A | Survey | Once off | M. Plopa’s Parental Attitudes Scale, which distinguishes 5 types of attitudes. Medication adherence was evaluated on the basis of the Morisky Medication Adherence Scale (MMAS-8) | Accepting attitude and overly protective attitude corresponded with increased adherence. | Other factors not controlled in study. |
| Kärrfelt [43] Sweden | To understand the emotional and psychological adaption of patients after undergoing transplant | 20 | A | Mixed methods interviews. Quantitative and qualitative interviews. | Once | Thematic analysis | Mostly felt unaffected. Improved relationship with donor. One deceased donor recipient had nightmares about alien kidney. Psychological adaption seemed to rely of denial & avoidance. | High drop out rate. Voluntary recruitment may have led to a selection bias. |
| Kim [52] South Korea | To understand the experiences of adolescents undergoing renal transplant | 9 | A | Qualitative descriptive study. | Once | Content analysis | “being different from others,” “not being invited as a decision maker,” “becoming one of them,” “still being different from others,” “having mixed feeling toward mothers,” and “coping with new circumstances.” | Small-specific population |
| Korus [40] Canada | Understanding the information needs of adolescent transplant recipients. | 8 | A | Qualitative descriptive study | Once | Content analysis | Transplant a stressful situation. 4 main stressors: changes in body image, wanting to be normal, pain, and breakdown in communication processes. Two coping strategies were gaining more information and seeking social support. | Small study |
| Kullgren [53] USA | Validate measurement tool “transplant responsibility questionnaire.” And determine between TRQ and adherence | 59 | A | Survey-TRQ scores vs TAC levels | Once | Bivariate correlations were calculated between TRQ average scores, caregiver–child TRQ discrepancy scores, and adherence. Oneway ANOVAs were used to assess differences between adherent and non-adherent groups on the TRQ | Adherence unrelated to TRQ score. Disparity between parent and recipient perception of self-management. Older more self reliant than younger | Self reported |
| Lugasi [33] Canada | To assess the identity formation of renal transplant patients and type 1 diabetic patients | 85 | A | Qualitative | Once | Demographic questionnaire. Quality of Life Profile Adolescent Version (QOLPAV) | Differences in ideological identity, with tx recipeints showing higher levels of diffusion and controls showing higher levels of foreclosure. No differences with respect to interpersonal identity, QOL, perceived control over the QOL domains, and perceived opportunities for growth and development were found | Convenience sampling. Questionnaire based data collection. |
| Malekahmadi [42] Iran | To evaluate the extent to which socioeconomic, clinical, and psychological characteristics explain the variance in the health-related quality of life of adolescent Iranian kidney transplant recipients. | 55 | A | Cross-sectional study | Once | Hierarchal regression analysis, the cross-sectional socioeconomic, clinical and psychological variables associated with health outcomes. | The relative predictive power of socioeconomic, clinical, and psychological variables with respect to health-related quality of life was 21.8% (p = 0.088), 21.2% (p = 0.014), and 27.6% (p = 0.001). Psychological factors had a greater relative predictive power in postrenal transplant health-related quality of life of adolescents than did the socioeconomic and clinical characteristics. | Small sample size. Cross-sectional rather than longitudinal analysis. |
| Massey [31] Netherlands | The aim of this study was to investigate (a) the extent to which age at first renal replacement therapy, achievement of developmental milestones, satisfaction of psychological needs, and coping were related to subjective well-being and medication adherence | 62 | YA | Cross-sectional interview study | Once | subjective well-being (Positive And Negative Affect Schedule; Satisfaction With Life Scale), medication adherence (Basel Assessment of Adherence to Immunosuppressive Medication Scale), dispositional coping (Brief COPE), achievement of developmental milestones (Course of Life Questionnaire), and satisfaction of psychological needs (Basic Psychological Needs Scale) | Sixty-five percent were classified as nonadherent in the past month. In contrast, subjective self-rated overall adherence was high. None of the variables measured were related to nonadherence. Higher feelings of competence and autonomy, and timely achievement of social and psychosexual developmental milestones were related to higher subjective well-being. Well-being and adherence did not differ according to age at diagnosis or first renal replacement therapy | Limited by cross-sectional and retrospective analysis. Self-selected participants so selection bias may be present. Small sample analysis. |
| Mellerio, [8] France | To document the semiprofessional outcomes of adults who underwent kidney transplantation before age 16 years between 1985 and 2002 | 374 | A | Retrospective cohort study. | Once | Questionnaire which was then compared to data from the general French population. | The median ages were 27.1 years at survey time and 12.3 years at first transplantation. Of the participants, 31.1% lived with a partner (vs. 52.2%; PG0.01) and 35.7% lived with their parents. | Self-reporting-more frequently women and those with better graft function. |
| Mintzer [44] USA | To assess prevalence and correlates of self-reported symptoms of posttraumatic stress in a nonreferred sample of adolescent liver, heart, and kidney transplant recipients. | 104 | Both | Cross-sectional analysis | once | PTSD Index for the Diagnostic and Statistical Manual of Mental Disorders | 16% of the adolescents met all symptom criteria for PTSD, and an additional 14.4% met 2 of 3 symptom-cluster criteria. Regression analysis indicated no effect of gender, ethnicity, age at interview, organ type, time since transplant, or age at transplant | Retrospective analysis. Patients transplanted over a large time span 80s to 90s. |
| Nguyen [55] Canada & USA | To gather the perspectives of recipients, parents, and health professionals concerning their needs, challenges, and potential intervention strategies to design an optimal, multi-component medication adherence intervention | 32 | Both | Qualitative study design- focus groups | Once | Content analysis-leading to themes | Multi-component behavioural intervention, including an expanded electronic pillbox and companion website, education materials, and customized digitized features to support shared responsibility and communication among recipients, parents, and health professionals were all suggested by participants. | Self-selecting so potential selection bias. Predominantly white population. |
| Penkower [39] USA | (a) describes the prevalence of psychological distress, (b) describes the prevalence of nonadherence, and (c) explores the association between the recipient’s psychological distress and his/her subsequent medical adherence | 22 | A | Qualitative design- interviews. | Twice | Beck Depression Inventory II (BDI). State Anxiety subscale of the Spielberger State-Trait Anxiety Scale. State Anger subscale of the Spielberger State-Trait Anger Scale. | At the initial interview, 36.4% had symptoms of depression, 36.4% endorsed anxiety, and 18.2% endorsed excessive state anger. Non-adherence rates were 13.6% for medication, 22.7% for blood work, and 50% for missed clinic. | Small study-pilot. Self-reporting adherence. |
| Quast [56] USA | The current study examines associations between personality (i.e., agreeableness, conscientiousness, neuroticism) and adherence barriers in a group of adolescent and young adult (AYA) solid organ transplant recipients | 90 | Both | Cross-sectional study | Once | Agreeableness, Conscientiousness, and Neuroticism scales from the NEO Five-Factor Inventory and the Adolescent Medication Barriers Scale (AMBS) | Lower levels of agreeableness and conscientiousness and higher levels of neuroticism were related to higher self-reported barrier scores (AMBS; r’s ¼ 0.31–0.53, p’s < 0.001). The relations differed by personality factor and barrier type. | Small study, self reporting-limited by cross sectional and retrospective nature of study design. |
| Quinn [36] USA | Explored the novel role of resilience constructs as protective factors in securing stable HCT among AYA with KT | 32 (17 stable, 15 unstable). | Both | Qualitative study | Once | Semi-structured interviews. Content analysis. | Confidence in and connection to one’s healthcare team appear to be linked with a stable HCT among AYA with KT. This suggests that interdependence, the ability to foster connections with and elicit support from healthcare providers, as opposed to complete independence or autonomy, which is often advised in the HCT process, is a critical component of resilience linked to stable HCT. | Small study. Retrospective and clinical factor determining stable vs unstable less clear. |
| Simons [34] USA | To evaluate whether different factors would be associated with lower mental health scores on the CHQ | 39 | Adolescents | Comparative study | Once | Semi-structured interviews. Multiple validated questionnaires around medication, knowledge, mental health. Hierarchal regression analyses to determine strength of association. | Perceived frequency of medication side-effects and family conflict significantly contributed to adolescent physical functioning and mental health outcomes. Taken together, transplant consequences and family environment significantly impact physical and mental health outcomes in adolescent transplant recipients | Risk of type 1 error as multiple variables investigated. |
| Silva [54] Brazil | To assess the prevalence and correlates of nonadherence to immunosuppressive medications in a pediatric kidney transplant population who received free access to immunosuppressive medications within the health care system | 156 | Adolescents | Single centre cross sectional analysis | Once | Implementation nonadherence to immunosuppressive medications was measured by the 4 questions of the Basel Assessment of Adherence to Immunosuppressive Medications Scale. Multilevel correlates to non—adherence (patient, micro, and macro levels) were assessed | 33% were nonadherent to immuno—suppressive medications, mainly in timing (25%) and taking (10.9%) dimensions. Being an adolescent (odds ratio: 2.66; CI, 1.02–6.96), religion other than Catholic or Protestant (odds ratio: 4.33; CI, 1.13–16.67), and family income higher than 4 reference wages (odds ratio: 3.50; CI, 1.14–10.75) were factors associated with nonadherence. | Convenience sample from a single centre. Adherence self-reported. Limitations associated with cross sectional design. |
| Tielen, Mirjam [57] Netherlands | To identify young people at risk of non-adherent behaviour. | 26 | Young adults | Comparative study. Q-methodological study. | Once | Questionnaire Q-methodology | Four distinct attitude profiles concerning posttransplant health lifestyle were found among these young adults: (a) concerned and controlled, (b) appearance orientated, (c) opinionated and independent, and (d) easy going and pliable | Self-selecting population. Pilot study. |
| Tong [35] Australia | To explore experiences and perspectives of adolescent kidney transplant recipients following kidney transplantation | 22 | Adolescents | Qualitative study | Once | In-depth interviews. Grounded and thematic analysis. | The overarching theme was achieving a sense of normality. Having the same opportunities and potential to achieve as other adolescents facilitated better adjustment, well-being and positive development after transplant. | Variability in some interviews parents present. Wide age range. |
| Varnell [58] USA | Assess barriers to taking medication for adolescents and young adults | 98 | Both | Prospective cohort study | Over two years | Patients assessed for 14 barriers to medication adherence using the barriers assessment tool | Patients with an identified barrier to adherence were more likely to have BPAR (p = 0.02) than patients without an identified barrier in the 24-months following barriers assessment. | Single centre |
| Wolf [7] USA | To quantify physical activity and grip strength in pediatric kidney transplant recipients and describe attitudes about exercise and exercise counseling given concerns about allograft injury | 101 | Both | Cross sectional analysis. | Once | Patients completed the Physical Activity Questionnaire (PAQ). Grip strength was measured with a dynamometer. We asked about activity limitations and provider counseling. Univariate analysis and multiple linear regression were used to determine independent predictors of PAQ score and grip strength z score. | Median PAQ score was 2.2 (range 0–5) and was lower compared with controls (p < 0.001). The average grip strength z score was −1.1 and −0.7 in the right and left hand, respectively. Predictors of lower grip strength were younger age (p = 0.036), non-African American race (p = 0.029), lower height z score (p = 0.010), and longer percentage of lifetime with kidney disease (p = 0.029). | Non-longitudinal design. Single-centre. Relying on patient recall. |
| Zelikovsky [59] USA | To examine the potentially modifiable barriers related to adherence among adolescent kidney transplant candidates | 56 | Adolescents | Cross-sectional study | Once. | Interviews- around medical adherence and semi-structured interviews (parents present). Medical Adherence Measure (MAM) adherence interview. Qualitative Study. | Better knowledge of the medication regimen was associated with fewer missed doses Patients who perceived more barriers had more missed doses. Patients who endorsed “just forget,” the most common barrier (56.4%), reported significantly more missed doses. | Patient self-reporting. Small sample size. Didn’t look at health provider related issues to adherence. |
References
- Gotta, V.; Tancev, G.; Marsenic, O.; Vogt, J.E.; Pfister, M. Identifying key predictors of mortality in young patients on chronic haemodialysis-a machine learning approach. Nephrol. Dial. Transplant. 2021, 20, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Modi, Z.J.; Lu, Y.; Ji, N.; Kapke, A.; Selewski, D.T.; Dietrich, X.; Abbott, K.; Nallamothu, B.K.; Schaubel, D.E.; Saran, R.; et al. Risk of cardiovascular disease and mortality in young adults with end-stage renal disease: An analysis of the US renal data system. JAMA Cardiol. 2019, 4, 353–362. [Google Scholar] [CrossRef]
- Huang, Y.; Samaniego, M. Preemptive kidney transplantation: Has it come of age? Nephrol. Ther. 2012, 8, 428–432. [Google Scholar] [CrossRef]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef]
- Port, F.K.; Wolfe, R.A.; Mauger, E.A.; Berling, D.P.; Jiang, K. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA 1993, 270, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Tangeraas, T.; Midtvedt, K.; Cvancarova, M.; Hirth, A.; Fredriksen, P.M.; Tonstad, S.; Isaksen, G.A.; Bjerre, A. Cardiorespiratory fitness in young adults with a history of renal transplantation in childhood. Pediatr. Nephrol. 2011, 26, 2041–2049. [Google Scholar] [CrossRef]
- Wolf, M.F.; George, R.P.; Warshaw, B.; Wang, E.; Greenbaum, L.A. Physical Activity and Kidney Injury in Pediatric and Young Adult Kidney Transplant Recipients. J. Pediatr. 2016, 179, 90–95.e2. [Google Scholar] [CrossRef]
- Mellerio, H.; Alberti, C.; Labèguerie, M.; Andriss, B.; Savoye, E.; Lassalle, M.; Jacquelinet, C.; Loirat, C. French Working Group on the Long-Term Outcome of Transplanted Children. Adult social and professional outcomes of pediatric renal transplant recipients. Transplantation 2014, 97, 196–205. [Google Scholar] [CrossRef]
- Supelana, C.; Annunziato, R.A.; Kaplan, D.; Helcer, J.; Stuber, M.L.; Shemesh, E. PTSD in solid organ transplant recipients: Current understanding and future implications. Pediatr. Transplant. 2016, 20, 23–33. [Google Scholar] [CrossRef]
- Dobbels, F.; Skeans, M.A.; Snyder, J.J.; Tuomari, A.V.; Maclean, J.R.; Kasiske, B.L. Depressive disorder in renal transplantation: An analysis of medicare claims. Am. J. Kidney Dis. 2008, 51, 819–828. [Google Scholar] [CrossRef]
- Anthony, S.J.; Hebert, D.; Todd, L.; Korus, M.; Langlois, V.; Pool, R.; Robinson, L.A.; Williams, A.; Pollock-BarZiv, S.M. Child and parental perspectives of multidimensional quality of life outcomes after kidney transplantation. Pediatr Transplant. 2010, 14, 249–256. [Google Scholar] [CrossRef]
- NHS Blood and Transplant. Activity Report 2020–2021. Available online: https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/24043/section-5-kidney-activity.pdf (accessed on 17 January 2023).
- Foster, B.J.; Dahhou, M.; Zhang, X.; Platt, R.W.; Samuel, S.M.; Hanley, J.A. Association between age and graft failure rates in young kidney transplant recipients. Transplantation 2011, 92, 1237–1243. [Google Scholar] [CrossRef]
- Hamilton, A.; Plumb, L.; Casula, A.; Sinha, M.D. P1627 kidney transplant outcomes for children and young adults in the UK. Nephrol. Dial. Transplant. 2021, 36, 1767. [Google Scholar] [CrossRef]
- McCaughan, J.A.; Patterson, C.C.; Maxwell, A.P.; Courtney, A.E. Factors influencing survival after kidney transplant failure. Transplant. Res. 2014, 3, 18. [Google Scholar] [CrossRef]
- Rees, L. Long-term outcome after renal transplantation in childhood. Pediatr. Nephrol. 2009, 24, 475–484. [Google Scholar] [CrossRef]
- Smith, J.M.; Ho, M.; McDonald, R.A. Renal transplant outcomes in adolescents: A report of the North American Pediatric Renal Transplant Cooperative Study. Pediatr. Transplant. 2002, 6, 493–499. [Google Scholar] [CrossRef]
- Melanson, T.A.; Mersha, K.; Patzer, R.E.P.; George, R.P. Loss to follow-up in adolescent and young adult renal transplant recipients. Transplantation 2020, 105, 1326–1336. [Google Scholar] [CrossRef]
- Weeda, E.; Su, Z.; Taber, D.J.; Bian, J.; Morinelli, T.A.; Pilch, N.A.; Mauldin, P.D.; Dubay, D.A. Hospital admissions and emergency department visits among kidney transplant recipients. Clin. Transplant. 2019, 33, e13522. [Google Scholar] [CrossRef]
- Shrestha, B.M. Strategies for reducing the renal transplant waiting list: A review. Exp. Clin. Transplant. 2009, 7, 173–179. [Google Scholar]
- Wallace, D.; Robb, M.; Hughes, W.; Johnson, R.; Ploeg, R.; Neuberger, J.; Forsythe, J.; Cacciola, R. Outcomes of patients suspended from the National Kidney Transplant Waiting List in the United Kingdom Between 2000 and 2010. Transplantation 2020, 104, 1654–1661. [Google Scholar] [CrossRef]
- Van der Heide, I.; Poureslami, I.; Mitic, W.; Shum, J.; Rootman, I.; FitzGerald, J.M. Health literacy in chronic disease management: A matter of interaction. J. Clin. Epidemiol. 2018, 102, 134–138. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K.; Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Pearson, A.; White, H.; Bath-Hextall, F.; Salmond, S.; Apostolo, J.L.A.; Kirkpatrick, P. A mixed-methods approach to systematic reviews. Int. J. Evid.-Based Health 2015, 13, 121–131. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Aasebø, W.; Homb-Vesteraas, N.A.; Hartmann, A.; Stavem, K. Life situation and quality of life in young adult kidney transplant recipients. Nephrol. Dial. Transplant. 2009, 24, 304–308. [Google Scholar] [CrossRef]
- Massey, E.K.; Meys, K.; Kerner, R.; Weimar, W.; Roodnat, J.; Cransberg, K. Young adult kidney transplant recipients: Nonadherent and happy. Transplantation 2015, 99, e89–e96. [Google Scholar]
- Hamilton, A.J.; Caskey, F.J.; Casula, A.; Inward, C.D.; Ben-Shlomo, Y. Associations with Wellbeing and medication adherence in young adults receiving kidney replacement therapy. Clin. J. Am. Soc. Nephrol. 2018, 13, 1669–1679, Erratum in: Clin. J. Am. Soc. Nephrol. 2019, 14, 431. [Google Scholar] [CrossRef] [PubMed]
- Lugasi, T.; Achille, M.; Blydt-Hansen, T.; Clermont, M.-J.; Geoffroy, L.; Legault, L.; Phan, V.; Bell, L.E. Assessment of identity and quality of life in diabetic and renal transplant adolescents in comparison to healthy adolescents. J. Clin. Psychol. Med. Settings 2013, 20, 361–372. [Google Scholar] [CrossRef]
- Simons, L.E.; Anglin, G.; Warshaw, B.L.; Mahle, W.T.; Vincent, R.N.; Blount, R.L. Understanding the pathway between the transplant experience and health-related quality of life outcomes in adolescents. Pediatr. Transplant. 2008, 12, 187–193. [Google Scholar] [CrossRef]
- Tong, A.; Morton, R.; Howard, K.; McTaggart, S.; Craig, J.C. “When I had my transplant, I became normal”. Adolescent perspectives on life after kidney transplantation. Pediatr. Transplant. 2011, 15, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Quinn, S.M.; Fernandez, H.; McCorkle, T.; Rogers, R.; Hussain, S.; Ford, C.A.; Barg, F.K.; Ginsburg, K.R.; Amaral, S. The role of resilience in healthcare transitions among adolescent kidney transplant recipients. Pediatr. Transplant. 2019, 23, e13559. [Google Scholar] [CrossRef] [PubMed]
- Boucquemont, J.; Pai, A.L.H.; Dharnidharka, V.R.; Hebert, D.; Zelikovsky, N.; Amaral, S.; Furth, S.L.; Foster, B.J. Association between day of the week and medication adherence among adolescent and young adult kidney transplant recipients. Am. J. Transplant. 2020, 20, 274–281. [Google Scholar] [CrossRef]
- Jakubowska-Winecka, A.; Biernacka, M. Parental attitudes and medication adherence in groups of adolescents after liver and kidney transplantations. Transplant. Proc. 2018, 50, 2145–2149. [Google Scholar] [CrossRef]
- Penkower, L.; Dew, M.A.; Ellis, D.; Sereika, S.M.; Kitutu, J.M.M.; Shapiro, R. Psychological distress and adherence to the medical regimen among adolescent renal transplant recipients. Am. J. Transplant. 2003, 3, 1418–1425. [Google Scholar] [CrossRef]
- Korus, M.; Stinson, J.N.; Pool, R.; Williams, A.; Kagan, S. Exploring the information needs of adolescents and their parents throughout the kidney transplant continuum. Prog. Transplant. 2011, 21, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Dobbels, F.; Decorte, A.; Roskams, A.; Van Damme-Lombaerts, R. Health-related quality of life, treatment adherence, symptom experience and depression in adolescent renal transplant patients. Pediatr. Transplant. 2010, 14, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Malekahmadi, M.R.; Rahimzadeh, S.; Nejad, M.L.D.; Lankarani, M.M.; Einollahi, B.; Assari, S. Importance of socioeconomic, clinical, and psychological factors on health-related quality of life in adolescents after kidney transplant. Exp. Clin. Transplant. 2011, 9, 50–55. [Google Scholar]
- Kärrfelt, H.M.; Lindblad, F.I.; Crafoord, J.; Berg, U.B. Renal transplantation: Long-term adaptation and the children’s own reflections. Pediatr. Transplant. 2003, 7, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Mintzer, L.L.; Stuber, M.L.; Seacord, D.; Castaneda, M.; Mesrkhani, V.; Glover, D. Traumatic stress symptoms in adolescent organ transplant recipients. Pediatrics 2005, 115, 1640–1644. [Google Scholar] [CrossRef] [PubMed]
- Milton, B.; Holland, P.; Whitehead, M. The social and economic consequences of childhood-onset Type 1 diabetes mellitus across the lifecourse: A systematic review. Diabet. Med. 2006, 23, 821–829. [Google Scholar] [CrossRef]
- Enskär, K.; Berterö, C. Young adult survivors of childhood cancer; Experiences affecting self-image, relationships, and present life. Cancer Nurs. 2010, 33, E18–E24. [Google Scholar] [CrossRef] [PubMed]
- Wahl, A.K.; Rustøen, T.; Hanestad, B.R.; Gjengedal, E.; Moum, T. Living with cystic fibrosis: Impact on global quality of life. Heart Lung 2005, 34, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Akchurin, O.M.; Melamed, M.L.; Hashim, B.L.; Kaskel, F.J.; Del Rio, M. Medication adherence in the transition of adolescent kidney transplant recipients to the adult care. Pediatr. Transplant. 2014, 18, 538–548. [Google Scholar] [CrossRef]
- Ashoor, I.; Avilés, D.; Pasternak, R.; Vehaskari, V.M. Sexually transmitted infections in pediatric renal transplant recipients: Time to take notice! Pediatr. Transplant. 2015, 19, 584–587. [Google Scholar] [CrossRef]
- Bullington, P.; Pawola, L.; Walker, R.; Valenta, A.; Briars, L.; John, E. Identification of medication non-adherence factors in adolescent transplant patients: The patient’s viewpoint. Pediatr. Transplant. 2007, 11, 914–921. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Jones, C.L.; Walker, R.G.; Sawyer, S.M. The transition of kidney transplant recipients: A work in progress. Pediatr. Nephrol. 2009, 24, 1055–1060. [Google Scholar] [CrossRef]
- Kim, S.; Choi, H. Experiences of Korean adolescent renal transplant recipients. J. Spéc. Pediatr. Nurs. 2016, 21, 158–165. [Google Scholar] [CrossRef]
- Kullgren, K.A.; Hmiel, S.P.; Gevers, A. Measuring family management of transplant tasks: The transplant responsibility questionnaire. Pediatr. Transplant. 2013, 17, 307–314. [Google Scholar] [CrossRef]
- Silva, A.C.M.; Sanders-Pinheiro, H.; Leite, R.F.; Joseph, M.P.C.; Pestana, J.O.M.; Schirmer, J.; de Aguiar, R.B. Nonadherence to immunosuppressive medications following pediatric kidney transplantation within full cost coverage health system: Prevalence and correlates. Exp. Clin. Transplant. 2020, 18, 577–584. [Google Scholar] [CrossRef]
- Nguyen, C.; Dew, M.A.; Irizarry, T.; McNulty, M.; Rennick, J.; Knäuper, B.; Descoteaux, A.; Grenier, A.; Jeannot, L.; Foster, B.J.; et al. Promoting medication adherence from the perspective of adolescent and young adult kidney transplant recipients, parents, and health care professionals: A TAKE-IT TOO study. Pediatr. Transplant. 2020, 24, e13709. [Google Scholar] [CrossRef]
- Quast, L.F.; Gutiérrez-Colina, A.M.; Cushman, G.K.; Rea, K.E.; Eaton, C.K.; Lee, J.L.; George, R.P.; Blount, R.L. Adherence barriers for adolescent and young adult transplant recipients: Relations to personality. J. Pediatr. Psychol. 2020, 45, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Tielen, M.; van Staa, A.L.; Jedeloo, S.; van Exel, N.J.A.; Weimar, W. Q-Methodology to identify young adult renal transplant recipients at risk for nonadherence. Transplantation 2008, 85, 700–706. [Google Scholar] [CrossRef]
- Varnell, C.D.; Rich, K.L.; Zhang, B.; Carle, A.C.; Pai, A.L.H.; Modi, A.C.; Hooper, D.K. Predicting acute rejection in children, adolescents, and young adults with a kidney transplant by assessing barriers to taking medication. Pediatr. Nephrol. 2021, 36, 2453–2461. [Google Scholar] [CrossRef] [PubMed]
- Zelikovsky, N.; Schast, A.P.; Palmer, J.; Meyers, K.E. Perceived barriers to adherence among adolescent renal transplant candidates. Pediatr. Transplant. 2008, 12, 300–308. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corr, M.; McKeaveney, C.; Wurm, F.; Courtney, A.E.; Noble, H. The Educational Needs of Adolescent and Young Adult Renal Transplant Recipients—A Scoping Review. Healthcare 2023, 11, 566. https://doi.org/10.3390/healthcare11040566
Corr M, McKeaveney C, Wurm F, Courtney AE, Noble H. The Educational Needs of Adolescent and Young Adult Renal Transplant Recipients—A Scoping Review. Healthcare. 2023; 11(4):566. https://doi.org/10.3390/healthcare11040566
Chicago/Turabian StyleCorr, Michael, Clare McKeaveney, Fina Wurm, Aisling E. Courtney, and Helen Noble. 2023. "The Educational Needs of Adolescent and Young Adult Renal Transplant Recipients—A Scoping Review" Healthcare 11, no. 4: 566. https://doi.org/10.3390/healthcare11040566