
The Executive-Function-Related Cognitive–Motor Dual Task Walking Performance and Task Prioritizing Effect on People with Parkinson’s Disease


Abstract
:1. Introduction
2. Materials and Methods
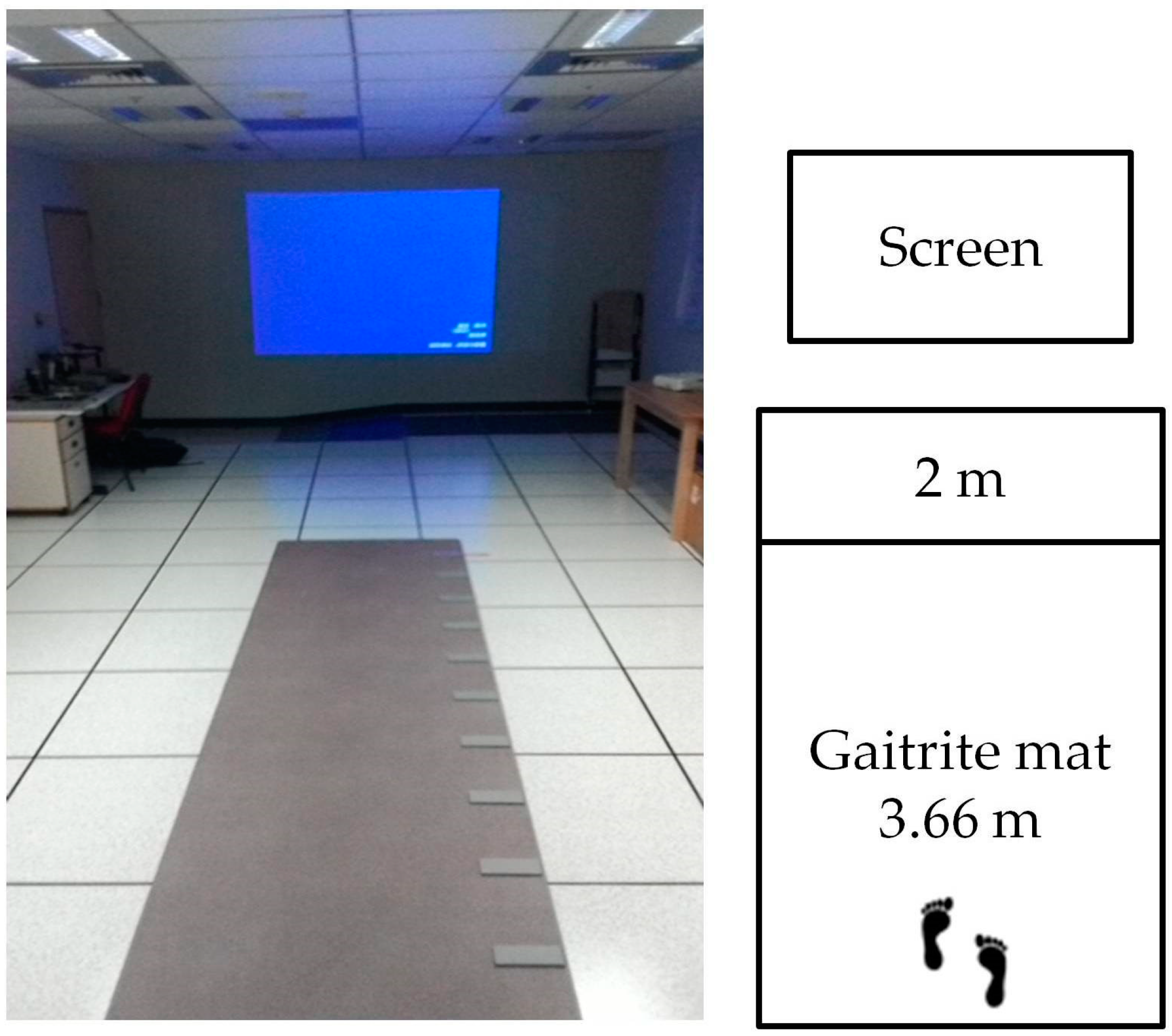
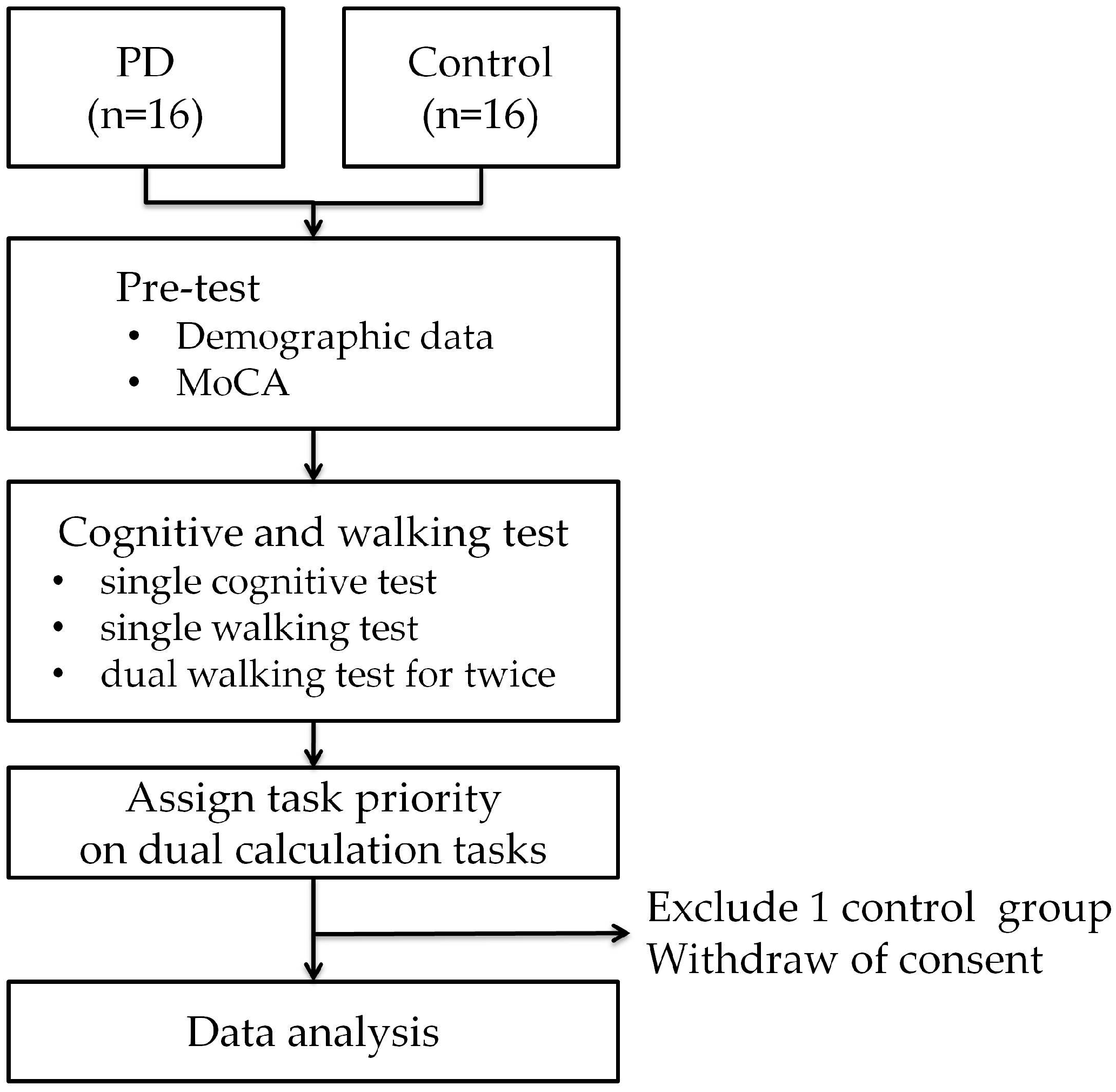
2.1. Research Design and Subjects
2.2. Data Processing and Analysis
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
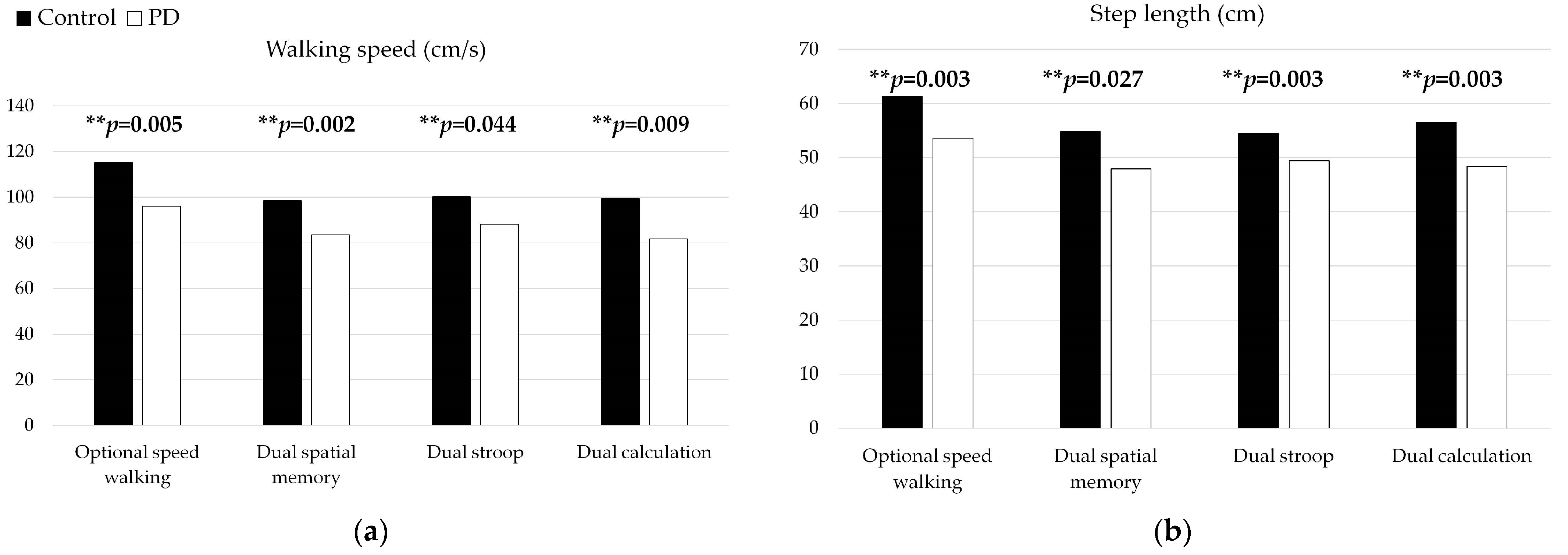
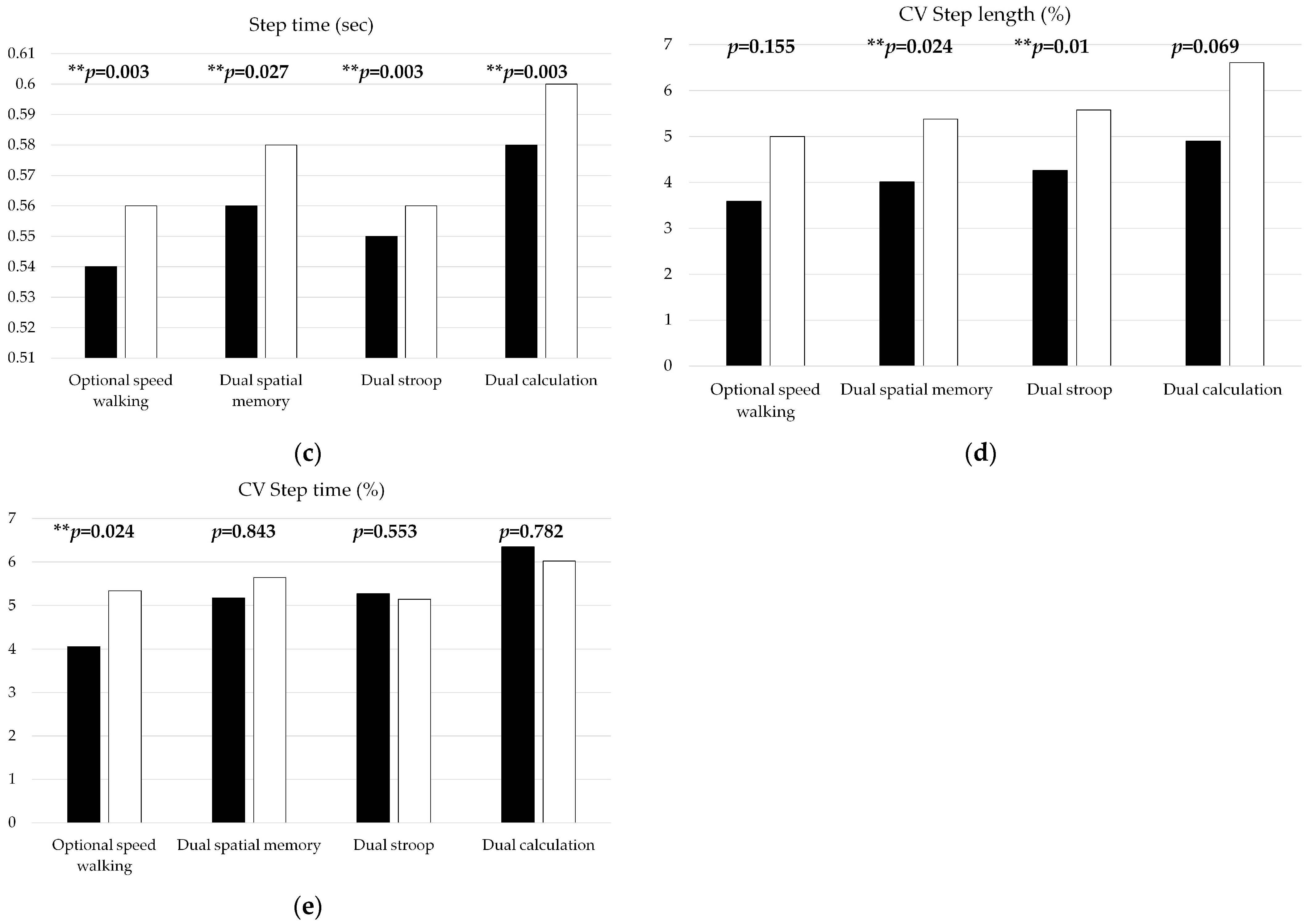
3.2. Gait Performance of Healthy Group and Parkinson’s Disease Group under Single Walking Task and Dual Task
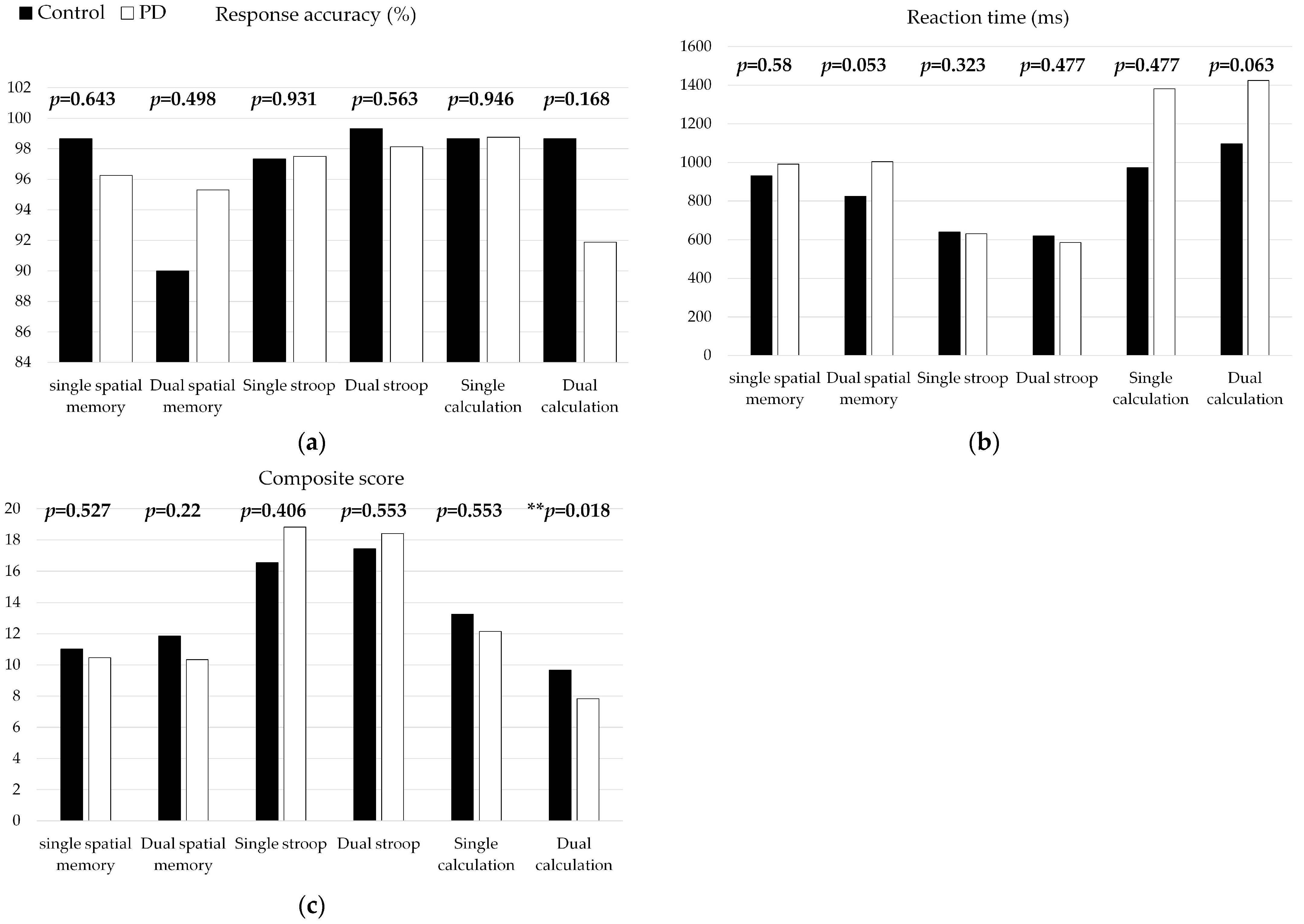
3.3. Cognitive Performance of Healthy Group and PD Group under Single Cognitive Task and Dual Task
3.4. The Performance of Dual Calculation Tasks in the Control Group and the Parkinson’s Disease Group under Designated Task Priority (Comparing the Difference between Gait Priority and Calculation Priority)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beitz, J.M. Parkinson’s disease: A review. Front. Biosci. 2014, 6, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural. Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef] [PubMed]
- de Lau, L.M.; Breteler, M.M. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Foltynie, T.; Brayne, C.E.; Robbins, T.W.; Barker, R.A. The cognitive ability of an incident cohort of Parkinson’s patients in the UK. The CamPaIGN study. Brain 2004, 127, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Zgaljardic, D.J.; Borod, J.C.; Foldi, N.S.; Mattis, P. A review of the cognitive and behavioral sequelae of Parkinson’s disease: Relationship to frontostriatal circuitry. Cogn. Behav. Neurol. 2003, 16, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.M.; Martins, E.F.; Delattre, A.M.; Proenca, M.B.; Mori, M.A.; Carabelli, B.; Ferraz, A.C. Motor and non-motor features of Parkinson’s disease-a review of clinical and experimental studies. CNS Neurol. Disord. Drug Targets 2012, 11, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Hiura, M.; Nemoto, H.; Nishisaka, K.; Higashi, K.; Katoh, T. The association between walking ability and falls in elderly Japanese living in the community using a path analysis. J. Community Health 2012, 37, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.H.; Hariz, G.M.; Iwarsson, S.; Hagell, P. Walking ability is a major contributor to fear of falling in people with Parkinson’s disease: Implications for rehabilitation. Park. Dis. 2012, 2012, 713236. [Google Scholar] [CrossRef] [PubMed]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342; quiz 472. [Google Scholar] [CrossRef]
- Kimura, N.; van Deursen, R. The Effect Of Visual Dual-Tasking Interference On Walking In Healthy Young Adults. Gait Posture 2020, 79, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Chawla, H.; Walia, S.; Behari, M.; Noohu, M.M. Effect of type of secondary task on cued gait on people with idiopathic Parkinson’s disease. J. Neurosci. Rural. Pract. 2014, 5, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Kelly, V.E.; Eusterbrock, A.J.; Shumway-Cook, A. A review of dual-task walking deficits in people with Parkinson’s disease: Motor and cognitive contributions, mechanisms, and clinical implications. Park. Dis. 2012, 2012, 918719. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.; Baker, K.; Nieuwboer, A.; Burn, D.; Rochester, L. Gait variability in Parkinson’s disease: An indicator of non-dopaminergic contributors to gait dysfunction? J. Neurol. 2011, 258, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Yogev-Seligmann, G.; Giladi, N.; Gruendlinger, L.; Hausdorff, J.M. The contribution of postural control and bilateral coordination to the impact of dual tasking on gait. Exp. Brain Res. 2013, 226, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Zirek, E.; Ersoz Huseyinsinoglu, B.; Tufekcioglu, Z.; Bilgic, B.; Hanagasi, H. Which cognitive dual-task walking causes most interference on the Timed Up and Go test in Parkinson’s disease: A controlled study. Neurol. Sci. 2018, 39, 2151–2157. [Google Scholar] [CrossRef]
- Johansson, H.; Ekman, U.; Rennie, L.; Peterson, D.S.; Leavy, B.; Franzén, E. Dual-Task Effects During a Motor-Cognitive Task in Parkinson’s Disease: Patterns of Prioritization and the Influence of Cognitive Status. Neurorehabil. Neural. Repair 2021, 35, 356–366. [Google Scholar] [CrossRef]
- Clark, D.J. Automaticity of walking: Functional significance, mechanisms, measurement and rehabilitation strategies. Front. Hum. Neurosci. 2015, 9, 246. [Google Scholar] [CrossRef] [PubMed]
- Poldrack, R.A.; Sabb, F.W.; Foerde, K.; Tom, S.M.; Asarnow, R.F.; Bookheimer, S.Y.; Knowlton, B.J. The neural correlates of motor skill automaticity. J. Neurosci. 2005, 25, 5356–5364. [Google Scholar] [CrossRef]
- Yogev, G.; Giladi, N.; Peretz, C.; Springer, S.; Simon, E.S.; Hausdorff, J.M. Dual tasking, gait rhythmicity, and Parkinson’s disease: Which aspects of gait are attention demanding? Eur. J. Neurosci. 2005, 22, 1248–1256. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Schweiger, A.; Herman, T.; Yogev-Seligmann, G.; Giladi, N. Dual-task decrements in gait: Contributing factors among healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 1335–1343. [Google Scholar] [CrossRef]
- O’Shea, S.; Morris, M.E.; Iansek, R. Dual task interference during gait in people with Parkinson disease: Effects of motor versus cognitive secondary tasks. Phys. Ther. 2002, 82, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Pashler, H. Dual-task interference in simple tasks: Data and theory. Psychol. Bull. 1994, 116, 220–244. [Google Scholar] [CrossRef] [PubMed]
- Ruthruff, E.; Pashler, H.E.; Klaassen, A. Processing bottlenecks in dual-task performance: Structural limitation or strategic postponement? Psychon. Bull. Rev. 2001, 8, 73–80. [Google Scholar] [CrossRef]
- Salazar, R.D.; Ren, X.; Ellis, T.D.; Toraif, N.; Barthelemy, O.J.; Neargarder, S.; Cronin-Golomb, A. Dual tasking in Parkinson’s disease: Cognitive consequences while walking. Neuropsychology 2017, 31, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Plotnik, M.; Dagan, Y.; Gurevich, T.; Giladi, N.; Hausdorff, J.M. Effects of cognitive function on gait and dual tasking abilities in patients with Parkinson’s disease suffering from motor response fluctuations. Exp. Brain Res. 2011, 208, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Giladi, N.; McDermott, M.P.; Fahn, S.; Przedborski, S.; Jankovic, J.; Stern, M.; Tanner, C. Freezing of gait in PD: Prospective assessment in the DATATOP cohort. Neurology 2001, 56, 1712–1721. [Google Scholar] [CrossRef] [PubMed]
- Muslimović, D.; Schmand, B.; Speelman, J.D.; de Haan, R.J. Course of cognitive decline in Parkinson’s disease: A meta-analysis. J. Int. Neuropsychol. Soc. 2007, 13, 920–932. [Google Scholar] [CrossRef]
- Watson, G.S.; Leverenz, J.B. Profile of cognitive impairment in Parkinson’s disease. Brain Pathol. 2010, 20, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Springer, S.; Giladi, N.; Peretz, C.; Yogev, G.; Simon, E.S.; Hausdorff, J.M. Dual-tasking effects on gait variability: The role of aging, falls, and executive function. Mov. Disord. 2006, 21, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Gauggel, S.; Rieger, M.; Feghoff, T.A. Inhibition of ongoing responses in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2004, 75, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Pillon, B.; Deweer, B.; Vidailhet, M.; Bonnet, A.M.; Hahn-Barma, V.; Dubois, B. Is impaired memory for spatial location in Parkinson’s disease domain specific or dependent on ‘strategic’ processes? Neuropsychologia 1998, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Small, G.H.; Neptune, R.R. Task-prioritization and balance recovery strategies used by young healthy adults during dual-task walking. Gait. Posture 2022, 95, 115–120. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.; van Dijk, J.G.; Munneke, M. The “posture second” strategy: A review of wrong priorities in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 196–204. [Google Scholar] [CrossRef]
- Longhurst, J.K.; Rider, J.V.; Cummings, J.L.; John, S.E.; Poston, B.; Held Bradford, E.C.; Landers, M.R. A Novel Way of Measuring Dual-Task Interference: The Reliability and Construct Validity of the Dual-Task Effect Battery in Neurodegenerative Disease. Neurorehabil. Neural. Repair 2022, 36, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Yogev-Seligmann, G.; Rotem-Galili, Y.; Mirelman, A.; Dickstein, R.; Giladi, N.; Hausdorff, J.M. How does explicit prioritization alter walking during dual-task performance? Effects of age and sex on gait speed and variability. Phys. Ther. 2010, 90, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Nazem, S.; Siderowf, A.D.; Duda, J.E.; Have, T.T.; Colcher, A.; Horn, S.S.; Moberg, P.J.; Wilkinson, J.R.; Hurtig, H.I.; Stern, M.B.; et al. Montreal cognitive assessment performance in patients with Parkinson’s disease with “normal” global cognition according to mini-mental state examination score. J. Am. Geriatr. Soc. 2009, 57, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Zadikoff, C.; Fox, S.H.; Tang-Wai, D.F.; Thomsen, T.; de Bie, R.M.; Wadia, P.; Miyasaki, J.; Duff-Canning, S.; Lang, A.E.; Marras, C. A comparison of the mini mental state exam to the Montreal cognitive assessment in identifying cognitive deficits in Parkinson’s disease. Mov. Disord. 2008, 23, 297–299. [Google Scholar] [CrossRef]
- Walton, C.C.; Shine, J.M.; Mowszowski, L.; Gilat, M.; Hall, J.M.; O’Callaghan, C.; Naismith, S.L.; Lewis, S.J. Impaired cognitive control in Parkinson’s disease patients with freezing of gait in response to cognitive load. J. Neural. Transm. 2015, 122, 653–660. [Google Scholar] [CrossRef]
- Brauer, S.G.; Morris, M.E. Can people with Parkinson’s disease improve dual tasking when walking? Gait Posture 2010, 31, 229–233. [Google Scholar] [CrossRef]
- Zanardi, A.P.J.; da Silva, E.S.; Costa, R.R.; Passos-Monteiro, E.; Dos Santos, I.O.; Kruel, L.F.M.; Peyré-Tartaruga, L.A. Gait parameters of Parkinson’s disease compared with healthy controls: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 752. [Google Scholar] [CrossRef] [PubMed]
- Welzel, J.; Wendtland, D.; Warmerdam, E.; Romijnders, R.; Elshehabi, M.; Geritz, J.; Berg, D.; Hansen, C.; Maetzler, W. Step Length Is a Promising Progression Marker in Parkinson’s Disease. Sensors 2021, 21, 2292. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.R.; Lien, C.Y.; Huang, C.C.; Lin, W.C.; Chen, Y.S.; Yu, C.C.; Cheng, B.C.; Kung, C.T.; Kung, C.F.; Chiang, Y.F.; et al. Clinical Disease Severity Mediates the Relationship between Stride Length and Speed and the Risk of Falling in Parkinson’s Disease. J. Pers. Med. 2022, 12, 192. [Google Scholar] [CrossRef] [PubMed]
- Gabell, A.; Nayak, U.S. The effect of age on variability in gait. J. Gerontol. 1984, 39, 662–666. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Cudkowicz, M.E.; Firtion, R.; Wei, J.Y.; Goldberger, A.L. Gait variability and basal ganglia disorders: Stride-to-stride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov. Disord. 1998, 13, 428–437. [Google Scholar] [CrossRef]
- Hirata, K.; Hattori, T.; Kina, S.; Chen, Q.; Ohara, M.; Yokota, T. Striatal Dopamine Denervation Impairs Gait Automaticity in Drug-Naïve Parkinson’s Disease Patients. Mov. Disord. 2020, 35, 1037–1045. [Google Scholar] [CrossRef]
- Collett, J.; Fleming, M.K.; Meester, D.; Al-Yahya, E.; Wade, D.T.; Dennis, A.; Salvan, P.; Meaney, A.; Cockburn, J.; Dawes, J.; et al. Dual-task walking and automaticity after Stroke: Insights from a secondary analysis and imaging sub-study of a randomised controlled trial. Clin. Rehabil. 2021, 35, 1599–1610. [Google Scholar] [CrossRef]
- Palliyath, S.; Hallett, M.; Thomas, S.L.; Lebiedowska, M.K. Gait in patients with cerebellar ataxia. Mov. Disord. 1998, 13, 958–964. [Google Scholar] [CrossRef]
- Wu, T.; Hallett, M. Neural correlates of dual task performance in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2008, 79, 760–766. [Google Scholar] [CrossRef]
- Martin-Signes, M.; Paz-Alonso, P.M.; Chica, A.B. Connectivity of Frontoparietal Regions Reveals Executive Attention and Consciousness Interactions. Cereb Cortex 2019, 29, 4539–4550. [Google Scholar] [CrossRef]
- Chajut, E.; Schupak, A.; Algom, D. Are spatial and dimensional attention separate? evidence from Posner, Stroop, and Eriksen tasks. Mem. Cognit. 2009, 37, 924–934. [Google Scholar] [CrossRef]
- Ambrosini, E.; Vallesi, A. Domain-general Stroop Performance and Hemispheric Asymmetries: A Resting-state EEG Study. J. Cogn. Neurosci. 2017, 29, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Papanicolaou, A.C.; Schmidt, A.L.; Moore, B.D.; Eisenberg, H.M. Cerebral activation patterns in an arithmetic and a visuospatial processing task. Int. J. Neurosci. 1983, 20, 283–287. [Google Scholar] [CrossRef]
- Nolde, S.F.; Johnson, M.K.; D’Esposito, M. Left prefrontal activation during episodic remembering: An event-related fMRI study. Neuroreport 1998, 9, 3509–3514. [Google Scholar] [CrossRef]
- Kazui, H.; Kitagaki, H.; Mori, E. Cortical activation during retrieval of arithmetical facts and actual calculation: A functional magnetic resonance imaging study. Psychiatry Clin. Neurosci. 2000, 54, 479–485. [Google Scholar] [CrossRef]
- Sanchez-Gomez, J.; Villafaina, S.; Dominguez-Munoz, F.J.; Leon-Llamas, J.L.; Murillo-Garcia, A.; Gusi, N. Comparison between the Impacts of Memory and Arithmetic-Based Dual Tasks on Physical Performance in Women with Fibromyalgia. Biology 2022, 11, 947. [Google Scholar] [CrossRef]
- Wild, L.B.; de Lima, D.B.; Balardin, J.B.; Rizzi, L.; Giacobbo, B.L.; Oliveira, H.B.; de Lima, A., II; Peyré-Tartaruga, L.A.; Rieder, C.R.; Bromberg, E. Characterization of cognitive and motor performance during dual-tasking in healthy older adults and patients with Parkinson’s disease. J. Neurol. 2013, 260, 580–589. [Google Scholar] [CrossRef]
- Cooper, J.A.; Sagar, H.J.; Jordan, N.; Harvey, N.S.; Sullivan, E.V. Cognitive impairment in early, untreated Parkinson’s disease and its relationship to motor disability. Brain 1991, 114, 2095–2122. [Google Scholar] [CrossRef] [PubMed]
- Fitts, P.M. The information capacity of the human motor system in controlling the amplitude of movement. J. Exp. Psychol. 1954, 47, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Burn, D.J.; Rowan, E.N.; Allan, L.M.; Molloy, S.; O’Brien, J.T.; McKeith, I.G. Motor subtype and cognitive decline in Parkinson’s disease, Parkinson’s disease with dementia, and dementia with Lewy bodies. J. Neurol. Neurosurg. Psychiatry 2006, 77, 585–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankovic, J.; Kapadia, A.S. Functional decline in Parkinson disease. Arch. Neurol. 2001, 58, 1611–1615. [Google Scholar] [CrossRef] [PubMed]
- Onder, H.; Ozyurek, O. The impact of distinct cognitive dual-tasks on gait in Parkinson’s disease and the associations with the clinical features of Parkinson’s disease. Neurol. Sci. 2021, 42, 2775–2783. [Google Scholar] [CrossRef] [PubMed]
- Baker, K.; Rochester, L.; Nieuwboer, A. The immediate effect of attentional, auditory, and a combined cue strategy on gait during single and dual tasks in Parkinson’s disease. Arch. Phys. Med. Rehabil. 2007, 88, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Canning, C.G. The effect of directing attention during walking under dual-task conditions in Parkinson’s disease. Park. Relat. Disord. 2005, 11, 95–99. [Google Scholar] [CrossRef]
- Fok, P.; Farrell, M.; McMeeken, J. Prioritizing gait in dual-task conditions in people with Parkinson’s. Hum. Mov. Sci. 2010, 29, 831–842. [Google Scholar] [CrossRef] [PubMed]
- Yogev-Seligmann, G.; Rotem-Galili, Y.; Dickstein, R.; Giladi, N.; Hausdorff, J.M. Effects of explicit prioritization on dual task walking in patients with Parkinson’s disease. Gait Posture 2012, 35, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Siciliano, M.; Trojano, L.; Santangelo, G.; De Micco, R.; Tedeschi, G.; Tessitore, A. Fatigue in Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2018, 33, 1712–1723. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Healthy Group (n = 15) | PD Group (n = 16) | p-Value |
|---|---|---|---|
| Male | 11 (73.33%) | 11 (68.75%) | 0.779 |
| Female | 4 (26.67%) | 5 (31.25%) | |
| Age (years) | 60.93 ± 2.87 | 63.13 ± 5.75 | 0.241 |
| Height (cm) | 164.33 ± 8.09 | 163.59 ± 8.22 | 0.968 |
| Weight (kg) | 66.23 ± 10.85 | 64.34 ± 9.86 | 0.579 |
| Left Foot Length (cm) | 96.40 ± 5.11 | 94.50 ± 4.95 | 0.405 |
| Right Foot Length (cm) | 96.37 ± 5.13 | 94.59 ± 4.71 | 0.394 |
| Education Level (years) | 12.93 ± 3.26 | 13.06 ± 3.49 | 0.777 |
| Montreal Cognitive Assessment Score | 27.80 ± 1.42 | 27.81 ± 1.28 | 0.855 |
| PD Group No. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | M | M | M | F | M | F | F | M | M | F | M | M | M | M | M | F |
| Age (yrs) | 63 | 63 | 71 | 63 | 64 | 61 | 64 | 60 | 74 | 58 | 58 | 57 | 54 | 65 | 61 | 74 |
| Height (cm) | 161 | 169 | 169 | 150 | 168 | 148 | 155 | 165 | 155 | 161 | 172 | 172 | 170 | 163 | 176 | 163 |
| Weight (kg) | 75 | 68 | 63 | 62 | 80 | 51 | 57 | 62 | 58 | 55 | 80 | 65 | 73 | 62 | 72 | 46 |
| Left Leg Length (cm) | 93 | 97 | 97 | 88 | 93 | 85 | 91 | 94 | 88 | 92 | 102 | 99 | 98 | 95 | 102 | 98 |
| Right Leg Length (cm) | 92 | 97 | 98 | 89 | 93 | 86 | 92 | 94 | 87 | 92 | 102 | 98 | 98 | 94 | 101 | 99 |
| Education Level (yrs) | 6 | 14 | 14 | 12 | 16 | 14 | 6 | 16 | 14 | 12 | 18 | 14 | 16 | 16 | 12 | 9 |
| MoCA | 26 | 28 | 26 | 28 | 26 | 28 | 27 | 26 | 28 | 28 | 29 | 29 | 28 | 29 | 30 | 29 |
| Modified H&Y | 2.5 | 1.5 | 3 | 1.5 | 1.5 | 2.5 | 1.5 | 2.5 | 2.5 | 1.5 | 2.5 | 2.5 | 1.5 | 1 | 1 | 2 |
| Disease Duration (yrs) | 4 | 3 | 6 | 5 | 7 | 3 | 7 | 11 | 6 | 2 | 4 | 6 | 4 | 4 | 3 | 9 |
| Levodopa Equivalent Dosage (mg/day) | 600 | 500 | 770 | 500 | 600 | 360 | 850 | 750 | 710 | 460 | 400 | 700 | 500 | 360 | 180 | 620 |
| Control Group (n = 15) | PD Group (n = 16) | p-Value | |
|---|---|---|---|
| Focus on Walking Task | |||
| Walking Speed (cm/s) | 127.93 ± 14.54 | 120.39 ± 27.90 | 0.22 |
| Step Length (cm) | 63.98 ± 5.43 | 62.49 ± 10.99 | 0.519 |
| Step Time(s) | 0.50 ± 0.04 | 0.53 ± 0.06 | 0.317 |
| CV Step Length (%) | 4.12 ± 1.93 | 4.78 ± 2.51 | 0.401 |
| CV Step Time (%) | 4.43 ± 1.39% | 6.25 ± 2.54 | 0.093 |
| Response Accuracy (%) | 95.33 ± 13.56 | 72.50 ± 32.51 | 0.037 |
| Reaction Time (ms) | 1027.29 ± 243.03 | 957.83 ± 347.68 | 0.651 |
| Composite Score | 9.86 ± 3.15 | 8.21 ± 4.80 | 0.156 |
| Focus on Cognitive Task | |||
| Walking Speed (cm/s) | 106.77 ± 17.38 | 93.60 ± 17.55 | 0.106 |
| Step Length (cm) | 58.26 ± 6.38 | 52.19 ± 8.49 | 0.081 |
| Step Time(s) | 0.55 ± 0.05 | 0.56 ± 0.05 | 0.561 |
| CV Step Length (%) | 3.69 ± 2.24 | 4.29 ± 1.39 | 0.121 |
| CV Step Time (%) | 4.53 ± 1.05% | 7.02 ± 3.08% | 0.053 |
| Response Accuracy (%) | 100.00 ± 0.00 | 95.00 ± 14.14 | 0.171 |
| Reaction Time (ms) | 1171.15 ± 387.49 | 1033.89 ± 290.91 | 0.366 |
| Composite Score | 9.52 ± 3.39 | 9.94 ± 3.08 | 0.438 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-P.; Lin, I.-I.; Chiou, W.-D.; Chang, H.-C.; Chen, R.-S.; Lu, C.-S.; Chang, Y.-J. The Executive-Function-Related Cognitive–Motor Dual Task Walking Performance and Task Prioritizing Effect on People with Parkinson’s Disease. Healthcare 2023, 11, 567. https://doi.org/10.3390/healthcare11040567
Lin Y-P, Lin I-I, Chiou W-D, Chang H-C, Chen R-S, Lu C-S, Chang Y-J. The Executive-Function-Related Cognitive–Motor Dual Task Walking Performance and Task Prioritizing Effect on People with Parkinson’s Disease. Healthcare. 2023; 11(4):567. https://doi.org/10.3390/healthcare11040567
Chicago/Turabian StyleLin, Yen-Po, I-I Lin, Wei-Da Chiou, Hsiu-Chen Chang, Rou-Shayn Chen, Chin-Song Lu, and Ya-Ju Chang. 2023. "The Executive-Function-Related Cognitive–Motor Dual Task Walking Performance and Task Prioritizing Effect on People with Parkinson’s Disease" Healthcare 11, no. 4: 567. https://doi.org/10.3390/healthcare11040567