
A Service Reconfiguration Bundle for Expanding Access to Peritoneal Dialysis Including for Older Frailer Patients
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Service Offered Prior to Reconfiguration
2.2. Service Reconfiguration Bundle
2.3. Technical Details
2.3.1. Laparoscopic Surgical PD Catheter Insertion
2.3.2. Percutaneous PD Catheter Insertions
2.3.3. Peri-Procedural Care
2.4. Data Collection and Analysis
3. Results
3.1. Introduction of a Wider Portfolio of PD Catheter Insertion Techniques
3.2. Offering PD to a Wider Group of Patients, Including Those Considered High-Risk for General Anaesthesia and with Extensive Previous Surgery
3.3. Offering Urgent and Early Start PD
3.4. Performing Elective PD Catheter Insertions in Multiple NHS and Independent Sector Sites
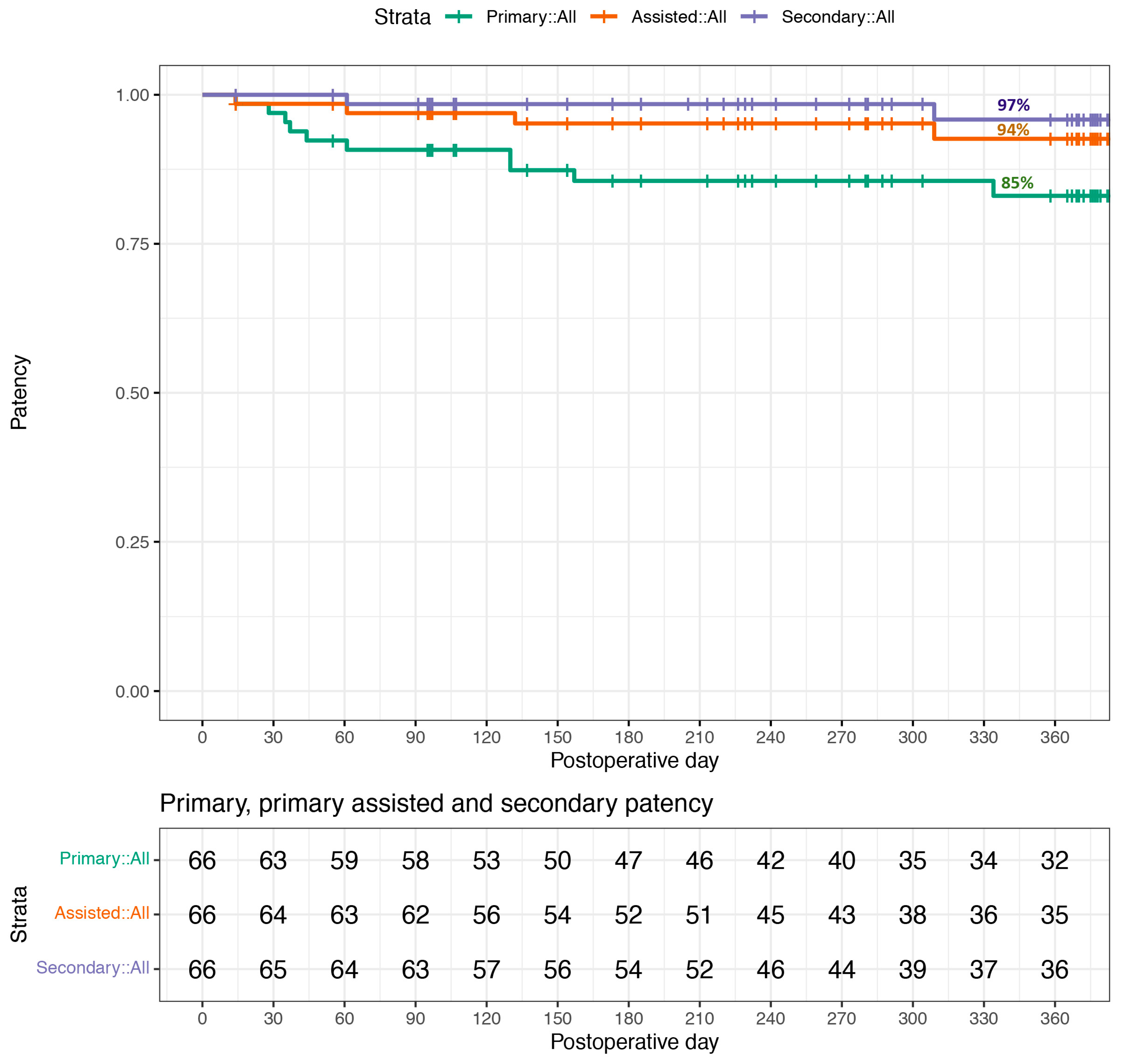
3.5. Outcomes
4. Discussion
4.1. Staffing Expertise and Training
4.2. Introducing a Wider Portfolio of PD Catheter Insertion Techniques
4.3. Being Able to Facilitate Urgent and Early Start PD
4.4. Use of Elective Hubs
4.5. Future Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brück, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Völzke, H.; Ärnlöv, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. 2015, 27, 2135–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liyanage, T.; Ninomiya, T.; Jha, V.; Neal, B.; Patrice, H.M.; Okpechi, I.; Zhao, M.-H.; Lv, J.; Garg, A.X.; Knight, J.; et al. World-wide access to treatment for end-stage kidney disease: A systematic review. Lancet 2015, 385, 1975–1982. [Google Scholar] [CrossRef] [PubMed]
- Marshall, M.R. The benefit of early survival on PD versus HD—Why this is (still) very important. Perit. Dial. Int. 2020, 40, 405–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardezi, A.I.; Aziz, F.; Parajuli, S. The Role of Peritoneal Dialysis in Different Phases of Kidney Transplantation. Kidney 2022, 3, 779–787. [Google Scholar] [CrossRef]
- Dimkovic, N.; Oreopoulos, D.G. Chronic Peritoneal Dialysis in the Elderly. Semin. Dial. 2002, 15, 94–97. [Google Scholar] [CrossRef]
- Woodrow, G.; Fan, S.L.; Reid, C.; Denning, J.; Pyrah, A.N. Renal Association Clinical Practice Guideline on peritoneal dialysis in adults and children. BMC Nephrol. 2017, 18, 333. [Google Scholar] [CrossRef] [Green Version]
- Cameron, J.; Whiteside, C.; Katz, J.; Devins, G.M. Differences in quality of life across renal replacement therapies: A meta-analytic comparison. Am. J. Kidney Dis. 2000, 35, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Tang, S.C.; Yu, X.; Chen, H.C.; Kashihara, N.; Park, H.C.; Liew, A.; Goh, B.L.; Nazareth, M.G.C.; Bunnag, S.; Tan, J.; et al. Dialysis Care and Dialysis Funding in Asia. Am. J. Kidney Dis. 2020, 75, 772–781. [Google Scholar] [CrossRef]
- Karopadi, A.N.; Mason, G.; Rettore, E.; Ronco, C. Cost of peritoneal dialysis and haemodialysis across the world. Nephrol. Dial. Transplant. 2013, 28, 2553–2569. [Google Scholar] [CrossRef] [Green Version]
- Manera, K.E.; Johnson, D.W.; Craig, J.C.; Shen, J.I.; Gutman, T.; Cho, Y.; Wang, A.Y.-M.; Brown, E.A.; Brunier, G.; Dong, J.; et al. Establishing a Core Outcome Set for Peritoneal Dialysis: Report of the SONG-PD (Standardized Outcomes in Nephrology–Peritoneal Dialysis) Consensus Workshop. Am. J. Kidney Dis. 2020, 75, 404–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UK Renal Registry. UK Renal Registry 23rd Annual Report—Data to 31/12/2019, Bristol, UK. 2021. Available online: https://ukkidney.org/audit-research/annual-report (accessed on 25 January 2023).
- de Crespigny, P.J.C.; Cai, M.X.; Holt, S.G. Providing a PD Service. In Primer on Nephrology; Harber, M., Ed.; Springer: Cham, Switzerland, 2022; pp. 1385–1408. [Google Scholar] [CrossRef]
- Shen, J.I.; Schreiber, M.J.; Zhao, J.; Robinson, B.M.; Pisoni, R.L.; Mehrotra, R.; Oliver, M.J.; Tomo, T.; Tungsanga, K.; Teitelbaum, I.; et al. Attitudes toward Peritoneal Dialysis among Peritoneal Dialysis and Hemodialysis Medical Directors. Clin. J. Am. Soc. Nephrol. 2019, 14, 1067–1070. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.J.; Garg, A.X.; Blake, P.G.; Johnson, J.F.; Verrelli, M.; Zacharias, J.M.; Pandeya, S.; Quinn, R.R. Impact of contraindications, barriers to self-care and support on incident peritoneal dialysis utilization. Nephrol. Dial. Transplant. 2010, 25, 2737–2744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, S.J. Peritoneal dialysis—Current status and future challenges. Nat. Rev. Nephrol. 2013, 9, 399–408. [Google Scholar] [CrossRef]
- Crabtree, J.H.; Shrestha, B.M.; Chow, K.-M.; Figueiredo, A.E.; Povlsen, J.V.; Wilkie, M.; Abdel-Aal, A.; Cullis, B.; Goh, B.-L.; Briggs, V.R.; et al. Creating and Maintaining Optimal Peritoneal Dialysis Access in the Adult Patient: 2019 Update. Perit. Dial. Int. 2019, 39, 414–436. [Google Scholar] [CrossRef] [Green Version]
- Blake, P.G.; Jain, A.K. Urgent Start Peritoneal Dialysis. Clin. J. Am. Soc. Nephrol. 2018, 13, 1278–1279. [Google Scholar] [CrossRef] [Green Version]
- NHS Blood and Transplant. Activity Report 2021-Section 5-Kidney Activity. Available online: https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/27118/section-5-kidney-activity.pdf (accessed on 25 January 2023).
- Li, P.K.-T.; Chow, K.M. Peritoneal dialysis–first policy made successful: Perspectives and actions. Am. J. Kidney Dis. 2013, 62, 993–1005. [Google Scholar] [CrossRef]
- Reeves, S.; Pelone, F.; Harrison, R.; Goldman, J.; Zwarenstein, M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2017, 2018, CD000072. [Google Scholar] [CrossRef]
- Available online: https://www.gmc-uk.org/-/media/documents/renal-medicine-2022-curriculum-final-v1_0_pdf-92050078.pdf (accessed on 27 January 2023).
- Jha, V.; Abrahams, A.C.; Al-Hwiesh, A.; Brown, E.A.; Cullis, B.; Dor, F.J.M.F.; Mendu, M.; Ponce, D.; Divino-Filho, J.C. Peritoneal catheter insertion: Combating barriers through policy change. Clin. Kidney J. 2022, 15, 2177–2185. [Google Scholar] [CrossRef]
- Goh, B.L.; Yudisthra, M.G.; Lim, T.O. Establishing learning curve for tenckhoff catheter insertion by interventional nephrologist using CUSUM analysis: How many procedures and in which situation? Semin. Dial. 2009, 22, 199–203. [Google Scholar] [CrossRef]
- Fraher, E.; Brandt, B. Toward a system where workforce planning and interprofessional practice and education are designed around patients and populations not professions. J. Interprof. Care 2019, 33, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Nimako, K.; Kruk, M.E. Seizing the moment to rethink health systems. Lancet Glob. Health 2021, 9, e1758–e1762. [Google Scholar] [CrossRef] [PubMed]
- Ballini, L.; Negro, A.; Maltoni, S.; Vignatelli, L.; Flodgren, G.; Simera, I.; Holmes, J.; Grilli, R. Interventions to reduce waiting times for elective procedures. Cochrane Database Syst. Rev. 2015, 2, CD005610. [Google Scholar] [CrossRef]
- Chao, C.-T.; Huang, J.-W.; Yen, C.-J. Intradialytic hypotension and cardiac remodeling: A vicious cycle. BioMed Res. Int. 2015, 2015, 724147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, E.A.; Hurst, H. Delivering peritoneal dialysis for the multimorbid, frail and palliative patient. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2020, 40, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Brown, E.A.; Ryan, L.; Corbett, R.W. A novel programme of supportive two-exchange assisted continuous ambulatory peritoneal dialysis for frail patients with end-stage kidney disease. Perit. Dial. Int. 2022, 43, 100–103. [Google Scholar] [CrossRef]
- Mohamed, A.; Bennett, M.; Gomez, L.; Massingill, E.; Le, L.; Peden, E.; Bechara, C.F. Laparoscopic Peritoneal Dialysis Surgery is Safe and Effective in Patients with Prior Abdominal Surgery. Ann. Vasc. Surg. 2018, 53, 133–138. [Google Scholar] [CrossRef]
- Agarwal, A.; Whitlock, R.H.; Bamforth, R.J.; Ferguson, T.W.; Sabourin, J.M.; Hu, Q.; Armstrong, S.; Rigatto, C.; Tangri, N.; Dunsmore, S.; et al. Percutaneous Versus Surgical Insertion of Peritoneal Dialysis Catheters: A Systematic Review and Meta-Analysis. Can. J. Kidney Health Dis. 2021, 8, 20543581211052731. [Google Scholar] [CrossRef]
- Tullavardhana, T.; Akranurakkul, P.; Ungkitphaiboon, W.; Songtish, D. Surgical versus percutaneous techniques for peritoneal dialysis catheter placement: A meta-analysis of the outcomes. Ann. Med. Surg. 2016, 10, 11–18. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, M.J.; Ye, B.-M.; Kim, J.H.; Kim, S.; Kim, I.Y.; Kim, H.J.; Han, M.; Rhee, H.; Song, S.H.; et al. Percutaneous peritoneal dialysis catheter implantation with no break-in period: A viable option for patients requiring unplanned urgent-start peritoneal dialysis. Kidney Res. Clin. Pract. 2020, 39, 365–372. [Google Scholar] [CrossRef]
- Wang, J.; Zeng, J.; Liu, B.; Cai, B.; Li, Y.; Dong, L. Outcomes after transfer from hemodialysis to peritoneal dialysis vs peritoneal dialysis as initial therapy: A systematic review and meta-analysis. Semin. Dial. 2020, 33, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, H.; Nunes, A.T.; Oliveira, A.; Beco, A.; Santos, J.; Pestana, M. Planning Vascular Access in Peritoneal Dialysis—Defining High-Risk Patients. Perit. Dial. Int. 2018, 38, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Bergström, S.; McPake, B.; Pereira, C.; Dovlo, D. Workforce Innovations to Expand the Capacity for Surgical Services. In Essential Surgery: Disease Control Priorities, 3rd ed.; Chapter 17; Debas, H.T., Donkor, P., Gawande, A., Jamison, D.T., Kruk, M.E., Mock, C.N., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2015; Volume 1. [Google Scholar]
- Schreiber, M.J.; Chatoth, D.K.; Salenger, P. Challenges and Opportunities in Expanding Home Hemodialysis for 2025. Adv. Chronic Kidney Dis. 2021, 28, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Wallace, E.L.; Jain, G. Setting Up and Expanding a Home Dialysis Program: Is There a Recipe for Success? Kidney 2020, 1, 569–579. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Median (Range) or n (%) |
|---|---|
| Age | 67 (18–88) |
| Sex | |
| Female | 23 (35%) |
| Male | 43 (65%) |
| BMI | 26 (19–43) |
| Primary renal disease | |
| Diabetic nephropathy | 20 (30%) |
| IgA nephropathy | 5 (8%) |
| Polycystic kidney disease | 4 (6%) |
| Focal segmental glomerulosclerosis | 3 (5%) |
| Other (including unknown) | 34 (52%) |
| Pre-procedure glomerular filtration rate | 10 (5–15) |
| Switching from haemodialysis | 11 (17%) |
| Outcome | n (%) |
|---|---|
| Completed 1-year follow-up on Peritoneal Dialysis | 36 (55%) |
| Transplanted | 14 (21%) |
| Died * | 7 (11%) |
| Switch to Haemodialysis ** | 9 (14%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corr, M.; Hunter, C.; Conroy, D.; McGrogan, D.; Fogarty, D.; O’Neill, S. A Service Reconfiguration Bundle for Expanding Access to Peritoneal Dialysis Including for Older Frailer Patients. Healthcare 2023, 11, 1654. https://doi.org/10.3390/healthcare11111654
Corr M, Hunter C, Conroy D, McGrogan D, Fogarty D, O’Neill S. A Service Reconfiguration Bundle for Expanding Access to Peritoneal Dialysis Including for Older Frailer Patients. Healthcare. 2023; 11(11):1654. https://doi.org/10.3390/healthcare11111654
Chicago/Turabian StyleCorr, Michael, Carolyn Hunter, Daniel Conroy, Damian McGrogan, Damian Fogarty, and Stephen O’Neill. 2023. "A Service Reconfiguration Bundle for Expanding Access to Peritoneal Dialysis Including for Older Frailer Patients" Healthcare 11, no. 11: 1654. https://doi.org/10.3390/healthcare11111654