

Assessment of Functional Capacity in Patients with Nondialysis-Dependent Chronic Kidney Disease with the Glittre Activities of Daily Living Test
 ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
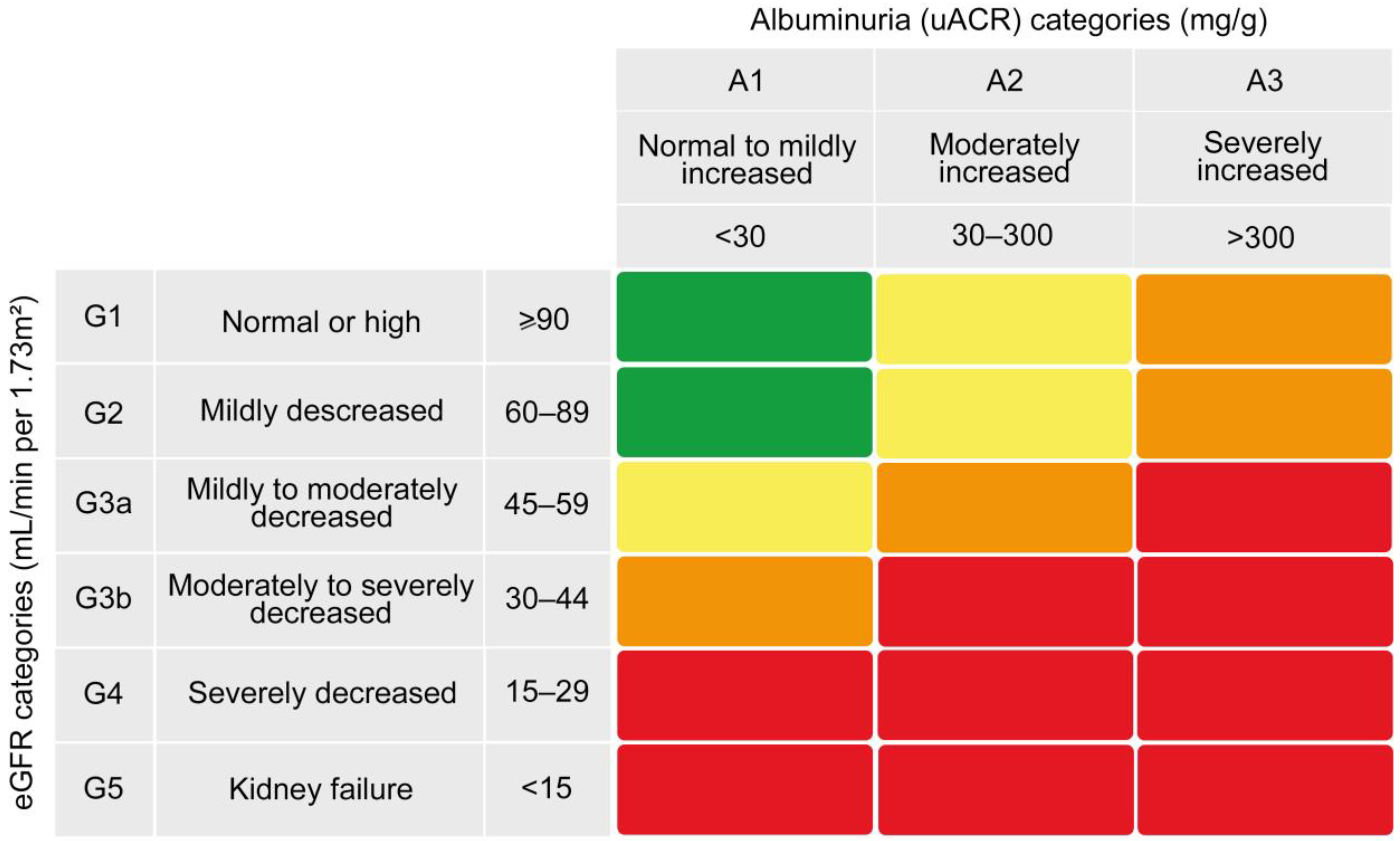
2.2. Chronic Kidney Disease Risk Categories
2.3. Assessment of Physical Activity Level
2.4. Assessment of Health-Related Quality of Life
2.5. Assessment of Handgrip Strength
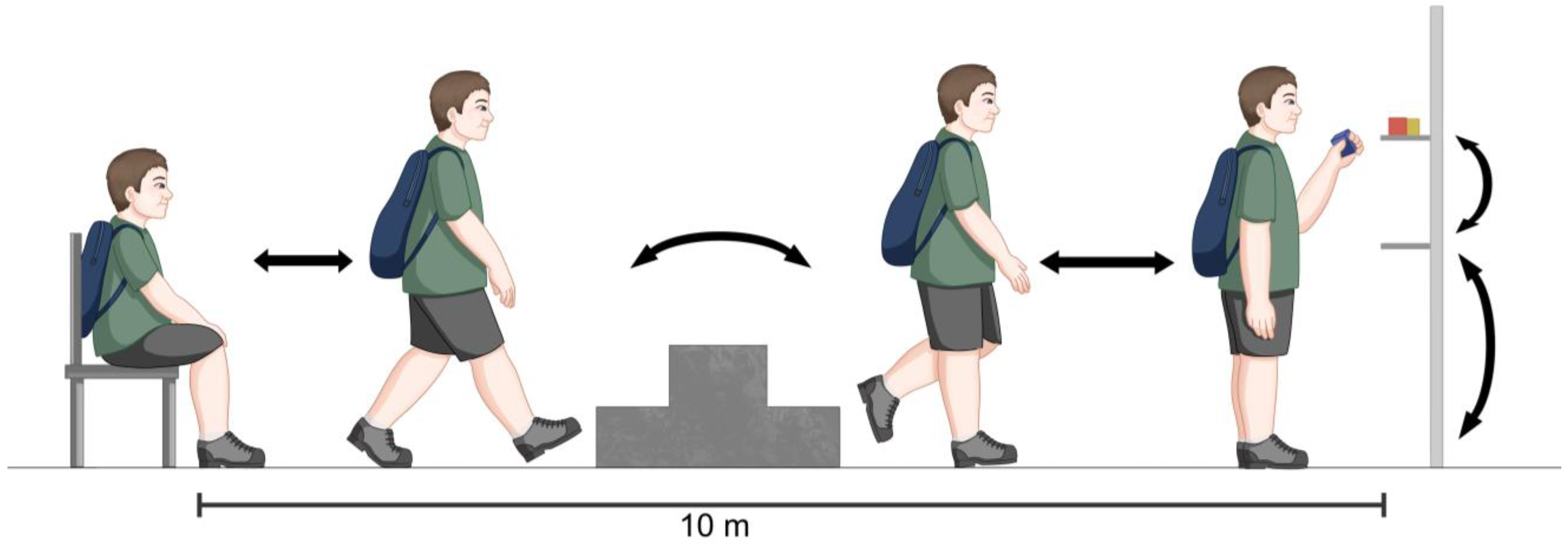
2.6. Assessment of Functional Capacity
2.7. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evans, M.; Lewis, R.D.; Morgan, A.R.; Whyte, M.B.; Hanif, W.; Bain, S.C.; Davies, S.; Dashora, U.; Yousef, Z.; Patel, D.C.; et al. A Narrative Review of Chronic Kidney Disease in Clinical Practice: Current Challenges and Future Perspectives. Adv. Ther. 2021, 39, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aucella, F.; Battaglia, Y.; Bellizzi, V.; Bolignano, D.; Capitanini, A.; Cupisti, A. Physical excercise programs in CKD: Lights, shades and perspectives: A position paper of the “Physical Exercise in CKD Study Group” of the Italian Society of Nephrology. J. Nephrol. 2015, 28, 143–150. [Google Scholar] [CrossRef] [PubMed]
- da Silva, K.B.; Leal, D.V.; da Rocha, J.L.; Ballico, A.L.; Haupenthal, A.; Viana, J.L.; Bündchen, D.C. Glittre activities of daily living test is reliable and valid in hemodialysis patients. Disabil. Rehabil. 2022, 1–7. [Google Scholar] [CrossRef]
- Leal, D.V.; Ferreira, A.; Watson, E.L.; Wilund, K.R.; Viana, J.L. Muscle-Bone Crosstalk in Chronic Kidney Disease: The Potential Modulatory Effects of Exercise. Calcif. Tissue. Int. 2021, 108, 461–475. [Google Scholar] [CrossRef]
- Costa, M.J.C.; Cavalcanti, F.C.B.; Bezerra, S.D.; Filho, J.C.d.A.; Fernandes, J.; Marinho, P.E.M. Relationship between quadriceps thickness and 60-second sit-to-stand test in patients with chronic kidney disease. Braz. J. Nephrol. 2022, 44, 164–170. [Google Scholar] [CrossRef]
- Sabatino, A.; Cuppari, L.; Stenvinkel, P.; Lindholm, B.; Avesani, C.M. Sarcopenia in chronic kidney disease: What have we learned so far? J. Nephrol. 2020, 34, 1347–1372. [Google Scholar] [CrossRef]
- Mariani, H.R.; Andrade, T.A.C.; Cruz, A.D.F.C.; Oliveira, P.C.D.S.; Christofoletti, G.; Seki, K.L.M. Evaluation of the functional capacity of patients with chronic kidney disease using the ADL-Glittre test. 2019, 43, 870–883. [Google Scholar] [CrossRef]
- Figueiredo, P.H.S.; da Silva, A.C.R.; Costa, H.S.; Nominato, G.A.; Lopes, P.H.; Campos, P.; Santos, L.M.D.M.; Alcântara, M.A.; Alves, F.L.; Rodrigues, V.G.B.; et al. The Glittre activities of daily living as a potential test for functional evaluation of patients on hemodialysis: A validation study. Disabil. Rehabil. 2020, 44, 2083–2090. [Google Scholar] [CrossRef]
- Segura-Ortí, E.; Gordon, P.L.; Doyle, J.W.; Johansen, K.L. Correlates of Physical Functioning and Performance Across the Spectrum of Kidney Function. Clin. Nurs. Res. 2017, 27, 579–596. [Google Scholar] [CrossRef]
- Verberne, W.R.; Wittenboer, I.D.V.D.; Voorend, C.G.N.; Abrahams, A.C.; van Buren, M.; Dekker, F.W.; van Jaarsveld, B.C.; van Loon, I.N.; Mooijaart, S.P.; Ocak, G.; et al. Health-related quality of life and symptoms of conservative care versus dialysis in patients with end-stage kidney disease: A systematic review. Nephrol. Dial. Transplant. 2020, 36, 1418–1433. [Google Scholar] [CrossRef] [PubMed]
- KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Available online: https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf (accessed on 10 December 2022).
- Murton, M.; Goff-Leggett, D.; Bobrowska, A.; Sanchez, J.J.G.; James, G.; Wittbrodt, E.; Nolan, S.; Sörstadius, E.; Pecoits-Filho, R.; Tuttle, K. Burden of Chronic Kidney Disease by KDIGO Categories of Glomerular Filtration Rate and Albuminuria: A Systematic Review. Adv. Ther. 2020, 38, 180–200. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C–Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nonato, C.P.; Azevedo, B.L.P.A.; Oliveira, J.G.M.; Gardel, D.; de Souza, D.C.N.; Lopes, A.J. The Glittre Activities of Daily Living Test in women with scleroderma and its relation to hand function and physical capacity. Clin. Biomech. 2020, 73, 71–77. [Google Scholar] [CrossRef]
- Neves, R.S.; Lopes, A.J.; De Menezes, S.L.S.; Lima, T.R.D.L.; Ferreira, A.D.S.; Guimarães, F.S. Hand grip strength in healthy young and older Brazilian adults: Development of line development of a linear prediction model using simple anthropometric variable. Kinesiology 2017, 49, 208–216. [Google Scholar] [CrossRef] [Green Version]
- Novaes, R.D.; De Miranda, A.S.; Silva, J.D.O.; Tavares, B.V.F.; Dourado, V.Z. Equações de referência para a predição da força de preensão manual em brasileiros de meia idade e idosos. Fisioter. E Pesqui. 2009, 16, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Skumlien, S.; Hagelund, T.; Bjørtuft, O.; Ryg, S.M. A field test of functional status as performance of activities of daily living in COPD patients. Respir. Med. 2006, 100, 316–323. [Google Scholar] [CrossRef] [Green Version]
- de Alegria, S.G.; Kasuki, L.; Gadelha, M.; Lopes, A.J. The Glittre Activities of Daily Living Test in patients with acromegaly: Associations with hand function and health-related quality of life. J. Back Musculoskelet. Rehabil. 2021, 34, 441–451. [Google Scholar] [CrossRef]
- Dos Reis, C.M.; Karloh, M.; Fonseca, F.R.; Biscaro, R.R.M.; Mazo, G.Z.; Mayer, A.F. Functional capacity measurement: Reference equations for the Glittre Activities of Daily Living test. J. Bras. Pneumol. 2018, 44, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Lima, T.R.L.; Almeida, V.P.; Ferreira, A.S.; Guimarães, F.S.; Lopes, A.J. Handgrip Strength and Pulmonary Disease in the Elderly: What is the Link? Aging Dis. 2019, 10, 1109–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glavinovic, T.; Ferguson, T.; Komenda, P.; Rigatto, C.; Duhamel, T.; Tangri, N.; Bohm, C. CKD and Sedentary Time: Results From the Canadian Health Measures Survey. Am. J. Kidney Dis. 2018, 72, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.A.; Cordeiro, A.C.; Avesani, C.M.; Carrero, J.J.; Lindholm, B.; Amparo, F.C.; Amodeo, C.; Cuppari, L.; Kamimura, M.A. Sarcopenia in chronic kidney disease on conservative therapy: Prevalence and association with mortality. Nephrol. Dial. Transplant. 2015, 30, 1718–1725. [Google Scholar] [CrossRef] [Green Version]
- Montenegro, J.; Klein, M.R.S.T.; Bregman, R.; Prado, C.M.; Silva, M.I.B. Osteosarcopenia in patients with non-dialysis dependent chronic kidney disease. Clin. Nutr. 2022, 41, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Kaltsatou, A.; Sakkas, G.K.; Poulianiti, K.P.; Koutedakis, Y.; Tepetes, K.; Christodoulidis, G.; Stefanidis, I.; Karatzaferi, C. Uremic myopathy: Is oxidative stress implicated in muscle dysfunction in uremia? Front. Physiol. 2015, 6, 102. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Milton, J.; Hsu, F.-C.; Beavers, K.; Yank, V.; Church, T.; Shegog, J.; Kashaf, S.; Nayfield, S.; Newman, A.; et al. The Effect of Chronic Kidney Disease on a Physical Activity Intervention: Impact on Physical Function, Adherence, and Safety. J. Clin. Nephrol. Ren. Care 2016, 3, 21. [Google Scholar] [CrossRef]
- Hussien, H.; Apetrii, M.; Covic, A. Health-related quality of life in patients with chronic kidney disease. Expert Rev. Pharm. Outcomes Res. 2020, 21, 43–54. [Google Scholar] [CrossRef]
- Krishnan, P. A review of the non-equivalent control group post-test-only design. Nurse Res. 2019, 26, 37–40. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Values |
|---|---|
| Anthropometry | |
| Male/female | 19/11 |
| Age (years) | 58.1 ± 13.9 |
| Weight (kg) | 69.5 ± 10.6 |
| Height (m) | 1.63 ± 0.08 |
| BMI (kg/m2) | 26.2 ± 3.8 |
| Comorbidities, n (%) | |
| Hypertension | 23 (76.7) |
| Diabetes | 12 (40) |
| Chronic heart disease | 8 (26.7) |
| Chronic glomerulopathy | 5 (16.7) |
| Chronic vascular disease | 5 (16.7) |
| Renal function | |
| eGFR (mL/min) | 39.9 ± 22 |
| uACR (mg/g) | 489.3 ± 78.2 |
| Risk of disease progression, n (%) | |
| Low/moderate | 7 (23.3) |
| High | 9 (30) |
| Very high | 14 (46.7) |
| SF-36 | |
| Physical functioning (score) | 80 (54–95) |
| Physical role limitations (score) | 50 (19–100) |
| Bodily pain (score) | 62 (41–100) |
| General health perceptions (score) | 60 (42–67) |
| Vitality (score) | 68 (55–90) |
| Social functioning (score) | 81 (50–100) |
| Emotional role limitations (score) | 100 (0–100) |
| Mental health (score) | 76 (60–92) |
| Variable | Values |
|---|---|
| IPAQ stages, n (%) | |
| Sedentary | 13 (43.3) |
| Irregularly active | 10 (33.3) |
| Active | 7 (23.3) |
| Muscle function | |
| HGS (kgf) | 29 (26–41) |
| Glittre-ADL test | |
| Time (min) | 4.3 (3.3–5.2) |
| Time (% predicted) | 143.3 ± 32.7 |
| Highest-difficulty task, n (%) | |
| No difficulty | 16 (53.3) |
| Squatting to perform shelving tasks | 6 (20) |
| Manual tasks | 5 (16.7) |
| Stair tasks | 3 (10) |
| Variable | Time (% Predicted) | |
|---|---|---|
| r | p-value | |
| Age | 0.296 | 0.11 |
| Weight | −0.224 | 0.23 |
| Height | 0.254 | 0.17 |
| BMI | −0.075 | 0.69 |
| rs | p-value | |
| Physical functioning | −0.217 | 0.25 |
| Physical role limitations | −0.246 | 0.19 |
| Bodily pain | −0.219 | 0.25 |
| General health perceptions | 0.183 | 0.33 |
| Vitality | −0.098 | 0.61 |
| Social functioning | −0.098 | 0.61 |
| Emotional role limitations | −0.228 | 0.23 |
| Mental health | −0.074 | 0.70 |
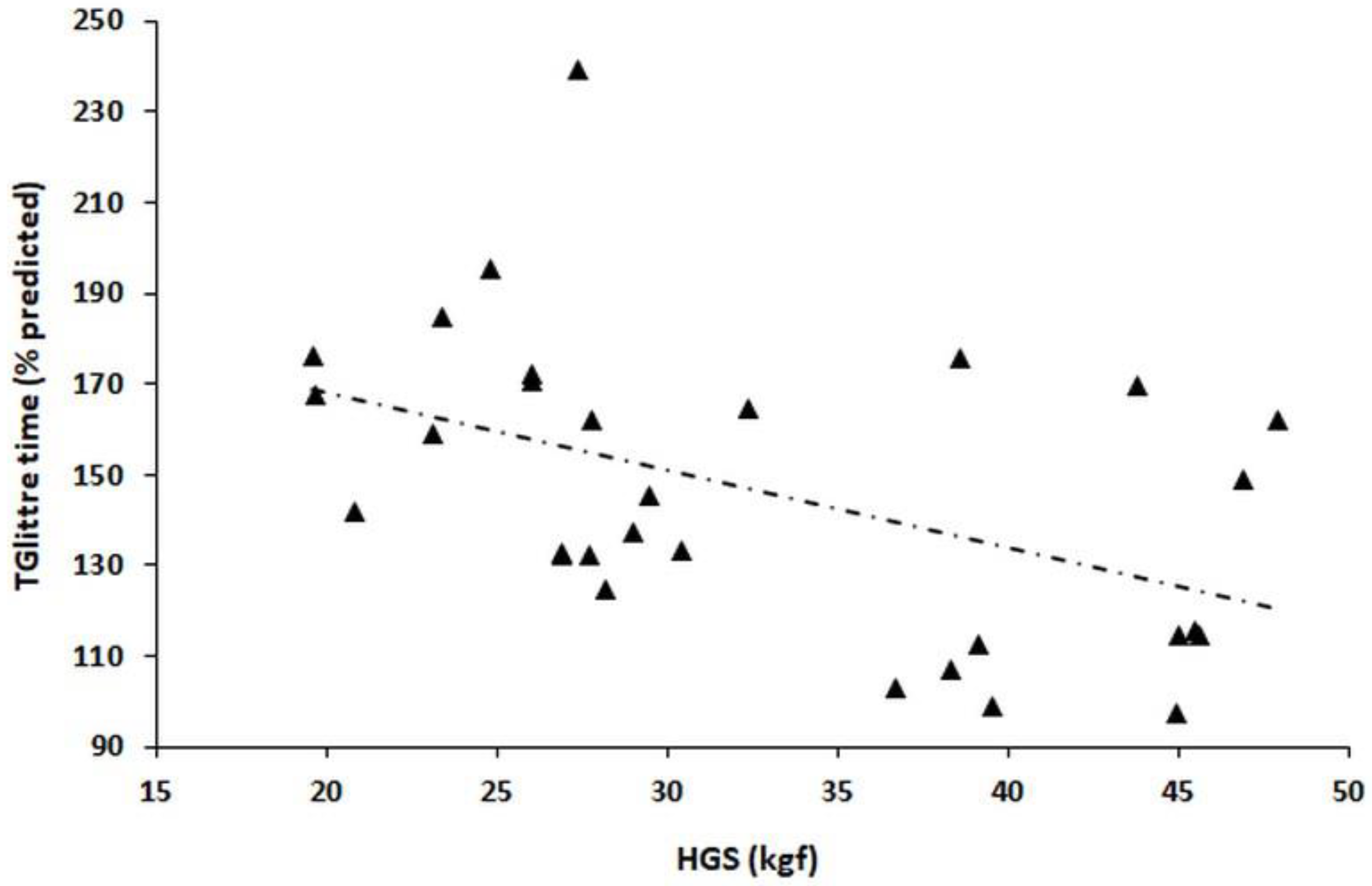
| HGS | −0.513 | 0.003 |
| Variable | Time (% Predicted) | p-Value |
|---|---|---|
| Gender | ||
| Male | 142 ± 38 | 0.36 * |
| Female | 154 ± 21 | |
| Hypertension | ||
| Yes | 148 ± 28 | 0.62 * |
| No | 141 ± 48 | |
| Diabetes | ||
| Yes | 147 ± 27 | 0.98 * |
| No | 146 ± 37 | |
| Chronic heart disease | ||
| Yes | 157 ± 24 | 0.31 * |
| No | 143 ± 35 | |
| Glomerulopathy | ||
| Yes | 138 ± 31 | 0.53 * |
| No | 148 ± 33 | |
| Chronic vascular disease | ||
| Yes | 141 ± 34 | 0.71 * |
| No | 147 ± 33 | |
| Risk of disease progression | ||
| Low/moderate | 147 ± 48 | 0.69 # |
| High | 139 ± 28 | |
| Very high | 151 ± 28 | |
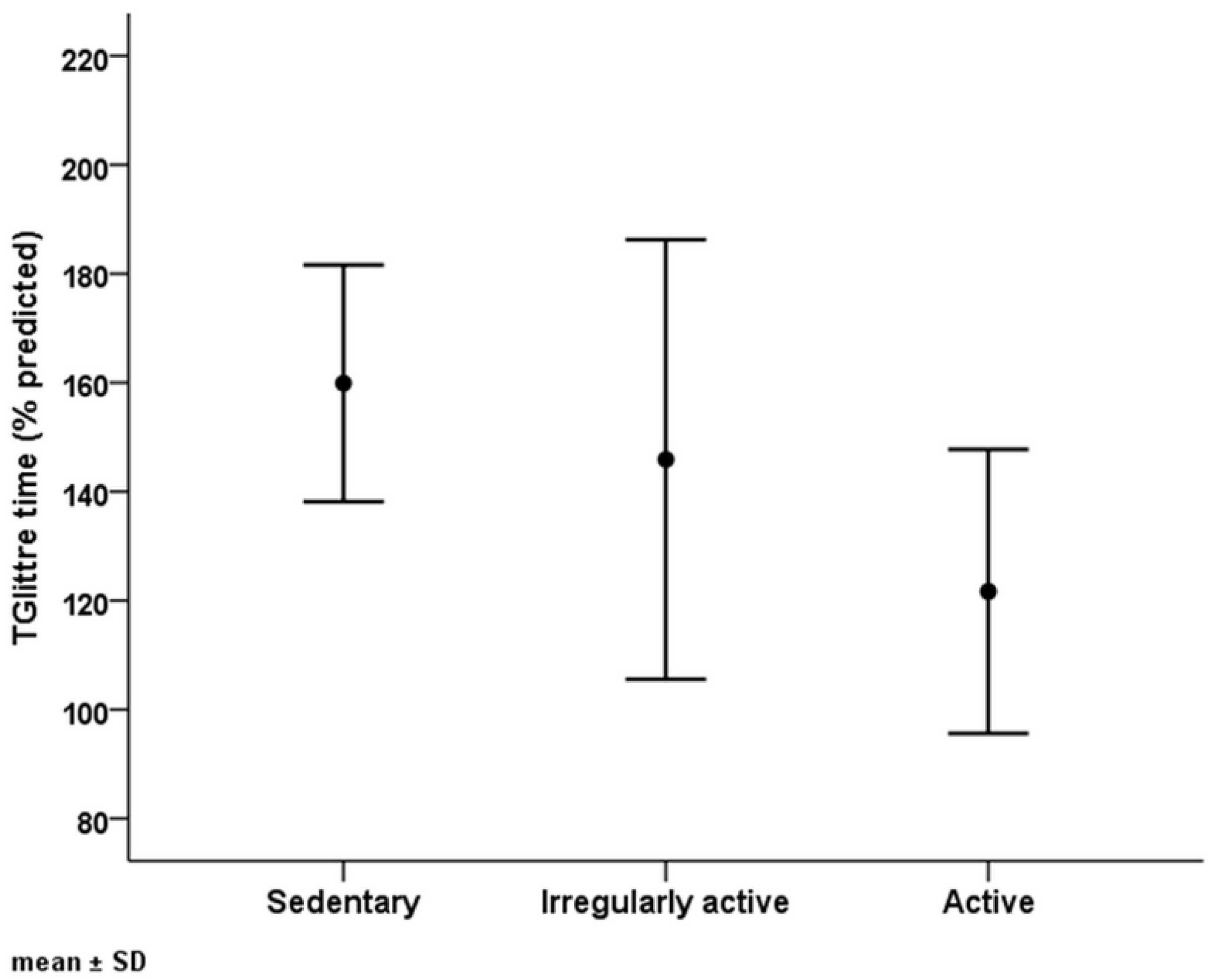
| IPAQ stages | ||
| Sedentary | 160 ± 22 | 0.038 # |
| Irregularly active | 146 ± 40 | |
| Active | 122 ± 26 |
| Independent Variable | Coefficient | Standard Error | p-Value |
|---|---|---|---|
| HGS | −1.367 | 0.477 | 0.004 |
| IPAQ stages | |||
| Sedentary | Reference | ||
| Irregularly active | −15.9 | 12 | 0.18 |
| Active | −28.1 | 11.5 | 0.014 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balata, M.R.; Ferreira, A.S.; da Silva Sousa, A.; Meinertz, L.F.; de Sá, L.M.; Araujo, V.G.; Papathanasiou, J.; Lopes, A.J. Assessment of Functional Capacity in Patients with Nondialysis-Dependent Chronic Kidney Disease with the Glittre Activities of Daily Living Test. Healthcare 2023, 11, 1809. https://doi.org/10.3390/healthcare11121809
Balata MR, Ferreira AS, da Silva Sousa A, Meinertz LF, de Sá LM, Araujo VG, Papathanasiou J, Lopes AJ. Assessment of Functional Capacity in Patients with Nondialysis-Dependent Chronic Kidney Disease with the Glittre Activities of Daily Living Test. Healthcare. 2023; 11(12):1809. https://doi.org/10.3390/healthcare11121809
Chicago/Turabian StyleBalata, Mauro Ribeiro, Arthur Sá Ferreira, Ariane da Silva Sousa, Laura Felipe Meinertz, Luciana Milhomem de Sá, Vinicius Guterres Araujo, Jannis Papathanasiou, and Agnaldo José Lopes. 2023. "Assessment of Functional Capacity in Patients with Nondialysis-Dependent Chronic Kidney Disease with the Glittre Activities of Daily Living Test" Healthcare 11, no. 12: 1809. https://doi.org/10.3390/healthcare11121809