
Acupuncture Improves Sleep Disorders and Depression among Patients with Parkinson’s Disease: A Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction Process
2.4. Quality Assessment of the Included Studies
2.5. Statistical Analysis Methods
3. Results
3.1. Identification and Selection of Studies
3.2. Study Characteristics and Patient Populations
3.3. Quality Assessment of Included Studies and Adverse Events
3.4. The Primary Outcome of Acupuncture in Sleep Disorders Improvement
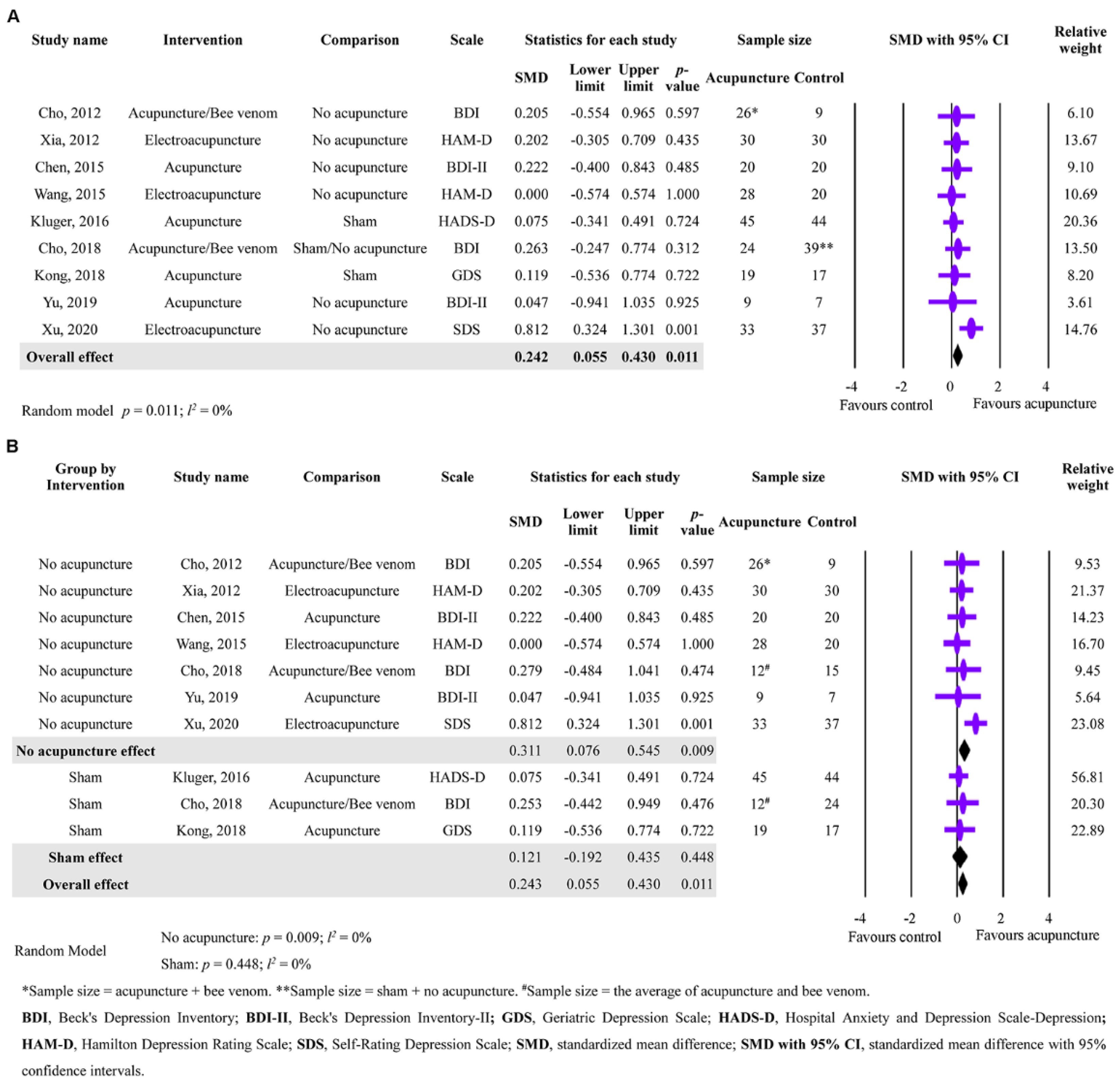
3.5. The Secondary Outcome of Acupuncture in Depression Improvement
3.6. The Secondary Outcomes of Acupuncture in Anxiety and Fatigue Improvement
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jankovic, J.; Tan, E.K. Parkinson’s disease: Etiopathogenesis and treatment. J. Neurol. Neurosurg. Psychiatry 2020, 91, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Kalia, L.V.; Lang, A.E. Parkinson’s disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef] [PubMed]
- Prasad, E.M.; Hung, S.Y. Current Therapies in Clinical Trials of Parkinson’s Disease: A 2021 Update. Pharmaceuticals 2021, 14, 717. [Google Scholar] [CrossRef]
- Schapira, A.H.V.; Chaudhuri, K.R.; Jenner, P. Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Ma, T. Effects of Acupuncture on Neurological Disease in Clinical- and Animal-Based Research. Front. Integr. Neurosci. 2019, 13, 47. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.G.; Chen, C.J.; Yang, H.B.; Chen, Y.H.; Hung, S.Y. Electroacupuncture Promotes Recovery of Motor Function and Reduces Dopaminergic Neuron Degeneration in Rodent Models of Parkinson’s Disease. Int. J. Mol. Sci. 2017, 18, 1846. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.; Cui, Y.; Li, S.; Le, W. Current Pharmaceutical Treatments and Alternative Therapies of Parkinson’s Disease. Curr. Neuropharmacol. 2016, 14, 339–355. [Google Scholar] [CrossRef]
- Cho, S.Y.; Shim, S.R.; Rhee, H.Y.; Park, H.J.; Jung, W.S.; Moon, S.K.; Park, J.M.; Ko, C.N.; Cho, K.H.; Park, S.U. Effectiveness of acupuncture and bee venom acupuncture in idiopathic Parkinson’s disease. Park. Relat. Disord. 2012, 18, 948–952. [Google Scholar] [CrossRef]
- Toosizadeh, N.; Lei, H.; Schwenk, M.; Sherman, S.J.; Sternberg, E.; Mohler, J.; Najafi, B. Does integrative medicine enhance balance in aging adults? Proof of concept for the benefit of electroacupuncture therapy in Parkinson’s disease. Gerontology 2015, 61, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Lei, H.; Toosizadeh, N.; Schwenk, M.; Sherman, S.; Karp, S.; Sternberg, E.; Najafi, B. A Pilot Clinical Trial to Objectively Assess the Efficacy of Electroacupuncture on Gait in Patients with Parkinson’s Disease Using Body Worn Sensors. PLoS ONE 2016, 11, e0155613. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Xu, S.; Wang, R.; Zou, X.; Liu, H.; Fan, C.; Li, J.; Li, G.; Wu, Y.; Ma, X.; et al. Electroacupuncture for motor dysfunction and constipation in patients with Parkinson’s disease: A randomised controlled multi-centre trial. EClinicalMedicine 2023, 56, 101814. [Google Scholar] [CrossRef]
- Chae, Y.; Lee, H.; Kim, H.; Kim, C.H.; Chang, D.I.; Kim, K.M.; Park, H.J. Parsing brain activity associated with acupuncture treatment in Parkinson’s diseases. Mov. Disord. 2009, 24, 1794–1802. [Google Scholar] [CrossRef]
- Hsu, W.T.; Chen, Y.H.; Yang, H.B.; Lin, J.G.; Hung, S.Y. Electroacupuncture Improves Motor Symptoms of Parkinson’s Disease and Promotes Neuronal Autophagy Activity in Mouse Brain. Am. J. Chin. Med. 2020, 48, 1651–1669. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Blazquez, C.; Schrag, A.; Rizos, A.; Chaudhuri, K.R.; Martinez-Martin, P.; Weintraub, D. Prevalence of Non-Motor Symptoms and Non-Motor Fluctuations in Parkinson’s Disease Using the MDS-NMS. Mov. Disord. Clin. Pract. 2021, 8, 231–239. [Google Scholar] [CrossRef]
- Schutz, L.; Sixel-Doring, F.; Hermann, W. Management of Sleep Disturbances in Parkinson’s Disease. J. Parkinsons Dis. 2022, 12, 2029–2058. [Google Scholar] [CrossRef]
- Reijnders, J.S.; Ehrt, U.; Weber, W.E.; Aarsland, D.; Leentjens, A.F. A systematic review of prevalence studies of depression in Parkinson’s disease. Mov. Disord. 2008, 23, 183–189, quiz 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broen, M.P.; Narayen, N.E.; Kuijf, M.L.; Dissanayaka, N.N.; Leentjens, A.F. Prevalence of anxiety in Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2016, 31, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Niimi, Y.; Shima, S.; Mizutani, Y.; Ueda, A.; Ito, S.; Mutoh, T. Fatigue evaluated using the 16-item Parkinson Fatigue Scale (PFS-16) predicts Parkinson’s disease prognosis. Fujita Med. J. 2019, 5, 45–48. [Google Scholar] [CrossRef]
- Li, L.; Jin, X.; Cong, W.; Du, T.; Zhang, W. Acupuncture in the Treatment of Parkinson’s Disease with Sleep Disorders and Dose Response. Biomed. Res. Int. 2022, 2022, 7403627. [Google Scholar] [CrossRef] [PubMed]
- Kluger, B.M.; Rakowski, D.; Christian, M.; Cedar, D.; Wong, B.; Crawford, J.; Uveges, K.; Berk, J.; Abaca, E.; Corbin, L.; et al. Randomized, Controlled Trial of Acupuncture for Fatigue in Parkinson’s Disease. Mov. Disord. 2016, 31, 1027–1032. [Google Scholar] [CrossRef]
- Li, Q.; Wu, C.; Wang, X.; Li, Z.; Hao, X.; Zhao, L.; Li, M.; Zhu, M. Effect of acupuncture for non-motor symptoms in patients with Parkinson’s disease: A systematic review and meta-analysis. Front. Aging Neurosci. 2022, 14, 995850. [Google Scholar] [CrossRef]
- Fan, J.Q.; Lu, W.J.; Tan, W.Q.; Liu, X.; Wang, Y.T.; Wang, N.B.; Zhuang, L.X. Effectiveness of Acupuncture for Anxiety Among Patients with Parkinson Disease: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2232133. [Google Scholar] [CrossRef]
- Kong, K.H.; Ng, H.L.; Li, W.; Ng, D.W.; Tan, S.I.; Tay, K.Y.; Au, W.L.; Tan, L.C.S. Acupuncture in the treatment of fatigue in Parkinson’s disease: A pilot, randomized, controlled, study. Brain Behav. 2018, 8, e00897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2020. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Oremus, M.; Wolfson, C.; Perrault, A.; Demers, L.; Momoli, F.; Moride, Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement. Geriatr. Cogn. Disord. 2001, 12, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Wang, H.D.; Ding, Y.; Kang, B.; Liu, W.G. Parkinson’s disease combined with depression treated with electroacupuncture and medication and its effect on serum BDNF. Zhongguo Zhen Jiu 2012, 32, 1071–1074. [Google Scholar]
- Chen, F.P.; Chang, C.M.; Shiu, J.H.; Chiu, J.H.; Wu, T.P.; Yang, J.L.; Kung, Y.Y.; Chen, F.J.; Chern, C.M.; Hwang, S.J. A clinical study of integrating acupuncture and Western medicine in treating patients with Parkinson’s disease. Am. J. Chin. Med. 2015, 43, 407–423. [Google Scholar] [CrossRef]
- Wang, F.; Sun, L.; Zhang, X.Z.; Jia, J.; Liu, Z.; Huang, X.Y.; Yu, S.Y.; Zuo, L.J.; Cao, C.J.; Wang, X.M.; et al. Effect and Potential Mechanism of Electroacupuncture Add-On Treatment in Patients with Parkinson’s Disease. Evid. Based Complement. Alternat. Med. 2015, 2015, 692795. [Google Scholar] [CrossRef] [Green Version]
- Aroxa, F.H.; Gondim, I.T.; Santos, E.L.; Coriolano, M.D.; Asano, A.G.; Asano, N.M. Acupuncture as Adjuvant Therapy for Sleep Disorders in Parkinson’s Disease. J. Acupunct. Meridian. Stud. 2017, 10, 33–38. [Google Scholar] [CrossRef]
- Cho, S.Y.; Lee, Y.E.; Doo, K.H.; Lee, J.H.; Jung, W.S.; Moon, S.K.; Park, J.M.; Ko, C.N.; Kim, H.; Rhee, H.Y.; et al. Efficacy of Combined Treatment with Acupuncture and Bee Venom Acupuncture as an Adjunctive Treatment for Parkinson’s Disease. J. Altern. Complement. Med. 2018, 24, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.W.; Lin, S.H.; Tsai, C.C.; Chaudhuri, K.R.; Huang, Y.C.; Chen, Y.S.; Yeh, B.Y.; Wu, Y.R.; Wang, J.J. Acupuncture Effect and Mechanism for Treating Pain in Patients with Parkinson’s Disease. Front. Neurol. 2019, 10, 1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Cai, X.; Qu, S.; Zhang, J.; Zhang, Z.; Yao, Z.; Huang, Y.; Zhong, Z. Madopar combined with acupuncture improves motor and non-motor symptoms in Parkinson’s disease patients: A multicenter randomized controlled trial. Eur. J. Integr. Med. 2020, 34, 101049. [Google Scholar] [CrossRef]
- Nazarova, L.; Liu, H.; Xie, H.; Wang, L.; Ding, H.; An, H.; Huang, D. Targeting gut-brain axis through scalp-abdominal electroacupuncture in Parkinson’s disease. Brain Res. 2022, 1790, 147956. [Google Scholar] [CrossRef]
- Goodarzi, Z.; Mrklas, K.J.; Roberts, D.J.; Jette, N.; Pringsheim, T.; Holroyd-Leduc, J. Detecting depression in Parkinson disease: A systematic review and meta-analysis. Neurology 2016, 87, 426–437. [Google Scholar] [CrossRef] [Green Version]
- Maniaci, A.; Ferlito, S.; Lechien, J.R.; Di Luca, M.; Iannella, G.; Cammaroto, G.; Cannavicci, A.; Pollicina, I.; Stilo, G.; Di Mauro, P.; et al. Anxiety, depression and sleepiness in OSA patients treated with barbed reposition pharyngoplasty: A prospective study. Eur. Arch. Otorhinolaryngol. 2022, 279, 4189–4198. [Google Scholar] [CrossRef]
- Maniaci, A.; Di Luca, M.; Lechien, J.R.; Iannella, G.; Grillo, C.; Grillo, C.M.; Merlino, F.; Calvo-Henriquez, C.; De Vito, A.; Magliulo, G.; et al. Lateral pharyngoplasty vs. traditional uvulopalatopharyngoplasty for patients with OSA: Systematic review and meta-analysis. Sleep Breath. 2022, 26, 1539–1550. [Google Scholar] [CrossRef] [PubMed]
- Marsh, L. Depression and Parkinson’s disease: Current knowledge. Curr. Neurol. Neurosci. Rep. 2013, 13, 409. [Google Scholar] [CrossRef] [Green Version]
- Siciliano, M.; Trojano, L.; Santangelo, G.; De Micco, R.; Tedeschi, G.; Tessitore, A. Fatigue in Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2018, 33, 1712–1723. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Design | Comparison | Subjects (N) | Age Mean ± SD | Diagnostic Criteria for Non-Motor Symptoms | Treatment Duration | Population |
|---|---|---|---|---|---|---|---|---|
| Cho et al., 2012 [8] | Korea | Randomized controlled trial | Acupuncture Bee venom No acupuncture | 13 13 9 | 55.0 (52.0, 66.0) * 57.0 (49.0, 69.0) * 57.0 (48.0, 68.0) * | BDI, PDQL | 8 weeks | Idiopathic PD |
| Xia et al., 2012 [28] | China | Randomized controlled trial | Electroacupuncture No acupuncture | 30 30 | 72 ± 7 72 ± 8 | HAM-D, BDNF | 3 months | PD with depression |
| Chen et al., 2015 [29] | Taiwan | Clinical trial | Acupuncture No acupuncture | 20 20 | 72.1 ± 8.5 75.4 ± 12.2 | BAI, BDI-II, WHOQOL | 18 weeks | PD |
| Wang et al., 2015 [30] | China | Randomized controlled trial | Electroacupuncture No acupuncture | 28 20 | 62.1 ± 8.7 59.1 ± 12.4 | NMSQ, MoCA, MMSE, HAM-D, HAM-A, PSQI, PDQ-39 | 2 months | PD |
| Kluger et al., 2016 [20] | USA | Randomized controlled trial | Acupuncture Sham | 45 44 | 64.4 ± 10.3 63.0 ± 13.0 | MFIS, PDSS, ESS, HADS-A, HADS-D, PDQ-39 | 6 weeks | PD |
| Aroxa et al., 2017 [31] | Brazil | Randomized controlled trial | Acupuncture No acupuncture | 11 11 | 65 ± 10 56 ± 12 | PDSS, MMSE | 8 weeks | Idiopathic PD |
| Cho et al., 2018 [32] | Korea | Randomized controlled trial | Acupuncture + Bee venom Sham Conventional treatment | 24 24 15 | 64.42 ± 8.24 61.33 ± 8.20 64.07 ± 6.33 | BDI, PDQL | 12 weeks | Idiopathic PD |
| Kong et al., 2018 [23] | Singapore | Randomized controlled trial | Acupuncture Sham | 19 17 | 66.4 ± 6.5 62.9 ± 9.7 | ESS, GDS, MFI-GF, PDQ-39 | 5 weeks | PD |
| Yu et al., 2019 [33] | Taiwan | Clinical trial | Acupuncture No acupuncture | 9 7 | 60.7 ± 6.3 70.4 ± 8.2 | PDSS-2, BDI-II, MMSE, KPPS, VAS, PDQ-39 | 8 weeks | Idiopathic PD |
| Xu et al., 2020 [34] | China | Randomized controlled trial | Electroacupuncture No acupuncture | 33 37 | 61.73 ± 10.28 61.95 ± 9.77 | PDSS, SDS | 8 weeks | PD |
| Fan et al., 2022 [22] | China | Randomized controlled trial | Acupuncture Sham | 32 32 | 61.03 ± 9.80 62.66 ± 6.94 | HAM-A, PDQ-39 | 8 weeks | Idiopathic PD |
| Li et al., 2022 [19] | China | Randomized controlled trial | Acupuncture Sham | 30 27 | 63 ± 6.73 59 ± 9.28 | PDSS-2, ESS | 30 days | PD |
| Nazarova et al., 2022 [35] | China | Randomized controlled trial | Electroacupuncture No acupuncture | 15 15 | 70.1 ± 6.2 66.9 ± 7.8 | PDSS, NMSS, BSFS, PAC-QOL | 8 weeks | PD |
| Study | Was the Study Described as Randomized? (Yes: 1; No: 0) | Was the Method of Randomization Appropriate? (Yes: 1; No: −1; Not Described: 0) | Was the Study Described as Blinding? (Yes: 1; No: 0) | Was the Method of Blinding Appropriate? (Yes: 1; No: −1; Not Described: 0) | Was There a Description of Withdrawals and Dropouts? (Yes: 1; No: 0) | Was There a Clear Description of the Inclusion and Exclusion Criteria? (Yes: 1; No: 0) | Was the Method Used to Assess Adverse Effects Described? (Yes: 1; No: 0) | Was the Methods of Statistical Analysis Described? (Yes: 1; No: 0) | Total Scores |
|---|---|---|---|---|---|---|---|---|---|
| Cho et al., 2012 [8] | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Xia et al., 2012 [28] | 1 | −1 | 0 | 0 | 1 | 1 | 0 | 1 | 3 |
| Chen et al., 2015 [29] | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 3 |
| Wang et al., 2015 [30] | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 4 |
| Kluger et al., 2016 [20] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Aroxa et al., 2017 [31] | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 4 |
| Cho et al., 2018 [32] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Kong et al., 2018 [23] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Yu et al., 2019 [33] | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 2 |
| Xu et al., 2020 [34] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Fan et al., 2022 [22] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Li et al., 2022 [19] | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 4 |
| Nazarova et al., 2022 [35] | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, W.-T.; Hsu, C.-M.; Hung, S.-C.; Hung, S.-Y. Acupuncture Improves Sleep Disorders and Depression among Patients with Parkinson’s Disease: A Meta-Analysis. Healthcare 2023, 11, 2042. https://doi.org/10.3390/healthcare11142042
Hsu W-T, Hsu C-M, Hung S-C, Hung S-Y. Acupuncture Improves Sleep Disorders and Depression among Patients with Parkinson’s Disease: A Meta-Analysis. Healthcare. 2023; 11(14):2042. https://doi.org/10.3390/healthcare11142042
Chicago/Turabian StyleHsu, Wei-Ti, Chieh-Min Hsu, Shao-Chi Hung, and Shih-Ya Hung. 2023. "Acupuncture Improves Sleep Disorders and Depression among Patients with Parkinson’s Disease: A Meta-Analysis" Healthcare 11, no. 14: 2042. https://doi.org/10.3390/healthcare11142042