
A Pilot Study to Examine the Effects of a Workplace Cyberbullying Cognitive Rehearsal Mobile Learning Program for Head Nurses: A Quasi-Experimental Study

Abstract
:1. Introduction
2. Methods
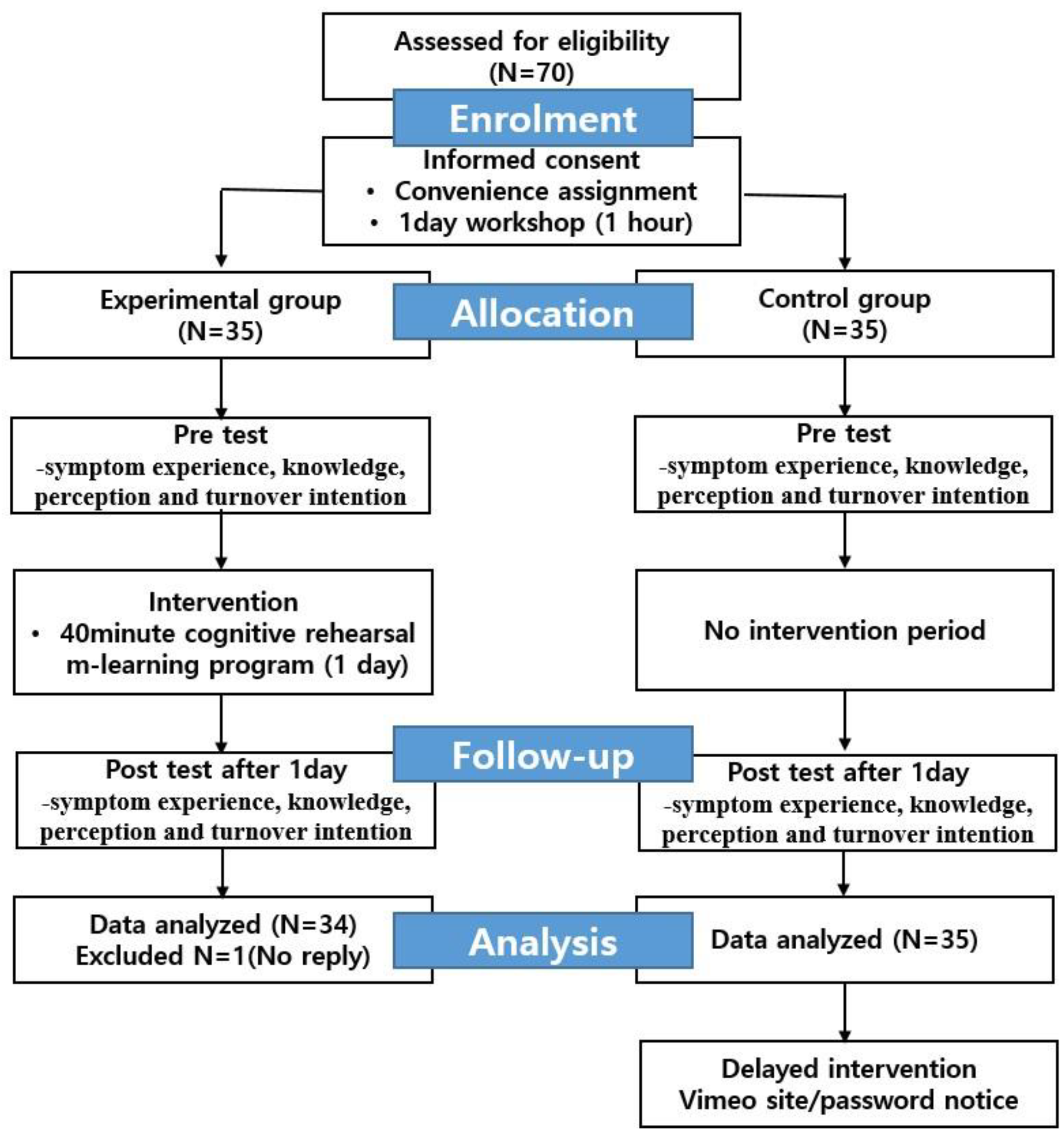
2.1. Study Design
2.2. Setting and Participants
2.3. Procedures
2.4. Intervention
2.5. Measurements
2.5.1. Symptom Experience
2.5.2. Knowledge of Workplace Cyberbullying
2.5.3. Perception of Workplace Cyberbullying
2.5.4. Turnover Intention
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Participants’ General Characteristics
3.2. Differences in Symptom Experience, Knowledge and Perception of Workplace Cyberbullying, and Turnover Intention between the Experimental and Control Groups
4. Discussion
5. Conclusions
Relevance for Clinical Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, Y.; Choi, J.S. Individual and organizational factors influencing workplace cyberbullying of nurses: A cross-sectional study. Nurs. Health Sci. 2021, 23, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Natalia, D.; Darryl, F.; David, T.; Bevan, C. Workplace Cyberbullying in New Zealand Nursing: A Report for Participants and Professional Bodies; School of Management, Massey University: Auckland, New Zealand, 2017; Available online: https://www.massey.ac.nz/shadomx/apps/fms/fmsdownload.cfm?file_uuid=D5ECA077-0C0D-4603-894F-AC2EBADE3FBE (accessed on 5 May 2020).
- Farley, S.; Coyne, I.; Axtell, C.; Sprigg, C. Design, development and validation of a workplace cyberbullying measure, the WCM. Work Stress 2016, 30, 293–317. [Google Scholar] [CrossRef]
- Smith, P.K.; Mahdavi, J.; Carvalho, M.; Fisher, S.; Russell, S.; Tippett, N. Cyberbullying: Its nature and impact in secondary school pupils. J. Child. Psychol. Psychiatry 2008, 49, 376–385. [Google Scholar] [CrossRef]
- Coyne, I.; Farley, S.; Axtell, C.; Sprigg, C.; Best, L.; Kwok, O. Understanding the relationship between experiencing workplace cyberbullying, employee mental strain and job satisfaction: A dysempowerment approach. Int. J. Hum. Resour. Manag. 2017, 28, 945–972. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Park, M. Effects of nursing organisational culture on face-to-face bullying and cyberbullying in the workplace. J. Clin. Nurs. 2019, 28, 2577–2588. [Google Scholar] [CrossRef]
- Forssell, R.C. Cyberbullying in a boundary blurred working life: Distortion of the private and professional face on social media. Qual. Res. Organ. Manag. 2019, 15, 89–107. [Google Scholar] [CrossRef] [Green Version]
- Vranjes, I.; Baillien, E.; Vandebosch, H.; Erreygers, S.; Witte, H.D. The dark side of working online: Towards a definition and an Emotion Reaction model of workplace cyberbullying. Comput. Hum. Behav. 2017, 69, 324–334. [Google Scholar] [CrossRef]
- Weiss, H.M.; Cropanzano, R. Affective events theory: A theoretical discussion of the structure, causes and consequences of affective experiences at work. In Research in Organizational Behavior; Staw, B.M., Cummings, L.L., Eds.; JAI Press: Greenwich, CT, USA, 1996; pp. 1–74. [Google Scholar]
- Johnson, S.L. An ecological model of workplace bullying: A guide for intervention and research. Nurs. Forum. 2011, 46, 55–63. [Google Scholar] [CrossRef]
- Kowalski, R.M.; Giumetti, G.W.; Schroeder, A.N.; Lattanner, M.R. Bullying in the digital age: A critical review and meta-analysis of cyberbullying research among youth. Psychol. Bull. 2014, 140, 1073–1137. [Google Scholar] [CrossRef]
- Park, M.; Choi, J.S. Effects of workplace cyberbullying on nurses’ symptom experience and turnover intention. J. Nurs. Manag. 2019, 27, 1108–1115. [Google Scholar] [CrossRef]
- Griffin, M. Teaching cognitive rehearsal as a shield for lateral violence: An intervention for newly licensed nurses. J. Contin. Educ. Nurs. 2004, 35, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stagg, S.J.; Sheridan, D.; Jones, R.A.; Speroni, K.G. Evaluation of a workplace bullying cognitive rehearsal program in a hospital setting. J. Contin. Educ. Nurs. 2011, 42, 395–401, quiz 402. [Google Scholar] [CrossRef] [PubMed]
- Stagg, S.J.; Sheridan, D.J.; Jones, R.A.; Speroni, K.G. Workplace bullying: The effectiveness of a workplace program. Workplace Health Saf. 2013, 61, 333–338. [Google Scholar] [CrossRef]
- Karakaş, S.A.; Okanli, A. The effect of assertiveness training on the mobbing that nurses experience. Workplace Health Saf. 2015, 63, 446–451. [Google Scholar] [CrossRef] [Green Version]
- Rush, K.L.; Adamack, M.; Gordon, J.; Janke, R. New graduate nurse transition programs: Relationships with bullying and access to support. Contemp. Nurse 2014, 48, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.; Jeong, Y.J. Effects of a smartphone application for cognitive rehearsal intervention on workplace bullying and turnover intention among nurses. Int. J. Nurs. Pract. 2019, 25, e12786. [Google Scholar] [CrossRef]
- Park, S.Y.; Shin, H.; Cho, Y.; Kim, S. Effectiveness of interventions for workplace bullying among nurses: A systematic review. J. Korean Acad. Nurs. Adm. 2018, 24, 339–351. [Google Scholar] [CrossRef] [Green Version]
- Hay, B.; Carr, P.J.; Dawe, L.; Clark-Burg, K. ‘iM Ready to Learn’: Undergraduate nursing students knowledge, preferences, and practice of mobile technology and social media. Comput. Inform. Nurs. 2017, 35, 8–17. [Google Scholar] [CrossRef]
- Forehand, J.W.; Miller, B.; Carter, H. Integrating mobile devices into the nursing classroom. Teach. Learn. Nurs. 2017, 12, 50–52. [Google Scholar] [CrossRef]
- Stagg, S.J.; Sheridan, D. Effectiveness of bullying and violence prevention programs. AAOHN J. 2010, 58, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Kim, J.I.; Yun, S. Effects of a cognitive rehearsal program on interpersonal relationships, workplace bullying, symptom experience, and turnover intention among nurses: A randomized controlled trial. J. Korean Acad. Nurs. 2017, 47, 689–699. [Google Scholar] [CrossRef] [Green Version]
- Peterson, C. Bringing ADDIE to life: Instructional design at its best. J. Educ. Multimed. Hypermedia 2003, 12, 227–242. [Google Scholar]
- Kile, D.; Eaton, M.; de Valpine, M.; Gilbert, R. The effectiveness of education and cognitive rehearsal in managing nurse-to-nurse incivility: A pilot study. J. Nurs. Manag. 2019, 27, 453–552. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Choi, J.S. Development and evaluation of a workplace bullying cognitive rehearsal-based nursing simulation education Program: A mixed-methods study. Int. J. Environ. Res. Public Health 2023, 11, 4974. [Google Scholar] [CrossRef]
- Derogatis, L.R. Brief Symptom Inventory (BSI-18). Administration, Scoring and Procedures Manual; NCS Pearson Inc.: Minneapolis, MN, USA, 2001. [Google Scholar]
- Park, K.P.; Woo, S.W.; Chang, M.S. Validational study of brief symptoms inventory-18 (BSI-18) in college students. Korean J. Clin. Psychol. 2012, 31, 507–521. [Google Scholar] [CrossRef] [Green Version]
- Haq, N.U.; Arshad, Z.; Lehri, S.A.; Nasim, A.; Saood, M.; Zarak, M.S. Assessment of knowledge, perception and prevalence of bullying practices among medical students of Quetta. J. Adv. Med. Med. Res. 2018, 26, 1–20. [Google Scholar] [CrossRef]
- Mobley, W.H.; Horner, S.O.; Hollingsworth, A.T. An evaluation of the precursors of hospital employee turnover. J. Appl. Psychol. 1978, 63, 408–414. [Google Scholar] [CrossRef]
- Shin, H.R.; Cho, Y.C. Relationship between job stress and turnover intention among nurses in university hospitals. J. Korea Acad.-Ind. Coop. Soc. 2013, 14, 3958–3970. [Google Scholar] [CrossRef] [Green Version]
- Cuevas, H.E.; Timmerman, G.M. Use of an objective structured clinical examination in clinical nurse specialist education. Clin. Nurse Spec. 2016, 30, 172–176. [Google Scholar] [CrossRef]
- Smith, C.R.; Gillespie, G.L.; Brown, K.C.; Grubb, P.L. Seeing students squirm: Nursing students’ experiences of bullying behaviors during clinical rotations. J. Nurs. Educ. 2016, 55, 505–513. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Categories | Construct | Item | Content Validity |
|---|---|---|---|
| 1. Theoretical concepts of workplace cyberbullying. | Text, picture, photograph, voice recording, and video lecture | General information | 1.00 |
| Question: Is the following situation workplace cyberbullying? (1) Work-related cyberbullying scenario 1 (2) Person-related cyberbullying scenario 1 | |||
| Definition; other terms | |||
| Common theories regarding workplace cyberbullying | |||
| Prevalence of workplace bullying | |||
| Target characteristics | |||
| Causes and effects of workplace cyberbullying | |||
| 2. Common workplace cyberbullying behaviors. | Text, picture, photograph, and voice recording | Characteristics of cyberbullying | 1.00 |
| Types of workplace cyberbullying | |||
| (1) 10 Work-related cyberbullying behaviors (2) 11 Person-related cyberbullying behaviors | |||
| 3. What can be done about workplace cyberbullying? | Text, picture, photograph, and voice recording | Individual; micro level (1) 11 ways to handle workplace cyberbullying | 0.95 |
| Organizational; meso level | |||
| Industry and national; macro level (1) Legal response (2) School Violence Prevention Law (3) Workplace Harassment Prevention Law | |||
| 4. Workplace cyberbullying 10 cognitive rehearsal scenarios. | Text, picture, photograph, voice recording, and video lecture | Demonstration scenarios Practice scenarios | 1.00 |
| (1) 5 Work-related cyberbullying scenarios (2) 5 Person-related cyberbullying scenarios | |||
| 5. Summary. | Text, picture, photograph, voice recording, and video lecture | Summary | 1.00 |
| Total | 0.97 | ||
| Variables (Range) | Categories | Experimental (n = 35) n (%) or Mean ± SD | Control (n = 34) n (%) or Mean ± SD | χ2 or t | p |
|---|---|---|---|---|---|
| Gender | Female | 35(100.0) | 34(100.0) | ||
| Age (in years) | 50.60 ± 5.07 | 48.76 ± 4.81 | 1.541 | 0.128 | |
| Marital status | Married | 29(82.9) | 28(82.4) | 0.003 | 0.998 |
| Unmarried | 5(14.3) | 5(14.7) | |||
| Others | 1(2.9) | 1(2.9) | |||
| Education | Associate degree | 1(2.9) | 0(0.0) | 1.348 | 0.718 |
| Bachelor | 8(22.9) | 6(17.6) | |||
| Master | 25(71.4) | 27(79.4) | |||
| PhD | 1(2.9) | 1(2.9) | |||
| Department | General ward | 17(48.6) | 13(38.2) | 4.274 | 0.370 |
| Intensive care unit | 3(8.6) | 5(14.7) | |||
| Operation room | 2(5.7) | 6(17.6) | |||
| Outpatient unit | 4(11.4) | 5(14.7) | |||
| Others | 9(25.7) | 5(14.7) | |||
| Position | Head nurse | 35(100.0) | 34(100.0) | ||
| Salary | <5000 | 1(2.9) | 2(5.9) | 1.410 | 0.703 |
| (10,000 KRW/year) | 5000–<7000 | 27(77.1) | 27(79.4) | ||
| 7000–<9000 | 6(17.1) | 5(14.7) | |||
| ≥9000 | 1(2.9) | 0(0.0) | |||
| Clinical experience length (in years) | 28.24 ± 5.10 | 26.79 ± 4.59 | 0.926 | 0.339 | |
| Three-shift system | No | 35(100.0) | 34(100.0) | ||
| Experience with face-to–face workplace bullying | Yes | 2(5.7) | 2(5.9) | 0.001 a | 1.000 |
| (in the past 6 months) | No | 33(94.3) | 32(94.1) | ||
| Experience with workplace cyberbullying | Yes | 3(8.6) | 0(0.0) | 3.047 a | 0.239 |
| (in the past 6 months) | No | 32(91.4) | 34(100.0) | ||
| Symptom experience (1–5) | 3.10 ± 1.12 | 2.89 ± 1.04 | 0.809 | 0.422 | |
| Knowledge of workplace cyberbullying (0–100) | 84.06 ± 11.59 | 88.08 ± 8.22 | −1.657 | 0.102 | |
| Perception of workplace cyberbullying (1–5) | 3.98 ± 0.52 | 3.76 ± 0.65 | 1.575 | 0.120 | |
| Turnover intention (1–5) | 2.04 ± 0.83 | 2.29 ± 0.66 | −1.372 | 0.175 | |
| Variables | Group | Pretest | Posttest | Difference | t or U | p |
|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | ||||
| Symptom experience | Exp.(n = 35) | 3.10 ± 1.12 | 3.47 ± 1.13 | 0.37 ± 0.76 | 414.50 * | 0.030 |
| Con.(n = 34) | 2.89 ± 1.04 | 2.86 ± 1.10 | −0.03 ± 0.50 | |||
| Knowledge of workplace cyberbullying | Exp.(n = 35) | 84.06 ± 11.59 | 95.19 ± 5.32 | 11.13 ± 11.89 | 319.00 * | 0.001 |
| Con.(n = 34) | 88.08 ± 8.22 | 88.85 ± 9.50 | 0.77 ± 11.15 | |||
| Perception of workplace cyberbullying | Exp.(n = 35) | 3.98 ± 0.52 | 4.45 ± 0.82 | 0.47 ± 0.99 | 2.01 | 0.048 |
| Con.(n = 34) | 3.76 ± 0.65 | 3.83 ± 0.65 | 0.07 ± 0.60 | |||
| Turnover intention | Exp.(n = 35) | 2.04 ± 0.83 | 1.94 ± 0.80 | −0.09 ± 0.58 | 538.50 * | 0.485 |
| Con.(n = 34) | 2.29 ± 0.66 | 2.25 ± 0.77 | −0.03 ± 0.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, M.; Cho, O.Y.; Choi, J.S. A Pilot Study to Examine the Effects of a Workplace Cyberbullying Cognitive Rehearsal Mobile Learning Program for Head Nurses: A Quasi-Experimental Study. Healthcare 2023, 11, 2041. https://doi.org/10.3390/healthcare11142041
Park M, Cho OY, Choi JS. A Pilot Study to Examine the Effects of a Workplace Cyberbullying Cognitive Rehearsal Mobile Learning Program for Head Nurses: A Quasi-Experimental Study. Healthcare. 2023; 11(14):2041. https://doi.org/10.3390/healthcare11142041
Chicago/Turabian StylePark, Mijeong, Ok Yeon Cho, and Jeong Sil Choi. 2023. "A Pilot Study to Examine the Effects of a Workplace Cyberbullying Cognitive Rehearsal Mobile Learning Program for Head Nurses: A Quasi-Experimental Study" Healthcare 11, no. 14: 2041. https://doi.org/10.3390/healthcare11142041