
Shared Decision-Making to Improve Health-Related Outcomes for Adults with Stroke Disease

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
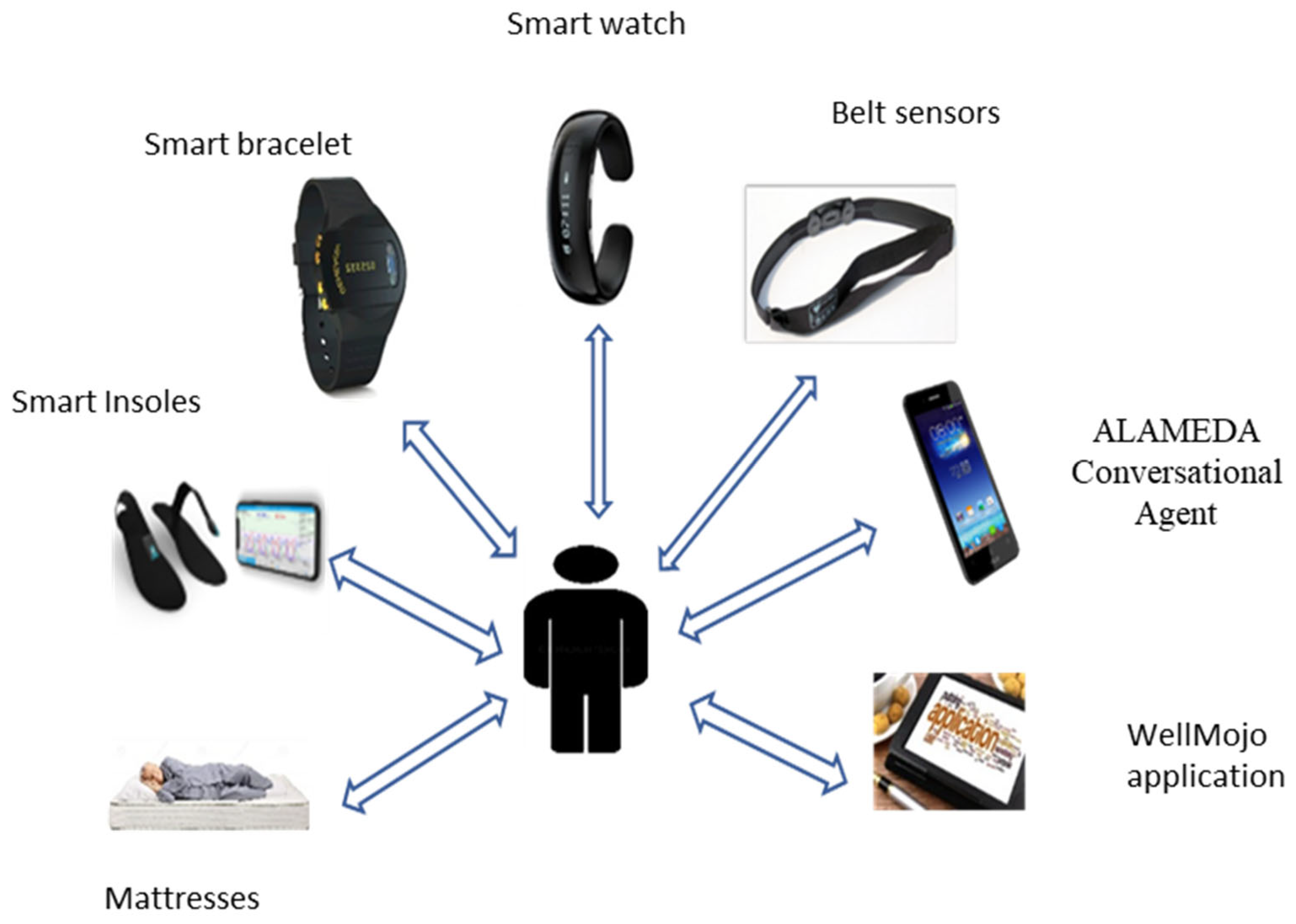
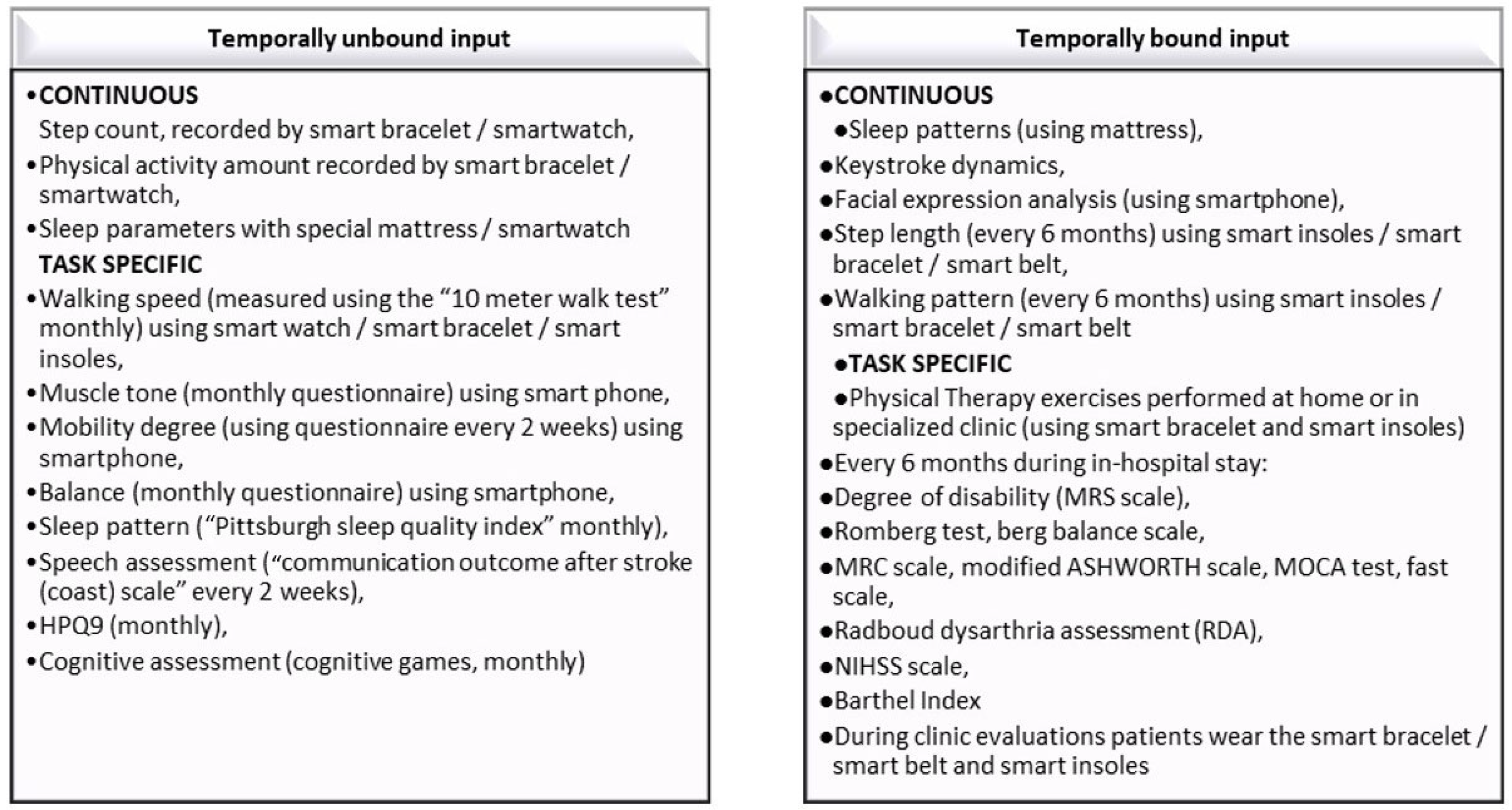
2.1. Patient’s Data Collection Journey for the Stroke Pilot
- Temporally unbound inputs: data that can be collected from sensors or self-reported by the patient all throughout the duration of the pilot.
- Temporally bound inputs: data that will be collected in a predefined window of time around the milestones defined for the trial (e.g., two weeks before and/or after the milestone).
- Continuous input—the patient will provide data by normal wearing of the sensors and consistent response to simple lifestyle and wellbeing questions, with the minimum intrusive level.
- Task-specific input—the patient performs (upon being prompted by ALAMEDA) a specific type of activity at home. The instructions on how to perform the activity have to be available in the ALAMEDA app and the patient can call upon the support of the Patient Engagement Team.
2.2. Methodology of Shared Decision-Making for Stroke Pilot
- Three representatives affected by the neurological conditions under study: one person with Multiple Sclerosis (MS), one person with Parkinson’s Disease (PD) and one person in recovery after a Stroke incident.
- Medical practitioner representatives, each being an expert in one of the three considered neurological conditions.
- One representative from the technical partners of the ALAMEDA consortium.
- One ethics expert.
- One person with expertise in implementing the MULTI-ACT methodology, actively assisting and supporting the activities of the ECT.
- One person acting as the task leader for the stakeholder engagement activities throughout ALAMEDA project.
Local Community Group for Stroke Pilot
- 1.
- Breaking down boundaries: as early testers of the ALAMEDA system, members of the LCG facilitate describe the facilities, infrastructure and research agenda of ALAMEDA to each patient that will be onboarded in the Pilot studies. They would help patients and caregivers understand the monitoring protocol and research questions posed in the project and facilitate end-user engagement in the research activities.
- 2.
- Research priorities: LCG members and the patients engage in validation of the usability and personal impact/satisfaction metrics that will be used in the project.
- 3.
- Steering institutions: Patients are invited to be members in the Local Community Groups.
- 4.
- Design and Plan: LCG members and the patients will participate in customizing the Patient Data Collection Journey, as well as the data interaction modalities (definition of the appropriate means to deliver and receive comprehensive visualizations of the data collected from a person throughout the pilot).
- 5.
- Research Execution: LCG members are engaged in the monitoring of ALAMEDA Pilots execution to increase compliance with the monitoring protocol and facilitate meaningful data collection.
- 6.
- Evaluation: LCG members and the patients are involved in results assessment relative to the ALAMEDA usability and personal impact metrics, collected through questionnaires that are handed out during Pilot milestones.
- 7.
- Translation to the Community: LCG members actively collect feedback on the experience of ALAMEDA pilot study participants and are engaged in the dissemination process of this knowledge to other persons affected by the same neurological disorder.
- Identifying the possible health care journeys for patients, i.e., consideration of the most common treatment trajectories taken by persons affected by PMSS and accounting the most common patient concerns.
- A clear presentation of the ALAMEDA sensing devices and software applications (e.g., ALAMEDA digital companion, ALAMEDA conversational agent) and of the research objectives considered by the medical experts.
- A discussion around the when, how and with what of the data collection process during the pilots, as well as the prioritization of patient-reported outcomes (PRO) referring to non-disease related factors (e.g., psychological, social status, quality of life, financial issues).
- Identification and prioritization of options for data interaction (i.e., the technical means by which participants in the pilots submit and visualize their data, respond to notifications or engage in dialog with the ALAMEDA Conversational Agent).
2.3. The Specific Questionnaire Result of Local Community Group consultation
3. Results Obtained by Consulting the Members of the LCG
3.1. Preferences on Device Wearing
3.2. Preferences for Filling out PROs
3.3. The Preferences for Using the Conversational Agent
3.4. Preferences Regarding the Disease Self-Management Module
3.5. Preferences and Other Aspects
- The specific devices (smart bracelets, smart insoles, smart belts) will be worn by all patients during home exercises. The devices must be worn by those patients that undergo physical rehabilitation sessions. The patients need to use the ALAMEDA application to label the type, start and end time of physical rehabilitation exercises (according to a predefined list of exercises).
- There were predominant preferences for standard interfaces to fill out medical questionnaires and also predominant preferences for stage-wise fill out of the questionnaires. The majority of LCG members agreed that the conversational agent should be maintained as an option to fill in medical questionnaires.
- The Conversational Agent acts as a rapid interface and it is used to report on non-disease-related aspects (taking into account the records of each patient’s emotional status). The Conversational Agent interface is also accepted to be used to receive input from the caregivers.
- The ALAMEDA application must support the quick visualization of patient-submitted information and video tutorials from medical experts.
- Localization data collection must be made only upon request and at a general level of granularity. The smartphone on which to run the ALAMEDA application (own phone or one provided within the project) is a choice that will be left as a personal preference for each participant that enters the study.
Discussion Related to Technical Aspects of Wearable Devices and ALAMEDA Applications
- Feedback (from doctors):
- Applications to collect questionnaires were easy to use but a better interaction in natural langue would be desirable.
- Insoles. The following problems for the patients wearing insoles were detected:
- −
- Attachment to the hospital slippers-patients is not allowed with other type of shoes, it is difficult to wear Snickers during hospitalization;
- −
- Turn off due to the detachment of the plastic piece that holds the battery
- −
- The smartphone supporting the insole application should be kept close to the patient, otherwise the insoles will disconnect
- −
- Some patients remove the insoles them because they seem not to be properly attached and they fear they might fall
- Belt. The sending data indicator of the belt was not always functioning.
- −
- Mini smart-mattress. Smart-mattress must be restarted with a pin after every patient–impossible to configure it without restarting
- Feedback (from patients):
- Applications to collect questionnaires were easy to use but a better interaction in natural langue would be desirable.
- Insoles:
- −
- Difficult to wear in slippers
- −
- Most of the patients had the tendency to fall: they slipped when wearing the insoles
- −
- They prefer using them only during the exercises
- −
- Difficulties in changing the batteries of the insoles: almost always changed by a team member
- Belt: Difficult to wear due to weight. They preferred using it during exercises
- Mini smart-mattress: No problem except the fact that one patient tried to install the mattress at home but he could not manage it.
3.6. Guidelines for Stroke Pilot
- General Guidelines: Inform the patient and caregiver about project goals, devices, and applications used in the project, and discuss the data collection journey and data viewing options
- Pilot Specific Guidelines: discussion over data collection journey for specific devices (smart belt, smart bracelet, and smart insoles), and over content and the method of transmitting the patient-reported outcomes related to impact on activities of daily living
3.7. Specific Guidelines for Stroke Pilot
3.7.1. Discussion over Data Collection Journey for Specific Devices
Participants: Patients, Clinicians, Physical Therapists, Technical Support
3.7.2. Discussion over Content and Method of Transmitting PROs Related to Impact on Activities of Daily Living
Participants: Patients, Clinicians, and Technical Support
- Fill in the entire questionnaire upon each received notification.
- Notifications display only two to three questions per day, such that the full questionnaire is completed over the course of a week.
Opportunities, Disadvantages and Barriers of SDM Model
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MS | Multiple Sclerosis |
| PD | Parkinson’s Disease |
| PMSS | Parkinson’s, MS and Stroke |
| PRO | Results reported by the patient |
| LCG | Local Community Group |
| 6MWT | Six Meter Walk Test |
| MRC | Medical Research Council scale for motor weakness |
| MoCA | Montreal Cognitive Assessment |
| FAST | Functional Assessment Staging Tool |
| PHQ9 | Patient Health Questionnaire |
| PSQI | Pittsburgh Sleep Quality Index |
| HIHSS | National Institutes of Health Stroke Scale |
| MRS | Modified Rankin Scale |
| COAST | Communication Outcome after Stroke |
| MFIS | Modified Fatigue Impact Scale |
| FH-Q | Food Habits Questionnaire |
References
- Borumandnia, N.; Majd, H.A.; Doosti, H.; Olazadeh, K. The trend analysis of neurological disorders as major causes of death and disability according to human development, 1990–2019. Environ. Sci. Pollut. Res. 2022, 29, 14348–14354. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 US Neurological Disorders Collaborators. Burden of neurological disorders across the US from 1990-2017: A global burden of disease study. JAMA Neurol. 2020, 78, 165–176. [Google Scholar] [CrossRef]
- Deuschl, G.; Beghi, E.; Fazekas, F.; Varga, T.; Christoforidi, K.A.; Sipido, E.; Bassetti, C.L.; Vos, T.; Feigin, V.L. The burden of neurological diseases in Europe: An analysis for the Global Burden of Disease Study 2017. Lancet Public Health 2020, 5, e551–e567. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef]
- Huang, J.; Chen, W.; Zhang, X. Multiple sclerosis: Pathology, diagnosis and treatments. Exp. Ther. Med. 2017, 13, 3163–3166. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. American Heart Association Statistics Committee and stroke Statistics Subcommittee. Heart Disease and stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Wafa, H.A.; Wolfe, C.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef]
- Dobkin, B.H.; Dorsch, A. New evidence for therapies in stroke rehabilitation. Curr. Atheroscler. Rep. 2013, 15, 331. [Google Scholar] [CrossRef] [Green Version]
- Canova, C.; Danieli, S.; Barbiellini Amidei, C.; Simonato, L.; Di Domenicantonio, R.; Cappai, G.; Bargagli, A.M. A Systematic Review of Case-Identification Algorithms Based on Italian Healthcare Administrative Databases for Three Relevant Diseases of the Nervous System: Parkinson’s Disease, Multiple Sclerosis, and Epilepsy. Epidemiol. Prev. 2019, 43, 62–74. [Google Scholar] [CrossRef]
- Thimbleby, H. Technology and the Future of Healthcare. J. Public Health Res. 2013, 2, e28. [Google Scholar] [CrossRef] [Green Version]
- Kuriakose, D.; Xiao, Z. Pathophysiology and Treatment of stroke: Present Status and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 7609. [Google Scholar] [CrossRef] [PubMed]
- Ellis, T.D.; Earhart, G.M. Digital Therapeutics in Parkinson’s Disease: Practical Applications and Future Potential. J. Park. Dis. 2021, 11, S95–S101. [Google Scholar] [CrossRef] [PubMed]
- Mehl, G.; Tamrat, T.; Labrique, A.; Orton, M.; Baker, E.; Blaschke, S.; BonTempo, J.; DeBorma, N.; Eskandar, H.; Falzon, D.; et al. Classification of Digital Health Interventions v 1.0; Report number: WHO/RHR/18.06; World Health Organization WHO: Geneva, Switzerland, 2018. [Google Scholar] [CrossRef]
- Adams, J.L.; Lizarraga, K.; Waddell, E.M.; Myers, T.L.; Jensen-Roberts, S.; Modica, J.S.; Schneider, R.B. Digital Technology in Movement Disorders: Updates, Applications, and Challenges. Curr. Neurol. Neurosci. Rep. 2021, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P. Smartphone Subscriptions Worldwide 2016–2027. Available online: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/ (accessed on 18 January 2023).
- Coravos, A.; Goldsack, J.C.; Karlin, D.R.; Nebeker, C.; Perakslis, E.; Zimmerman, N.; Erb, M.K. Digital medicine: A primer on measurement. Digit Biomark 2019, 3, 31–71. [Google Scholar] [CrossRef] [PubMed]
- Metz, M.J.; Veerbeek, M.A.; Twisk, J.; van der Feltz-Cornelis, C.M.; de Beurs, E.; Beekman, A. Shared decision-making in mental health care using routine outcome monitoring: Results of a cluster randomised-controlled trial. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, Y. Shared decision making for adults with severe mental illness: A concept analysis. Jpn. J. Nurs. Sci. JJNS 2020, 17, e12365. [Google Scholar] [CrossRef] [PubMed]
- Curtis, L.C.; Wells, S.M.; Penney, D.J.; Ghose, S.S.; Mistler, L.A.; Mahone, I.H.; Delphin-Rittmon, M.; del Vecchio, P.; Lesko, S. Pushing the envelope: Shared decision making in mental health. Psychiatr. Rehabil. J. 2010, 34, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.J. Shared decision-making in stroke: An evolving approach to improved patient care. Stroke Vasc. Neurol. 2017, 2, 84–87. [Google Scholar] [CrossRef] [Green Version]
- Zaratin, P.; Bertorello, D.; Guglielmino, R.; Devigili, D.; Brichetto, G.; Tageo, V.; Dati, G.; Kramer, S.; Battaglia, M.A.; Luca, M. The MULTI-ACT model: The path forward for participatory and anticipatory governance in health research and care. Health Res. Policy Syst. 2022, 20, 22. [Google Scholar] [CrossRef]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Violato, M.; Candio, P.; Leal, J. Economic burden of stroke across Europe: A population-based cost analysis. Eur. Stroke J. 2020, 5, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 10267. [Google Scholar] [CrossRef]
- Feigin, V.L.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Ferede Abera, S.; Abyu, G.Y.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; et al. Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feigin, V.L.; Nguyen, G.; Cercy, K.; Johnson, C.O.; Alam, T.; Parmar, P.G.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abejie, A.N.; et al. Global, regional, and country-specific lifetime risks of stroke, 1990–2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef] [PubMed]
- National Research Council (US) Committee on A Framework for Developing a New Taxonomy of Disease. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Xian, Y.; O’Brien, E.C.; Fonarow, G.C.; Olson, D.M.; Schwamm, L.H.; Hannah, D.; Lindholm, B.; Maisch, L.; Lytle, B.L.; Greiner, M.A.; et al. Patient-Centered Research into Outcomes stroke Patients Prefer and Effectiveness Research: Implementing the patient-driven research paradigm to aid decision making in stroke care. Am. Heart J. 2015, 170, 36–45.e11. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Johnston, S.C. Decision making in acute stroke care: Learning from neuroeconomics, neuromarketing, and poker players. Stroke 2014, 45, 2144–2150. [Google Scholar] [CrossRef] [Green Version]
- Shay, L.A.; Lafata, J.E. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2015, 35, 114–131. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Smith, E.E.; Saver, J.L.; Reeves, M.J.; Bhatt, D.L.; Grau- Sepulveda, M.V.; Olson, D.M.; Hernandez, A.F.; Peterson, E.D.; Schwamm, L.H. Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: Patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation 2011, 123, 750–758. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.J.; Mullins, C.D. Value assessment at the point of care: Incorporating patient values throughout care delivery and a draft taxonomy of patient values. Value Health 2017, 20, 292–295. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, C.; Hendriks, J. Partnering with patients in shared decision-making for stroke prevention in atrial fibrillation. Eur. J. Cardiovasc. Nurs. 2017, 16, 178–180. [Google Scholar] [CrossRef] [PubMed]
- Kunneman, M.; Branda, M.E.; Hargraves, I.G.; Sivly, A.L.; Lee, A.T.; Gorr, H.; Burnett, B.; Suzuki, T.; Jackson, E.A.; Hess, E.; et al. Shared Decision Making for Atrial Fibrillation (SDM4AFib) Trial Investigators. Assessment of Shared Decision-making for stroke Prevention in Patients With Atrial Fibrillation: A Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1215–1224. [Google Scholar] [CrossRef]
- De Boer, M.E.; Depla, M.; Wojtkowiak, J.; Visser, M.C.; Widdershoven, G.A.; Francke, A.L.; Hertogh, C.M. Life-and-death decision-making in the acute phase after a severe stroke: Interviews with relatives. Palliat. Med. 2015, 29, 451–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webster, D.; Celik, O. Systematic review of Kinect applications in elderly care and stroke rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 108. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.H.; Siewiorek, D.P.; Smailagic, A.; Bernardino, A.; Badia, S.B. Learning to assess the quality of stroke rehabilitation exercises. In Proceedings of the 24th International Conference on Intelligent User Interfaces, Marina del Ray, CA, USA, 16–20 March 2019. [Google Scholar]
- Lang, C.E.; Bland, M.D.; Bailey, R.R.; Schaefer, S.Y.; Birkenmeier, R.L. Assessment of upper extremity impairment, function, and activity after stroke: Foundations for clinical decision making. J Hand Ther. 2013, 26, 104–114. [Google Scholar] [CrossRef] [Green Version]
- Berner, E.S. Clinical Decision Support Systems; Springer: Berlin/Heidelberg, Germany, 2007; p. 233. [Google Scholar]
- Adomavičienė, A.; Daunoravičienė, K.; Kubilius, R.; Varžaitytė, L.; Raistenskis, J. Influence of New Technologies on Post-Stroke Rehabilitation: A Comparison of Armeo Spring to the Kinect System. Medicina (Kaunas) 2019, 55, 98. [Google Scholar] [CrossRef] [Green Version]
- Batcho, C.S.; Tennant, A.; Thonnard, J.L. ACTIVLIM-Stroke: A crosscultural Rasch-built scale of activity limitations in patients with stroke. Stroke 2012, 43, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Glidden, A.M.; Holloway, M.R.; Birbeck, G.L.; Schwamm, L.H. Teleneurology and mobile technologies: The future of neurological care. Nat. Rev. Neurol. 2018, 14, 285–297. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Hausdorff, J.M.; Sa’nchez-Ferro, A.; Klucken, J.; Merola, A.; Bonato, P.; Paul, S.S.; Horak, F.B.; Vizcarra, J.A.; Mestre, T.A.; et al. A roadmap for implementation of patient-centered digital outcome measures in Parkinson’s disease obtained using mobile health technologies. Mov. Disord. 2019, 34, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Joseph-Williams, N.; Elwyn, G.; Edwards, A. Knowledge is not power for patients: A systematic review and thematic synthesis of patient- reported barriers and facilitators to shared decision making. Patient Educ. Couns. 2014, 94, 291–309. [Google Scholar] [CrossRef]
- Légaré, F.; Witteman, H.O. Shared decision making: Examining key elements and barriers to adoption into routine clinical practice. Health Aff. 2013, 32, 276–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, M.; Davies, M.; Edwards, A. What are the external influences on information exchange and shared decision-making in healthcare consultations: A meta-synthesis of the literature. Patient Educ. Couns. 2009, 75, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Waddell, A.; Lennox, A.; Spassova, G.; Bragge, P. Barriers and facilitators to shared decision-making in hospitals from policy to practice: A systematic review. Implement. Sci. 2021, 16, 74. [Google Scholar] [CrossRef] [PubMed]
- Tringale, M.; Stephen, G.; Boylan, A.M.; Heneghan, C. Integrating patient values and preferences in healthcare: A systematic review of qualitative evidence. BMJ Open 2022, 12, e067268. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Domains | Predictor Variables | Inferred Variables |
|---|---|---|
| Domain I Mobility, general motor or physical function |
|
|
| Domain II Sleep disorders |
|
|
| Domain III Mental and cognitive ability |
|
|
| Domain IV Emotional status |
|
|
| Domain V Quality of life and daily living |
|
|
| Customization Points/Discussion and Decision Points | Key Issues | Features | Proposed Options |
|---|---|---|---|
| 1. Customization points | 1.1. Data Collection Journey for specific devices (smart bracelet, smart insoles, smart belt) |
|
|
| 1.2 Submission of Patient Reported Outcomes (PRO) |
|
| |
|
| ||
|
| ||
| 1.3. Preferred Use of the Conversational Agent |
| ||
| 1.4. Preference for Visualization of own health status |
| ||
| 2. Discussion and Decision points | 2.1. Discussion over the functionality and form of the Disease Self-Management Module (means and methods by which a patient can ascertain his/her own treatment progress) |
| |
| 2.2. Discussion over submission of non-disease related factors |
| ||
| 2.3. Discussion over using own smart phone or one given by ALAMEDA to run the Digital Companion and Conversational Agent applications | |||
| 2.4. Discussion over need and permission to collect patient location information during the pilot studies |
| Sections | Questions | Options |
|---|---|---|
| 1. Preference for wearing the device |
| (a) At home; (b) During physical therapy sessions; (c) During a visit to the family doctor; (d) The patient must be able to decide between (a), (b) and (c) |
| Yes/No | |
| 2. Preference for filling out PROs |
| (a) Standard digital interface; (b) Using the conversational agent; (c) Using a combination of (a) and (b); (d) The patient must be able to choose between (a), (b) and (c) |
| (a) App sends notification at any time of day, repeatedly, until the patient fills in the questionnaire; (b) can receive notification only in the morning or in the evening; (c) receives a notification as an invitation to chat with the conversational agent; (d) must be able to choose between (a), (b) and (c) | |
| (a) always filled in completely (b) filled in partially and completed later in the day/next day (c) filled in as part of a conversation with the ALAMEDA conversation agent (d) the patient must be able to choose between (a), (b) and (c) | |
| 3. Preference for using the Conversational Agent |
| (a) means to send PRO data (b) means to quickie query one’s own health status (c) both (a) and (b) |
| 1—strongly disagree, 5—strongly agree | |
| (a) using a standard questionnaire (b) through conversations (c) the patient must be able to choose between a) and b) | |
| Yes/No | |
| 4. Preference regarding the Disease Self-Management Module |
| 1—not at all, 5—very |
| (a) on smartphone (b) external discussion group on social media (e.g., WhatsApp group, Facebook group) (c) Video tutorials on ALAMEDA app in which a medical expert explains disease management techniques | |
| 5. Preference regarding other Aspects |
| (a) install on own phone (b) receive a new smartphone with a dual SIM card |
| (a) yes, but only if distinction is between: home, work a and other (b) Yes, but only when I want and only by answering to a question, NOT by GPS tracking (c) No, in no way |
| (a) At home | (b) During physical therapy sessions | (c) During a visit to the family doctor | (d) The patient must be able to decide between (a), (b) and (c) |
| Nr. Respondents | 5 | 3 | 3 |
| (a) Standard digital interface | (b) Using the conversational agent; | (c) Using a combination of (a) and (b);data | (d) The patient must be able to choose between (a), (b) and (c) data |
| Nr. Respondents | 6 | 1 | 4 | |
| (a) App sends notification at any time of day, repeatedly, until the patient fills in the questionnaire; | (b) can receive notification only in the morning or in the evening | (c) receives a notification as an invitation to chat with the conversational agent; | (d) must be able to choose between (a), (b) and (c) |
| Nr. Respondents | 4 | 2 | 5 | |
| (a) always filled in completely | (b) filled in partially and completed later in the day/next day | (c) filled in as part of a conversation with the ALAMEDA conversation agent | (d) the patient must be able to choose between (a), (b) and (c) |
| Nr. Respondents | 1 | 5 | 2 | 3 |
| (a) means to send PRO data | (b) means to quickie query one’s own health status | (c) both (a) and (b) |
| Nr. Respondents | 1 | 7 | 3 |
| 1–4 | 5—strongly agree | |
| Nr. Respondents | 6 | 5 | |
| (a) using a standard questionnaire | (b) through conversations | (c) the patient must be able to choose between (a) and (b) |
| Nr. Respondents | 5 | 4 | 2 |
| Yes | No | |
| Nr. Respondents | 10 | 1 |
| 1–4 | 5—very necessary | |
| Nr. Respondents | 5 | 6 | |
| (a) on smartphone | (b) external discussion group on social media | (c) Video tutorials on ALAMEDA app |
| Nr. Respondents | 5 | 3 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajenaru, L.; Sorici, A.; Mocanu, I.G.; Florea, A.M.; Antochi, F.A.; Ribigan, A.C. Shared Decision-Making to Improve Health-Related Outcomes for Adults with Stroke Disease. Healthcare 2023, 11, 1803. https://doi.org/10.3390/healthcare11121803
Bajenaru L, Sorici A, Mocanu IG, Florea AM, Antochi FA, Ribigan AC. Shared Decision-Making to Improve Health-Related Outcomes for Adults with Stroke Disease. Healthcare. 2023; 11(12):1803. https://doi.org/10.3390/healthcare11121803
Chicago/Turabian StyleBajenaru, Lidia, Alexandru Sorici, Irina Georgiana Mocanu, Adina Magda Florea, Florina Anca Antochi, and Athena Cristina Ribigan. 2023. "Shared Decision-Making to Improve Health-Related Outcomes for Adults with Stroke Disease" Healthcare 11, no. 12: 1803. https://doi.org/10.3390/healthcare11121803