
The Association between Electronic Health Literacy and Oral Health Outcomes among Dental Patients in Saudi Arabia: A Cross-Sectional Study
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
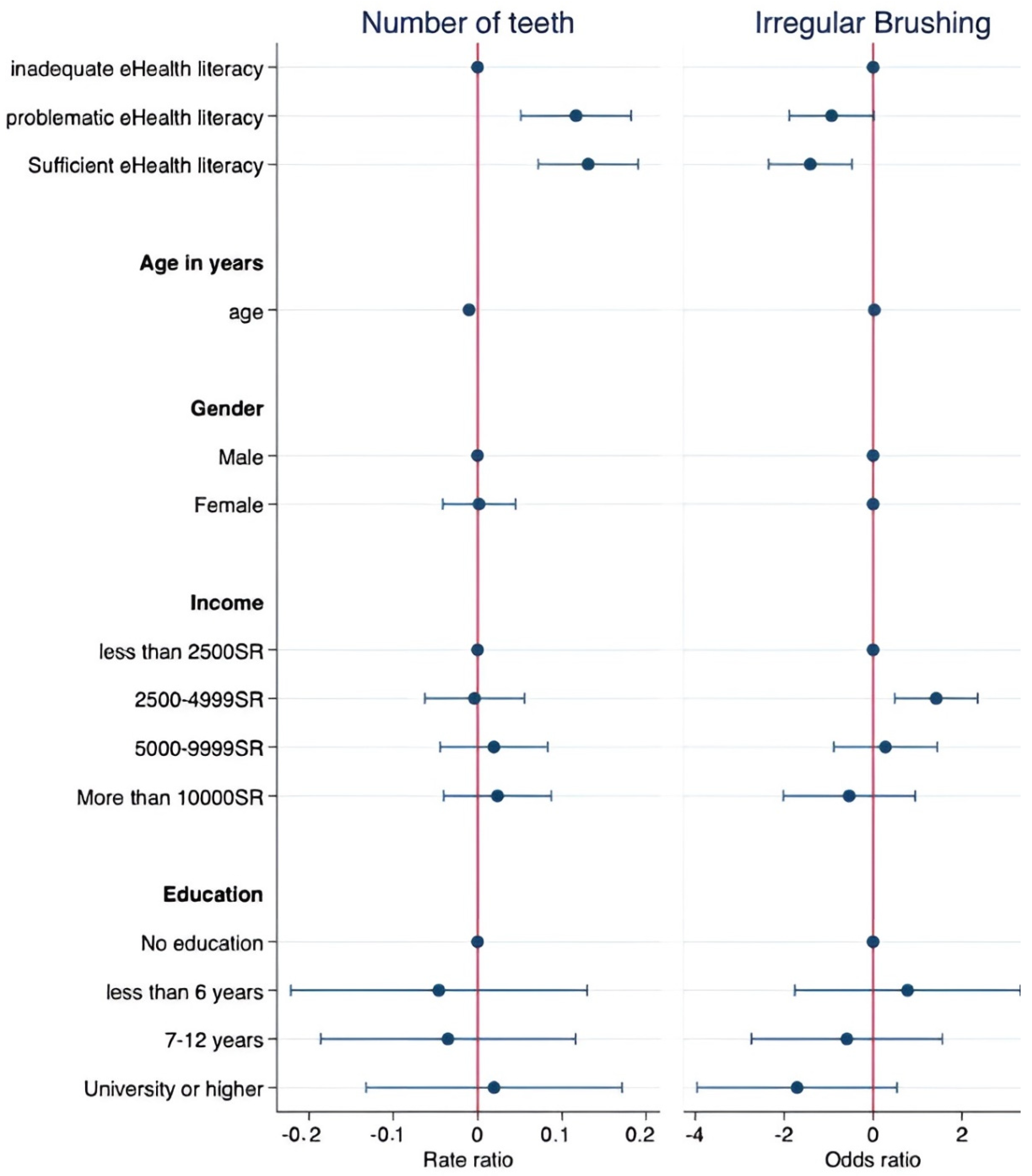
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Locker, D.; Gibson, B. The concept of positive health: A review and commentary on its application in oral health research. Community Dent. Oral Epidemiol. 2006, 34, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Hollis, C.; Falconer, C.J.; Martin, J.L.; Whittington, C.; Stockton, S.; Glazebrook, C.; Davies, E.B. Annual Research Review: Digital health interventions for children and young people with mental health problems–a systematic and meta-review. J. Child Psychol. Psychiatry 2017, 58, 474–503. [Google Scholar] [CrossRef] [PubMed]
- Shaw, T.; McGregor, D.; Brunner, M.; Keep, M.; Janssen, A.; Barnet, S. What is eHealth (6)? Development of a Conceptual Model for eHealth: Qualitative Study with Key Informants. J. Med. Internet Res. 2017, 19, e324. [Google Scholar] [CrossRef] [PubMed]
- da Fonseca, M.H.; Kovaleski, F.; Picinin, C.T.; Pedroso, B.; Rubbo, P. E-health practices and technologies: A systematic review from 2014 to 2019. Healthcare 2021, 9, 1192. [Google Scholar] [CrossRef]
- Ko, M.-S.; Kang, K.-J. Influence of health literacy and health empowerment on health behavior practice in elderly outpatients with coronary artery disease. J. Korean Clin. Nurs. Res. 2018, 24, 293–302. [Google Scholar]
- Harris, C.; Chestnutt, I. The use of the Internet to access oral health-related information by patients attending dental hygiene clinics. Int. J. Dent. Hyg. 2005, 3, 70–73. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. eHealth literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 2006, 8, e506. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Lim, S.-R. Effects of e-health literacy and oral health knowledge on oral health behavior in adults. J. Korean Soc. Dent. Hyg. 2022, 22, 11–19. [Google Scholar]
- Parthasarathy, D.S.; McGrath, C.; Bridges, S.M.; Wong, H.M.; Yiu, C.; Au, T. Efficacy of instruments measuring oral health literacy: A systematic review. Oral Health Prev. Dent. 2014, 12, 201–207. [Google Scholar]
- Batista, M.J.; Lawrence, H.P.; Sousa, M.d.L.R.d. Oral health literacy and oral health outcomes in an adult population in Brazil. BMC Public Health 2018, 18, 60. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Li, C.; Zhao, Y.; Sun, J. Trends and developments in oral health literacy: A scientometric research study (1991–2020). BDJ Open 2021, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, M.; Rakhshanderou, S.; Ramezankhani, A.; Mehrabi, Y.; Safari-Moradabadi, A. Systematic review of the tools of oral and dental health literacy: Assessment of conceptual dimensions and psychometric properties. BMC Oral Health 2020, 20, 186. [Google Scholar] [CrossRef] [PubMed]
- Dickson-Swift, V.; Kenny, A.; Farmer, J.; Gussy, M.; Larkins, S. Measuring oral health literacy: A scoping review of existing tools. BMC Oral Health 2014, 14, 148. [Google Scholar] [CrossRef] [Green Version]
- VanWormer, J.J.; Tambe, S.R.; Acharya, A. Oral health literacy and outcomes in rural Wisconsin adults. J. Rural Health 2019, 35, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Kleinman, D.V.; Horowitz, A.M.; Atchison, K.A. A framework to foster oral health literacy and oral/general health integration. Front. Dent. Med. 2021, 2, 723021. [Google Scholar] [CrossRef]
- Lee, D.-I.; Han, S.-J. Factors which affect the oral health-related quality of life of workers. J. Dent. Hyg. Sci. 2013, 13, 480–486. [Google Scholar]
- Mialhe, F.L.; Pereira, P.L.; de Oliveira Júnior, A.J.; Cortellazzi, K.L.; Soares, G.H. Patient’s oral health literacy and associations with sociodemographic, source of information, and oral health variables. Rev. Da ABENO 2022, 22, 1971. [Google Scholar] [CrossRef]
- Firmino, R.T.; Martins, C.C.; Faria, L.d.S.; Martins Paiva, S.; Granville-Garcia, A.F.; Fraiz, F.C.; Ferreira, F.M. Association of oral health literacy with oral health behaviors, perception, knowledge, and dental treatment related outcomes: A systematic review and meta-analysis. J. Public Health Dent. 2018, 78, 231–245. [Google Scholar] [CrossRef]
- Tennant, B.; Stellefson, M.; Dodd, V.; Chaney, B.; Chaney, D.; Paige, S.; Alber, J. eHealth literacy and Web 2.0 health information seeking behaviors among baby boomers and older adults. J. Med. Internet Res. 2015, 17, e70. [Google Scholar] [CrossRef]
- Gatto, S.L.; Tak, S.H. Computer, Internet, and e-mail use among older adults: Benefits and barriers. Educ. Gerontol. 2008, 34, 800–811. [Google Scholar] [CrossRef]
- Estai, M.; Kanagasingam, Y.; Tennant, M.; Bunt, S. A systematic review of the research evidence for the benefits of teledentistry. J. Telemed. Telecare 2018, 24, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, F.R.; Alamri, H.; Aljohani, M.; Sabbah, W.; O’Malley, L.; Glenny, A.-M. Dental caries in Saudi Arabia: A systematic review. J. Taibah Univ. Med. Sci. 2021, 16, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31. [Google Scholar] [CrossRef] [PubMed]
- Wångdahl, J.; Dahlberg, K.; Jaensson, M.; Nilsson, U. Arabic version of the electronic health literacy scale in Arabic-speaking individuals in Sweden: Prospective psychometric evaluation study. J. Med. Internet Res. 2021, 23, e24466. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth literacy scale. J. Med. Internet Res. 2006, 8, e507. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Silva-Junior, M.F.; Rosário de Sousa, M.d.L.; Batista, M.J. Health literacy on oral health practice and condition in an adult and elderly population. Health Promot. Int. 2021, 36, 933–942. [Google Scholar] [CrossRef]
- Geltman, P.L.; Adams, J.H.; Cochran, J.; Doros, G.; Rybin, D.; Henshaw, M.; Barnes, L.L.; Paasche-Orlow, M. The impact of functional health literacy and acculturation on the oral health status of Somali refugees living in Massachusetts. Am. J. Public Health 2013, 103, 1516–1523. [Google Scholar] [CrossRef]
- Ueno, M.; Takeuchi, S.; Oshiro, A.; Kawaguchi, Y. Relationship between oral health literacy and oral health behaviors and clinical status in Japanese adults. J. Dent. Sci. 2013, 8, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Tenani, C.F.; Silva Junior, M.F.; Lino, C.M.; Sousa, M.d.L.R.d.; Batista, M.J. The role of health literacy as a factor associated with tooth loss. Rev. Saúde Pública 2021, 55, 116. [Google Scholar] [CrossRef]
- Sermsuti-Anuwat, N.; Piyakhunakorn, P. Association between oral health literacy and number of remaining teeth among the Thai elderly: A cross-sectional study. Clin. Cosmet. Investig. Dent. 2021, 13, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Wehmeyer, M.M.; Corwin, C.L.; Guthmiller, J.M.; Lee, J.Y. The impact of oral health literacy on periodontal health status. J. Public Health Dent. 2014, 74, 80–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldoory, L.; Macek, M.D.; Atchison, K.A.; Chen, H. Comparing well-tested health literacy measures for oral health: A pilot assessment. J. Health Commun. 2016, 21, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Macek, M.D.; Atchison, K.A.; Watson, M.R.; Holtzman, J.; Wells, W.; Braun, B.; Aldoory, L.; Messadi, D.; Gironda, M.; Haynes, D. Assessing health literacy and oral health: Preliminary results of a multi-site investigation. J. Public Health Dent. 2016, 76, 303–313. [Google Scholar] [CrossRef]
- Alauddin, M.S.; Baharuddin, A.S.; Mohd Ghazali, M.I. The modern and digital transformation of oral health care: A mini review. Healthcare 2021, 9, 118. [Google Scholar] [CrossRef]
- Fadahunsi, K.P.; O’Connor, S.; Akinlua, J.T.; Wark, P.A.; Gallagher, J.; Carroll, C.; Car, J.; Majeed, A.; O’Donoghue, J. Information quality frameworks for digital health technologies: Systematic review. J. Med. Internet Res. 2021, 23, e23479. [Google Scholar] [CrossRef] [PubMed]
- Risling, T.; Martinez, J.; Young, J.; Thorp-Froslie, N. Evaluating patient empowerment in association with eHealth technology: Scoping review. J. Med. Internet Res. 2017, 19, e329. [Google Scholar] [CrossRef]
- Xu, R.H.; Zhou, L.-M.; Wong, E.L.-Y.; Wang, D. The association between patients’ eHealth literacy and satisfaction with shared decision-making and well-being: Multicenter cross-sectional study. J. Med. Internet Res. 2021, 23, e26721. [Google Scholar] [CrossRef]
- Xie, L.; Zhang, S.; Xin, M.; Zhu, M.; Lu, W.; Mo, P.K.-H. Electronic health literacy and health-related outcomes among older adults: A systematic review. Prev. Med. 2022, 157, 106997. [Google Scholar] [CrossRef]
- Sabbah, W.; Tsakos, G.; Chandola, T.; Sheiham, A.; Watt, R. Social gradients in oral and general health. J. Dent. Res. 2007, 86, 992–996. [Google Scholar] [CrossRef]
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic status and access to healthcare: Interrelated drivers for healthy aging. Front. Public Health 2020, 8, 231. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Zhao, S.Z.; Guo, N.; Wu, Y.; Weng, X.; Wong, J.Y.-H.; Lam, T.H.; Wang, M.P. Socioeconomic disparities in eHealth literacy and preventive behaviors during the COVID-19 pandemic in Hong Kong: Cross-sectional study. J. Med. Internet Res. 2021, 23, e24577. [Google Scholar] [CrossRef] [PubMed]
- Busse, T.S.; Nitsche, J.; Kernebeck, S.; Jux, C.; Weitz, J.; Ehlers, J.P.; Bork, U. Approaches to Improvement of Digital Health Literacy (eHL) in the Context of Person-Centered Care. Int. J. Environ. Res. Public Health 2022, 19, 8309. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Beauchamp, A.; Elsworth, G.R.; Osborne, R.H. Applying the electronic health literacy lens: Systematic review of electronic health interventions targeted at socially disadvantaged groups. J. Med. Internet Res. 2020, 22, e18476. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.A.; Currie, L.M.; Bakken, S.; Vawdrey, D.K.; Stone, P.W. Health literacy screening instruments for eHealth applications: A systematic review. J. Biomed. Inform. 2012, 45, 598–607. [Google Scholar] [CrossRef]
- Hernandez, L.M. Health Literacy, EHealth, and Communication: Putting the Consumer First: Workshop Summary; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Gurgel-Juarez, N.; Torres-Pereira, C.; Haddad, A.E.; Sheehy, L.; Finestone, H.; Mallet, K.; Wiseman, M.; Hour, K.; Flowers, H.L. Accuracy and effectiveness of teledentistry: A systematic review of systematic reviews. Evid.-Based Dent. 2022, 1–8. [Google Scholar] [CrossRef]
- Kim, K.; Shin, S.; Kim, S.; Lee, E. The relation between eHealth literacy and health-related behaviors: Systematic review and meta-analysis. J. Med. Internet Res. 2023, 25, e40778. [Google Scholar] [CrossRef]
- Walters, R.; Leslie, S.J.; Polson, R.; Cusack, T.; Gorely, T. Establishing the efficacy of interventions to improve health literacy and health behaviors: A systematic review. BMC Public Health 2020, 20, 1040. [Google Scholar] [CrossRef]
- Latulippe, K.; Hamel, C.; Giroux, D. Social health inequalities and eHealth: A literature review with qualitative synthesis of theoretical and empirical studies. J. Med. Internet Res. 2017, 19, e136. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Song, Y.; Zhu, Y.; Ji, H.; Wang, A. Association of eHealth literacy with health promotion behaviors of community-dwelling older people: The chain mediating role of self-efficacy and self-care ability. Int. J. Environ. Res. Public Health 2022, 19, 6092. [Google Scholar] [CrossRef]
- World Health Organization. Digital Education for Building Health Workforce Capacity; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Sharma, S.; Mohanty, V.; Balappanavar, A.Y.; Chahar, P.; Rijhwani, K.; Balappanavar, A. Role of digital media in promoting oral health: A systematic review. Cureus 2022, 14, e28893. [Google Scholar] [CrossRef] [PubMed]
- Bastani, P.; Manchery, N.; Samadbeik, M.; Ha, D.H.; Do, L.G. Digital Health in Children’s Oral and Dental Health: An Overview and a Bibliometric Analysis. Children 2022, 9, 1039. [Google Scholar] [CrossRef] [PubMed]
- El Benny, M.; Kabakian-Khasholian, T.; El-Jardali, F.; Bardus, M. Application of the eHealth literacy model in digital health interventions: Scoping review. J. Med. Internet Res. 2021, 23, e23473. [Google Scholar] [CrossRef] [PubMed]
- Pourrazavi, S.; Kouzekanani, K.; Bazargan-Hejazi, S.; Shaghaghi, A.; Hashemiparast, M.; Fathifar, Z.; Allahverdipour, H. Theory-based E-health literacy interventions in older adults: A systematic review. Arch. Public Health 2020, 78, 72. [Google Scholar] [CrossRef]
- Tossaint-Schoenmakers, R.; Versluis, A.; Chavannes, N.; Talboom-Kamp, E.; Kasteleyn, M. The challenge of integrating eHealth into health care: Systematic literature review of the Donabedian model of structure, process, and outcome. J. Med. Internet Res. 2021, 23, e27180. [Google Scholar] [CrossRef]
- World Health Organization. Mobile Technologies for Oral Health: An Implementation Guide; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Samorani, M.; Blount, L.G. Machine learning and medical appointment scheduling: Creating and perpetuating inequalities in access to health care. Am. Public Health Assoc. 2020, 110, 440–441. [Google Scholar] [CrossRef]
- Kumar, Y.; Koul, A.; Singla, R.; Ijaz, M.F. Artificial intelligence in disease diagnosis: A systematic literature review, synthesizing framework and future research agenda. J. Ambient Intell. Humaniz. Comput. 2022, 14, 8459–8486. [Google Scholar] [CrossRef]
- Sabbah, W.; Tsakos, G.; Sheiham, A.; Watt, R.G. The role of health-related behaviors in the socioeconomic disparities in oral health. Soc. Sci. Med. 2009, 68, 298–303. [Google Scholar] [CrossRef]
- Sun, Y.; Sun, J.; Zhao, Y.; Cheng, A.; Zhou, J. A new comprehensive oral health literacy scale: Development and psychometric evaluation. BMC Oral Health 2021, 21, 429. [Google Scholar] [CrossRef]


{kind=link}
| eHealth Literacy | ||||||
|---|---|---|---|---|---|---|
| Inadequate | Problematic | Sufficient | Total Sample | |||
| Variable | Category | n = 81 | n = 115 | n = 282 | n = 478 | p-Value |
| Age, mean (SD) | 36.8 (15.2) | 33.1 (11.3) | 30.6(10.8) | 31.9 (12.1) | 0.001 | |
| Gender, n (%) | Male | 65 (80.2) | 82 (71.3) | 171 (60.6) | 318 (66.5) | 0.002 |
| Female | 16(19.8) | 33 (28.7) | 111 (39.4) | 160 (33.5) | ||
| Education | No Education, n (%) | 4 (4.9) | 3 (2.6) | 2 (0.7) | 9 (1.9) | 0.001 |
| Less than 6 years, n (%) | 9 (11.1) | 5 (4.3) | 7 (2.5) | 21 (4.4) | ||
| 7–12 years, n (%) | 35 (43.2) | 50(43.5) | 100 (30.5) | 185 (38.7) | ||
| University or Higher, n (%) | 33 (40.7) | 57 (49.6) | 173 (61.3) | 263 (55.0) | ||
| Income | Less than 2500SR, n (%) | 42 (51.9) | 57 (49.6) | 155 (55.0) | 254 (53.1) | 0.623 |
| 2500–4999SR, n (%) | 13 (16.0) | 24 (20.9) | 37 (13.1) | 74 (15.5) | ||
| 5000–9999SR, n (%) | 14 (17.3) | 16 (13.9) | 41 (14.5) | 71 (14.9) | ||
| More than 10,000SR, n (%) | 12 (14.8) | 18 (15.7) | 49 (17.4) | 79 (16.5) | ||
| Number of teeth, mean (SD) | 22.6 (8.55) | 26.3 (5.8) | 27.6 (5.5) | 26.4 (6.5) | 0.001 | |
| Brushing frequency | Do not brush, n (%) | 22 (27.2) | 14 (12.2) | 10 (3.5) | 46 (9.6) | 0.001 |
| Brush once/day, n (%) | 34 (42.0) | 62 (53.9) | 127 (45.0) | 223 (46.7) | ||
| Brush twice/day, n (%) | 25 (30.9) | 39 (33.9) | 145 (51.4) | 209 (43.7) | ||
| Fully Adjusted Model | ||||
|---|---|---|---|---|
| Variable | RR | (95% CI) | p-Value | |
| Age | 0.99 | (0.98–0.99) | 0.000 | |
| Gender | Male | (Reference) | ||
| Female | 1.00 | (0.95–1.04) | 0.940 | |
| Health Literacy | Inadequate | (Reference) | ||
| Problematic | 1.12 | (1.05–1.20) | 0.000 | |
| Sufficient | 1.14 | (1.07–1.20) | 0.000 | |
| Income | Less than 25,005R | (Reference) | ||
| 2500–49,995R | 0.99 | (0.93–1.05) | 0.904 | |
| 5000–99,995R | 1.01 | (0.95–1.09) | 0.554 | |
| More than 100,005R | 1.02 | (0.96–1.09) | 0.469 | |
| Education | No Education | (Reference) | ||
| Less than 6 years | 0.96 | (0.80–1.14) | 0.608 | |
| 7–12 years | 0.97 | (0.83–1.12) | 0.648 | |
| University or Higher | 1.01 | (0.88–1.19) | 0.802 | |
| RR = Rate Ratio | ||||
| Fully Adjusted Model | ||||
|---|---|---|---|---|
| Variable | OR | (95% CI) | p-Value | |
| Age | 1.02 | (0.99–1.06) | 0.070 | |
| Gender | Male | (Reference) | ||
| Female | 1 | Empty * | Empty * | |
| Health Literacy | Inadequate | (Reference) | ||
| Problematic | 0.39 | (0.15–1.01) | 0.054 | |
| Sufficient | 0.24 | (0.95–0.62) | 0.003 | |
| Income | Less than 25,005R | (Reference) | ||
| 2500–49,995R | 4.14 | (1.62–10.52) | 0.003 | |
| 5000–99,995R | 1.31 | (0.41–4.22) | 0.640 | |
| More than 100,005R | 0.58 | (0.13–2.57) | 0.477 | |
| Education | No Education | (Reference) | ||
| Less than 6 years | 2.17 | (0.17–27.57) | 0.549 | |
| 7–12 years | 0.55 | (0.06–4.75) | 0.591 | |
| University or Higher | 0.18 | (0.19–1.71) | 0.136 | |
| OR = Odds ratio | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hakeem, F.F.; Abdouh, I.; Hamadallah, H.H.; Alarabi, Y.O.; Almuzaini, A.S.; Abdullah, M.M.; Altarjami, A.A. The Association between Electronic Health Literacy and Oral Health Outcomes among Dental Patients in Saudi Arabia: A Cross-Sectional Study. Healthcare 2023, 11, 1804. https://doi.org/10.3390/healthcare11121804
Hakeem FF, Abdouh I, Hamadallah HH, Alarabi YO, Almuzaini AS, Abdullah MM, Altarjami AA. The Association between Electronic Health Literacy and Oral Health Outcomes among Dental Patients in Saudi Arabia: A Cross-Sectional Study. Healthcare. 2023; 11(12):1804. https://doi.org/10.3390/healthcare11121804
Chicago/Turabian StyleHakeem, Faisal F., Ismail Abdouh, Hatem Hazzaa Hamadallah, Yunus Osama Alarabi, Abdulrahman Saad Almuzaini, Majed Maher Abdullah, and Ammar Abdulrahman Altarjami. 2023. "The Association between Electronic Health Literacy and Oral Health Outcomes among Dental Patients in Saudi Arabia: A Cross-Sectional Study" Healthcare 11, no. 12: 1804. https://doi.org/10.3390/healthcare11121804