
Computer-Based Intelligent Solutions for the Diagnosis of Gastroesophageal Reflux Disease Phenotypes and Chicago Classification 3.0

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GERD | Gastroesophageal Reflux Disease |
| CC 3.0 | Chicago Classification 3.0 |
| DSS | Decision Support System |
| AI | Artificial Intelligence |
| NERD | Non-erosive Reflux Disease |
| QoLRAD | Quality of Life in Reflux and Dyspepsia Questionnaire |
| SF-36 | Short Form-36 |
| RDQ | Reflux Disease Questionnaire |
| MMS | Medical Measurement Systems |
| PPI | Proton Pump Inhibitors |
References
- Kök, M.; Çekin, Y.; Çekin, A.H.; Uyar, S.; Harmandar, F.; Şahintürk, Y. The role of Blastocystis hominis in the activation of ulcerative colitis. Turk. J. Gastroenterol. 2019, 30, 40–46. [Google Scholar] [CrossRef]
- Bulut, E.A.; Törüner, M. The influence of disease type and activity to sexual life and health quality in inflammatory bowel disease. Turk. J. Gastroenterol. 2019, 30, 33–39. [Google Scholar] [CrossRef]
- Tongtawee, T.; Simawaranon, T.; Wattanawongdon, W.; Dechsukhum, C.; Leeanansaksiri, W. Toll-like receptor 2 and 4 polymorphisms associated with Helicobacter pylori susceptibility and gastric cancer. Turk. J. Gastroenterol. 2019, 30, 15–20. [Google Scholar] [CrossRef]
- Van Brunt, E.E. The Kaiser-Permanente medical information system. Comput. Biomed. Res. 1970, 3, 477–487. [Google Scholar] [CrossRef]
- Winter, A.; Haux, R.; Ammenwerth, E.; Brigl, B.; Hellrung, N.; Jahn, F. Health information systems. Health Inf. Syst. 2010, 1, 33–42. [Google Scholar] [CrossRef]
- Huff, S.M.; Craig, R.B.; Gould, B.L.; Castagno, D.L.; Smilan, R.E. A medical data dictionary for decision support applications. In Proceedings of the Annual Symposium on Computer Application in Medical Care, Washington, DC, USA, 4 November 1987; pp. 310–317. [Google Scholar]
- Farooqui, N.A.; Mehra, R. Design of a data warehouse for medical information system using data mining techniques. In Proceedings of the Fifth International Conference on Parallel, Distributed and Grid Computing, Solan, India, 20–22 December 2018; pp. 199–203. [Google Scholar] [CrossRef]
- Mishra, S.; Panda, M. Artificial intelligence in medical science. Intell. Syst. Healthc. Manag. Deliv. 2019, 1, 306–330. [Google Scholar] [CrossRef]
- Currie, G.; Hawk, K.E.; Rohren, E.; Vial, A.; Klein, R. Machine learning and deep learning in medical imaging: Intelligent imaging. J. Med. Imaging Radiat. Sci. 2019, 50, 477–487. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, S.; Singh, B.; Kumar, R.; Dey, N. Machine learning for medical diagnosis: A neural network classifier optimized via the directed bee colony optimization algorithm. U-Healthc. Monit. Syst. 2019, 1, 197–215. [Google Scholar] [CrossRef]
- Habermann, W.; Schmid, C.; Neumann, K.; DeVaney, T.; Hammer, H.F. Reflux symptom index and reflux finding score in otolaryngologic practice. J. Voice 2012, 26, 123–127. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Knill-Jones, R.P. Statistical and knowledge-based approaches to clinical decision-support systems, with an application in gastroenterology. J. R. Stat. Soc. Ser. A (Gen.) 1984, 147, 35–58. [Google Scholar] [CrossRef]
- Kuhn, K.; Gaus, W.; Wechsler, J.G.; Janowitz, P.; Tudyka, J.; Kratzer, W.; Swobodnik, W.; Ditschuneit, H. Structured reporting of medical findings: Evaluation of a system in gastroenterology. Methods Inf. Med. 1992, 31, 268–274. [Google Scholar] [CrossRef]
- Dormann, H.; Criegee-Rieck, M.; Neubert, A.; Egger, T.; Levy, M.; Hahn, E.G.; Brune, K. Implementation of a computer-assisted monitoring system for the detection of adverse drug reactions in gastroenterology. Aliment. Pharmacol. Ther. 2004, 19, 303–309. [Google Scholar] [CrossRef]
- Ruffle, J.K.; Farmer, A.D.; Aziz, Q. Artificial intelligence in gastroenterology. Precis. Med. Investig. Pract. Provid. 2020, 343–350. [Google Scholar] [CrossRef]
- Adadi, A.; Adadi, S.; Berrada, M. Gastroenterology meets machine learning: Status quo and quo vadis. Adv. Bioinform. 2019, 2019, 1870975. [Google Scholar] [CrossRef] [Green Version]
- Bor, S. Reflux esophagitis, functional and non-functional. Best Pract. Res. Clin. Gastroenterol. 2019, 40, 101649. [Google Scholar] [CrossRef]
- Bor, S.; Kalkan, İ.H.; Çelebi, A.; Dinçer, D.; Akyüz, F.; Dettmar, P.; Özen, H. Alginates: From the ocean to gastroesophageal reflux disease treatment. Turk. J. Gastroenterol. 2019, 30, 109–136. [Google Scholar] [CrossRef]
- Bor, S.; Mandiracioglu, A.; Kitapcioglu, G.; Caymaz, C.B.; Gilbert, R.J. Gastroesophageal reflux disease in a low-income region in Turkiye. Am. J. Gastroenterol. 2005, 100, 759–765. [Google Scholar] [CrossRef]
- Bossuyt, P.; Vermeire, S.; Ferrante, M.; Makino, T.; Bisschops, R. Automated real time endoscopic scoring based on machine learning in ulcerative colitis: Red density reliability and responsiveness study. Endoscopy 2019, 51, 80–81. [Google Scholar] [CrossRef]
- Shung, D.L.; Au, B.; Taylor, R.A.; Tay, J.K.; Laursen, S.B.; Stanley, A.J.; Dalton, H.R.; Ngu, J.; Schultz, M.; Laine, L. Validation of a machine learning model that outperforms clinical risk scoring systems for upper gastrointestinal bleeding. Gastroenterology 2020, 158, 160–167. [Google Scholar] [CrossRef]
- Ruffle, J.; Tinkler, L.; Emmett, C.; Aziz, Q.; Farmer, A.; Yiannakou, Y. PWE-097 Machine learning can accurately classify chronic constipation patients by symptom burden using pain measures alone. Gut 2019, 156, 590–591. [Google Scholar] [CrossRef]
- Guimarães, P.; Keller, A.; Fehlmann, T.; Lammert, F.; Casper, M. Deep-learning based detection of gastric precancerous conditions. Gut 2020, 69, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Song, E.M.; Park, B.; Ha, C.A.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Kim, N.; Byeon, J.S. Endoscopic diagnosis and treatment planning for colorectal polyps using a deep-learning model. Sci. Rep. 2020, 10, 30. [Google Scholar] [CrossRef] [Green Version]
- Danis, N.; Bor, S. Effect of advanced diagnosis modalities and disease phenotypes on PPI response of gastroesophageal reflux disease. Neurogastroenterol. Motil. 2018, 30. Available online: https://gcris.ege.edu.tr/handle/11454/30156 (accessed on 21 April 2023).
- Hançerlioğlu, S.; Yıldırım, Y.; Bor, S. Validity and reliability of the Quality of Life in Reflux and Dyspepsia (QoLRAD) questionnaire in patients with gastroesophageal reflux disease for the Turkish population. Turk. J. Gastroenterol. 2019, 30, 511–516. [Google Scholar] [CrossRef]
- Levine, M.E.; Albers, D.J.; Burgermaster, M.; Davidson, P.G.; Smaldone, A.M.; Mamykina, L. Behavioral-clinical phenotyping with type 2 diabetes self-monitoring data. arXiv 2018, arXiv:1802.08761. [Google Scholar] [CrossRef]
- Vandromme, M.; Jun, T.; Perumalswami, P.; Dudley, J.T.; Branch, A.; Li, L. Automated phenotyping of patients with non-alcoholic fatty liver disease reveals clinically relevant disease subtypes. In Proceedings of the Pacific Symposium Biocomputing, Kohala Coast, HI, USA, 3–7 January 2020; pp. 91–102. [Google Scholar] [CrossRef]
- Kahrilas, P.J.; Bredenoord, A.J.; Fox, M.; Gyawali, C.P.; Roman, S.; Smout, A.J.; Pandolfino, J.E. International High Resolution Manometry Working Group. Chic. Classif. Esophageal Motil. Disord. Neurogastroenterol. Motil. 2015, 27, 160–174. [Google Scholar] [CrossRef] [Green Version]
- Ge, Z.; Wang, B.; Chang, J.; Yu, Z.; Zhou, Z.; Zhang, J.; Duan, Z. Using deep learning and explainable artificial intelligence to assess the severity of gastroesophageal reflux disease according to the Los Angeles Classification System. Scand. J. Gastroenterol. 2023, 1–9. [Google Scholar] [CrossRef]
- Wong, M.W.; Liu, M.X.; Lei, W.Y.; Liu, T.T.; Yi, C.H.; Hung, J.S.; Liang, S.W.; Lin, L.; Tseng, C.W.; Wang, J.H.; et al. Artificial intelligence facilitates measuring reflux episodes and postreflux swallow-induced peristaltic wave index from impedance-pH studies in patients with reflux disease. Neurogastroenterol. Motil. 2023, 35, e14506. [Google Scholar] [CrossRef]
- Emile, S.H.; Ghareeb, W.; Elfeki, H.; El Sorogy, M.; Fouad, A.; Elrefai, M. Development and validation of an artificial intelligence-based model to predict gastroesophageal reflux disease after sleeve gastrectomy. Obes. Surg. 2022, 32, 2537–2547. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Questions | Total Answers | Total Entries | Total Amount of Data | |
|---|---|---|---|---|
| QoLRAD1 | 12 | 84 | 4276 | 48,917 |
| QoLRAD2 | 25 | 175 | 1723 | 38,800 |
| GERD Question Form 1 | 57 | 238 | 653 | 33,942 |
| GERD Question Form 2 | 66 | 353 | 5041 | 189,765 |
| GERD Question Form 3 | 81 | 444 | 1873 | 185,774 |
| SF-36 | 11 | 149 | 5399 | 119,252 |
| Otolaryngology Form (11) | 20 | 115 | 1446 | 21,196 |
| Otolaryngology Score (11) | 9 | 28 | 1602 | 10,603 |
| GERD Postoperative Symptoms Question Form | 22 | 96 | 156 | 2922 |
| RDQ | 2 | 72 | 82 | 906 |
| Eckardt Score | 5 | 17 | 10 | 50 |
| Total | 310 | 1771 | 22,261 | 613,715 |
| Erosive Esophagitis (EE) | Reflux Hypersensitivity (RH) | Functional Heartburn (FH) | Non-Erosive Reflux Disease (NR) | Total | |
|---|---|---|---|---|---|
| Male | 641 | 12 | 48 | 307 | 1008 |
| Female | 590 | 49 | 121 | 284 | 1044 |
| Age (10–19) | 18 | 4 | 2 | 10 | 34 |
| Age (20–29) | 119 | 8 | 18 | 60 | 205 |
| Age (30–39) | 271 | 19 | 42 | 127 | 459 |
| Age (40–49) | 298 | 13 | 49 | 149 | 509 |
| Age (50–59) | 299 | 13 | 37 | 144 | 493 |
| Age (60–69) | 169 | 3 | 19 | 77 | 268 |
| Age (70–90) | 57 | 1 | 2 | 24 | 84 |
| Total | 1231 (60%) | 61 (3%) | 169 (8%) | 591 (29%) | 2052 |
| Male | Female | Age < 40 | Age ≥ 40 | Total | |
|---|---|---|---|---|---|
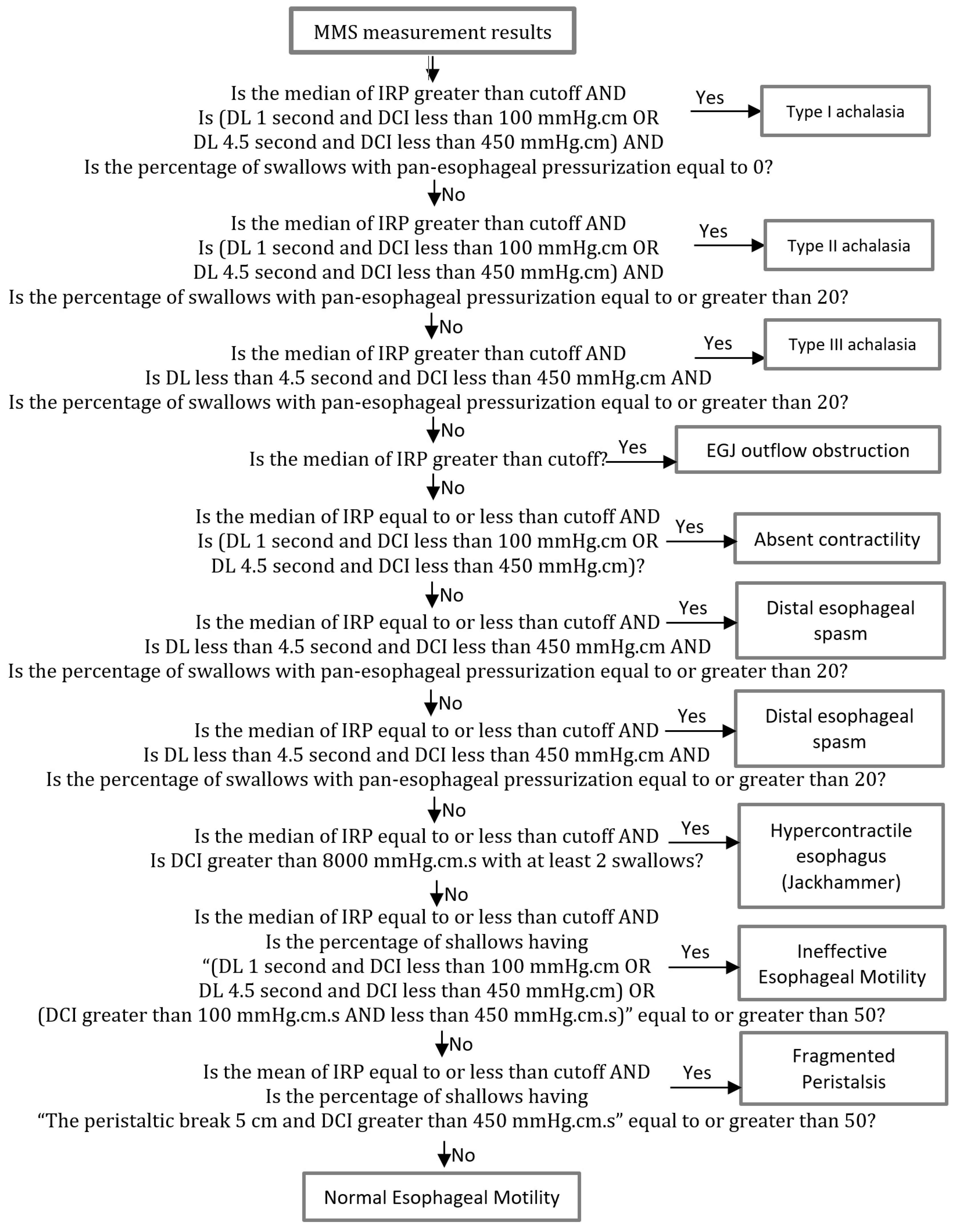
| Type I achalasia (classic achalasia) | 7 | 7 | 5 | 9 | 14 (11%) |
| Type II achalasia (with esophageal compression) | 10 | 21 | 10 | 21 | 31 (23%) |
| Type III achalasia (spastic achalasia) | 4 | 4 | 1 | 7 | 8 (6%) |
| EGJ outflow obstruction | 1 | 0 | 0 | 1 | 1 (1%) |
| Absent contractility | 4 | 4 | 2 | 6 | 8 (6%) |
| Distal esophageal spasm | 1 | 0 | 0 | 1 | 1 (1%) |
| Hypercontractile esophagus (jackhammer) | 5 | 4 | 0 | 9 | 9 (7%) |
| Ineffective esophageal motility | 37 | 23 | 29 | 31 | 60 (45%) |
| Fragmented peristalsis | 1 | 0 | 0 | 1 | 1 (1%) |
| Total | 70 | 63 | 47 | 86 | 133 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doğan, Y.; Bor, S. Computer-Based Intelligent Solutions for the Diagnosis of Gastroesophageal Reflux Disease Phenotypes and Chicago Classification 3.0. Healthcare 2023, 11, 1790. https://doi.org/10.3390/healthcare11121790
Doğan Y, Bor S. Computer-Based Intelligent Solutions for the Diagnosis of Gastroesophageal Reflux Disease Phenotypes and Chicago Classification 3.0. Healthcare. 2023; 11(12):1790. https://doi.org/10.3390/healthcare11121790
Chicago/Turabian StyleDoğan, Yunus, and Serhat Bor. 2023. "Computer-Based Intelligent Solutions for the Diagnosis of Gastroesophageal Reflux Disease Phenotypes and Chicago Classification 3.0" Healthcare 11, no. 12: 1790. https://doi.org/10.3390/healthcare11121790