Role of Tele-Physical Therapy Training on Glycemic Control, Pulmonary Function, Physical Fitness, and Health-Related Quality of Life in Patients with Type 2 Diabetes Mellitus (T2DM) Following COVID-19 Infection—A Randomized Controlled Trial


 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
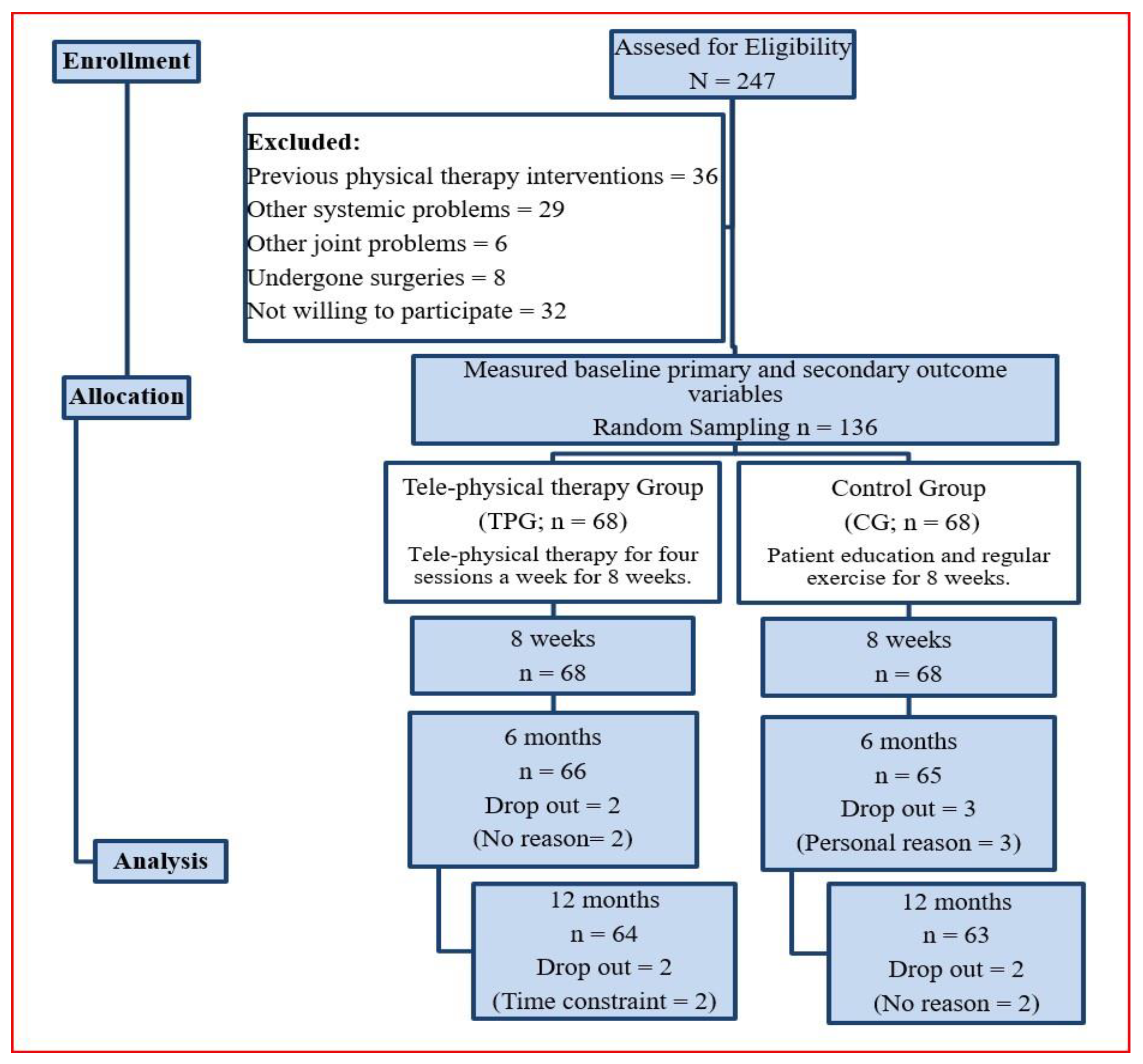
2.2. Participants
2.3. Randomization
2.4. Blinding
2.5. Intervention
2.6. Outcome Measures
2.6.1. Primary Outcome
2.6.2. Secondary Outcome
2.7. Sample Size
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2009, 32 (Suppl. S1), S62–S67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Economic costs of diabetes in the U.S. Diabetes Care 2008, 31, 596–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kivimäki, M.; Vahtera, J.; Pentti, J.; Virtanen, M.; Elovainio, M.; Hemingway, H. Increased sickness absence in diabetic employees: What is the role of co-morbid conditions? Diabet Med. 2007, 24, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fang, X.; Cai, Z.; Wu, X.; Gao, X.; Min, J.; Wang, F. Comorbid Chronic Diseases and Acute Organ Injuries Are Strongly Correlated with Disease Severity and Mortality among COVID-19 Patients: A Systemic Review and Meta-Analysis. Research 2020, 2020, 2402961. [Google Scholar] [CrossRef] [Green Version]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Hemmingsen, B.; Gimenez-Perez, G.; Mauricio, D.; Roqué I Figuls, M.; Metzendorf, M.I.; Richter, B. Diet, physical activity or both for prevention or delay of type 2 diabetes mellitus and its associated complications in people at increased risk of developing type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2017, 12, CD003054. [Google Scholar] [CrossRef] [Green Version]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Braun, B. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [Green Version]
- Forducey, P.G.; Ruwe, W.D.; Dawson, S.J.; Scheideman-Miller, C.; McDonald, N.B.; Hantla, M.R. Using telerehabilitation to promote TBI recovery and transfer of knowledge. Neuro. Rehabil. 2003, 18, 103–111. [Google Scholar] [CrossRef]
- McCue, M.; Fairman, A.; Pramuka, M. Enhancing quality of life through telerehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 195–205. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef]
- Duruturk, N.; Özköslü, M.A. Effect of tele-rehabilitation on glucose control, exercise capacity, physical fitness, muscle strength and psychosocial status in patients with type 2 diabetes: A double blind randomized controlled trial. Prim. Care Diabetes 2019, 13, 542–548. [Google Scholar] [CrossRef]
- Verhoeven, F.; van Gemert-Pijnen, L.; Dijkstra, K.; Nijland, N.; Seydel, E.; Steehouder, M. The contribution of teleconsultation and videoconferencing to diabetes care: A systematic literature review. J. Med. Internet Res. 2007, 9, e37. [Google Scholar] [CrossRef] [PubMed]
- Garfan, S.; Alamoodi, A.H.; Zaidan, B.B.; Al-Zobbi, M.; Hamid, R.A.; Alwan, J.K.; Momani, F. Telehealth utilization during the COVID-19 pandemic: A systematic review. Comput. Biol. Med. 2021, 138, 104878. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.C.; Nicolucci, A.; Di Bartolo, P.; Bruttomesso, D.; Girelli, A.; Ampudia, F.J.; Vespasiani, G. Diabetes Interactive Diary: A new telemedicine system enabling flexible diet and insulin therapy while improving quality of life: An open-label, international, multicenter, randomized study. Diabetes Care 2010, 33, 109–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstock, R.S.; Teresi, J.A.; Goland, R.; Palmas, W.; Eimicke, J.P. Glycemic control and health disparities in older ethnically diverse underserved adults with diabetes: Five-year results from the Informatics for Diabetes Education and Telemedicine (IDEATel) study. Diabetes Care 2011, 34, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mani, S.; Sharma, S.; Omar, B.; Paungmali, A.; Joseph, L. Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: A systematic review. J. Telemed. Telecare 2017, 23, 379–391. [Google Scholar] [CrossRef]
- Hwang, R.; Bruning, J.; Morris, N.; Mandrusiak, A.; Russell, T. A Systematic Review of the Effects of Telerehabilitation in Patients With Cardiopulmonary Diseases. J. Cardiopulm. Rehabil. Prev. 2015, 35, 380–389. [Google Scholar] [CrossRef] [Green Version]
- Khair, R.M.; Nwaneri, C.; Damico, R.L.; Kolb, T.; Hassoun, P.M.; Mathai, S.C. The Minimal Important Difference in Borg Dyspnea Score in Pulmonary Arterial Hypertension. Ann. Am. Thorac. Soc. 2016, 13, 842–849. [Google Scholar] [CrossRef] [Green Version]
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark. Insights 2016, 11, 95–104. [Google Scholar] [CrossRef]
- Fernández-Villar, A.; Represas-Represas, C.; Mouronte-Roibás, C.; Ramos-Hernández, C.; Priegue-Carrera, A.; Fernández-García, S.; López-Campos, J.L. Reliability and usefulness of spirometry performed during admission for COPD exacerbation. PLoS ONE 2018, 13, e0194983. [Google Scholar] [CrossRef]
- Lee, M.C. Validity of the 6-min walk test and step test for evaluation of cardio respiratory fitness in patients with type 2 diabetes mellitus. J. Exerc. Nutr. Biochem. 2018, 22, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Haddad, C.; Sacre, H.; Obeid, S.; Salameh, P.; Hallit, S. Validation of the Arabic version of the “12-item short-form health survey” (SF-12) in a sample of Lebanese adults. Arch. Public Health 2021, 79, 56. [Google Scholar] [CrossRef]
- Najafipour, F.; Mobasseri, M.; Yavari, A.; Nadrian, H.; Aliasgarzadeh, A.; Abbasi, N.M.; Niafar, M.; Gharamaleki, J.H.; Sadra, V. Effect of regular exercise training on changes in HbA1c, BMI and VO2max among patients with type 2 diabetes mellitus: An 8-year trial. BMJ Open Diabetes Res Care. 2017, 5, e000414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishna, S.; Boren, S.A. Diabetes self-management care via cell phone: A systematic review. J. Diabetes Sci. Technol. 2008, 2, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Balducci, S.; Zanuso, S.; Cardelli, P.; Salvi, L.; Mazzitelli, G.; Bazuro, A. Changes in physical fitness predict improvements in modifiable cardiovascular risk factors independently of body weight loss in subjects with type 2 diabetes participating in the Italian Diabetes and Exercise Study (IDES). Diabetes Care 2012, 35, 1347–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maillard, F.; Rousset, S.; Pereira, B.; Traore, A.; Del Amaze, P.D.P.; Boirie, Y.; Boisseau, N. High-intensity interval training reduces abdominal fat mass in postmenopausal women with type 2 diabetes. Diabetes Metab. 2016, 42, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, P.; Li, N.; Wang, Z.; Li, J.; Liu, X.; Wu, W. Effects of Home-Based Breathing Exercises in Subjects With COPD. Respir. Care 2020, 65, 377–387. [Google Scholar] [CrossRef]
- Kokkinos, P.; Myers, J.; Nylen, E.; Panagiotakos, D.B.; Manolis, A.; Pittaras, A.; Singh, S. Exercise capacity and all-cause mortality in African American and Caucasian men with type 2 diabetes. Diabetes Care 2009, 32, 623–628. [Google Scholar] [CrossRef] [Green Version]
- Kolt, G.S.; Schofield, G.M.; Kerse, N.; Garrett, N.; Oliver, M. Effect of telephone counseling on physical activity for low-active older people in primary care: A randomized, controlled trial. J. Am. Geriatr. Soc. 2007, 55, 986–992. [Google Scholar] [CrossRef]
- Cox, N.; Corso, S.D.; McDonald, C.; Hill, C.; O’Halloran, P.; Macdonald, H.; Zanaboni, P.; Alison, J.; Hansen, H.; Holland, A. Telerehabilitation for chronic respiratory disease. Cochrane Database Syst. Rev. 2021, 1, CD013040. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Baranowski, R.; Bilinska, M.; Stepnowska, M.; Piotrowska, M.; Wójcik, A.; Piotrowicz, R. A new model of home-based telemonitored cardiac rehabilitation in patients with heart failure: Effectiveness, quality of life, and adherence. Eur. J. Heart Fail. 2010, 12, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Klonoff, D.C. Using telemedicine to improve outcomes in diabetes--an emerging technology. J. Diabetes Sci. Technol. 2009, 3, 624–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lysy, Z.; Da Costa, D.; Dasgupta, K. The association of physical activity and depression in Type 2 diabetes. Diabet. Med. 2008, 25, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Economic Costs of Diabetes in the U.S. in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Exercise Type | Description | Duration | Intensity | Frequency |
|---|---|---|---|---|
| Breathing exercise | Diaphragmatic breathing exercise: Step 1: The patient sits down on a chair and relaxes the upper chest and shoulders. Both hands are positioned on the abdomen. The patient should breathe slowly and deeply. Upon inhaling and exhaling, the hands should be felt to move out and in. Step 2: The patient breathes slowly and deeply from the diaphragm and upon inhaling maintains pressure with the hands to provide resistance on the abdomen. | Total: 10 min 4 min plus 1 min break between sets. | 12 reps/set for 2 sets. | 4 sessions per week for 8 weeks. |
| Aerobic exercise | Moderate intensity aerobic exercises: Brisk walking or running outside near home or on a treadmill at home with warm up comprising walking at regular speed and cool down comprising seated muscle stretching exercises. | Total: 30 min 20 min plus 5 min warm up and 5 min cool down. | Target heart rate (THR): 40–60% | 4 sessions per week for 8 weeks. |
| Resistance exercise | Supine position:
| Total: 40 min 2 min each exercise. 30 min plus 5 min warm up and 5 min cool down. | 1–2 weeks: 10–15 repetitions. 3–4 weeks: 15–20 repetitions. 5–6 weeks: 20–25 repetitions. 7–8 weeks: 25–30 repetitions. 2 sets with 30 s break. | 4 sessions per week for 8 weeks. |
| Sr. No | Variable | TPG (n = 68) | CG (n = 68) | p-Value | |
|---|---|---|---|---|---|
| 1 | Age (year) | - | 48.6 ± 4.2 | 47.8 ± 4.5 | 0.285 * |
| 2 | Gender | Male | 33 (49%) | 32 (47%) | - |
| Female | 35 (51%) | 36 (53%) | - | ||
| 3 | Height (cm) | - | 165.2 ± 4.2 | 166.3 ± 3.9 | 0.115 * |
| 4 | Weight (kg) | - | 77.89 ± 4.3 | 78.01 ± 4.2 | 0.869 * |
| 5 | BMI (kg/m2) | - | 24.2 ± 2.13 | 24.4 ± 2.32 | 0.601 * |
| 6 | HbA1c (%) | - | 7.52 ± 0.86 | 7.48 ± 0.91 | 0.792 * |
| 7 | Blood pressure (mm/Hg) | Systolic | 128.2 ± 7.21 | 127.2 ± 7.55 | 0.431 * |
| 8 | Diastolic | 91.2 ± 5.32 | 92.0 ± 5.64 | 0.396 * | |
| 9 | Disease duration (years) | - | 7.84 ± 0.92 | 7.92 ± 0.89 | 0.607 * |
| 10 | Disease severity | Severe | 8 (12%) | 10 (15%) | - |
| Non-severe | 60 (88%) | 58 (85%) | - | ||
| 11 | Co-morbidity | Heart disease | 6 (9%) | 5 (7%) | - |
| Hypertension | 23 (34%) | 18 (26%) | - | ||
| Obesity | 12 (18%) | 9 (13%) | - | ||
| Lung disease | 5 (7%) | 3 (4%) | - | ||
| Other problems | 9 (13%) | 6 (9%) | - | ||
| 12 | Smoking | Yes | 22 (32%) | 24 (35%) | - |
| No | 46 (68%) | 44 (65%) | - | ||
| 13 | Medications | Yes | 48 (71%) | 51 (75%) | - |
| No | 20 (29%) | 17 (25%) | - | ||
| 14 | Insulin | Yes | 18 (26%) | 15 (22%) | - |
| No | 50 (74%) | 53 (78%) | - |
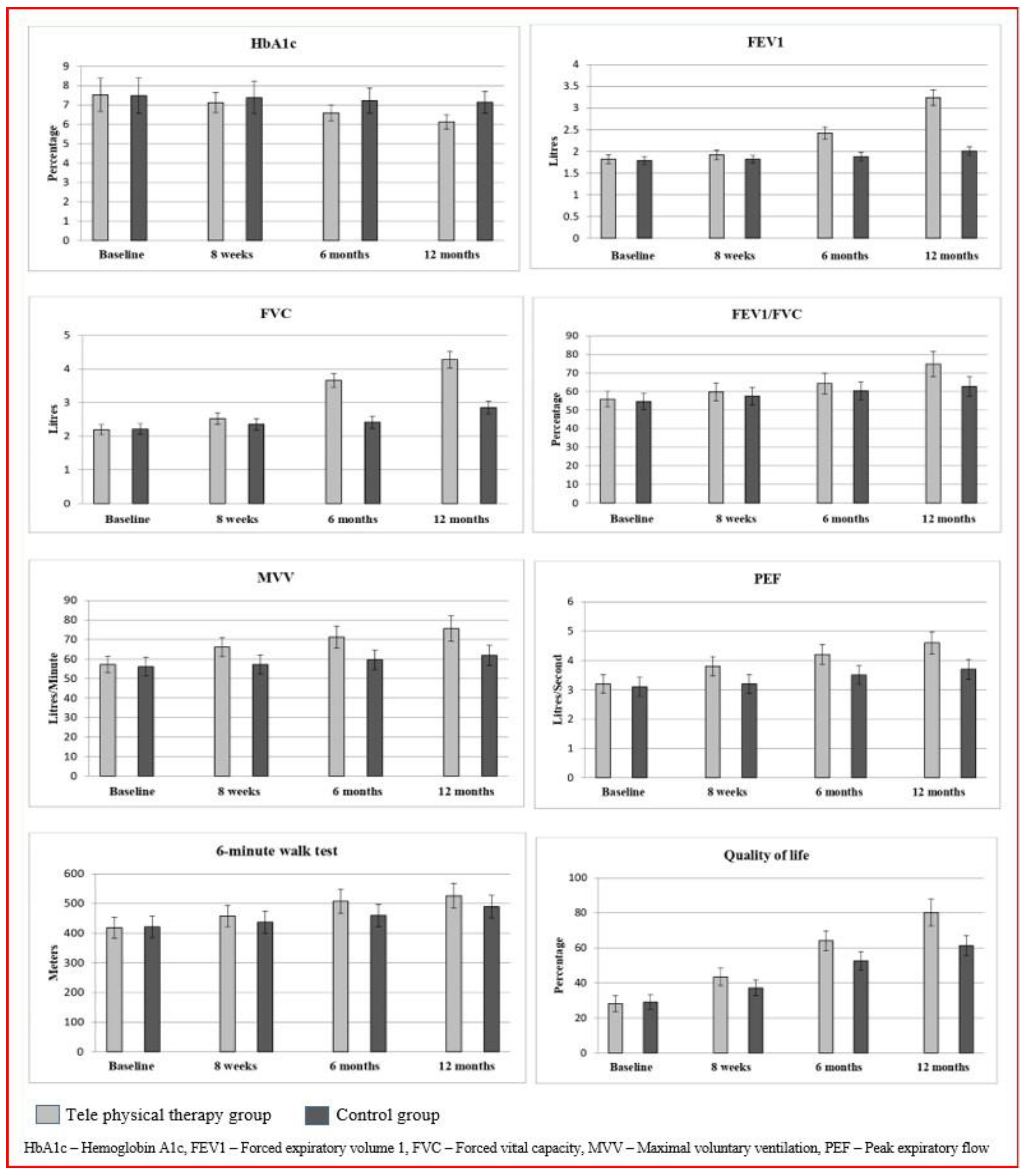
| Sr. No | Variable | TPG (n = 68) | CG (n = 68) | p-Value | |
|---|---|---|---|---|---|
| 1 | HbA1c (Percentage) | Base line | 7.52 ± 0.86 | 7.48 ± 0.91 | 0.792 * |
| 8 weeks | 7.12 ± 0.52 | 7.38 ± 0.84 | 0.031 | ||
| 6 months | 6.59 ± 0.41 | 7.22 ± 0.65 | 0.001 | ||
| 12 months | 6.12 ± 0.36 | 7.14 ± 0.56 | 0.001 | ||
| p-value | 0.001 | 0.001 | |||
| 2 | FEV1 (liters) | Base line | 1.82 ± 0.10 | 1.79 ± 0.09 | 0.068 * |
| 8 weeks | 1.92 ± 0.11 | 1.82 ± 0.09 | 0.001 | ||
| 6 months | 2.42 ± 0.14 | 1.88 ± 0.10 | 0.001 | ||
| 12 months | 3.24 ± 0.18 | 2.01 ± 0.10 | 0.001 | ||
| p-value | 0.001 | 0.001 | |||
| 3 | FVC (liters) | Base line | 2.19 ± 0.15 | 2.21 ± 0.16 | 0.453 * |
| 8 weeks | 2.52 ± 0.17 | 2.35 ± 0.17 | 0.001 | ||
| 6 months | 3.66 ± 0.21 | 2.41 ± 0.18 | 0.001 | ||
| 12 months | 4.28 ± 0.25 | 2.85 ± 0.19 | 0.001 | ||
| p-value | 0.001 | 0.001 | |||
| 4 | FEV1/FVC (Percentage) | Base line | 55.9 ± 4.2 | 54.6 ± 4.4 | 0.080 * |
| 8 weeks | 59.8 ± 4.8 | 57.5 ± 4.7 | 0.005 | ||
| 6 months | 64.3 ± 5.6 | 60.3 ± 4.9 | 0.001 | ||
| 12 months | 74.8 ± 6.8 | 62.7 ± 5.2 | 0.001 | ||
| p-value | 0.001 | 0.001 | |||
| 5 | MVV (liters/minute) | Base line | 57.2 ± 4.21 | 56.1 ± 4.81 | 0.158 * |
| 8 weeks | 66.1 ± 4.89 | 57.2 ± 4.92 | 0.001 | ||
| 6 months | 71.2 ± 5.63 | 59.6 ± 5.05 | 0.001 | ||
| 12 months | 75.6 ± 6.45 | 61.9 ± 5.21 | 0.001 | ||
| p-value | 0.001 | 0.001 | |||
| 6 | PEF (liters/second) | Base line | 3.2 ± 0.31 | 3.1 ± 0.32 | 0.066 * |
| 8 weeks | 3.8 ± 0.32 | 3.2 ± 0.32 | 0.001 | ||
| 6 months | 4.2 ± 0.34 | 3.5 ± 0.32 | 0.001 | ||
| 12 months | 4.6 ± 0.38 | 3.7 ± 0.34 | 0.001 | ||
| p-value | 0.001 | 0.001 | |||
| 7 | 6-min walk test (meters) | Base line | 418.18 ± 35.4 | 421.12 ± 36.3 | 0.633 * |
| 8 weeks | 457.44 ± 36.7 | 436.98 ± 37.4 | 0.015 | ||
| 6 months | 507.31 ± 40.2 | 459.79 ± 37.9 | 0.000 | ||
| 12 months | 526.28 ± 42.3 | 489.22 ± 38.1 | 0.000 | ||
| p-value | 0.001 | 0.001 | |||
| 8 | Quality of life (SF-12) | Base line | 28.2 ± 4.5 | 29.1 ± 4.1 | 0.224 * |
| 8 weeks | 43.4 ± 4.9 | 37.2 ± 4.5 | 0.001 | ||
| 6 months | 64.1 ± 5.7 | 52.5 ± 5.4 | 0.001 | ||
| 12 months | 80.2 ± 7.6 | 61.3 ± 5.7 | 0.001 | ||
| p-value | 0.001 | 0.001 |
| Variable/Time | Baseline | 8 Weeks | 6 Months | 12 Months | |
|---|---|---|---|---|---|
| Mean Difference CI95% (Upper Limit—Lower Limit) | |||||
| HbA1c | TPG × CG | −0.04 (−0.34 to 0.26) | 0.26 (0.02 to 0.49) | 0.63 (0.43 to 0.82) | 1.02 (0.86 to 1.17) |
| p-value | 0.7928 * | 0.031 | 0.001 | 0.001 | |
| FEV1 | TPG × CG | −0.03 (−0.06 to 0.00) | −0.1 (−0.13 to −0.06) | −0.5 (−0.58 to −0.49) | −1.7 (−3.84 to 0.44) |
| p-value | 0.068 * | 0.001 | 0.001 | 0.119 * | |
| FVC | TPG × CG | 0.02 (−0.03 to 0.07) | −0.17 (−0.22 to −0.11) | −1.25 (−1.31 to −1.18) | −1.43 (−1.50 to −1.34) |
| p-value | 0.453 * | 0.001 | 0.001 | 0.001 | |
| FEV1/FVC | TPG × CG | −1.3 (−2.75 to 0.15) | −2.3 (−3.91 to −0.68) | −4.0 (−5.78 to −2.21) | −12.1 (−14.15 to −10.04) |
| p-value | 0.080 * | 0.005 | 0.001 | 0.001 | |
| MVV | TPG × CG | −1.1 (−2.63 to 0.43) | −8.9 (−10.56 to −7.23) | −11.6 (−13.4 to −9.78) | −13.7 (−15.53 to −11.86) |
| p-value | 0.158 * | 0.001 | 0.001 | 0.001 | |
| PEF | TPG × CG | −0.1 (−0.20 to 0.00) | −0.6 (−0.70 to −0.49) | −0.7 (−0.81 to −0.58) | −0.9 (−1.02 to −0.77) |
| p-value | 0.066 * | 0.001 | 0.001 | 0.001 | |
| 6-min walk test | TPG × CG | 2.94 (−9.2 to 15.1) | −20.4 (−33.0 to −7.8) | −47.5 (−60.7 to −34.2) | −37.0 (−50.7 to −23.4) |
| p-value | 0.633 * | 0.004 | 0.001 | 0.001 | |
| Quality of life | TPG × CG | 0.9 (−0.56 to 2.36) | −6.2 (−7.79 to −4.60) | −11.6 (−13.4 to −9.7) | −18.9 (−21.17 to −16.62) |
| p-value | 0.224 * | 0.002 | 0.001 | 0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nambi, G.; Alghadier, M.; Vellaiyan, A.; Ebrahim, E.E.; Aldhafian, O.R.; Mohamed, S.H.P.; Albalawi, H.F.A.; Chevidikunnan, M.F.; Khan, F.; Mani, P.; et al. Role of Tele-Physical Therapy Training on Glycemic Control, Pulmonary Function, Physical Fitness, and Health-Related Quality of Life in Patients with Type 2 Diabetes Mellitus (T2DM) Following COVID-19 Infection—A Randomized Controlled Trial. Healthcare 2023, 11, 1791. https://doi.org/10.3390/healthcare11121791
Nambi G, Alghadier M, Vellaiyan A, Ebrahim EE, Aldhafian OR, Mohamed SHP, Albalawi HFA, Chevidikunnan MF, Khan F, Mani P, et al. Role of Tele-Physical Therapy Training on Glycemic Control, Pulmonary Function, Physical Fitness, and Health-Related Quality of Life in Patients with Type 2 Diabetes Mellitus (T2DM) Following COVID-19 Infection—A Randomized Controlled Trial. Healthcare. 2023; 11(12):1791. https://doi.org/10.3390/healthcare11121791
Chicago/Turabian StyleNambi, Gopal, Mshari Alghadier, Arul Vellaiyan, Elturabi Elsayed Ebrahim, Osama R. Aldhafian, Shahul Hameed Pakkir Mohamed, Hani Fahad Ateeq Albalawi, Mohamed Faisal Chevidikunnan, Fayaz Khan, Paramasivan Mani, and et al. 2023. "Role of Tele-Physical Therapy Training on Glycemic Control, Pulmonary Function, Physical Fitness, and Health-Related Quality of Life in Patients with Type 2 Diabetes Mellitus (T2DM) Following COVID-19 Infection—A Randomized Controlled Trial" Healthcare 11, no. 12: 1791. https://doi.org/10.3390/healthcare11121791