
The Effect of Kinesio Taping on Balance and Dynamic Stability in College-Age Recreational Runners with Ankle Instability
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Interventions
2.3.1. Kinesio Taping
2.3.2. The Standard Exercise Program
- The board was rocked forward and backward.
- The board was rocked from side to side.
- Then, with the feet wide apart, the board was rocked in a circulating movement.
- Stages 1–3 were repeated, but with the knees slightly bent and the hands on the buttocks.
- 5.
- The participants stood on their injured legs and kept the board level for 10 s.
- 6.
- If, in stage 5, the participant could maintain their balance without losing the stability of the board, then stage 5 was repeated with the eyes closed.
2.4. Outcomes
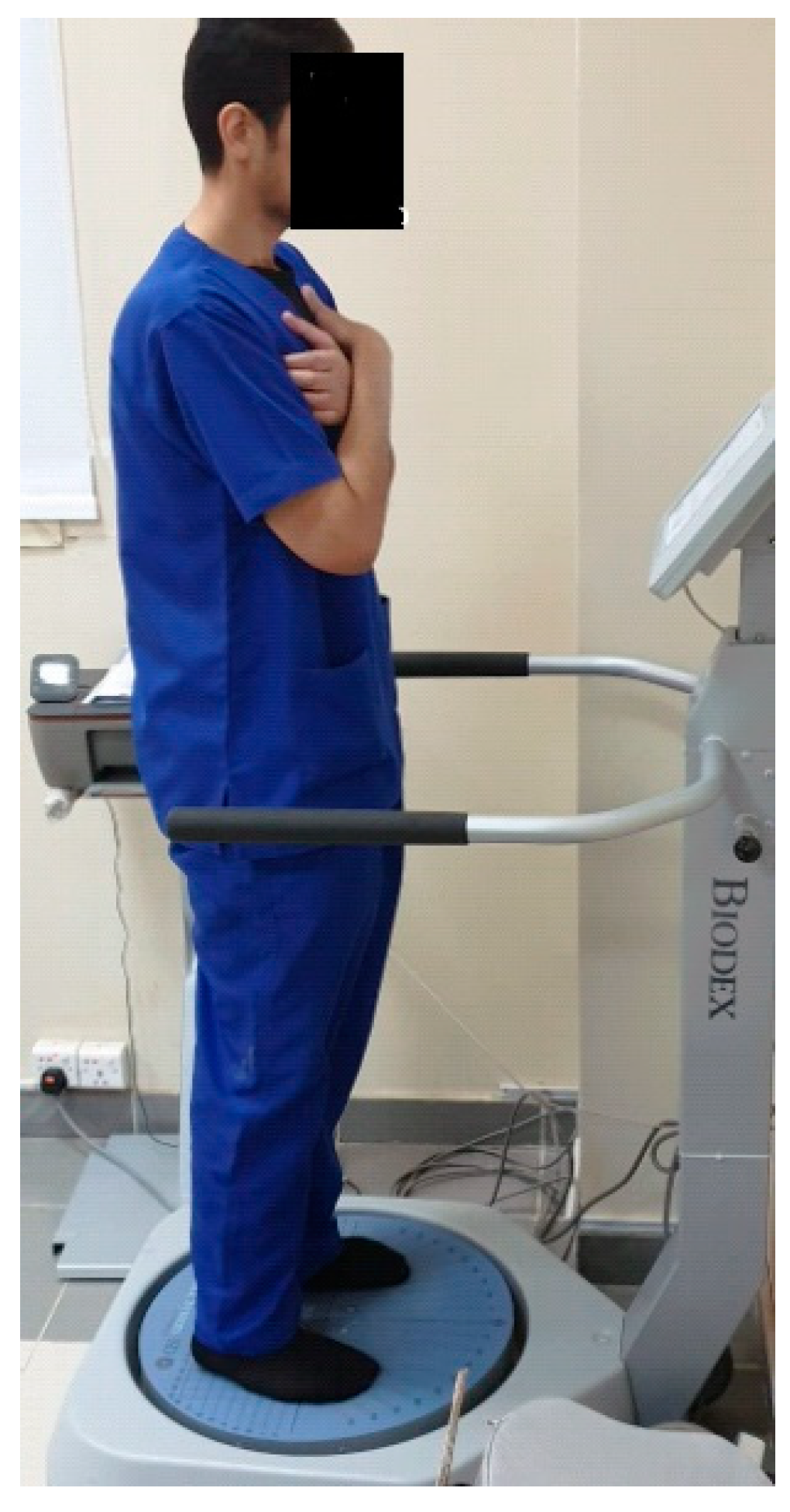
2.4.1. Postural Stability Assessment
2.4.2. Star Excursion Balance Test (SEBT)
2.5. Sample Size
2.6. Randomization
2.7. Allocation
2.8. Blinding
2.9. Statistical Methods
3. Results
3.1. Postural Indices Results
3.2. Dynamic Stability Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, D.C.; Pate, R.R.; Lavie, C.J.; Sui, X.; Church, T.S.; Blair, S.N. Leisure-time running reduces all-cause and cardiovascular mortality risk. J. Am. Coll. Cardiol. 2014, 64, 472–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hespanhol Junior, L.C.; Pena Costa, L.O.; Lopes, A.D. Previous injuries and some training characteristics predict running-related injuries in recreational runners: A prospective cohort study. J. Physiother. 2013, 59, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.; Brellenthin, A.G.; Thompson, P.D.; Sui, X.; Lee, I.-M.; Lavie, C.J. Running as a key lifestyle medicine for longevity. Prog. Cardiovasc. Dis. 2017, 60, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Junior, L.C.H.; Pillay, J.D.; van Mechelen, W.; Verhagen, E. Meta-analyses of the effects of habitual running on indices of health in physically inactive adults. Sport. Med. 2015, 45, 1455–1468. [Google Scholar] [CrossRef] [Green Version]
- Ellapen, T.J.; Satyendra, S.; Morris, J.; Van Heerden, H.J. Common running musculoskeletal injuries among recreational half-marathon runners in KwaZulu-Natal. S. Afr. J. Sport. Med. 2013, 25, 39–43. [Google Scholar] [CrossRef] [Green Version]
- Kluitenberg, B.; van Middelkoop, M.; Diercks, R.; van der Worp, H. What are the differences in injury proportions between different populations of runners? A systematic review and meta-analysis. Sport. Med. 2015, 45, 1143–1161. [Google Scholar] [CrossRef] [Green Version]
- Tonoli, C.; Cumps, E.; Aerts, I.; Verhagen, E.; Meeusen, R. Running related injuries in long-distance running: Incidence, risk factors and prevention. Sport Geneeskd. 2010, 43, 12. [Google Scholar] [CrossRef]
- Ziaei Ziabari, E.; Lubberts, B.; Chiou, D.; Razi, M.; Haghpanahi, M.; Ashkani-Esfahani, S.; DiGiovanni, C.W. Biomechanics Following Anatomic Lateral Ligament Repair of Chronic Ankle Instability: A Systematic Review. J. Foot Ankle Surg. 2021, 60, 762–769. [Google Scholar] [CrossRef]
- Lin, C.-I.; Houtenbos, S.; Lu, Y.-H.; Mayer, F.; Wippert, P.-M. The epidemiology of chronic ankle instability with perceived ankle instability—A systematic review. J. Foot Ankle Res. 2021, 14, 41–52. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, S.H.; Choi, G.W.; Jung, H.W.; Jang, W.Y. Individuals with recurrent ankle sprain demonstrate postural instability and neuromuscular control deficits in unaffected side. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 184–192. [Google Scholar] [CrossRef]
- Vaugoyeau, M.; Viel, S.; Amblard, B.; Azulay, J.P.; Assaiante, C. Proprioceptive contribution of postural control as assessed from very slow oscillations of the support in healthy humans. Gait Posture 2008, 27, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Pavailler, S.; Hintzy, F.; Horvais, N.; Forestier, N. Cutaneous stimulation at the ankle: A differential effect on proprioceptive postural control according to the participants’ preferred sensory strategy. J. Foot Ankle Res. 2016, 9, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, B.M.; Kosik, K.B.; Bain, K.A.; Houston, M.N.; Hoch, M.C.; Gribble, P.; Hoch, J.M. Exploratory factor analysis of the fear-avoidance beliefs questionnaire in patients with chronic ankle instability. Foot 2022, 51, 101902. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, R.; Abdollahi Khorasgani, M.; Tabatabaei, M.; Grampurohit, N. Effects of Elastic Therapeutic Taping on Joint Position Sense of the Ankle in Stroke Survivors. Am. J. Phys. Med. Rehabil. 2019, 98, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Qin, R.; Tan, Y.; Liu, H.; Wang, K.; Cheng, L. Effect of kinesio taping intervention on the muscle strength and balance of college basketball players with functional ankle instability. Front. Physiol. 2023, 14, 496. [Google Scholar] [CrossRef]
- Doğan, E.; Erail, S.; Mayda, M.H.; Yılmaz, C.; Karaduman, E.; Yılmaz, A.K.; Bayram, L.; Keskin, D.Ö.Y.; Ermiş, E. Acute effects of reverse kinesio taping on anaerobic performance in healthy subjects: A pilot study. Prog. Nutr. 2021, 23, 1–7. [Google Scholar] [CrossRef]
- do Carmo Silva Parreira, P.; da Cunha Menezes Costa, L.; Junior, L.C.H.; Lopes, A.D.; Costa, L.O.P. Current evidence does not support the use of Kinesio Taping in clinical practice: A systematic review. J. Physiother. 2014, 60, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Griebert, M.C.; Needle, A.R.; McConnell, J.; Kaminski, T.W. Lower-leg Kinesio tape reduces rate of loading in participants with medial tibial stress syndrome. Phys. Ther. Sport 2016, 18, 62–67. [Google Scholar] [CrossRef]
- Fereydounnia, S.; Shadmehr, A.; Moghadam, B.A.; Moghadam, S.T.; Mir, S.M.; Salemi, S.; Pourkazemi, F. Improvements in strength and functional performance after Kinesio taping in semi-professional male soccer players with and without functional ankle instability. Foot 2019, 41, 12–18. [Google Scholar] [CrossRef]
- Hadadi, M.; Haghighat, F.; Sobhani, S. Can fibular reposition taping improve balance performance in individuals with chronic ankle instability? A randomized controlled trial. Musculoskelet. Sci. Pract. 2020, 46, 102128. [Google Scholar] [CrossRef]
- Ramskov, D.; Nielsen, R.O.; Sørensen, H.; Parner, E.; Lind, M.; Rasmussen, S. The design of the run Clever randomized trial: Running volume,− intensity and running-related injuries. BMC Musculoskelet. Disord. 2016, 17, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korakakis, V.; Abassi, M.; Kotsifak, A.; Manai, H.; AbuEsba, A. Cross-cultural adaptation and psychometric properties’ evaluation of the modern standard Arabic version of Cumberland Ankle Instability Tool (CAIT) in professional athletes. PLoS ONE 2019, 14, e0217987. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.A.; Radwan, N.L.; Shimaa, A.; Azab, R. Effect of kinesio-taping on ankle joint stability. Int. J. Med. Res. Health Sci. 2016, 5, 51–58. [Google Scholar]
- Clark, V.M.; Burden, A.M. A 4-week wobble board exercise programme improved muscle onset latency and perceived stability in individuals with a functionally unstable ankle. Phys. Ther. Sport 2005, 6, 181–187. [Google Scholar] [CrossRef]
- Dawson, N.; Dzurino, D.; Karleskint, M.; Tucker, J. Examining the reliability, correlation, and validity of commonly used assessment tools to measure balance. Health Sci. Rep. 2018, 1, e98. [Google Scholar] [CrossRef]
- Testerman, C.; Vander Griend, R. Evaluation of ankle instability using the biodex stability system. Foot Ankle Int. 1999, 20, 317–321. [Google Scholar] [CrossRef]
- Hussein, H.M. Postural indices and limits of stability in subjects having chronic low back pain versus healthy control: A cross-sectional comparative study. Rehabil. Med. 2021, 25, 13–17. [Google Scholar] [CrossRef]
- Hertel, J.; Braham, R.A.; Hale, S.A.; Olmsted-Kramer, L.C. Simplifying the star excursion balance test: Analyses of subjects with and without chronic ankle instability. J. Orthop. Sport. Phys. Ther. 2006, 36, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Gribble, P.A.; Hertel, J.; Plisky, P. Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: A literature and systematic review. J. Athl. Train. 2012, 47, 339–357. [Google Scholar] [CrossRef] [Green Version]
- Wilson, B.; Bialocerkowski, A. The Effects of Kinesiotape Applied to the Lateral Aspect of the Ankle: Relevance to Ankle Sprains—A Systematic Review. PLoS ONE 2015, 10, e0124214. [Google Scholar] [CrossRef] [Green Version]
- Kulig, K.; Lee, S.P.; Reischl, S.F.; Noceti-DeWit, L. Effect of posterior tibial tendon dysfunction on unipedal standing balance test. Foot Ankle Int. 2015, 36, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Yam, M.L.; Yang, Z.; Zee, B.C.Y.; Chong, K.C. Effects of Kinesio tape on lower limb muscle strength, hop test, and vertical jump performances: A meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 212. [Google Scholar] [CrossRef] [PubMed]
- Do Seo, H.; Kim, M.Y.; Choi, J.E.; Lim, G.H.; Jung, S.I.; Park, S.H.; Cheon, S.H.; Lee, H.Y. Effects of kinesio taping on joint position sense of the ankle. J. Phys. Ther. Sci. 2016, 28, 1158–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.C.; Kim, J.H.; Nam, D.; Park, G.C.; Lee, J.S. Add-on effect of kinesiotape in patients with acute lateral ankle sprain: A randomized controlled trial. Trials 2020, 21, 176. [Google Scholar] [CrossRef] [Green Version]
- Stocco, M.R.; Del Antonio, A.C.F.T.; de Oliveira, R.G.; Jassi, F.J.; Del Antonio, T.T.; Andraus, R.A.C. Progressive tension protocol for muscle strength with Kinesio tape in runners—Double-blind randomized clinical trial. Fisioter. Mov. 2023, 36, e36104. [Google Scholar] [CrossRef]
- Siu, W.S.; Shih, Y.F.; Lin, H.C. Effects of Kinesio tape on supporting medial foot arch in runners with functional flatfoot: A preliminary study. Res. Sport. Med. 2020, 28, 168–180. [Google Scholar] [CrossRef]
- Lim, J.; Kim, S.; Moon, I.; Yi, C. The Effects of Elastic Ankle Taping on Static and Dynamic Postural Control in Individuals With Chronic Ankle Instability. Phys. Ther. Korea 2021, 28, 200–207. [Google Scholar] [CrossRef]
- Khalili, S.M.; Barati, A.H.; Oliveira, R.; Nobari, H. Effect of Combined Balance Exercises and Kinesio Taping on Balance, Postural Stability, and Severity of Ankle Instability in Female Athletes with Functional Ankle Instability. Life 2022, 12, 178. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | KTG n = 29 | MG n = 30 | EG n = 29 | p |
|---|---|---|---|---|
| Mean ± SD. | Mean ± SD. | Mean ± SD. | ||
| Age (years) | 32.69 ± 7.13 | 29.27 ± 8.65 | 31.87 ± 7.79 | >0.05 |
| Weight (kg) | 62.0 ± 10.81 | 61.6 ± 5.96 | 62.6 ± 6.85 | |
| Height (cm) | 159.7 ± 3.47 | 159.53 ± 6.01 | 156 ± 5.91 | |
| BMI | 24.30 ± 4.20 | 24.28 ± 2.97 | 25.78 ± 3.16 | |
| CAIT | 25.8 ± 1.47 | 25.4 ± 1.63 | 24.9 ± 1.74 | |
| Male/female n (%) | 25(86.2)/4(13.8) | 24(80)/6(20) | 24(82.7)/5(17.3) | |
| Rt (%)/Lt (%) dominance | 25(86.2)/4(13.8) | 25(83.3)/5(16.6) | 28(96.6)/1(3.4) |
| KTG n = 29 | MG n = 30 | EG n = 29 | ARMS (p and Cohen’s d) | ||
|---|---|---|---|---|---|
| Mean ± SD. | Mean ± SD. | Mean ± SD. | |||
| OSI | Pre | 0.35 ± 0.14 | 0.42 ± 0.19 | 0.38 ± 0.22 | KTG-MG: 0.113 (0.70) KTG-EG: 0.19 (0.45) MG-EG: 0.777 (0.17) |
| Post | 0.14 ± 0.05 | 0.23 ± 0.05 | 0.30 ± 0.12 | KTG-MG: 0.015 * (1.60) KTG-EG: 0.000 * (1.63) MG-EG: 0.040 * (0.70) | |
| p-value | 0.000 * | 0.008 * | 0.017 * | ||
| MD | 0.16 | 0.18 | 0.08 | ||
| APSI | Pre | 0.46 ± 0.05 | 0.44 ± 0.06 | 0.42 ± 0.06 | KTG-MG: 0.734 (0.26) KTG-EG: 0.311 (0.45) MG-EG: 0.179 (0.35) |
| Post | 0.33 ± 0.06 | 0.27 ± 0.07 | 0.36 ± 0.08 | KTG-MG: 0.028 * (0.95) KTG-EG: 0.213 (0.30) MG-EG: 0.001 * (1.22) | |
| p-value | 0.000 * | 0.000 * | 0.001 * | ||
| MD | 0.12 | 0.17 | 0.06 | ||
| MLSI | Pre | 0.38 ± 0.05 | 0.40 ± 0.06 | 0.36 ± 0.07 | KTG-MG: 0.311 (1.13) KTG-EG: 0.799 (0.36) MG-EG: 0.446 (0.61) |
| Post | 0.19 ± 0.07 | 0.25 ± 0.11 | 0.28 ± 0.12 | KTG-MG: 0.042 * (0.60) KTG-EG: 0.018 * (0.96) MG-EG: 0.728 (0.28) | |
| p-value | 0.000 * | 0.000 * | 0.005 * | ||
| MD | 0.19 | 0.15 | 0.08 | ||
| Test | KTG | MG | EG | ARM (p and Cohen’s d) | |
|---|---|---|---|---|---|
| Mean ± SD. | Mean ± SD. | Mean ± SD. | |||
| Anterior | Pre | 66.07 ± 12.69 | 68.73 ± 13.01 | 66.4 ± 15.23 | KTG-MG: 0.597 (0.208) KTG-EG: 0.947 (0.024) MG-EG: 0.643 (0.165) |
| Post | 75 ± 11.88 | 76.73 ± 10.03 | 75.53 ± 9.86 | KTG-MG: 0.658 (0.158) KTG-EG: 0.891 (0.049) MG-EG: 0.759 (0.121) | |
| p-value | 0.000 * | 0.001 * | 0.001 * | ||
| MD | 8.93 | 8.00 | 9.13 | ||
| Antero-medial | Pre | 59.47 ± 11.24 | 62.47 ± 12.26 | 63.87 ± 14.6 | KTG-MG: 0.524 (0.255) KTG-EG: 0.351 (0.338) MG-EG: 0.766 (0.104) |
| Post | 69.87 ± 10.41 | 70.73 ± 13.23 | 72.93 ± 14.37 | KTG-MG: 0.854 (0.073) KTG-EG: 0.515 (0.244) MG-EG: 0.640 (0.159) | |
| p-value | 0.005 * | 0.000* | 0.001 * | ||
| MD | 10.4 | 8.27 | 9.07 | ||
| Medial | Pre | 62.53 ± 15.54 | 70.6 ± 16 | 67 ± 16.0 | KTG-MG: 0.171 (0.211) KTG-EG: 0.445 (0.283) MG-EG: 0.537 (0.225) |
| Post | 72.87 ± 13.9 | 79.47 ± 16.63 | 75.2 ± 16.79 | KTG-MG: 0.260 (0.301) KTG-EG: 0.689 (0.151) MG-EG: 0.465 (0.255) | |
| p-value | 0.000 * | 0.000 * | 0.001 * | ||
| MD | 10.33 | 8.87 | 8.20 | ||
| Postero-medial | Pre | 59 ± 11.58 | 65.2 ± 12.01 | 67.8 ± 13.19 | KTG-MG: 0.174 (0.126) KTG-EG: 0.056 (0.249) MG-EG: 0.565 (0.206) |
| Post | 70 ± 9.82 | 74.53 ± 15.06 | 78 ± 16.97 | KTG-MG: 0.389 (0.357) KTG-EG: 0.132 (0.577) MG-EG: 0.510 (0.216) | |
| p-value | 0.000 * | 0.001 * | 0.007 * | ||
| MD | 11 | 9.33 | 10.2 | ||
| Posterior | Pre | 57.67 ± 9.39 | 58.8 ± 12.4 | 58.13 ± 11.04 | KTG-MG: 0.908 (0.046) KTG-EG: 0.779 (0.103) MG-EG: 0.869 (0.057) |
| Post | 61.6 ± 12.59 | 78.67 ± 15.68 | 68.13 ± 14.74 | KTG-MG: 0.002 * (1.2) KTG-EG: 0.221 (0.477) MG-EG: 0.052 (0.692) | |
| p-value | 0.223 | 0.021 * | 0.004 * | ||
| MD | 3.93 | 20.53 | 9.33 | ||
| Postero-lateral | Pre | 49.13 ± 11.71 | 55.07 ± 12.85 | 47.93 ± 12.34 | KTG-MG: 0.194 (0.283) KTG-EG: 0.791 (0.131) MG-EG: 0.120 (0.366) |
| Post | 56 ± 12.49 | 62.13 ± 15.75 | 59.53 ± 19.3 | KTG-MG: 0.303 (0.431) KTG-EG: 0.551 (0.217) MG-EG: 0.660 (0.148) | |
| p-value | 0.000 * | 0.001 * | 0.004 * | ||
| MD | 6.87 | 7.07 | 11.6 | ||
| Lateral | Pre | 40.93 ± 10.65 | 52.0 ± 17.86 | 50.2 ± 16.35 | KTG-MG: 0.054 (0.401) KTG-EG: 0.104 (0.222) MG-EG: 0.749 (0.105) |
| Post | 47.4 ± 10.53 | 60.13 ± 16.45 | 54.47 ± 16.03 | KTG-MG: 0.021 * (0.922) KTG-EG: 0.192 (0.521) MG-EG: 0.294 (0.349) | |
| p-value | 0.000 * | 0.000 * | 0.332 | ||
| MD | 6.47 | 8.13 | 4.27 | ||
| Antero-lateral | Pre | 49.93 ± 10.27 | 52.8 ± 10.76 | 52.4 ± 12.74 | KTG-MG: 0.491 (0.273) KTG-EG: 0.553 (0.213) MG-EG: 0.923 (0.034) |
| Post | 56.87 ± 10.33 | 58.47 ± 11.96 | 59.27 ± 11.18 | KTG-MG: 0.697 (0.143) KTG-EG: 0.560 (0.223) MG-EG: 0.846 (0.069) | |
| p-value | 0.000 * | 0.001 * | 0.19 | ||
| MD | 6.93 | 5.67 | 6.87 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, H.M.; Kamel, W.M.; Kamel, E.M.; Attyia, M.R.; Acar, T.; Kanwal, R.; Ibrahim, A.A. The Effect of Kinesio Taping on Balance and Dynamic Stability in College-Age Recreational Runners with Ankle Instability. Healthcare 2023, 11, 1749. https://doi.org/10.3390/healthcare11121749
Hussein HM, Kamel WM, Kamel EM, Attyia MR, Acar T, Kanwal R, Ibrahim AA. The Effect of Kinesio Taping on Balance and Dynamic Stability in College-Age Recreational Runners with Ankle Instability. Healthcare. 2023; 11(12):1749. https://doi.org/10.3390/healthcare11121749
Chicago/Turabian StyleHussein, Hisham M., Walid M. Kamel, Ehab M. Kamel, Mohamed R. Attyia, Tolgahan Acar, Raheela Kanwal, and Ahmed A. Ibrahim. 2023. "The Effect of Kinesio Taping on Balance and Dynamic Stability in College-Age Recreational Runners with Ankle Instability" Healthcare 11, no. 12: 1749. https://doi.org/10.3390/healthcare11121749