


Enhancing Functional Ability in Chronic Nonspecific Lower Back Pain: The Impact of EMG-Guided Trunk Stabilization Exercises
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
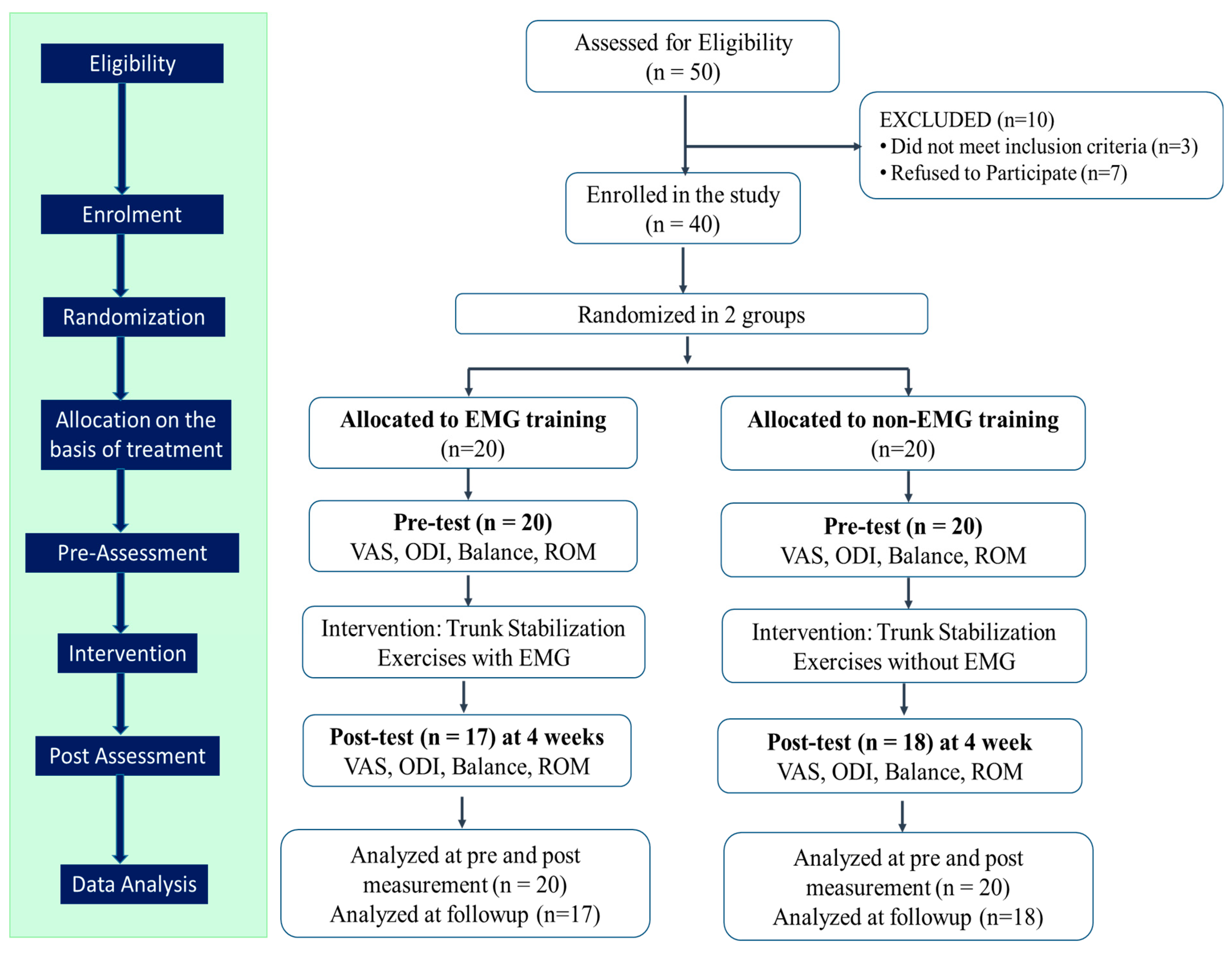
2.1. Study Design
2.2. Sample Size Calculation
2.3. Participants
2.4. Experimental Procedures and Measurements
2.5. Trunk-Stabilization Exercise Program
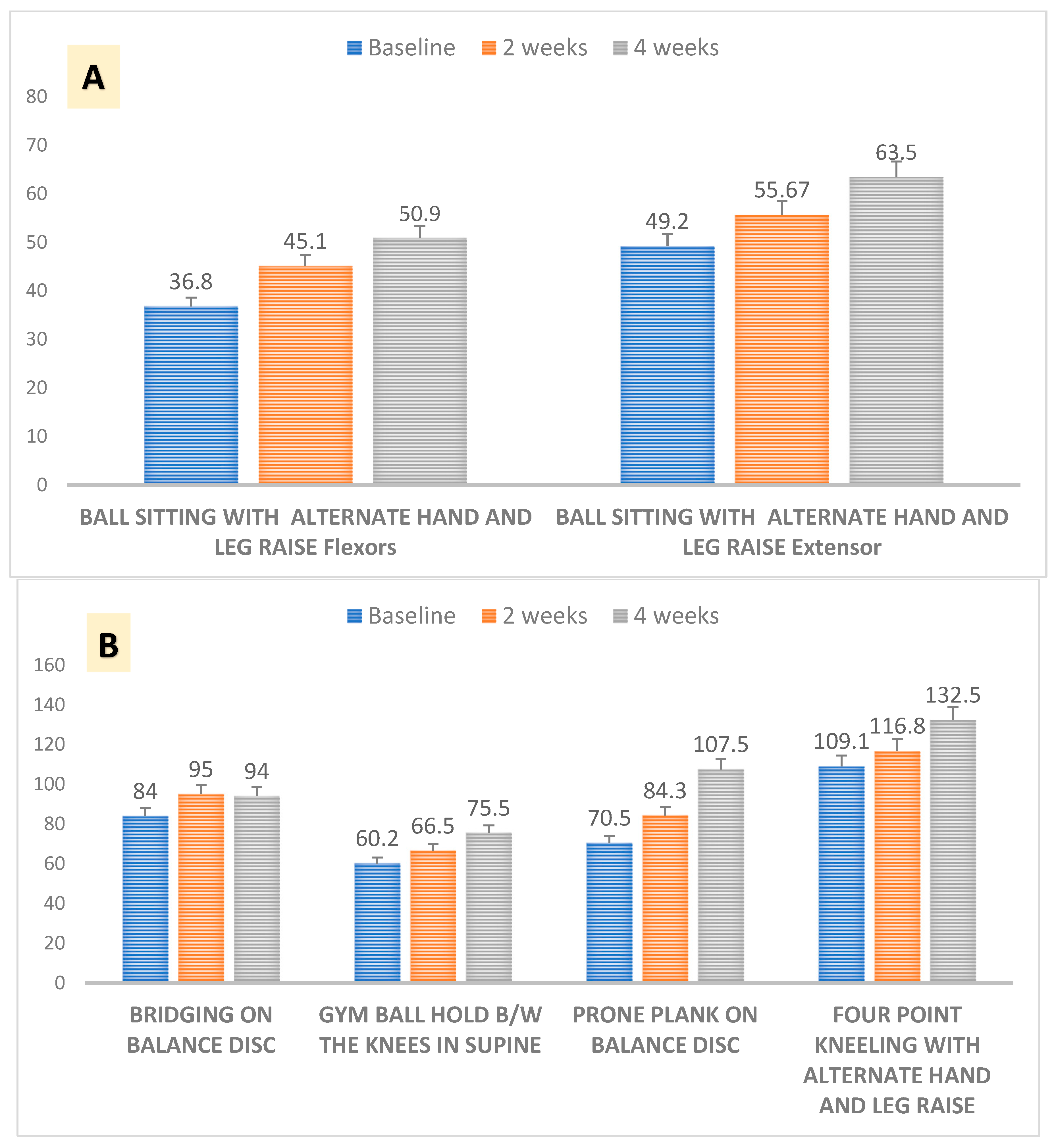
2.6. Flexor and Extensor Trunk EMG Activation during Trunk-Stability Exercises
2.7. Data Analysis
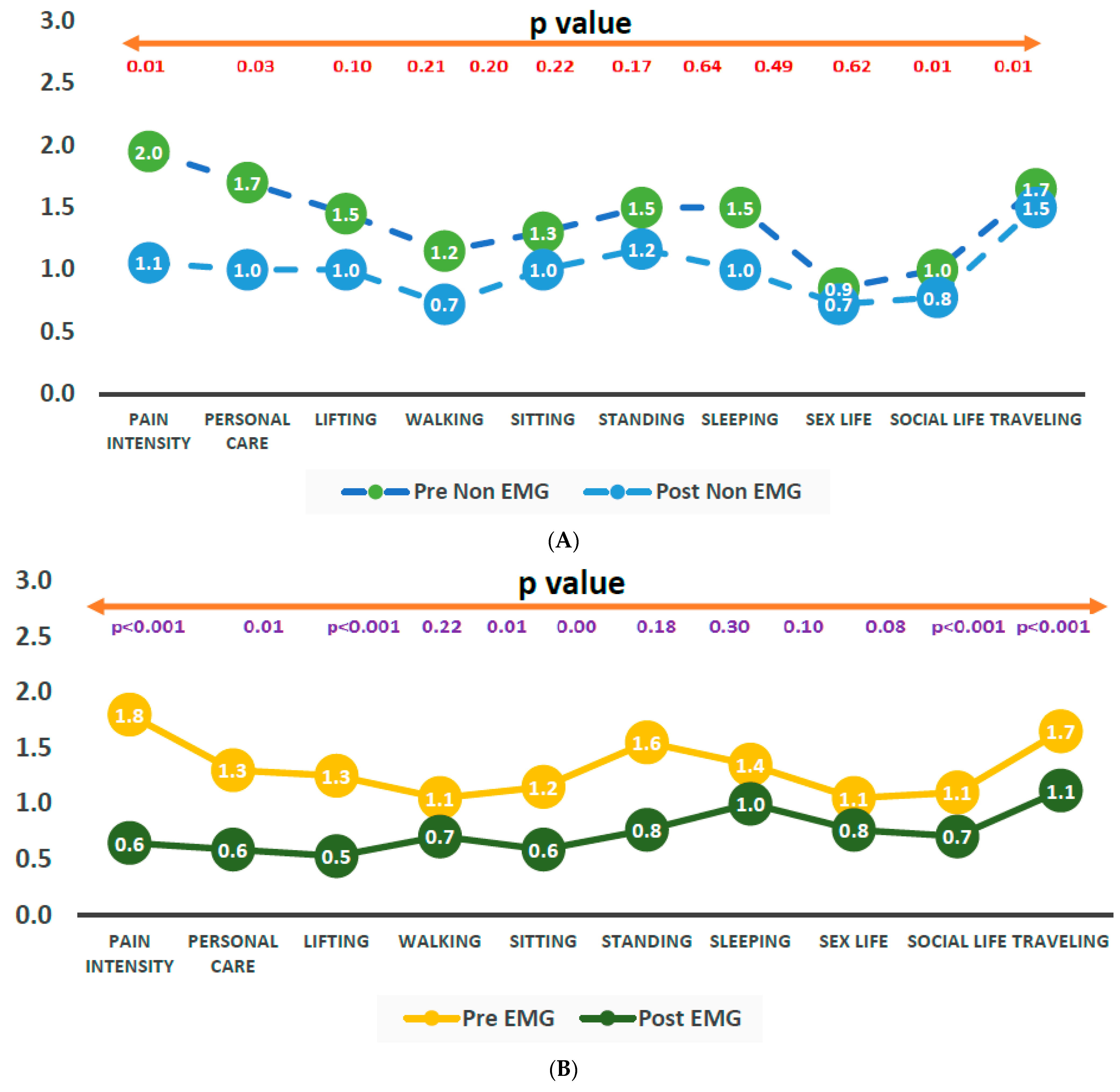
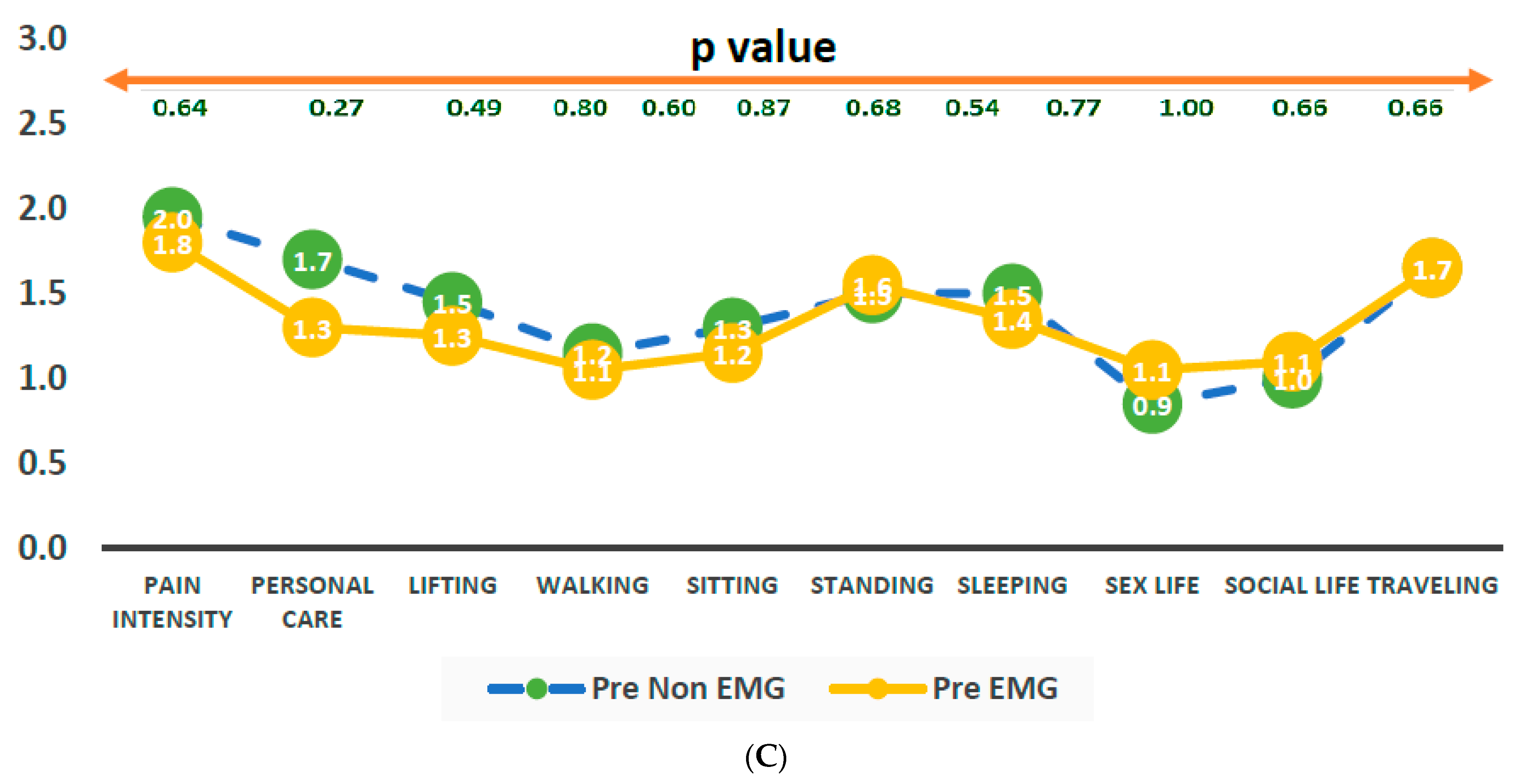
3. Results
4. Discussion
5. Conclusions
5.1. Future Scope
5.2. Clinical Application
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramdas, J.; Jella, V. Prevalence and risk factors of low back pain. Int. J. Adv. Med. 2018, 5, 1120–1123. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.; Iqbal, A.; Shaphe, M.A. Efficacy of electromyography biofeedback training on trunk stability in chronic low back pain. Indian J. Physiother. Occup. Ther. 2013, 7, 81. [Google Scholar] [CrossRef]
- Hemmati, S.; Rajabi, R.; Karimi, N. Effects of consecutive supervised core stability training on pain and disability in women with nonspecific chronic low back pain. Koomesh 2011, 12, 244–252. [Google Scholar]
- Ganesan, S.; Acharya, A.S.; Chauhan, R.; Acharya, S. Prevalence and Risk Factors for Low Back Pain in 1355 Young Adults: A Cross-Sectional Study. Asian Spine J. 2017, 11, 610–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, Y.; Sugiura, S.; Nakagawa, K.; Nakajima, A.; Takahashi, H.; Ohtori, S.; Nishikawa, S. Evaluation of nonspecific low back pain using a new detailed visual analogue scale for patients in motion, standing, and sitting: Characterizing nonspecific low back pain in elderly patients. Pain Res. Treat. 2012, 2012, 680496. [Google Scholar] [CrossRef] [Green Version]
- Suh, J.H.; Kim, H.; Jung, G.P.; Ko, J.Y.; Ryu, J.S. The effect of lumbar stabilization and walking exercises on chronic low back pain: A randomized controlled trial. Medicine 2019, 98, e16173. [Google Scholar] [CrossRef]
- Rajan Balakrishnan, E.Y.; Mahat, M.F.B. Effectiveness of the core stabilisation exercise on floor and Swiss ball on individual with non-Specific low back pain. Int. J. Phys. Educ. Sports Health 2016, 3, 347–356. [Google Scholar]
- Sugaya, T.; Sakamoto, M.; Nakazawa, R.; Wada, N. Relationship between spinal range of motion and trunk muscle activity during trunk rotation. J. Phys. Ther. Sci. 2016, 28, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, D. Mechanical low back pain—A rheumatologist’s view. Nat. Rev. Rheumatol. 2013, 9, 643–653. [Google Scholar] [CrossRef]
- Hwangbo, G.; Lee, C.W.; Kim, S.G.; Kim, H.S. The effects of trunk stability exercise and a combined exercise program on pain, flexibility, and static balance in chronic low back pain patients. J. Phys. Ther. Sci. 2015, 27, 1153–1155. [Google Scholar] [CrossRef] [Green Version]
- Puntumetakul, R.; Saiklang, P.; Yodchaisarn, W.; Hunsawong, T.; Ruangsri, J. Effects of Core Stabilization Exercise versus General Trunk-Strengthening Exercise on Balance Performance, Pain Intensity and Trunk Muscle Activity Patterns in Clinical Lumbar Instability Patients: A Single Blind Randomized Trial. Walailak J. Sci. Technol. 2021, 18, 9054. [Google Scholar] [CrossRef]
- Da Silva, R.A.; Vieira, E.R.; Fernandes, K.B.; Andraus, R.A.; Oliveira, M.R.; Sturion, L.A.; Calderon, M.G. People with chronic low back pain have poorer balance than controls in challenging tasks. Disabil. Rehabil. 2018, 40, 1294–1300. [Google Scholar] [CrossRef] [PubMed]
- Ruhe, A.; Fejer, R.; Walker, B. Center of pressure excursion as a measure of balance performance in patients with non-specific low back pain compared to healthy controls: A systematic review of the literature. Eur. Spine J. 2011, 20, 358–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neblett, R. Surface electromyographic (SEMG) biofeedback for chronic low back pain. Healthcare 2016, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcuria, G.; Marcotulli, C.; Galasso, C.; Pierelli, F.; Casali, C. 15-White Dots APP-Coo-Test: A reliable touch-screen application for assessing upper limb movement impairment in patients with cerebellar ataxias. J. Neurol. 2019, 266, 1611–1622. [Google Scholar] [CrossRef]
- Panjaitan, L.A.; Hon, W.H.C.; Baait, S.N.; Mawaddah, N. Comparison between Proprioceptive Neuromuscular Facilitation and Mckenzie Method in Lumbar Range of Motion on Non-Specific Low Back Pain. ACTIVE J. Phys. Educ. Sport Health Recreat. 2020, 9, 63–71. [Google Scholar] [CrossRef]
- Jenks, A.; Hoekstra, T.; van Tulder, M.; Ostelo, R.W.; Rubinstein, S.M.; Chiarotto, A. Roland Morris Disability Questionnaire, Oswestry Disability Index, and Quebec Back Pain Disability Scale: Which has Superior Measurement Properties in Older Adults with Low Back Pain? J. Orthop. Sports Phys. Ther. 2022, 52, 457–469. [Google Scholar] [CrossRef]
- Miyachi, R.; Sano, A.; Tanaka, N.; Tamai, M.; Miyazaki, J. Relationships among lumbar hip motion angle, perceptual awareness, and low back pain in young adults. J. Phys. Ther. Sci. 2021, 33, 880–886. [Google Scholar] [CrossRef]
- Gupta, G.; Nandini, N. Prevalence of low back pain in non working rural housewives of Kanpur, India. Int. J. Occup. Med. Environ. Health 2015, 28, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Stankovic, A.; Lazovic, M.; Kocic, M.; Dimitrijevic, L.; Stankovic, I.; Zlatanovic, D.; Dimitrijevic, I. Lumbar stabilization exercises in addition to strengthening and stretching exercises reduce pain and increase function in patients with chronic low back pain: Randomized clinical open-label study. Turk. J. Phys. Med. Rehabil./Turk. Fiz. Tip Ve Rehabil. Derg. 2012, 58, 177–183. [Google Scholar] [CrossRef]
- Slade, S.C.; Keating, J.L. Trunk-strengthening exercises for chronic low back pain: A systematic review. J. Manip. Physiol Ther. 2006, 29, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Tahan, N.; Arab, A.M.; Vaseghi, B.; Khademi, K. Electromyographic evaluation of abdominal-muscle function with and without concomitant pelvic-floor-muscle contraction. J. Sport Rehabil. 2013, 22, 108–114. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Robinson, R.C.; Pulliam, C.; Maddrey, A.M. Biofeedback with pain patients: Evidence for its effectiveness. Semin. Pain Med. 2003, 1, 55–66. [Google Scholar] [CrossRef]
- Yuvarani, G.; Kousalya, C.; Kamatchi, K.; Tharani, G.; Vaishnavi, G. To compare the effectiveness of Laser, EMG biofeedback assisted core stability exercise versus Laser and Core stability exercise alone on pain and disability in patients with non-specific low back pain. Res. J. Pharm. Technol. 2020, 13, 2563–2566. [Google Scholar] [CrossRef]
- Barr, K.P.; Griggs, M.; Cadby, T. Lumbar stabilization: A review of core concepts and current literature, part 2. Am. J. Phys. Med. Rehabil. 2007, 86, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Hartigan, C.; Rainville, M. Exercise-Based Therapy for Low Back Pain. UpToDate. 2016. Available online: https://www.uptodate.com/contents/exercise-based-therapy-for-low-back-pain (accessed on 25 October 2021).
- Stokes, I.A.; Gardner-Morse, M.G.; Henry, S.M. Abdominal muscle activation increases lumbar spinal stability: Analysis of contributions of different muscle groups. Clin. Biomech. 2011, 26, 797–803. [Google Scholar] [CrossRef] [Green Version]
- Akuthota, V.; Nadler, S.F. Core strengthening. Arch. Phys. Med. Rehabil. 2004, 85, S86–S92. [Google Scholar] [CrossRef]
- Shaughnessy, M.; Caulfield, B. A pilot study to investigate the effect of lumbar stabilisation exercise training on functional ability and quality of life in patients with chronic low back pain. Int. J. Rehabil. Res. 2004, 27, 297–301. [Google Scholar] [CrossRef]
- Cholewicki, J.; McGill, S.M. Mechanical stability of the in vivo lumbar spine: Implications for injury and chronic low back pain. Clin. Biomech. 1996, 11, 1–15. [Google Scholar] [CrossRef]
- Bellini, C.M.; Galbusera, F.; Raimondi, M.T.; Mineo, G.V.; Brayda-Bruno, M. Biomechanics of the lumbar spine after dynamic stabilization. J. Spinal Disord. Tech. 2007, 20, 423–429. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome Measures | Non-EMG Group (Mean ± SD) | EMG Group (Mean ± SD) | t or χ2 | p |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 30.45 ± 6.04 | 30.8 ± 6.7 | 0.91 | 0.37 |
| Height (m) | 1.59 ± 0.09 | 1.62 ± 0.08 | 0.64 | 0.53 |
| Weight (kg) | 60 ± 7.96 | 63.6 ± 8.88 | 0.83 | 0.42 |
| BMI (kg/m2) | 23.73 ± 3.51 | 24.17 ± 3.2 | 0.94 | 0.36 |
| Marital Status | ||||
| Single | 1 (5%) | 2 (10%) | 0.4 | 0.82 |
| Married | 8 (40%) | 7 (35%) | ||
| Divorced | 1 (5%) | 1 (5%) | ||
| Educational Qualification | ||||
| Undergraduate | 3 (15%) | 5 (25%) | 0.75 | 0.69 |
| Postgraduate | 5 (25%) | 4 (20%) | ||
| Doctorate | 1 (5%) | 2 (10%) | ||
| Clinical Characteristics | ||||
| Duration of NSLBP | ||||
| Less than 5 months | 3 (15%) | 4 (20%) | 0.22 | 0.64 |
| More than 5 months | 7 (35%) | 6 (30%) | ||
| Medications (NSAIDs) | ||||
| No | 2 (10%) | 3 (15%) | 0.61 | 0.44 |
| Yes | 9 (45%) | 6 (30%) | ||
| Sleep disturbance | ||||
| No | 3 (15%) | 3 (15%) | 0.09 | 0.77 |
| Yes | 6 (30%) | 8 (40%) | ||
| Outcome Measures | Non-EMG Group (Mean ± SD) | EMG Group (Mean ± SD) | t | p | Cohens d (CI) |
|---|---|---|---|---|---|
| Pain | |||||
| Pre | 5.00 ± 0.79 | 4.85 ± 0.87 | −0.57 | 0.57 | −0.18 (−0.8, 0.44) |
| Post | 2.11 ± 0.67 | 1.06 ± 0.74 | −4.37 | p < 0.01 | −1.48 (−2.22, −0.72) |
| Functional disability | |||||
| Pre (%) | 28.1 ± 11.28 | 26.5 ± 8.07 | −0.52 | 0.61 | −0.16 (−0.78, 0.46) |
| Post (%) | 19.89 ± 5.37 | 14.82 ± 3.08 | −3.39 | p < 0.01 | −1.15 (−1.86, −0.42) |
| Range of Motion | |||||
| Flexion | |||||
| Pre (cm) | 6.38 ± 0.92 | 5.82 ± 1.77 | −1.25 | 0.22 | −0.4 (−1.02, 0.23) |
| Post (cm) | 6.55 ± 0.95 | 7.61 ± 1.84 | 2.16 | 0.04 | 0.73 (0.04, 1.41) |
| Extension | |||||
| Pre (cm) | 3.82 ± 1.09 | 3.52 ± 1.06 | −0.88 | 0.38 | −0.28 (−0.9, 0.35) |
| Post (cm) | 3.91 ± 1.04 | 4.47 ± 1.21 | 1.45 | 0.16 | 0.49 (−0.19, 1.16) |
| Lateral Flexion Right | |||||
| Pre (cm) | 16.4 ± 3.01 | 15.88 ± 4.06 | −0.46 | 0.65 | −0.14 (−0.76, 0.48) |
| Post (cm) | 16.81 ± 2.6 | 17.14 ± 3.2 | 0.35 | 0.73 | 0.11 (−0.53, 0.76) |
| Lateral Flexion Left | |||||
| Pre (cm) | 16.83 ± 3.82 | 15.78 ± 3.68 | −0.89 | 0.38 | −0.28 (−0.9, 0.34) |
| Post (cm) | 17.07 ± 3.7 | 16.57 ± 3.62 | −0.40 | 0.69 | −0.14 (−0.8, 0.53) |
| Static Balance | |||||
| Eyes Open | |||||
| Pre | 4.84 ± 0.45 | 4.8 ± 0.56 | −0.23 | 0.82 | −0.07 (−0.69, 0.55) |
| Post | 4.87 ± 0.42 | 5.03 ± 0.41 | 1.11 | 0.28 | 0.37 (−0.3, 1.04) |
| Eyes Closed | |||||
| Pre | 4.95 ± 0.5 | 5.1 ± 0.51 | 0.94 | 0.36 | 0.3 (−0.33, 0.92) |
| Post | 5.06 ± 0.63 | 5.17 ± 0.44 | 0.58 | 0.56 | 0.2 (−0.47, 0.86) |
| Group | Pre Mean ± SD | Post Mean ± SD | MD | SD | t | p | 95%CI | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Pain | ||||||||
| Non-EMG Group | 5.00 ± 0.79 | 2.11 ± 0.67 | 2.94 | 0.63 | 19.54 | p < 0.001 | 2.62 | 3.26 |
| EMG Group | 4.85 ± 0.87 | 1.06 ± 0.74 | 3.64 | 0.86 | 17.44 | p < 0.001 | 3.2 | 4.09 |
| Functional disability (%) | ||||||||
| Non-EMG Group | 28.1 ± 11.28 | 19.89 ± 5.37 | 8.33 | 10.13 | 3.48 | p < 0.001 | 3.29 | 13.37 |
| EMG Group | 26.5 ± 8.07 | 14.82 ± 3.08 | 12.58 | 8.59 | 6.03 | p < 0.001 | 8.16 | 17 |
| Range of Motion (cm) | ||||||||
| Flexion (cm) | ||||||||
| Non-EMG Group | 6.38 ± 0.92 | 6.55 ± 0.95 | −0.1 | 0.24 | −1.73 | 0.1 | −0.22 | 0.02 |
| EMG Group | 5.82 ± 1.77 | 7.61 ± 1.84 | −1.94 | 2.43 | −3.28 | p < 0.001 | −3.19 | −0.68 |
| Extension (cm) | ||||||||
| Non-EMG Group | 3.82 ± 1.09 | 3.91 ± 1.04 | −0.19 | 0.54 | −1.51 | 0.14 | −0.46 | 0.07 |
| EMG Group | 3.52 ± 1.06 | 4.47 ± 1.21 | −0.88 | 0.49 | −7.3 | p < 0.001 | −1.13 | −0.62 |
| Lateral Flexion Right (cm) | ||||||||
| Non-EMG Group | 16.4 ± 3.01 | 16.81 ± 2.6 | −0.41 | 0.93 | −1.96 | 0.06 | −0.84 | 0.02 |
| EMG Group | 15.88 ± 4.06 | 17.14 ± 3.2 | −0.57 | 1.42 | −1.64 | 0.11 | −1.3 | 0.16 |
| Lateral Flexion Left (cm) | ||||||||
| Non-EMG Group | 16.83 ± 3.82 | 17.07 ± 3.7 | −0.06 | 1.03 | −0.25 | 0.8 | −0.57 | 0.45 |
| EMG Group | 15.78 ± 3.68 | 16.57 ± 3.62 | −0.3 | 0.92 | −1.33 | 0.2 | −0.77 | 0.17 |
| Static Balance (cm) | ||||||||
| Eyes Open | ||||||||
| Non-EMG Group | 4.84 ± 0.45 | 4.87 ± 0.42 | −0.14 | 0.33 | −1.78 | 0.09 | −0.3 | 0.02 |
| EMG Group | 4.8 ± 0.56 | 5.03 ± 0.41 | −0.1 | 0.21 | −1.99 | 0.06 | −0.2 | 0.00 |
| Eyes Closed | ||||||||
| Non-EMG Group | 4.95 ± 0.5 | 5.06 ± 0.63 | −0.14 | 0.31 | −1.91 | 0.07 | −0.29 | 0.01 |
| EMG Group | 5.1 ± 0.51 | 5.17 ± 0.44 | −0.11 | 0.18 | −2.61 | 0.01 | −0.21 | −0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porwal, S.; Rizvi, M.R.; Sharma, A.; Ahmad, F.; Alshahrani, M.S.; Raizah, A.; Shaik, A.R.; Seyam, M.K.; Miraj, M.; Alkhamis, B.A.; et al. Enhancing Functional Ability in Chronic Nonspecific Lower Back Pain: The Impact of EMG-Guided Trunk Stabilization Exercises. Healthcare 2023, 11, 2153. https://doi.org/10.3390/healthcare11152153
Porwal S, Rizvi MR, Sharma A, Ahmad F, Alshahrani MS, Raizah A, Shaik AR, Seyam MK, Miraj M, Alkhamis BA, et al. Enhancing Functional Ability in Chronic Nonspecific Lower Back Pain: The Impact of EMG-Guided Trunk Stabilization Exercises. Healthcare. 2023; 11(15):2153. https://doi.org/10.3390/healthcare11152153
Chicago/Turabian StylePorwal, Shivani, Moattar Raza Rizvi, Ankita Sharma, Fuzail Ahmad, Mastour Saeed Alshahrani, Abdullah Raizah, Abdul Rahim Shaik, Mohamed K. Seyam, Mohammad Miraj, Batool Abdulelah Alkhamis, and et al. 2023. "Enhancing Functional Ability in Chronic Nonspecific Lower Back Pain: The Impact of EMG-Guided Trunk Stabilization Exercises" Healthcare 11, no. 15: 2153. https://doi.org/10.3390/healthcare11152153