
CanCOG®: Cultural Adaptation of the Evidence-Based UCLA Cognitive Rehabilitation Intervention Program for Cancer Survivors in Portugal
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
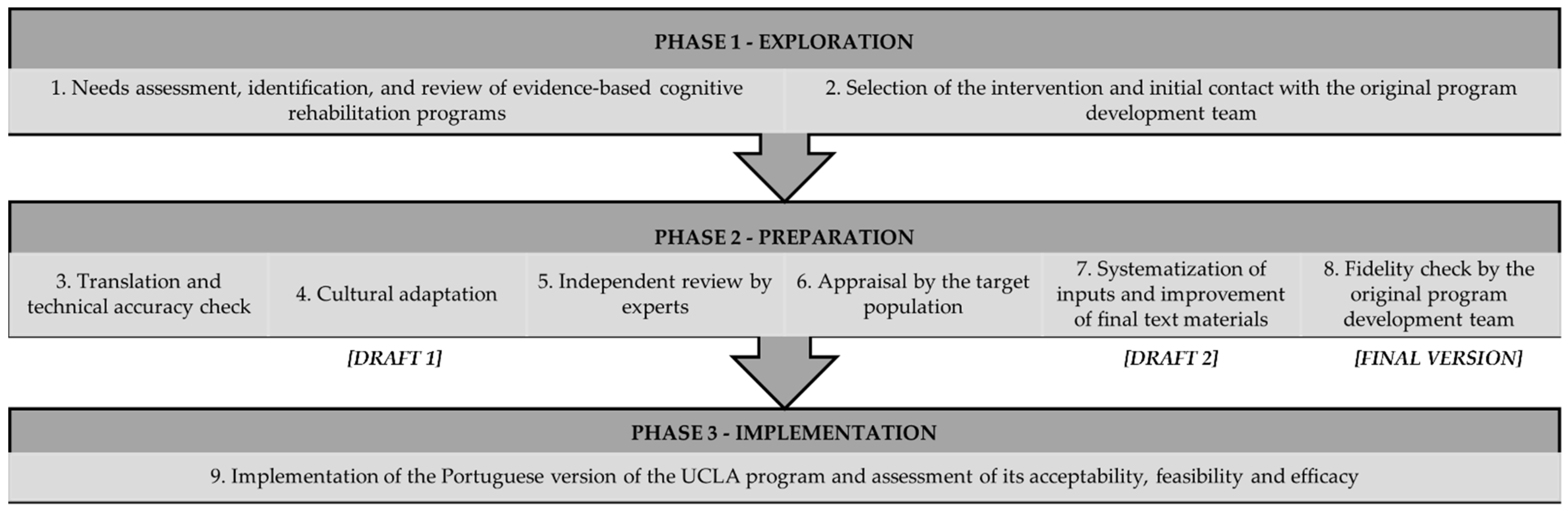
2.1. Framework for the Cultural Adaptation Process
2.1.1. Exploration Phase
2.1.2. Preparation Phase
- Words and expressions appropriate to the target population, considering adjustments to the level of reading difficulty and education to ensure content accessibility.
- Words and expressions for semantic and conceptual equivalence.
- Personal names used throughout the program (e.g., exercises, daily examples).
- References to different cultural aspects, such as habits, customs and traditions.
- Instructions and/or content of some exercises without cultural correspondence to the Portuguese context. Regarding instructions, guidelines were provided by the original program development team to maintain the equivalence of the exercises (e.g., substitute words that appear in the text a similar number of times and consider the word classes—for instance, nouns are easier to follow than conjunctions, determinants, or pronouns).
- One assistant professor with previous research experience in psycho-oncology, including aspects related to reproductive and sexual health and psychosocial adaptation of young female breast cancer survivors (e.g., breast and gynaecological cancer) and clinical intervention in other chronic diseases (e.g., chronic kidney disease, chronic obstructive pulmonary disease, caregivers of people with dementia).
- One doctoral student in health psychology, having worked as a clinical and health psychologist in a cancer patient support association and at a national reference centre in oncology. She also had research experience in neurosciences, including the study of CRCI.
- One assistant professor with extensive clinical and research experience in psycho-oncology, including group intervention (cognitive–behavioural therapy and psychoeducation), psychosocial adjustment, needs, work ability, and reproductive concerns in young cancer survivors, focusing on both patients and their caregivers.
- One assistant professor with extensive research experience in neuropsychology, namely ageing, cognitive rehabilitation, cultural adaptation and validation of neuropsychological instruments (e.g., attention, executive functions).
- One full researcher with clinical and research experience in neuropsychology, namely cognitive neurosciences and cognitive assessment and rehabilitation, specifically in the field of executive functions.
- One full researcher with extensive expertise in human memory.
3. Results
3.1. Translation and Cultural Adaptation of the Program Contents
3.2. Independent Review by a Panel of Experts
3.3. Appraisal by the Target Population
3.4. Systematization of Contributions, Improvement of the Final Text Materials of the Program, and Fidelity Check by the Original Program Development Team
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wefel, J.S.; Kesler, S.R.; Noll, K.R.; Schagen, S.B. Clinical Characteristics, Pathophysiology, and Management of Noncentral Nervous System Cancer-Related Cognitive Impairment in Adults. CA Cancer J. Clin. 2015, 65, 123–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, H.A.; Richard, N.M.; Edelstein, K. Cognitive Rehabilitation for Cancer-Related Cognitive Dysfunction: A Systematic Review. Support. Care Cancer 2019, 27, 3253–3279. [Google Scholar] [CrossRef] [PubMed]
- Ahles, T.A.; Root, J.C. Cognitive Effects of Cancer and Cancer Treatments. Annu. Rev. Clin. Psychol. 2018, 14, 425–451. [Google Scholar] [CrossRef] [PubMed]
- Janelsins, M.C.; Kesler, S.R.; Ahles, T.A.; Morrow, G.R. Prevalence, Mechanisms, and Management of Cancer-Related Cognitive Impairment. Int. Rev. Psychiatry 2014, 26, 102–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo, S.J.; Lustberg, M.; Dhillon, H.M.; Nakamura, Z.M.; Allen, D.H.; von Ah, D.; Janelsins, M.C.; Chan, A.; Olson, K.; Tan, C.J.; et al. Cancer-Related Cognitive Impairment in Patients with Non-Central Nervous System Malignancies: An Overview for Oncology Providers from the MASCC Neurological Complications Study Group. Support. Care Cancer 2021, 29, 2821–2840. [Google Scholar] [CrossRef] [PubMed]
- Országhová, Z.; Mego, M.; Chovanec, M. Long-Term Cognitive Dysfunction in Cancer Survivors. Front. Mol. Biosci. 2021, 8, 770413. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, T.S.; Treviño, M.; Gooch, I.M.; Duffy, K.A. Understanding the Profile of Cancer-Related Cognitive Impairments: A Critique of Meta-Analyses. JNCI J. Natl. Cancer Inst. 2019, 111, 1009–1015. [Google Scholar] [CrossRef]
- Dijkshoorn, A.B.C.; van Stralen, H.E.; Sloots, M.; Schagen, S.B.; Visser-Meily, J.M.A.; Schepers, V.P.M. Prevalence of Cognitive Impairment and Change in Patients with Breast Cancer: A Systematic Review of Longitudinal Studies. Psychooncology 2021, 30, 635–648. [Google Scholar] [CrossRef]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; de Ruiter, M.B.; Castel, H. Cancer-Related Cognitive Impairment: An Update on State of the Art, Detection, and Management Strategies in Cancer Survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef] [Green Version]
- Sleurs, C.; Amidi, A.; Wu, L.M.; Kiesl, D.; Zimmer, P.; Lange, M.; Rogiers, A.; Giffard, B.; Binarelli, G.; Borghgraef, C.; et al. Cancer-Related Cognitive Impairment in Non-CNS Cancer Patients: Targeted Review and Future Action Plans in Europe. Crit. Rev. Oncol./Hematol. 2022, 180, 103859. [Google Scholar] [CrossRef]
- Ramalho, M.; Fontes, F.; Ruano, L.; Pereira, S.; Lunet, N. Cognitive Impairment in the First Year after Breast Cancer Diagnosis: A Prospective Cohort Study. Breast 2017, 32, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, M.; Ogilvie, J.M.; Wilson, J.; Green, H.; Chambers, S.; Ownsworth, T.; Shum, D.H.K. A Meta-Analysis of Cognitive Impairment and Decline Associated with Adjuvant Chemotherapy in Women with Breast Cancer. Front. Oncol. 2015, 5, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Ah, D. Cognitive Changes Associated with Cancer and Cancer Treatment: State of the Science. Clin. J. Oncol. Nurs. 2015, 19, 47–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Ah, D.; Russell, K.M.; Storniolo, A.M.; Carpenter, J.S. Cognitive Dysfunction and Its Relationship to Quality of Life in Breast Cancer Survivors. Oncol. Nurs. Forum 2009, 36, 326–334. [Google Scholar] [CrossRef]
- Chao, D.; Hale, A.; Henry, N.L.; Kratz, A.L.; Gabel, N.M. Cancer-Related Cognitive Impairment or “Chemobrain:” Emerging Assessments, Treatments, and Targets for Intervention. Curr. Phys. Med. Rehabil. Rep. 2021, 9, 108–118. [Google Scholar] [CrossRef]
- Lange, M.; Licaj, I.; Clarisse, B.; Humbert, X.; Grellard, J.M.; Tron, L.; Joly, F. Cognitive Complaints in Cancer Survivors and Expectations for Support: Results from a Web–Based Survey. Cancer Med. 2019, 8, 2654–2663. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.S.K.; Wang, X.; Niu, N.; Liang, M.; Zeng, Y. Neuropsychological Interventions for Cancer-Related Cognitive Impairment: A Network Meta-Analysis of Randomized Controlled Trials. Neuropsychol. Rev. 2022, 32, 893–905. [Google Scholar] [CrossRef]
- Von Ah, D.; Crouch, A. Cognitive Rehabilitation for Cognitive Dysfunction after Cancer and Cancer Treatment: Implications for Nursing Practice. Semin. Oncol. Nurs. 2020, 36, 150977. [Google Scholar] [CrossRef]
- MacKenzie, L.; Marshall, K. Effective Non-Pharmacological Interventions for Cancer Related Cognitive Impairment in Adults (Excluding Central Nervous System or Head and Neck Cancer): Systematic Review and Meta-Analysis. Eur. J. Phys. Rehabil. Med. 2022, 58, 258–270. [Google Scholar] [CrossRef]
- Gaynor, A.M.; Root, J.C.; Ahles, T.A. Neuropsychological Impact of Cancer and Cancer Treatments. In Psycho-Oncology, 4th ed.; Breitbart, W., Butow, P., Jacobsen, P., Lam, W., Lazenby, M., Loscalzo, M., Eds.; Oxford University Press: New York, NY, USA, 2021; pp. 283–290. [Google Scholar]
- Zeng, Y.; Dong, J.; Huang, M.; Zhang, J.E.; Zhang, X.; Xie, M.; Wefel, J.S. Nonpharmacological Interventions for Cancer-Related Cognitive Impairment in Adult Cancer Patients: A Network Meta-Analysis. Int. J. Nurs. Stud. 2020, 104, 103514. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network NCCN Clinical Practice Guidelines in Oncology—Survivorship (Version 1.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf (accessed on 21 October 2022).
- Wilson, B.A. Neuropsychological Rehabilitation. Annu. Rev. Clin. Psychol. 2008, 4, 141–162. [Google Scholar] [CrossRef] [PubMed]
- Cicerone, K.D.; Dahlberg, C.; Kalmar, K.; Langenbahn, D.M.; Malec, J.F.; Bergquist, T.F.; Felicetti, T.; Giacino, J.T.; Harley, J.P.; Harrington, D.E.; et al. Evidence-Based Cognitive Rehabilitation: Recommendations for Clinical Practice. Arch. Phys. Med. Rehabil. 2000, 81, 1596–1615. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kang, S.J. Computerized Programs for Cancer Survivors with Cognitive Problems: A Systematic Review. J. Cancer Surviv. 2019, 13, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, N. Avaliação e Reabilitação Cognitiva Em Doentes Com Tumor Cerebral: O Programa Opportunity. Master’s Thesis, Universidade do Porto, Porto, Portugal, 2016. [Google Scholar]
- Ercoli, L.M.; Castellon, S.A.; Hunter, A.M.; Kwan, L.; Kahn-Mills, B.A.; Cernin, P.A.; Leuchter, A.F.; Ganz, P.A. Assessment of the Feasibility of a Rehabilitation Intervention Program for Breast Cancer Survivors with Cognitive Complaints. Brain Imaging Behav. 2013, 7, 543–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercoli, L.M.; Petersen, L.; Hunter, A.M.; Castellon, S.A.; Kwan, L.; Kahn-Mills, B.A.; Embree, L.M.; Cernin, P.A.; Leuchter, A.F.; Ganz, P.A.; et al. Cognitive Rehabilitation Group Intervention for Breast Cancer Survivors: Results of a Randomized Clinical Trial. Psychooncology 2015, 24, 1360–1367. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Bessa, A.; Fernandes, S.M.; Vázquez-Justo, E.; Conde, A. Anxiety and Cognitive Functioning in Breast Cancer Patients Treated with Chemotherapy. J. Neuropsychol. 2020, 14, 129–141. [Google Scholar] [CrossRef]
- Ferreira, A.S.; Teixeira, R.J.; Brandão, T.; Conde, A. Traumatic Symptomatology and Cognitive Functioning in Women with Breast Cancer Treated with Chemotherapy: An Exploratory Study. J. Neuropsychol. 2021, 15, 150–164. [Google Scholar] [CrossRef]
- Araújo, N.; Severo, M.; Lopes-Conceição, L.; Fontes, F.; Dias, T.; Branco, M.; Morais, S.; Cruz, V.T.; Ruano, L.; Pereira, S.; et al. Trajectories of Cognitive Performance over Five Years in a Prospective Cohort of Patients with Breast Cancer (NEON-BC). Breast 2021, 58, 130–137. [Google Scholar] [CrossRef]
- Araújo, N.; Morais, S.; Costa, A.R.; Braga, R.; Carneiro, A.F.; Cruz, V.T.; Ruano, L.; Oliveira, J.; Figueiredo, L.P.; Pereira, S.; et al. Cognitive Decline in Patients with Prostate Cancer: Study Protocol of a Prospective Cohort, NEON-PC. BMJ Open 2021, 11, e043844. [Google Scholar] [CrossRef]
- Araújo, N.; Costa, A.; Lopes, C.; Lopes-Conceição, L.; Ferreira, A.; Carneiro, F.; Oliveira, J.; Morais, S.; Pacheco-Figueiredo, L.; Ruano, L.; et al. Prevalence of Cognitive Impairment before Prostate Cancer Treatment. Cancers 2022, 14, 1355. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.F.; Torres, A.; Teixeira, R.J.; Monteiro, S.; Pereira, A.; Santos, I.M. Perceived Cognitive Functioning in Breast Cancer Patients Treated with Chemotherapy Compared to Matched Healthy Women: Evidence from a Portuguese Study. Int. J. Nurs. Pract. 2022, e13119. [Google Scholar] [CrossRef] [PubMed]
- Movsisyan, A.; Arnold, L.; Evans, R.; Hallingberg, B.; Moore, G.; O’Cathain, A.; Pfadenhauer, L.M.; Segrott, J.; Rehfuess, E. Adapting Evidence-Informed Complex Population Health Interventions for New Contexts: A Systematic Review of Guidance. Implement. Sci. 2019, 14, 105. [Google Scholar] [CrossRef] [Green Version]
- Bernal, G.; Sáez-Santiago, E. Culturally Centered Psychosocial Interventions. J. Community Psychol. 2006, 34, 121–132. [Google Scholar] [CrossRef]
- Griner, D.; Smith, T.B. Culturally Adapted Mental Health Intervention: A Meta-Analytic Review. Psychotherapy 2006, 43, 531–548. [Google Scholar] [CrossRef] [Green Version]
- Benish, S.G.; Quintana, S.; Wampold, B.E. Culturally Adapted Psychotherapy and the Legitimacy of Myth: A Direct-Comparison Meta-Analysis. J. Couns. Psychol. 2011, 58, 279–289. [Google Scholar] [CrossRef]
- Castro, F.G.; Barrera, M.; Holleran Steiker, L.K. Issues and Challenges in the Design of Culturally Adapted Evidence-Based Interventions. Annu. Rev. Clin. Psychol. 2010, 6, 213–239. [Google Scholar] [CrossRef] [Green Version]
- Movsisyan, A.; Arnold, L.; Copeland, L.; Evans, R.; Littlecott, H.; Moore, G.; O’Cathain, A.; Pfadenhauer, L.; Segrott, J.; Rehfuess, E.; et al. Adapting Evidence-Informed Population Health Interventions for New Contexts: A Scoping Review of Current Practice. Health Res. Policy Syst. 2021, 19, 13. [Google Scholar] [CrossRef]
- Lee, R.M.; Vu, A.M.; Lau, A. Culture and Evidence-Based Prevention Programs. In Handbook of Multicultural Mental Health: Assessment and Treatment of Diverse Populations, 2nd ed.; Paniagua, F.A., Yamada, A.M., Eds.; Elsevier Inc.: London, UK, 2013; pp. 527–546. [Google Scholar]
- Escoffery, C.; Lebow-Skelley, E.; Udelson, H.; Böing, E.A.; Wood, R.; Fernandez, M.E.; Mullen, P.D. A Scoping Study of Frameworks for Adapting Public Health Evidence-Based Interventions. Transl. Behav. Med. 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Bernal, G.; Bonilla, J.; Bellido, C. Ecological Validity and Cultural Sensitivity for Outcome Research: Issues for the Cultural Adaptation and Development of Psychosocial Treatments with Hispanics. J. Abnorm. Child Psychol. 1995, 23, 67–82. [Google Scholar] [CrossRef]
- Bernal, G.; Jiménez-Chafey, M.I.; Domenech Rodríguez, M.M. Cultural Adaptation of Treatments: A Resource for Considering Culture in Evidence-Based Practice. Prof. Psychol. Res. Pract. 2009, 40, 361–368. [Google Scholar] [CrossRef]
- Falicov, C.J. Commentary: On the Wisdom and Challenges of Culturally Attuned Treatments for Latinos. Fam. Process 2009, 48, 292–309. [Google Scholar] [CrossRef] [PubMed]
- McKleroy, V.S.; Galbraith, J.S.; Cummings, B.; Jones, P.; Harshbarger, C.; Collins, C.; Gelaude, D.; Carey, J.W.; Glassman, M.; Longdon, B.; et al. Adapting Evidence-Based Behavioral Interventions for New Settings and Target Populations. AIDS Educ. Prev. 2006, 18, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Stirman, S.W.; Baumann, A.A.; Miller, C.J. The FRAME: An Expanded Framework for Reporting Adaptations and Modifications to Evidence-Based Interventions. Implement. Sci. 2019, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- Resnicow, K.; Soler, R.; Braithwaite, K.L.; Ahluwalia, R.S.; Butler, J. Cultural Sensitivity in Substance Use Prevention. J. Community Psychol. 2000, 28, 271–290. [Google Scholar] [CrossRef]
- Castro, F.G.; Barrera, M.; Martinez, C.R. The Cultural Adaptation of Prevention Interventions: Resolving Tensions between Fidelity and Fit. Prev. Sci. 2004, 5, 41–45. [Google Scholar] [CrossRef]
- Baumann, A.A.; Powell, B.J.; Kohl, P.L.; Tabak, R.G.; Penalba, V.; Proctor, E.K.; Domenech-Rodriguez, M.M.; Cabassa, L.J. Cultural Adaptation and Implementation of Evidence-Based Parent-Training: A Systematic Review and Critique of Guiding Evidence. Child Youth Serv. Rev. 2015, 53, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Salamanca-Sanabria, A.; Richards, D.; Timulak, L. Adapting an Internet-Delivered Intervention for Depression for a Colombian College Student Population: An Illustration of an Integrative Empirical Approach. Internet Interv. 2019, 15, 76–86. [Google Scholar] [CrossRef]
- Bernal, G.; Adames, C. Cultural Adaptations: Conceptual, Ethical, Contextual, and Methodological Issues for Working with Ethnocultural and Majority-World Populations. Prev. Sci. 2017, 18, 681–688. [Google Scholar] [CrossRef]
- Ferrer-Wreder, L.; Sundell, K.; Mansoory, S. Tinkering with Perfection: Theory Development in the Intervention Cultural Adaptation Field. Child Youth Care Forum 2012, 41, 149–171. [Google Scholar] [CrossRef]
- Duarte, N.; Hughes, S.L.; Paúl, C. Cultural Adaptation and Specifics of the Fit & Strong! Program in Portugal. Transl. Behav. Med. 2019, 9, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Wingood, G.M.; DiClemente, R.J. The ADAPT-ITT Model: A Novel Method of Adapting Evidence-Based HIV Interventions. J. Acquir. Immune Defic. Syndr. 2008, 47, S40–S46. [Google Scholar] [CrossRef] [PubMed]
- Sangraula, M.; Kohrt, B.A.; Ghimire, R.; Shrestha, P.; Luitel, N.P.; van’t Hof, E.; Dawson, K.; Jordans, M.J.D. Development of the Mental Health Cultural Adaptation and Contextualization for Implementation (MhCACI) Procedure: A Systematic Framework to Prepare Evidence-Based Psychological Interventions for Scaling. Glob. Ment. Health 2021, 8, e6. [Google Scholar] [CrossRef]
- Teles, S.; Napolskij, M.S.; Paúl, C.; Ferreira, A.; Seeher, K. Training and Support for Caregivers of People with Dementia: The Process of Culturally Adapting the World Health Organization iSupport Programme to Portugal. Dementia 2021, 20, 672–697. [Google Scholar] [CrossRef]
- Kumpfer, K.L.; Pinyuchon, M.; de Melo, A.T.; Whiteside, H.O. Cultural Adaptation Process for International Dissemination of the Strengthening Families Program. Eval. Health Prof. 2008, 31, 226–239. [Google Scholar] [CrossRef]
- Barrera, M.; Castro, F.G.; Strycker, L.A.; Toobert, D.J. Cultural Adaptations of Behavioral Health Interventions: A Progress Report. J. Consult. Clin. Psychol. 2013, 81, 196–205. [Google Scholar] [CrossRef] [Green Version]
- Barrera, M.; Castro, F.G. A Heuristic Framework for the Cultural Adaptation of Interventions. Clin. Psychol. Sci. Pract. 2006, 13, 311–316. [Google Scholar] [CrossRef]
- Domenech-Rodríguez, M.; Wieling, E. Developing Culturally Appropriate, Evidence-Based Treatments for Interventions with Ethnic Minority Populations. In Voices of Color: First-Person Accounts of Ethnic Minority Therapists; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2012; pp. 313–334. [Google Scholar]
- Aguirre, E.; Spector, A.; Orrell, M. Guidelines for Adapting Cognitive Stimulation Therapy to Other Cultures. Clin. Interv. Aging 2014, 9, 1003–1007. [Google Scholar] [CrossRef]
- Hwang, W.C. The Formative Method for Adapting Psychotherapy (FMAP): A Community-Based Developmental Approach to Culturally Adapting Therapy. Prof. Psychol. Res. Pract. 2009, 40, 369–377. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.F.; Torres, A.; Pereira, A.; Santos, I.M. Cancer-Related Cognitive Impairment in Cancer: Examining Portuguese Cancer Survivors’ Acceptability and Expectations Regarding Cognitive Telerehabilitation Interventions. Eur. Psychiatry 2021, 64, S539. [Google Scholar] [CrossRef]
- Oh, P.J.; Kim, J.H. The Effects of Nonpharmacologic Interventions on Cognitive Function in Patients with Cancer: A Meta-Analysis. Oncol. Nurs. Forum 2016, 43, E205–E217. [Google Scholar] [CrossRef] [PubMed]
- Treanor, C.J.; Mcmenamin, U.C.; O’Neill, R.F.; Cardwell, C.R.; Clarke, M.J.; Cantwell, M.; Donnelly, M. Non-Pharmacological Interventions for Cognitive Impairment Due to Systemic Cancer Treatment. Cochrane Database Syst. Rev. 2016, 8, CD011325. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Y.; Cheng, A.S.K.; Chan, C.C.H. Meta-Analysis of the Effects of Neuropsychological Interventions on Cognitive Function in Non-Central Nervous System Cancer Survivors. Integr. Cancer Ther. 2016, 15, 424–434. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.J.; McCarthy, A.L.; Devenish, J.; Sullivan, K.A.; Chan, A. Systematic Review of Pharmacologic and Non-Pharmacologic Interventions to Manage Cognitive Alterations after Chemotherapy for Breast Cancer. Eur. J. Cancer 2015, 51, 437–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morean, D.F.; O’Dwyer, L.; Cherney, L.R. Therapies for Cognitive Deficits Associated with Chemotherapy for Breast Cancer: A Systematic Review of Objective Outcomes. Arch. Phys. Med. Rehabil. 2015, 96, 1880–1897. [Google Scholar] [CrossRef]
- Vance, D.E.; Frank, J.S.; Bail, J.; Triebel, K.L.; Niccolai, L.M.; Gerstenecker, A.; Meneses, K. Interventions for Cognitive Deficits in Breast Cancer Survivors Treated with Chemotherapy. Cancer Nurs. 2017, 40, E11–E27. [Google Scholar] [CrossRef] [PubMed]
- Von Ah, D.; Jansen, C.E.; Allen, D.H. Evidence-Based Interventions for Cancer- and Treatment-Related Cognitive Impairment. Clin. J. Oncol. Nurs. 2015, 18, 17–25. [Google Scholar] [CrossRef]
- Reiss, K.; Vermeer, H.J. Towards a General Theory of Translational Action: Skopos Theory Explained, 1st ed.; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Onwuegbuzie, A.J.; Dickinson, W.B.; Leech, N.L.; Zoran, A.G. A Qualitative Framework for Collecting and Analyzing Data in Focus Group Research. Int. J. Qual. Methods 2009, 8, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Noy, C. Sampling Knowledge: The Hermeneutics of Snowball Sampling in Qualitative Research. Int. J. Soc. Res. Methodol. 2008, 11, 327–344. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacheco-Figueiredo, L.; Lunet, N. Health Status, Use of Healthcare, and Socio-Economic Implications of Cancer Survivorship in Portugal: Results from the Fourth National Health Survey. J. Cancer Surviv. 2014, 8, 611–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helms, J.E. An Examination of the Evidence in Culturally Adapted Evidence-Based or Empirically Supported Interventions. Transcult. Psychiatry 2015, 52, 174–197. [Google Scholar] [CrossRef] [Green Version]
- Kautz, R.L.; Huggard, B.M. Chaos at the Amusement Park: Dynamics of the Tilt-A-Whirl. Am. J. Phys. 1994, 62, 59–66. [Google Scholar] [CrossRef]
- Cavaco, S.; Gonçalves, A.; Pinto, C.; Almeida, E.; Gomes, F.; Moreira, I.; Fernandes, J.; Teixeira-Pinto, A. Trail Making Test: Regression-Based Norms for the Portuguese Population. Arch. Clin. Neuropsychol. 2013, 28, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Berry, L.L.; Davis, S.W.; Godfrey Flynn, A.; Landercasper, J.; Deming, K.A. Is It Time to Reconsider the Term “Cancer Survivor”? J. Psychosoc. Oncol. 2019, 37, 413–426. [Google Scholar] [CrossRef]
- Cao, W.; Cho, H. Culture in Cancer Survivorship Interventions for Asian Americans: A Systematic Review and Critical Analyses. Asian Am. J. Psychol. 2021, 12, 65–75. [Google Scholar] [CrossRef]
- Torres, A.; Pereira, A.; Monteiro, S. Cognitive-Behavioral Group Therapy for Breast Cancer Survivors: Description of a Program and Preliminary Evaluation of Its Effectiveness. Psychol. Community Health 2012, 1, 300–312. [Google Scholar] [CrossRef]
- Soto, A.; Smith, T.B.; Griner, D.; Domenech Rodríguez, M.; Bernal, G. Cultural Adaptations and Therapist Multicultural Competence: Two Meta-Analytic Reviews. J. Clin. Psychol. 2018, 74, 1907–1923. [Google Scholar] [CrossRef] [Green Version]
- Crouch, A.; von Ah, D.; Storey, S. Addressing Cognitive Impairment after Breast Cancer: What Do Women Want? Clin. Nurse Spec. 2017, 31, 82–88. [Google Scholar] [CrossRef]
- Oliveira, A.F.; Santos, I.M.; Torres, A.; Ercoli, L.M. Cognition in Cancer: Proposal of a Web-Based Cognitive Rehabilitation Program for Portuguese Working Non-Central Nervous System (CNS) Cancer Survivors. J. Psychosoc. Oncol. Res. Pract. 2021, 3, 72–73. [Google Scholar] [CrossRef]
- Van der Linden, S.D.; Sitskoorn, M.M.; Rutten, G.J.M.; Gehring, K. Feasibility of the Evidence-Based Cognitive Telerehabilitation Program Remind for Patients with Primary Brain Tumors. J. Neuro-Oncol. 2018, 137, 523–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smidt, K.; Mackenzie, L.; Dhillon, H.; Vardy, J.; Lewis, J.; Loh, S.Y. The Perceptions of Australian Oncologists about Cognitive Changes in Cancer Survivors. Support. Care Cancer 2016, 24, 4679–4687. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.T.; Shwe, M.; Tan, E.H.J.; Chui, W.K.; Ng, R.; Chan, A. Acknowledging the Relevance of Cognitive Changes in Cancer Patients: Perspectives of Oncology Practitioners in Asia. J. Cancer Surviv. 2013, 7, 146–154. [Google Scholar] [CrossRef]
- Mitchell, T.; Turton, P. “Chemobrain”: Concentration and Memory Effects in People Receiving Chemotherapy—A Descriptive Phenomenological Study. Eur. J. Cancer Care 2011, 20, 539–548. [Google Scholar] [CrossRef]
- Munir, F.; Burrows, J.; Yarker, J.; Kalawsky, K.; Bains, M. Women’s Perceptions of Chemotherapy-Induced Cognitive Side Affects on Work Ability: A Focus Group Study. J. Clin. Nurs. 2010, 19, 1362–1370. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Item of the TIDieR Checklist | Explanation |
|---|---|
| Brief Name | UCLA Cognitive Rehabilitation Intervention Program. |
| Why | The UCLA Cognitive Rehabilitation Intervention Program is a small group face-to-face cognitive rehabilitation intervention developed for the specific needs of cancer survivors with cognitive complaints. The program’s main aim is to improve self-reported and performance-based cognitive functioning. |
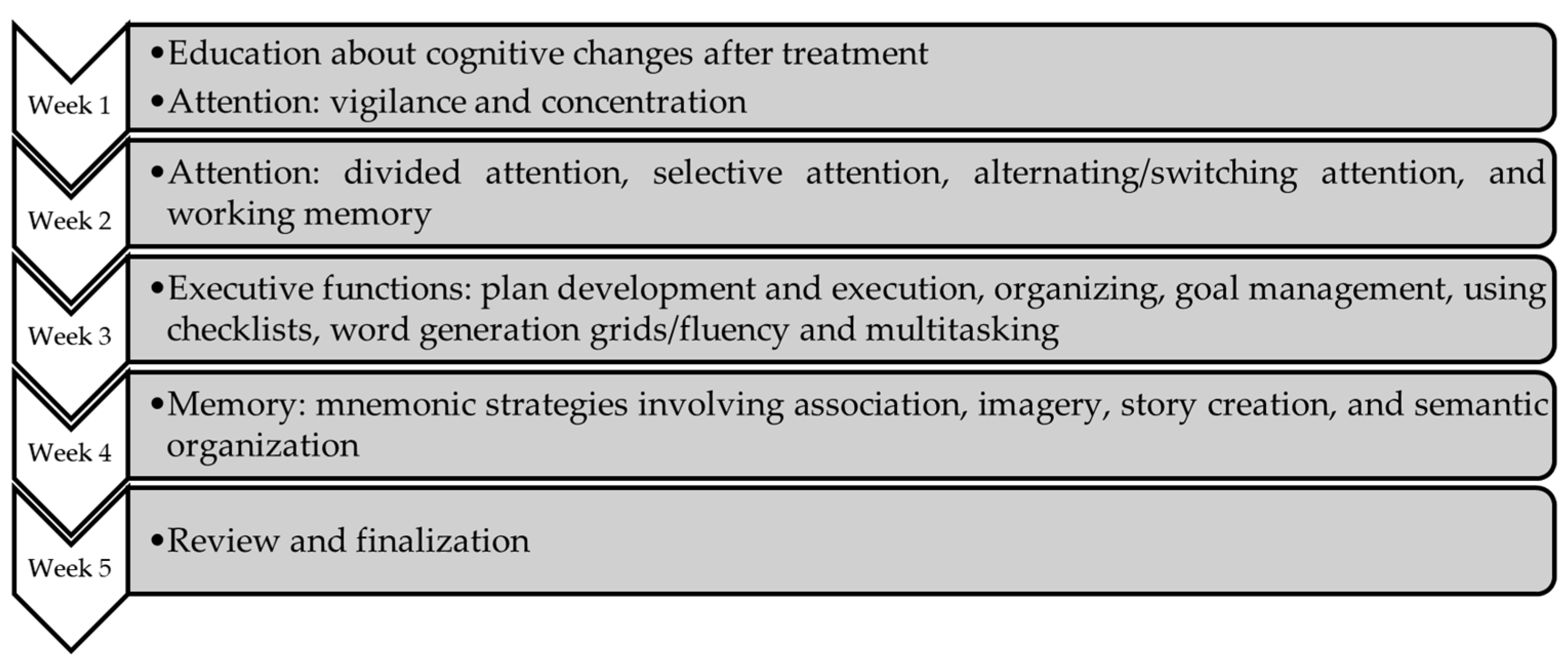
| What | The UCLA Cognitive Rehabilitation Intervention Program targets the most common complaints of cancer survivors (see Figure 1) and consists of three main components: (1) weekly education about cognitive functions at the beginning of each week related to the specific topic to be discussed (i.e., attention, executive functions, and memory) and training in technique instruction (e.g., deep breathing, muscle relaxation, countering negative thoughts); (2) in-class and homework cognitive exercises with three difficulty levels (level I—easy, level II—moderate and level III—difficult; levels I and II are performed in class to provide mastery experience, receive encouragement and support, engendering confidence and familiarity with the process; additional exercises of the three levels are assigned for homework); and (3) goal setting (short- and long-term goals, reviewed weekly and at the end of the intervention, respectively). Each of the components was derived from prior research on cognitive rehabilitation. Each session starts with a homework review (except week 1), followed by education, strategy training, in-class exercises, goal setting, and homework discussion. This intervention is a manualized program with teaching materials for the participants; the intervention manual was specifically developed for the program. There are four materials: Training Manual, Class Handouts, Home Practice Exercises, and Answer Keys, including audio files for cognitive exercises. Each participant receives a workbook with homework exercises, CDs for auditory exercises, answer keys, and a stopwatch for timing when needed. The participants are assigned homework relevant to their daily lives to make it easier to face challenges at home or work using strategies. Likewise, they are assigned exercises not discussed in class and are asked to set goals concerning specific daily life tasks that they need to accomplish. For the homework sessions, the participants are asked to track their homework practice on a log provided for them, explaining the importance of self-paced and distributed practice, and suggesting attempting at least four 20-min sessions per week of homework. The intervention is delivered by trained clinicians who use the Training Manual to guide them during the sessions. The manual includes references to handouts, which are printed and given to each participant, where they can give their answers to the exercises performed in class. |
| Who Provided | Intervention clinicians deliver the program. Clinicians are trained in the intervention content and monitored for the fidelity of delivery. |
| How | The intervention consists of five weekly sessions over five consecutive weeks. The intervention is delivered in a face-to-face small group format (3–9 participants) by trained clinicians. |
| Where | Face-to-face sessions take place at health or research facilities. |
| When and How Much | The intervention consists of five sessions over five consecutive weeks. Each session has 2 h in duration. Each component of the program has an approximate duration to be completed. |
| How Well | The feasibility study of the intervention showed promising results, being well-received and well-tolerated based on participants’ comments, their regular attendance, and the low attrition rate [27]. A randomized clinical trial evaluating the efficacy of the intervention compared with a waitlist control condition on cognitive complaints, and neuropsychological and brain functioning in breast cancer survivors was also conducted. Participants included in the intervention group showed immediate and sustained improvements in self-reported cognitive complaints and memory functioning on neurocognitive testing. These data were supported by the results of a quantitative electroencephalography (qEEG) substudy, providing some support for neurophysiological changes underlying the improvements in function associated with the intervention [28]. |
| Content of the Original Program | Cultural Adaptation | Reasons for Adaptation and Content Adapted |
|---|---|---|
| WEEK 1—ATTENTION | ||
| Auditory Attention Exercises (Home Practice Exercises) | ||
| 1. “The County Fair Story”—instruction “Listen for and mark each occurrence of the word “they”.” | “The County Fair Story” [PT-EU: “A História da Feira Popular”]—instruction “Listen for and mark each occurrence of the word “in” (PT-EU “na”).”. | With the translation, the word “they” does not exist throughout the text. Since the word “they” is a pronoun, a word that was repeated the same number of times and that was similar in difficulty to a pronoun (i.e., a preposition) was found. Theme and plot are maintained, while the following elements were adapted to the local culture:
|
| 2. “The Mechanic Story” | “The Mechanic Story” [PT-EU: “A História do Mecânico”]. Translated, with minor adaptations. | Theme and plot are maintained while the following element was adapted to the European unit of measurement:
|
| 3. “Art Institute of Chicago Story”—instruction “Listen for and mark each occurrence of the word “Chicago”.” | “Serralves Museum of Contemporary Art” [PT-EU: “O Museu de Arte Contemporânea de Serralves”]. “Listen for and mark each occurrence of the word “Serralves”.”. | The text was changed by a text about a similar Portuguese museum to improve the cultural identification by the Portuguese population. The theme is maintained (i.e., a contemporary art museum), but because the object of the informative text is changed, all the information transmitted to the listener also changes. |
| 4. “Maine Lighthouse Story”—instruction “Listen for and mark each occurrence of the word “would”.” | “Barra Lighthouse Story” (PT-EU “A História do Farol da Barra”)—instruction “Listen for and mark each occurrence of the word “lighthouse keeper” (PT-EU “faroleiro”).” | In PT-EU, the word “would” does not exist. Since the word “would” is a modal verb, a word that was repeated the same number of times and that was similar in difficulty to a verb (i.e., a noun) was found. The theme and plot are maintained, while the following elements were adapted to the local culture, language and characteristics of the object being described:
|
| 5. “African Violets” | “African Violets” [PT-EU: “A História das Violetas-Africanas”]. Translated. | Translated. |
| 6. “The Ginkgo Tree Story” | “The Ginkgo Tree Story” [PT-EU: “A História da Árvore Ginkgo”]. Translated, with minor adaptations. | The part of the text that referred to the US was adapted to Europe/Portugal. |
| WEEK 3—EXECUTIVE FUNCTIONS | ||
| Checklist exercise: “Easy Sugar Cookie Recipe” (Training Manual) | “Easy Lemon Cookie Recipe” | The recipe for cookies was replaced by a very common recipe that was found online. The ingredients and utensils of the recipe were changed to best fit Portuguese customs. |
| Checklist exercise: “Plan a Pot-Luck Bar-B-Q” (Training Manual and Home Practice Exercises) | Translated, with major adaptations. | Although bar-b-qs are a very common practice in Portugal, their organization is somewhat different. First, the budget and the food prices were changed from American dollars to euros. Then, the main dish, appetizers, side dishes, beverages, and desserts were changed to best fit Portuguese customs. |
| Visual Multitasking Exercises (Home Practice Exercises) | ||
| 1. “The County Fair”—instructions “Circle words that are numbers (e.g., one or 1); Underline words that are food or drinks; Cross off the names of Fair rides.”. | Same as week 1 | Same as week 1. Instructions are the same as the originals. |
| 2. “The Art Institute of Chicago”—instructions “Underline “Chicago”; Cross-out the word “art”.” | Same as week 1. Instructions “Underline “Serralves”; Cross-out the word “art”.” | Same as week 1. Instructions were adapted accordingly, substituting “Chicago” by “Serralves”. |
| 3. “Poem Tree, Tree by Federico García Lorca”—instructions “Circle colors; Underline “girl”.” | “Poem Adeus by Eugénio de Andrade”—instructions “Circle body parts; Underline “clouds”.” | The genre is maintained as in the original program but the text is replaced by a poem originally written in Portuguese. The main objective was to use a poem that would allow proposing and replicating similar exercises to those in the original program (i.e., to circle/underline/cross off specific words). Instructions were adapted accordingly. |
| 4. “The Mechanic”—instructions “Circle numbers; Underline tools; Cross-out types of clothing.” | Same as week 1. | Same as week 1. Instructions are the same as the originals. |
| 5. “Geography of South America”—instructions “Circle types of animals; Underline numbers; Cross-out types of water formations.” | Translated, with minor adaptations. | Theme and information given were maintained while the following element was updated:
|
| 6. “Canning”—instructions “Circle the word “lid”; Underline the word “canning”; Cross-out types of food.” | “Canned Food” [PT-EU “Comida em Conserva ou Enlatada”]—instructions “Circle the word “can” (PT-EU “latas”; Underline the word “canned” (PT-EU “enlatada”); Cross-out types of food.” | The text was initially translated, but it was later changed since home canning, as occurs in the US, is not common in Portugal (i.e., several processes are unfamiliar to the Portuguese population). Therefore, it was replaced by canned food, which is similar to home canning. Canned food is very common in Portugal. Instructions were adapted accordingly. |
| 7. “African Violets”—instructions “Circle the word “violet” (or “violets”); Underline colors; Cross-out numbers.” | Same as week 1. | Same as week 1. Instructions are the same as the originals. |
| 8. “The Ginkgo Tree”—instructions “Circle the word “Ginkgo” (or “Ginkgos”); Underline parts of plants; Cross-out the word “and”.” | Same as week 1. | Same as week 1. Instructions are the same as the originals. |
| 9. “The Maine Lighthouse”—instructions “Circle professions; Underline animals; Cross-out words that have to do with time.” | “The Barra Lighthouse” (PT-EU “O Farol da Barra”)—instructions “Circle professions; Underline animals; Cross-out words that have to do with time.” | The text was changed to a Portuguese lighthouse located in Aveiro, the Barra Lighthouse. The text was only adapted when it referred to information about Maine and animals. Instructions were adapted accordingly. |
| 10. “Zebras and Zebra Stripes”—instructions “Circle the word “stripes” (or “stripe”); Cross-out the word “Zebras” (or “Zebra”).” | Translated. | Instructions are the same as the originals. |
| 11. “Volcanic Plugs”—instructions “Circle the names of countries or states; Underline the word plug (or plugs); Cross-out the word “the”.” | “Volcanic Calderas” [PT-EU: “Caldeiras Vulcânicas”]—instructions “Circle the names of continents, countries or cities/islands; Underline the word “caldera” (PT-EU “caldeira”) (or “calderas”; PT-EU “caldeiras”); Cross-out the word “the”.” | The original text, when translated into PT-EU, raised many doubts because several technical terms did not have a specific Portuguese translation. After consulting a professor of Geology, it was decided to change that text for one with a similar theme which included examples from Portugal (Azores). Instructions were adapted accordingly. |
| Auditory Multitasking Exercises (Home Practice Exercises) | ||
| 1. Sunset (Poem by Lawrence Dunbar) | A Dor que a Minha Alma Sente (Poem by Luís Vaz de Camões) | The genre is maintained but the texts are replaced by poems originally written in Portuguese. Rather than maintaining the theme, the main objective was to use poems that would allow the implementation of the exercises in the original program (i.e., count repeated or specific words and listen for a given word and report the text that follows). Instructions were also changed according to the texts, but the research team tried to keep as faithful as possible to the original. |
| 2. Ozymandius of Egypt (Poem by Percy Shelley) | Poema (Poem by Sophia de Mello Breyner Andresen) | The genre is maintained but the texts are replaced by poems originally written in Portuguese. Rather than maintaining the theme, the main objective was to use poems that would allow the implementation of the exercises in the original program (i.e., count repeated or specific words and listen for a given word and report the text that follows). Instructions were also changed according to the texts, but the research team tried to keep as faithful as possible to the original. |
| 3. The Tiger (Poem by William Blake) | Tenho Tanto Sentimento (Poem by Fernando Pessoa) | The genre is maintained but the texts are replaced by poems originally written in Portuguese. Rather than maintaining the theme, the main objective was to use poems that would allow the implementation of the exercises in the original program (i.e., count repeated or specific words and listen for a given word and report the text that follows). Instructions were also changed according to the texts, but the research team tried to keep as faithful as possible to the original. |
| 4. The Great Zimbabwe (informational paragraph) | The Rome Coliseum (informational paragraph) | The genre is maintained (i.e., information about world history) but replaced by informational text about a European place. |
| 5. Mesa Verde (informational paragraph) | Ruins of Conímbriga (informational paragraph) | The genre is maintained (i.e., information about travel destination with archaeological history) but replaced by analogous informational text about a Portuguese place (i.e., an archaeological place in Portugal). |
| 6. Plato, the Story of a Cat (Story by A.S. Downs) | O Pastor feito Mercador (short story of Portuguese folklore by an unknown author) | The genre is maintained (i.e., traditional story) but replaced by a traditional short story of the Portuguese folklore that would allow implementing the exercises in the original program (i.e., questions about the content of the story). |
| 7. Ice on Mars (informational paragraph) | Ice on Mars (informational paragraph) | Translated. The research team tried to keep the texts simple and without English words to facilitate comprehension. |
| 8. Zebras and Zebra Stripes (informational paragraph) | Zebras and Zebra Stripes (informational paragraph) | Translated. The research team tried to keep the texts simple and without English words to facilitate comprehension. |
| 9. Kaleidoscopes | Kaleidoscopes | Translated. The research team tried to keep the texts simple and without English words to facilitate comprehension. Some instructions were also adapted (e.g., two questions referred to information regarding two personalities with foreign names, but since the names were in English, these questions were adapted). |
| 10. Igloos | Igloos | Translated. The research team tried to keep the texts simple and without English words to facilitate comprehension. |
| 11. Invention of the Wheel | Invention of the Wheel | Translated. The research team tried to keep the texts simple and without English words to facilitate comprehension. |
| WEEK 4—MEMORY | ||
| License plate number is: ZOD336 (Training Manual) | License plate number is: CA 59 LP | The license plate number was changed for the Portuguese context. |
| Get a key made for your long-lost cousin who will visit (Training Manual) | Get a key made for the younger son that goes to school | Getting a key for a cousin is not a Portuguese habit. |
| Make reservations for Sushi (Training Manual) | Make reservations for seafood restaurant | Although sushi is becoming more common in Portugal, it is more common to go eat shellfish (especially among 40–65 years). |
| Brunch (Training Manual) | Lunch | Brunch is also very common only for younger generations. |
| “Snakebite Junction” by Harry Kissinger (Home Practice Exercises) | Mar Me Quer by Mia Couto | The name was changed to a Portuguese name. |
| Crocker Canyon Exit off the 52 East Freeway (Home Practice Exercises) | Saída para Paço de Arcos da A5 em direção a Cascais | The name of the streets was adapted. |
| Chinese Restaurant called Ming How (Home Practice Exercises) | A Brazilian Restaurant called Estrela do Sul (Star of the South) | Although Chinese restaurants are becoming more familiar in Portugal, some people do not go to or know Chinese food. |
| Beecher Ave. (Home Practice Exercises) | Avenida de Ceuta | The name of the street was adapted. |
| Phone number 368-7621 (Home Practice Exercises) | Phone number 234370200 | The phone number was adapted. |
| Baseball mitt (Home Practice Exercises) | Soccer gloves | Soccer is more common in Portugal. |
| John Wayne (Home Practice Exercises) | Nicolau Breyner | Actor adapted. |
| Marshmallow (Home Practice Exercises) | Candy | Marshmallow is not very common in Portugal. |
| Washington Monument (Home Practice Exercises) | Torre de Belém | Monument in the country’s capital. |
| Week | 1. Sensitiveness (Mdn) | 2. Clarity and Comprehensibility (Mdn) | 3. Familiarity and Accessibility (Mdn) | 4. Precision (Mdn) | 5. Cultural Adequacy (Mdn) | 6. Adequacy of Cognitive Exercises (Mdn) |
|---|---|---|---|---|---|---|
| #1 | 4 | 3.5 | 3.5 | 4 | 4 | 3.5 |
| #2 | 4 | 3 | 3.5 | 4 | 4 | 3 |
| #3 | 3.5 | 4 | 4 | 3.5 | 4 | 3 |
| #4 | 4 | 3 | 3 | 3.5 | 4 | 3 |
| #5 | 4 | 4 | 4 | 4 | 4 | 3 |
| Global program | 4 | 3 | 4 | 3 | 4 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, A.F.; Sosa-Napolskij, M.; Torres, A.; Queiroz, D.F.; Bártolo, A.; Sousa, H.; Monteiro, S.; Van Dyk, K.; Ercoli, L.M.; Santos, I.M. CanCOG®: Cultural Adaptation of the Evidence-Based UCLA Cognitive Rehabilitation Intervention Program for Cancer Survivors in Portugal. Healthcare 2023, 11, 141. https://doi.org/10.3390/healthcare11010141
Oliveira AF, Sosa-Napolskij M, Torres A, Queiroz DF, Bártolo A, Sousa H, Monteiro S, Van Dyk K, Ercoli LM, Santos IM. CanCOG®: Cultural Adaptation of the Evidence-Based UCLA Cognitive Rehabilitation Intervention Program for Cancer Survivors in Portugal. Healthcare. 2023; 11(1):141. https://doi.org/10.3390/healthcare11010141
Chicago/Turabian StyleOliveira, Ana F., Milaydis Sosa-Napolskij, Ana Torres, Diâner Felipe Queiroz, Ana Bártolo, Helena Sousa, Sara Monteiro, Kathleen Van Dyk, Linda M. Ercoli, and Isabel M. Santos. 2023. "CanCOG®: Cultural Adaptation of the Evidence-Based UCLA Cognitive Rehabilitation Intervention Program for Cancer Survivors in Portugal" Healthcare 11, no. 1: 141. https://doi.org/10.3390/healthcare11010141