
Validation of the Portuguese Version of the Fear of Progression Questionnaire-Short Form (FoP-Q-SF) in Portuguese Cancer Survivors

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.2.1. Socio-Demographic and Clinical Questionnaire
2.2.2. Fear of Progression Questionnaire-Short Form (FoP-Q-SF)
2.2.3. Comparative Measures
Hospital Anxiety and Depression Scale (HADS)
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30 (EORTC QLQ-C30)
Post-Traumatic Stress Disorder Checklist-Civilian Version (PCL-C)
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Preliminary Analysis: Item Properties and Reliability
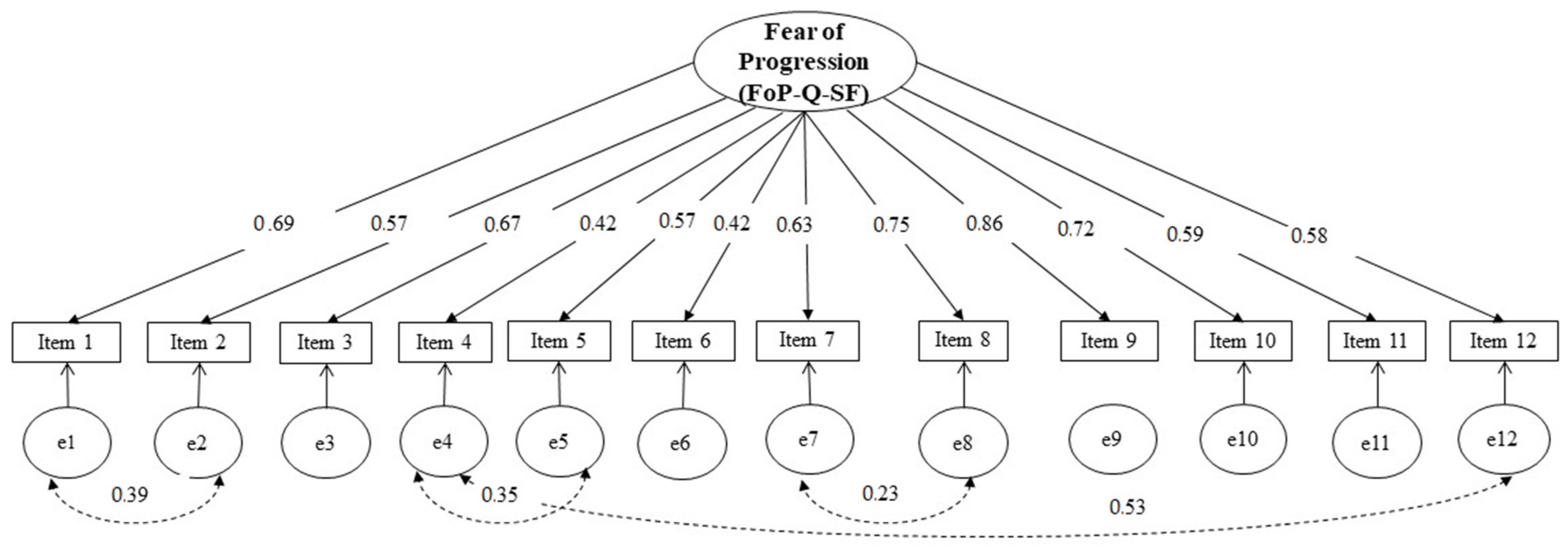
3.3. Confirmatory Factor Analysis
3.4. Convergent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| FoP-Q-SF (Mehnert et al., 2006; Portuguese Version: Silva, Bártolo, Santos, Paiva, & Monteiro, 2022) | Nunca | Raramente | Algumas Vezes | Frequentemente | Muito Frequentemente |
|---|---|---|---|---|---|
| 1. Fico ansioso se penso que a minha doença poderá progredir. | |||||
| 2. Fico nervoso antes das consultas médicas ou exames periódicos. | |||||
| 3. Tenho medo da dor. | |||||
| 4. Tenho preocupações relativas ao alcance dos meus objetivos profissionais por causa da minha doença. | |||||
| 5. Quando estou ansioso, tenho sintomas físicos: ex: coração a bater rápido, dor no estômago, nervosismo. | |||||
| 6. Perturba-me a possibilidade dos meus filhos terem a minha doença. | |||||
| 7. Incomoda-me que possa ter que depender de estranhos para atividades do dia-a-dia. | |||||
| 8. Estou preocupado que em algum momento da minha doença, eu não possa mais continuar com os meus hobbies. | |||||
| 9. Tenho medo de tratamentos severos no curso da minha doença. | |||||
| 10. Preocupa-me que a minha medicação possa prejudicar o meu organismo. | |||||
| 11. Eu preocupo-me com o que será da minha família se alguma coisa me acontecer. | |||||
| 12. O pensamento de que eu poderei não ser mais capaz de trabalhar devido à minha doença, perturba-me. |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, N.; Portugal, C.; Nogueira, P.J.; Farinha, C.S.; Oliveira, A.L.; Alves, M.I.; Martins, J. Portugal Doenças Oncológicas Em Números–2015; Direção-Geral da Saúde: Lisboa, Portugal, 2016. [Google Scholar]
- PORDATA Óbitos de Residentes Em Portugal Por Algumas Causas de Morte. Available online: https://www.pordata.pt/Portugal/%C3%93bitos+de+residentes+em+Portugal+por+algumas+causas+de+morte-156 (accessed on 7 October 2022).
- McCorkle, R.; Ercolano, E.; Lazenby, M.; Schulman-Green, D.; Schilling, L.S.; Lorig, K.; Wagner, E.H. Self-Management: Enabling and Empowering PatientsLiving With Cancer as a Chronic Illness. CA A Cancer J. Clin.-Manag. 2011, 61, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Miranda, N.; Gonçalves, M.B. Programa Nacional Para as Doenças Oncológicos; Direção Geral de Saúde: Lisboa, Portugal, 2017. [Google Scholar]
- Linden, W.; Vodermaier, A.; MacKenzie, R.; Greig, D. Anxiety and Depression after Cancer Diagnosis: Prevalence Rates by Cancer Type, Gender, and Age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Wagner, T.; Augustin, M.; Blome, C.; Forschner, A.; Garbe, C.; Gutzmer, R.; Hauschild, A.; Heinzerling, L.; Livingstone, E.; Loquai, C.; et al. Fear of Cancer Progression in Patients with Stage IA Malignant Melanoma. Eur. J. Cancer Care 2018, 27, e12901. [Google Scholar] [CrossRef] [PubMed]
- Herschbach, P.; Berg, P.; Dankert, A.; Duran, G.; Engst-Hastreiter, U.; Waadt, S.; Keller, M.; Ukat, R.; Henrich, G. Fear of Progression in Chronic Diseases. J. Psychosom. Res. 2005, 58, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Herschbach, P.; Dinkel, A. Fear of Progression. In Psycho-Oncology; Recent Results in Cancer Research; Springer: Berlin/Heidelberg, Germany, 2014; Volume 197, pp. 11–29. ISBN 978-3-642-40186-2. [Google Scholar]
- Mehnert, A.; Herschbach, P.; Berg, P.; Henrich, G.; Koch, U. Progredienzangst bei Brustkrebspatientinnen-Validierung der Kurzform des Progredienzangstfragebogens PA-F-KF/ Fear of progression in breast cancer patients–validation of the short form of the Fear of Progression Questionnaire (FoP-Q-SF). Z. Für Psychosom. Med. Und Psychother. 2006, 52, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Mehnert, A.; Ernst, J.; Herschbach, P.; Schulte, T. Fear of Progression in Patients 6 Months after Cancer Rehabilitation—A Validation Study of the Fear of Progression Questionnaire FoP-Q-12. Support Care Cancer 2015, 23, 1579–1587. [Google Scholar] [CrossRef] [PubMed]
- Mahendran, R.; Liu, J.; Kuparasundram, S.; Griva, K. Validation of the English and Simplified Mandarin Versions of the Fear of Progression Questionnaire–Short Form in Chinese Cancer Survivors. BMC Psychol. 2020, 8, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, N.A.; Hamdan, N.A. Validation of the Malay Version of the Fear of Progression Questionnaire-Short Form (FoP-Q-SF-M) in Malaysian Cancer Patients. Malays. J. Med. Health Sci. 2021, 17, 16–21. [Google Scholar]
- Pais-Ribeiro, J.; Silva, I.; Ferreira, T.; Martins, A.; Meneses, R.; Baltar, M. Validation Study of a Portuguese Version of the Hospital Anxiety and Depression Scale. Psychol. Health Med. 2007, 12, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Pais-Ribeiro, J.; Pinto, C.; Santos, C. Validation Study of the Portuguese Version of the QLC-C30-V.3. Psicol. Saúde Doenças 2008, 9, 89–102. [Google Scholar]
- Marcelino, D.; Gonçalves, S.P. Perturbação pós-stress traumático: Características psicométricas da versão portuguesa da Posttraumatic Stress Disorder Checklist–Civilian Version (PCL-C). Rev. Port. Saúde Pública 2012, 30, 71–75. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition-Text Revision (DSM-IV-TR); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Nunnaly, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Li, C.-H. The Performance of ML, DWLS, and ULS Estimation with Robust Corrections in Structural Equation Models with Ordinal Variables. Psychol. Methods 2016, 21, 369–387. [Google Scholar] [CrossRef] [PubMed]
- Kline, R. Principles and Practice of Structural Equation Modeling, 2nd ed.; The Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modelling with AMOS: Basic Concepts, Applications, and Programming, 3rd ed.; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Babyak, M.A.; Green, S.B. Confirmatory Factor Analysis: An Introduction for Psychosomatic Medicine Researchers. Psychosom. Med. 2010, 72, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Krauss, O.; Hauss, J.P.; Höckel, M.; Kortmann, R.D.; Stolzenburg, J.U.; Schwarz, R. Anxiety and Depression in Cancer Patients Compared with the General Population: Anxiety and Depression in Cancer Patients. Eur. J. Cancer Care 2009, 19, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, A.; Koch, U.; Sundermann, C.; Dinkel, A. Predictors of Fear of Recurrence in Patients One Year after Cancer Rehabilitation: A Prospective Study. Acta Oncol. 2013, 52, 1102–1109. [Google Scholar] [CrossRef] [PubMed]
- Lebel, S.; Ozakinci, G.; Humphris, G.; Mutsaers, B.; Thewes, B.; Prins, J.; Dinkel, A.; Butow, P. From Normal Response to Clinical Problem: Definition and Clinical Features of Fear of Cancer Recurrence. Support Care Cancer 2016, 24, 3265–3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Mahendran, R.; Chua, S.M.; Lam, K.F.; Lim, H.A.; Kuparasundram, S.; Chan, Y.H.; Simard, S.; Kua, E.H.; Griva, K. Validation of the English and Mandarin Versions of the Fear of Cancer Recurrence Inventory in an Asian Population. J. Health Psychol. 2020, 25, 617–628. [Google Scholar] [CrossRef] [PubMed]

| N | % | ||
|---|---|---|---|
| Type of cancer | Breast | 163 | 74.1% |
| Lymphoma | 7 | 3.2% | |
| Colorectal | 6 | 2.7% | |
| Lung | 5 | 2.3% | |
| Kidney | 3 | 1.4% | |
| Stomach | 2 | 0.9% | |
| Uterus | 2 | 0.9% | |
| Leukemia | 1 | 0.5% | |
| Melanoma | 1 | 0.5% | |
| Pancreas | 1 | 0.5% | |
| Prostate | 1 | 0.5% | |
| Bladder | 1 | 0.5% | |
| Sarcoma | 1 | 0.5% | |
| Other | 26 | 11.8% | |
| Disease stage | I | 23 | 10.5% |
| II | 43 | 19.5% | |
| III | 76 | 34.5% | |
| IV | 49 | 22.3% | |
| Unknown to the participant | 29 | 13.2% | |
| Disease phase | Diagnosis | 2 | 0.9% |
| Relapse | 13 | 5.9% | |
| Remission | 128 | 58.2% | |
| Treatment | 77 | 35% | |
| Time in months since diagnosis | ≤12 | 35 | 15.9% |
| >12 e ≤24 | 43 | 19.5% | |
| >24 e ≤36 | 39 | 17.7% | |
| >34 e ≤48 | 23 | 10.5% | |
| >46 e ≤60 | 22 | 9.6% | |
| >60 | 78 | 26.8% |
| Item | M | Min | Max | SD | Skewness | Kurtosis | Corrected Item-Total Correlation | Cronbach’s Alpha If Item Deleted |
|---|---|---|---|---|---|---|---|---|
| 1 | 3.40 | 1 | 5 | 0.981 | 0.063 | −0.523 | 0.621 | 0.845 |
| 2 | 3.69 | 1 | 5 | 1.116 | −0.379 | −0.776 | 0.497 | 0.841 |
| 3 | 3.20 | 1 | 5 | 1.172 | 0.078 | −0.913 | 0.554 | 0.847 |
| 4 | 2.97 | 1 | 5 | 1.407 | −0.021 | −1.278 | 0.438 | 0.857 |
| 5 | 3.40 | 1 | 5 | 1.066 | −0.273 | −0.490 | 0.512 | 0.850 |
| 6 | 3.25 | 1 | 5 | 1.435 | −0.279 | −1.191 | 0.334 | 0.865 |
| 7 | 3.38 | 1 | 5 | 1.286 | −0.301 | −1.026 | 0.553 | 0.847 |
| 8 | 3.27 | 1 | 5 | 1.133 | −0.087 | −0.753 | 0.684 | 0.839 |
| 9 | 3.25 | 1 | 5 | 1.211 | 0.007 | −1.011 | 0.870 | 0.837 |
| 10 | 3.46 | 1 | 5 | 1.280 | −0.370 | −0.860 | 0.592 | 0.845 |
| 11 | 3.85 | 1 | 5 | 1.087 | −0.571 | −0.552 | 0.503 | 0.851 |
| 12 | 3.27 | 1 | 5 | 1.332 | −0.248 | −1.033 | 0.553 | 0.848 |
| Questionnaire Scales | Mean Total Score | FoP-Q-SF |
|---|---|---|
| HADS—Anxiety subscale | 8.79 | 0.687 ** |
| HADS—Depression subscale | 6.04 | 0.480 ** |
| PSPT—Total Score | 2.75 | 0.507 ** |
| PSPT—Reexperience subscale | 2.73 | 0.464 ** |
| PSPT—Avoidance subscale | 2.60 | 0.424 ** |
| PSPT—Hyperactivation subscale | 2.96 | 0.488 ** |
| QLQ—Total Score | 39.38 | 0.380 ** |
| QLQ—Emotional functioning subscale | 49.37 | 0.576 ** |
| QLQ—Physical functioning subscale | 70.68 | 0.470 ** |
| QLQ—Role functioning subscale | 62.00 | 0.386 ** |
| QLQ—Social functioning subscale | 49.37 | 0.541 ** |
| FoP-Q-SF—Total Score | 40.40 | _ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, S.; Bártolo, A.; Santos, I.M.; Paiva, D.; Monteiro, S. Validation of the Portuguese Version of the Fear of Progression Questionnaire-Short Form (FoP-Q-SF) in Portuguese Cancer Survivors. Healthcare 2022, 10, 2466. https://doi.org/10.3390/healthcare10122466
Silva S, Bártolo A, Santos IM, Paiva D, Monteiro S. Validation of the Portuguese Version of the Fear of Progression Questionnaire-Short Form (FoP-Q-SF) in Portuguese Cancer Survivors. Healthcare. 2022; 10(12):2466. https://doi.org/10.3390/healthcare10122466
Chicago/Turabian StyleSilva, Sandra, Ana Bártolo, Isabel M. Santos, Débora Paiva, and Sara Monteiro. 2022. "Validation of the Portuguese Version of the Fear of Progression Questionnaire-Short Form (FoP-Q-SF) in Portuguese Cancer Survivors" Healthcare 10, no. 12: 2466. https://doi.org/10.3390/healthcare10122466