
Assessing Barriers Encountered by Women in Cervical Cancer Screening and Follow-Up Care in Urban Bolivia, Cochabamba

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
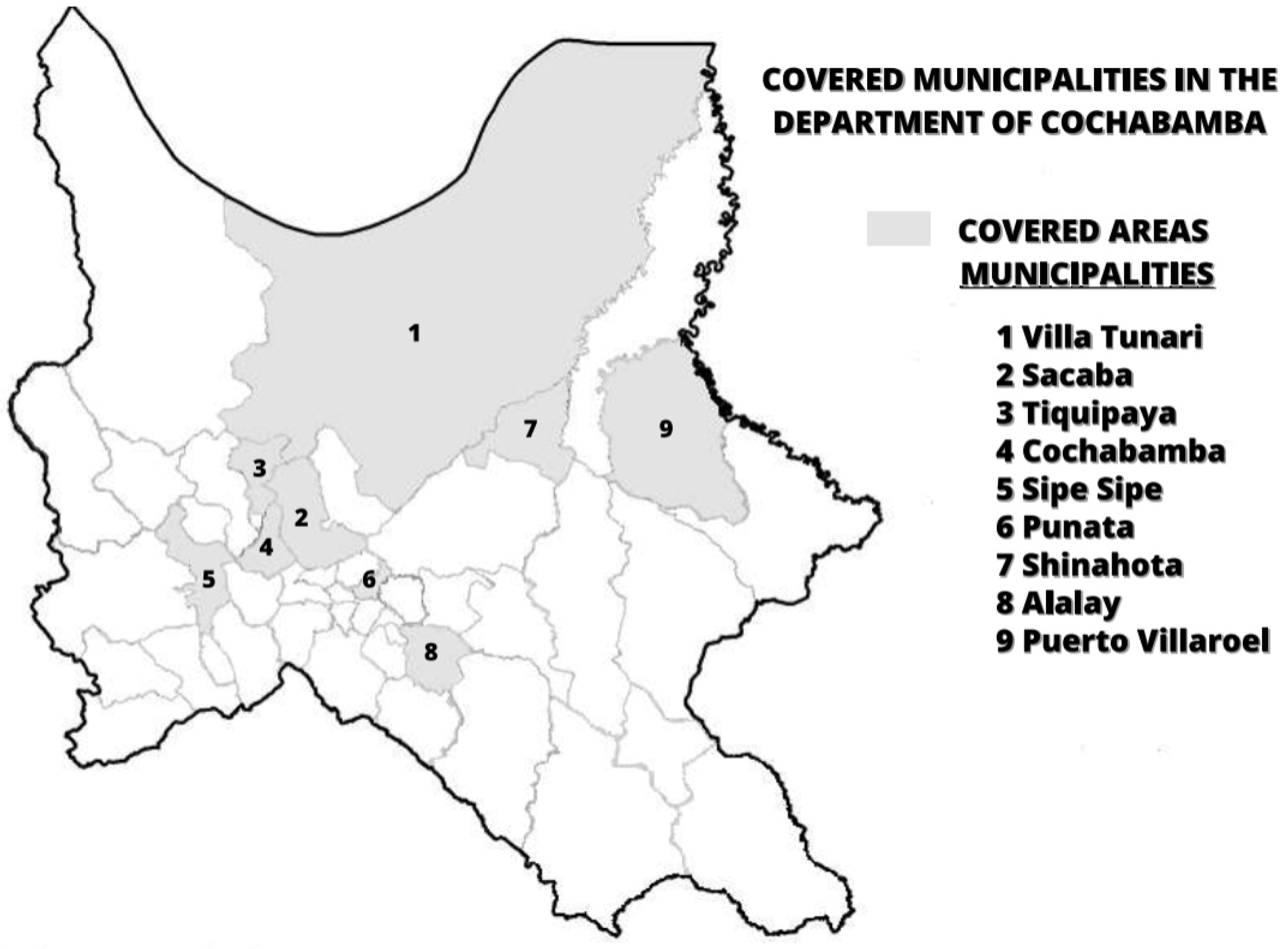
2.1. Study Setting and Design
2.2. Data Collection Tools and Guidelines
2.3. Procedure and Data Collection
2.4. Data Analysis
3. Results
3.1. Preliminary Interviews to Identify Common Patterns Possibly Involved in Reduced Cervical Cancer Screening and Follow-Up Care (Phase 1 Study)
3.1.1. Participant Characteristics
3.1.2. HPV Related Knowledge
“I believe that women don’t come to follow-up mainly because of lack of knowledge, lack of culture, but also because of the cost of the treatment because it is not completely free. They may give good drugs, but they are expensive and therefore not accessible.”
“What scares me is that sometimes they don’t explain you well. It came to a point where I did not understand anything, and I thought the delivery of my results was my death sentence. When I did the Papanicolaou in Tiquipaya (not in the project) the doctors told me that I had lesions and that I had to follow a treatment but did not tell me why I had to follow this treatment.”Woman #3
“HPV is a sexually transmitted virus. I don’t know what the risks of infection are. I got this information from my sister who is a nurse.”Woman #5
“I would like the explanations to be given in Quechua because here in the countryside people speak Quechua. I would also like them to explain things to us using a mannequin to be able to visualize the explanations that the doctors give.”Promotora #1
3.1.3. Traditional Practitioners
“In any case, patients do not have much confidence in what the health center does, and they prefer to be tested in a private institution.”HCP #9
“I would not agree that the doctor works with a traditional healer. I do not think the church, or my faith can cure diseases. I think there should be more medical attention.”Woman #1, woman screened within the pilot project
3.1.4. Treatment, Mistrust and Care Practices
“Some patients coming for screening already had a hysterectomy following Papanicolaou results. Doctors don’t have the right information to perform hysterectomies.”HCP #1
“In patients over 50, we perform hysterectomy because they no longer need it [the uterus].” HCP #9. Another HCP revealed: “the results showed that she had initial cancer, she was given a hysterectomy and now she is fine.”HCP #8
“The test result said: highly at risk or something like that. I was told to go that day, but I could not. I then went another day, but the staff was no longer there.”Woman #11
“I’m 27 years old. I did the HPV self-sampling test, it was positive. I was sent to Cochabamba Hospital and the doctor did an operation to remove my womb (uterus). I did not want to do the hysterectomy (…) The infection was low grade. The doctor told me that there were worms in my uterus and that it was going to cause me cancer.”Woman #15
3.1.5. Barriers to Access Health Care
“In our health center, we do not have a specialized gynecologist, the people who take care of the women are general practitioners and they are the ones who do the tests.”HCP #6 at Pucarita
“The lab had the results in two weeks, but we could only get them once a month. Sometimes the results were given in a month and sometimes it even took longer.”HCP #2
“The money, being a widow with children, and the distance from the hospital where the free follow-up was done kept this woman from going for the follow-up.”Promotora #1
“Treatment is free until it is an invasive cancer. After that, the patient must pay. The treatment is very expensive and not included in the free insurance because the government cannot pay.”HCP #9
“I did the self-sampling at Villa-Tunari, I received the results. I was thinking of going to the follow up, but I don’t know where it is.”Woman #7
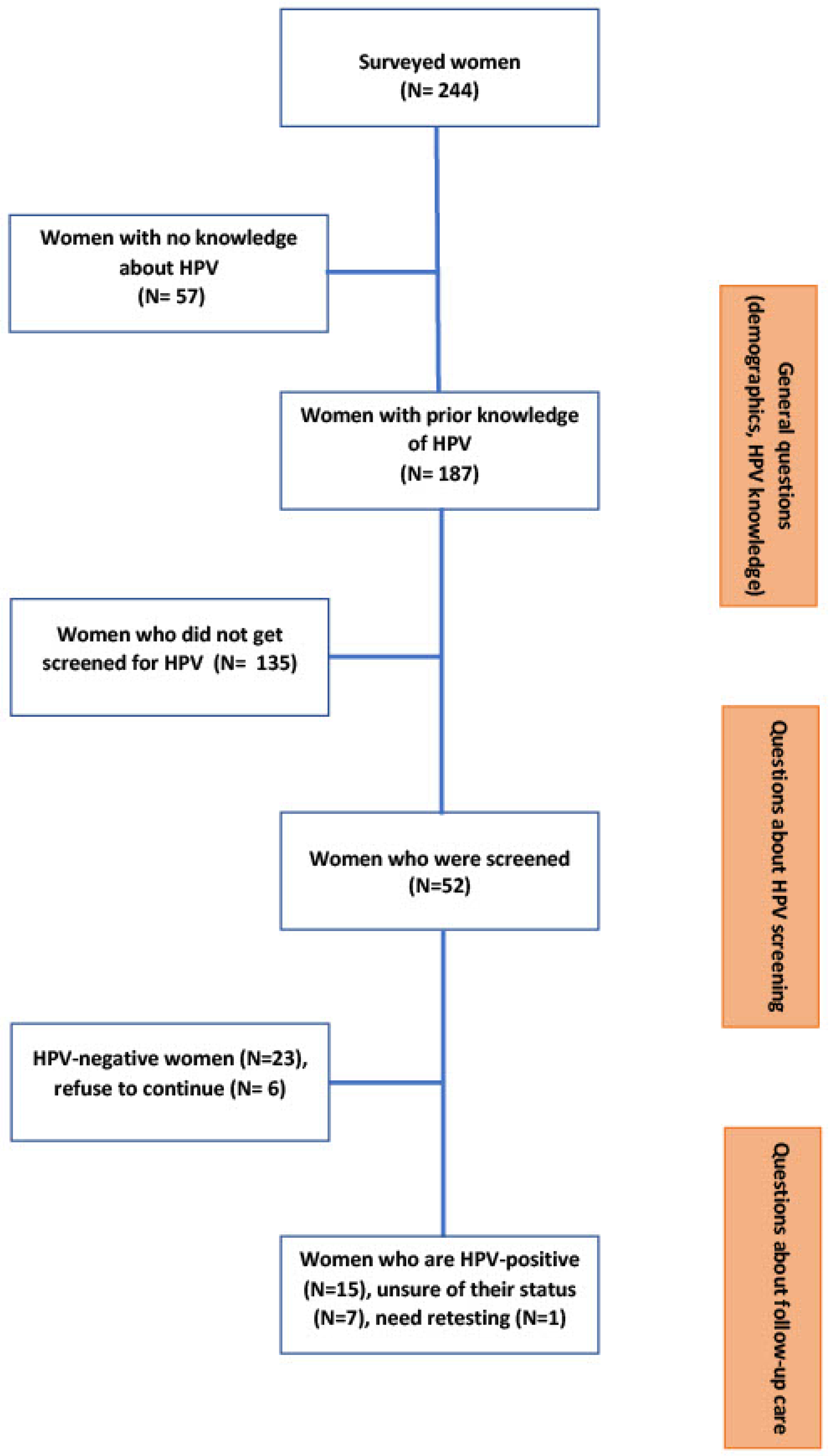
3.2. Surveys to Verify Common Patterns Possibly Involved in Reduced Cervical Cancer Screening and Follow-Up Care (Phase 2 Study)
3.2.1. Participant Characteristics
3.2.2. HPV Related Knowledge
3.2.3. Traditional Practitioners
3.2.4. Treatment, Mistrust and Care Practices
3.2.5. Barriers to Access Health Care
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- WHO. Cervical Cancer Bolivia (Plurinational State of) 2021 Country Profile; Technical Report; WHO: Geneva, Switzerland, 17 November 2021; Available online: https://www.who.int/publications/m/item/cervical-cancer-bol-country-profile-2021 (accessed on 1 January 2020).
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World. Summary Report 2021. Available online: https://hpvcentre.net/statistics/reports/XWX.pdf (accessed on 22 October 2021).
- Dzuba, I.G.; Calderón, R.; Bliesner, S.; Luciani, S.; Amado, F.; Jacob, M. A participatory assessment to identify strategies for improved cervical cancer prevention and treatment in Bolivia. Rev. Panam Salud Publica/Pan Am. J. Public Health 2005, 18, 53–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allende, G.; Surriabre, P.; Ovando, N.; Calle, P.; Torrico, A.; Villarroel, J.; Bossens, M.; Fontaine, V.; Rodriguez, P. Evaluation of the effectiveness of high-risk human papilloma self-sampling test for cervical cancer screening in Bolivia. BMC Infect. Dis. 2020, 20, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wentzensen, N.; Arbyn, M. HPV-based cervical cancer screening- facts, fiction, and misperceptions. Prev. Med. 2017, 98, 33–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surriabre, P.; Torrico, A.; Vargas, T.; Ugarte, F.; Rodriguez, P.; Fontaine, V. Assessment of a new low-cost, PCR-based strategy for high-risk human papillomavirus DNA detection for cervical cancer prevention. BMC Infect. Dis. 2019, 19, 842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruun, H.; Elverdam, B. Los Naturistas-Healers Who Integrate Traditional and Biomedical Explanations in Their Treatment in the Bolivian Health Care System. Anthropol. Med. 2006, 13, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.G.; Kumar, A.; Tewari, D.D. An ethnobotanical survey of medicinal plants used in Terai forest of western Nepal. J. Ethnobiol. Ethnomed. 2012, 8, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Instituto Nacional de Estadística. Censo de Población y Vivienda 2012; 2015; BOL-INE-CPV-2012. Available online: https://anda.ine.gob.bo/index.php/catalog/8 (accessed on 1 January 2022).
- Instituto Nacional de Estadística. Bolivia: Estudio temático de salud sexual y reproductiva, Encuentas de Demografía y Salud 2008 y 2016. UNFPA, 2018, ACA–EST–INE. Available online: https://bolivia.unfpa.org/sites/default/files/pub-pdf/Tem%C3%A1tico%20de%20Salud%20Sexual%20%281%29.pdf (accessed on 1 January 2022).
- Nacu, A. À quoi sert le culturalisme? Pratiques médicales et, catégorisations des femmes « migrantes » dans trois maternités franciliennes. Sociol. Trav. 2011, 53, 109–130. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Rajkumar, R.; Esmy, P.O.; Fayette, J.M.; Shanthakumary, S.; Frappart, L.; Thara, S.; Cherian, J. Effectiveness, safety and acceptability of ‘see and treat’ with cryotherapy by nurses in a cervical screening study in India. Br. J. Cancer 2007, 96, 738–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinder, L.F.; Parham, G.P.; Basu, P.; Muwonge, R.; Lucas, E.; Nyambe, N.; Sauvaget, C.; Mwanahamuntu, M.H.; Sankaranarayanan, R.; Prendiville, W. Thermal ablation versus cryotherapy or loop excision to treat women positive for cervical precancer on visual inspection with acetic acid test: Pilot phase of a randomised controlled trial. Lancet Oncol. 2020, 21, 175–184. [Google Scholar] [CrossRef]
- Ciavattini, A.; Morini, S.; Delli Carpini, G.; Del Fabro, A.; Serri, M.; Verdecchia, V.; Cigolot, F.; Cadel, M.; Clemente, N.; Sopracordevole, F. Factors Related to Overtreatment in the See-and-Treat Approach: A Retrospective Multicentric Observational Study. J. Low. Genit. Tract Dis. 2019, 23, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Ebisch, R.M.; Rovers, M.M.; Bosgraaf, R.P.; van der Pluijm-Schouten, H.W.; Melchers, W.J.; van den Akker, P.A.; Massuger, L.F.; Bekkers, R.L. Evidence supporting see-and-treat management of cervical intraepithelial neoplasia: A systematic review and meta-analysis. BJOG 2016, 123, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peral Dorado, F.; Guzmán Herrador, B.; Ruiz-Montero, R.; Fernández Martínez, N.; Padilla Escalante, J.; Salcedo Leal, I. Evaluation of cervical cancer prevention plan in a remote rural area in Bolivia. Actual. Med. 2020, 811, 190–201. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines for Screening and Treatment of Precancerous Lesions for Cervical Cancer Prevention; WHO: Geneva, Switzerland, 2013; ISBN 9789241548694. [Google Scholar]
- Maza, M.; Schocken, C.M.; Bergman, K.L.; Randall, T.C.; Cremer, M.L. Cervical Precancer Treatment in Low- and Middle-Income Countries: A Technology Overview. J. Glob. Oncol. 2016, 3, 400–408. [Google Scholar] [CrossRef]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N. Cervical cancer: ESMO clinical practice guidelines. Ann. Oncol. 2017, 28 (Suppl. S4), IV72–IV83. [Google Scholar] [CrossRef]
- [BO-DS-N1496]; Bolivia: Decreto Supremo Nº 1496, 20 de Febrero de 2013. Available online: https://www.lexivox.org/norms/BO-DS-N1496.html (accessed on 1 January 2021).
- [BO-L-N475]; Bolivia: Ley de Prestaciones Servicios de Salud Integral Del Estado Plurinacional de Bolivia, 30 de Diciembre de 2013. 2013. Available online: https://vdocuments.mx/bo-l-n475.html?page=1 (accessed on 1 January 2021).
- [BO-DS-N1984]; Bolivia: Reglamento a la Ley N° 475, de Prestaciones de Servicios de Salud Integral Del Estado Plurinacional de Bolivia, Ds Nº 1984, 30 de Abril de 2014. 2014. Available online: http://www.ilo.org/dyn/natlex/docs/ELECTRONIC/110619/137636/F-164521750/DS-N1984%20BOLIVIA.pdf (accessed on 1 January 2022).



{kind=link}
{kind=link}
| Categories | Women N = 15 (%) | Promotoras N = 4 (%) | HCP N = 10 (%) | |
|---|---|---|---|---|
| Applied treatment | Hysterectomy | 1 (6.67) | 0 | 7 (70) |
| Cryotherapy | 0.00 | 0 | 1 (10) | |
| Conization | 3 (20.00) | 0 | 1 (10) | |
| Medication | 0.00 | 1 (25) | 0 | |
| Drop-out | 6 (40.00 *) | 0 | 0 | |
| Traditional healers | 1 (6.67) | 0 | 0 | |
| Women’s HPV knowledge | No prior knowledge or low level | 4 (26.67) | 2 (50) | 3 (30) |
| Beliefs and misconception (HIV, HPV = cancer, disease, infidelity) | 0.00 | 2 (50) | 3 (30) | |
| Prior knowledge | 2 (13.33) | 1 (25) | 0 | |
| Good level | 1 (6.67) | 0 | 0 | |
| Traditional practitioners | Never used/Not in favor | 3 (20.00) | 0 | 2 (20) |
| Not frequent/Conditional use | 3 (20.00) | 4 (100) | 2 (20) | |
| Frequent use | 0.00 | 0 | 6 (60) | |
| Open to collaboration between tradi-practitioners and HCP | 2 (13.33) | 1 (25) | 3 (30) | |
| Barriers for testing and treatment/follow-up | Cost of the screening/testing | 0.00 | 2 (50) | 1 (10) |
| Cost of treatments | 1 (6.67) | 0 | 3 (30) | |
| Indirect costs (e.g., transports) | 0.00 | 1 (25) | 0 | |
| Delay to receive results | 6 (40.00) | 0 | 3 (70) | |
| Lack of (trained) staff | 1 (6.67) | 0 | 3 (30) | |
| Lack of material | 0.00 | 0 | 1 (10) | |
| Lack of training | 0.00 | 0 | 0 | |
| Distance to centers | 2 (13.33) | 2 (50) | 2 (20) | |
| Waiting time/Loss of a paid working day | 2 (13.33) | 3 (75) | 2 (20) | |
| The HCP/promotora explanation was insufficient | 8 (53.33) | 3 (75) | 3 (30) | |
| Difficulty to access information | 0.00 | 2 (50) | 0 | |
| Husband or family do not allow patient to come | 0.00 | 1 (25) | 5 (50) | |
| The difficulty of freeing oneself from family obligations | 2 (13.33) | 2 (50) | 2 (20) | |
| The sex of the doctor | 0.00 | 1 (25) | 2 (20) | |
| Healthcare professional attitude/discrimination | 0.00 | 1 (25) | 0 | |
| Cultural or religious barriers | 0.00 | 0 | 4 (40) | |
| Level of education | 0.00 | 0 | 2 (20) | |
| Embarrassment | 3 (20.00) | 2 (50) | 1 (10) | |
| Fear of results/of having a cancer/of getting hysterectomy | 4 (26.67) | 3 (75) | 6 (60) | |
| Distrust | 0 | 1 (25) | 3 (30) | |
| No barriers | 0 | 0 | 0 |
| N = 242 | Predictor | Prior Knowledge of HPV | Being HPV Screened | ||
|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | ||
| Age | 15–20 years old | NA | - | 0.19 ** | 0.5–0.64 |
| 21–35 years old (Ref.) | NA | - | 1 | - | |
| 36–50 years old | NA | - | 1.3 | 0.61–2.77 | |
| Over 50 years | NA | - | 0.55 | 0.12–2.59 | |
| Education | No education | 11.4 * | 1.47–88.44 | NA | - |
| Uncompleted primary education | 0.51 | 0.01–30.2 | NA | - | |
| Uncompleted secondary education | 11.4 * | 1.47–88.44 | NA | - | |
| Primary education | 9.14 *** | 3.3–27.59 | NA | - | |
| Secondary education | 2.86 * | 1.27–6.42 | NA | - | |
| University education | 1 | - | NA | - | |
| Type of Treatment * | Benign Cervical Lesions N = 36 (%) | Invasive Cervical Lesions N = 36 (%) | Uncertain Test Results N = 36 (%) |
|---|---|---|---|
| Hysterectomy | 1 (2.78) | 22 (61.11) | 2 (5.56) |
| Cryotherapy | 10 (27.78) | 5 (13.89) | 1 (2.78) |
| Conization | 10 (27.78) | 6 (16.67) | 1 (2.78) |
| Medication | 15 (41.67) | 3 (8.33) | 4 (11.11) |
| Referral to a specialist/gynecologist | 7 (19.45) | 9 (25) | 5 (13.89) |
| Radiotherapy | 0 | 1 (2.78) | 0 |
| Retesting | 0 | 1 (2.78) | 11 (30.56) |
| None | 2 (5.56) | 1 (2.78) | 9 (25) |
| Reasons * | Screening N = 36 (%) | Follow-Up N = 36 (%) |
|---|---|---|
| Cost of the test or treatment | 9 (25) | 3 (8.33) |
| Lack of material or medications | 7 (19.44) | 6 (16.67) |
| Lack of training to perform the test | 2 (5.56) | 4 (11.11) |
| Work overload | 2 (5.56) | 2 (5.56) |
| Lack of professionals | 2 (5.56) | 1 (2.78) |
| Husband or family do not allow the patient to come | 10 (27.78) | 7 (19.44) |
| Women do not accept a male physician performing the Papanicolaou | 1 (2.78) | 0 |
| Issues retrieving results | 3 (8.33) | 3 (8.33) |
| No barriers | 8 (22.22) | 11 (33.33) |
| Reasons * | Screening N = 187 (%) | Follow-Up N = 15 * (%) |
|---|---|---|
| Cost of test/treatment | 37 (19.79) | 2 (13.33) |
| Cost of transportation | 6 (3.21) | 0 |
| Distance | 15 (8.02) | 4 (26.67) |
| Healthcare professional attitude | 37 (19.79) | 1 (6.67) |
| The HCP explanation was insufficient | 46 (24.6) | 4 (26.67) |
| Husband or family do not allow the patient to come | 1 (0.53) | 0 |
| Waiting time | 50 (26.74) | 3 (20) |
| Difficulties to obtain a day-off from work | 27 (14.44) | 4 (26.67) |
| The difficulty of freeing oneself from one’s family obligations | 13 (6.95) | 1 (6.67) |
| No barriers | 53 (28.34) | 3 (20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bensemmane, S.; Loayza Villarroel, K.; Montaño, K.; Louati, E.; Ascarrunz, C.; Rodriguez, P.; Fontaine, V.; Laokri, S. Assessing Barriers Encountered by Women in Cervical Cancer Screening and Follow-Up Care in Urban Bolivia, Cochabamba. Healthcare 2022, 10, 1604. https://doi.org/10.3390/healthcare10091604
Bensemmane S, Loayza Villarroel K, Montaño K, Louati E, Ascarrunz C, Rodriguez P, Fontaine V, Laokri S. Assessing Barriers Encountered by Women in Cervical Cancer Screening and Follow-Up Care in Urban Bolivia, Cochabamba. Healthcare. 2022; 10(9):1604. https://doi.org/10.3390/healthcare10091604
Chicago/Turabian StyleBensemmane, Sherihane, Katherine Loayza Villarroel, Kevin Montaño, Elyas Louati, Carla Ascarrunz, Patricia Rodriguez, Véronique Fontaine, and Samia Laokri. 2022. "Assessing Barriers Encountered by Women in Cervical Cancer Screening and Follow-Up Care in Urban Bolivia, Cochabamba" Healthcare 10, no. 9: 1604. https://doi.org/10.3390/healthcare10091604