
Measurement of Skin Thickness Using Ultrasonography to Test the Usefulness of Elastic Compression Stockings for Leg Edema in Pregnant Women
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects and Study Approval
2.2. Clinical Characteristics of the Study Participants
2.3. Assessment and Grading of Edema of the Leg before and after Wearing Elastic Compression Stockings
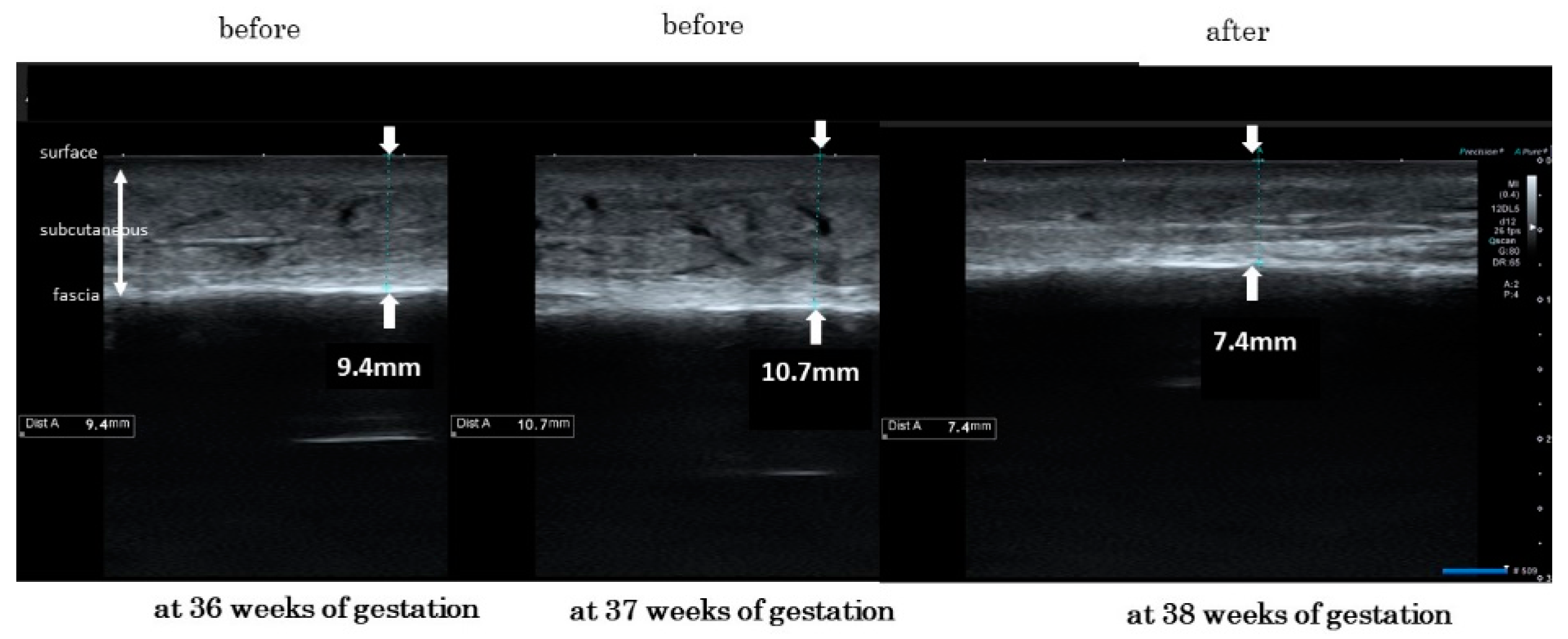
2.4. Measurements of the Skin Thickness in Leg Edema before and after Wearing Elastic Compression Stockings
2.5. Statical Analyses
3. Results
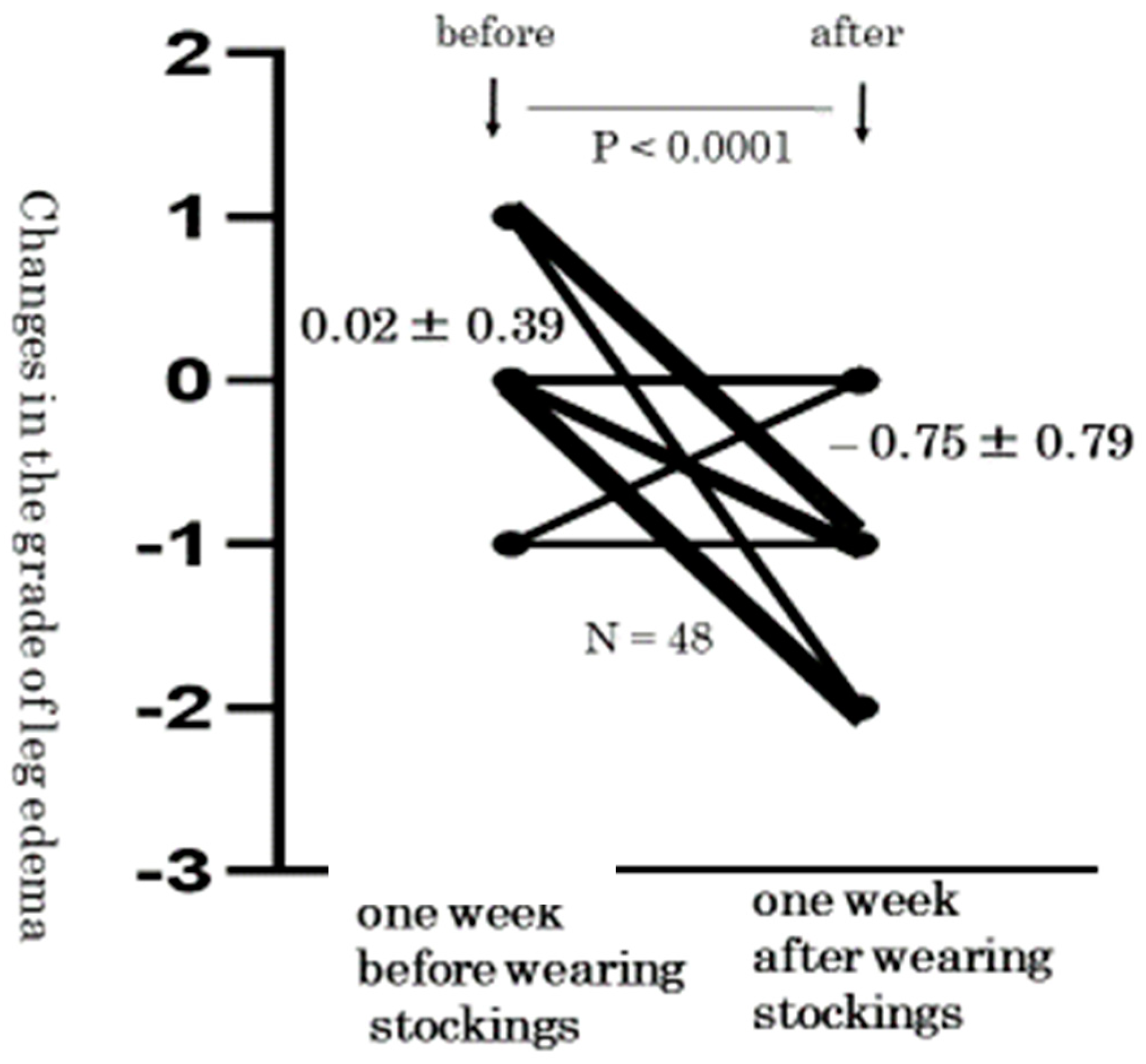
3.1. Level Changes in the Grade of Pitting Edema from before to after the Wearing of Elastic Compression Stockings
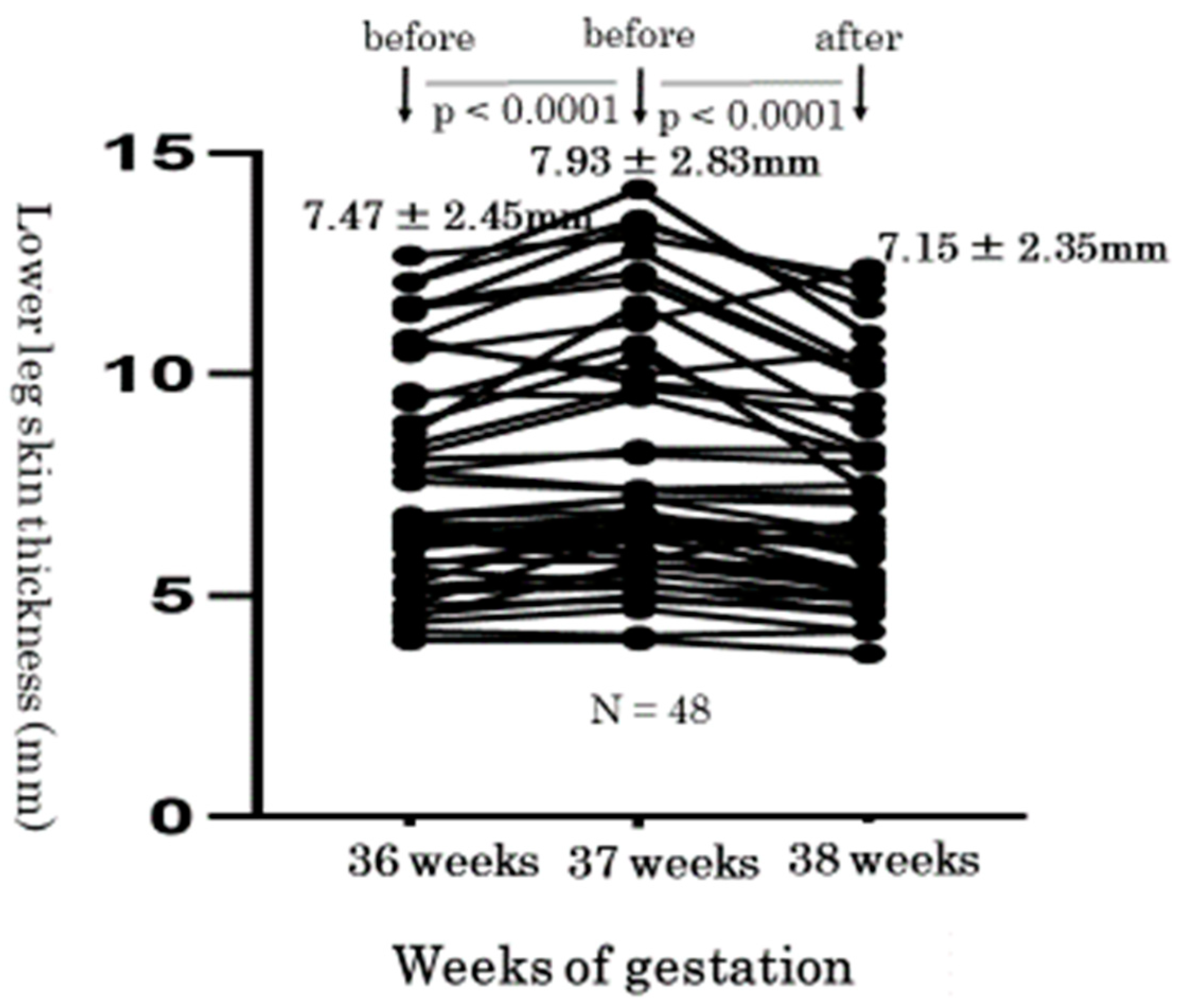
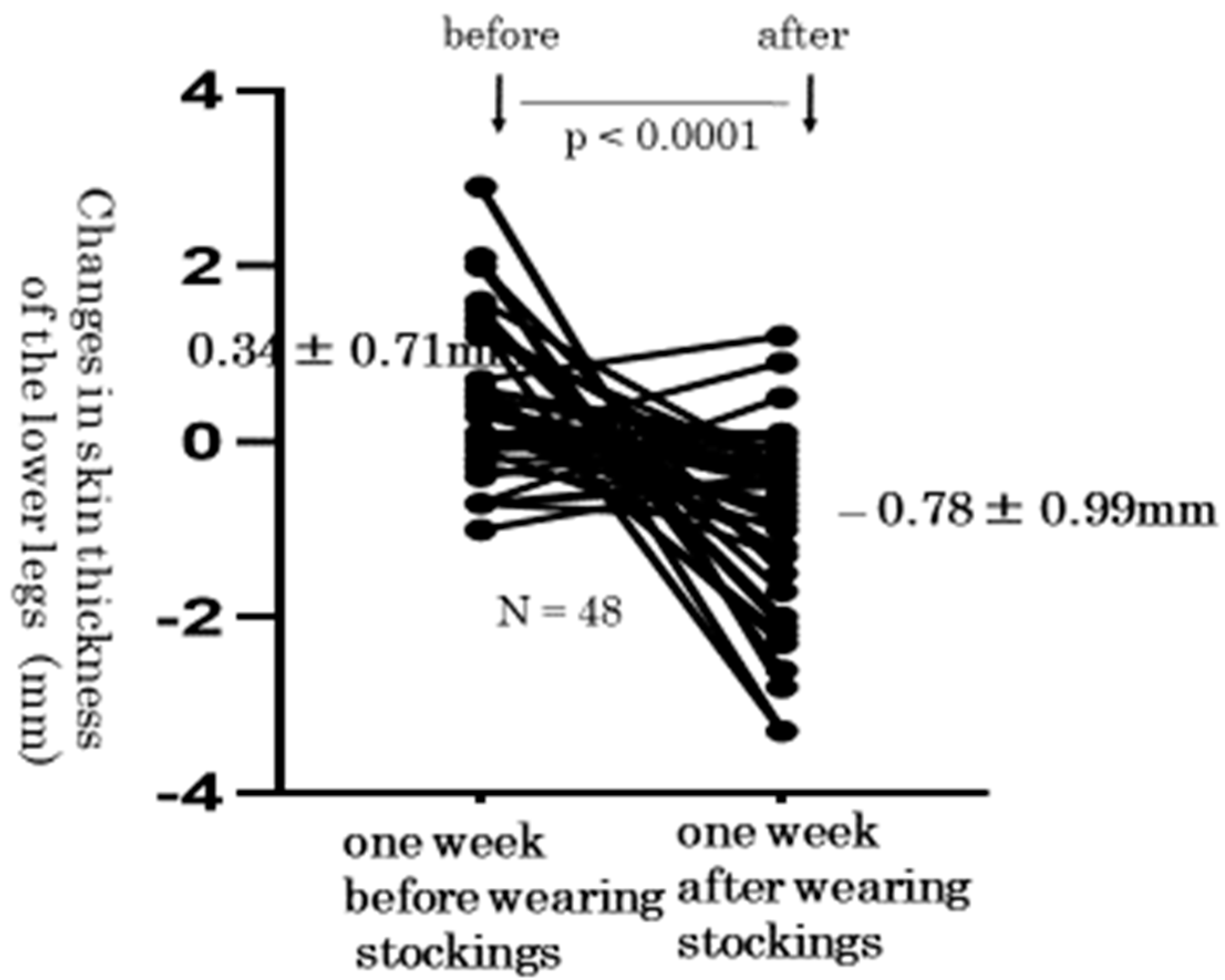
3.2. Level Changes of the Lower Leg Skin Thickness from before to after the Wearing of Elastic Compression Stockings
3.3. Women’s Impressions after Wearing Elastic Compression Stocking
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cho, S.; Atwood, J.E. Peripheral edema. Am. J. Med. 2002, 113, 580–586. [Google Scholar] [CrossRef]
- Trayes, K.P.; Studdiford, J.S. Edema: Diagnosis and management. Am. Fam. Phys. 2013, 88, 102–110. [Google Scholar] [PubMed]
- Tranveer, T.; Shahid, S. Frequency of lower extremity edema during third trimester of pregnancy. S. Asian. J. Med. Sci. 2015, 1, 41–43. [Google Scholar]
- Fitzpatrick, T.B.; Eisen, A.Z.; Wolff, K. Dermatology in General Medicine; McGraw-Hill: New York, NY, USA, 1987; p. 2082. [Google Scholar]
- De Swiet, M. Medical Disorders in Obstetric Practice, 3rd ed.; Blackwell Science: Oxford, UK, 1995; p. 612. [Google Scholar]
- Mayo Clinic Staff. Edema. Symptoms & Causes. Patient Care & Health Information. Mayo Clinic Home Page. Available online: https://www.mayoclinic.org/diseases-conditions/edema/symptoms-causes/syc-20366493 (accessed on 11 November 2021).
- Bamigboye, A.A.; Hofmeyr, G.J. Interventions for leg edema and varicosities in pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 129, 3–8. [Google Scholar] [CrossRef]
- Watanabe, Y.; Koshiyama, M.; Yanagisawa, N. Treatment of leg and foot edema in women. Women’s Health Open J. 2017, 3, 69–74. [Google Scholar] [CrossRef]
- Ochalek, K.; Pacyga, K.; Curylo, M.; Frydrych-Szymonik, A.; Szygula, Z. Risk factors related to lower limb edema, compression, and physical activity during pregnancy: A retrospective study. Lymphat. Res. Biol. 2017, 15, 166–171. [Google Scholar] [CrossRef]
- Smyth, R.M.; Aflaifel, N.; Bamigboye, A.A. Interventions for varicose veins and leg oedema in pregnancy. Cochrane Database Syst. Rev. 2015, 19, CD001066. [Google Scholar] [CrossRef]
- Junior, O.A.S.; Rollo, H.A.; Saliba, O.; Sobreira, M.L. Graduated compression stockings effects on chronic venous disease signs and symptoms during pregnancy. Phlebology 2020, 35, 46–55. [Google Scholar] [CrossRef]
- Berard, A.; Kurz, X.; Zuccarelli, F.; Ducros, J.J.; Abenhaim, L. Relaibility study of the Leg-O-Meter, an improved tape measure device, in patients with chronic venous insufficiency of the leg. Angiology 1998, 49, 169–173. [Google Scholar] [CrossRef]
- Saliba-Junior, O.A.; Rollo, H.A.; Salida, O.; Sobreira, M.L. Positive perception and efficacy of compression stockings for prevention of lower limb edema in pregnant women. J. Vasc. Bras. 2022, 21, e1–e7. [Google Scholar]
- Yanagisawa, M.; Koshiyama, M.; Watanabe, Y.; Sato, S.; Sakamoto, S. A quantitative method to measure skin thickness in leg edema in pregnant women using B-scan portable ultrasonography: A comparison between obese and non-obese women. Med. Sci. Monit. 2019, 25, 1–9. [Google Scholar] [CrossRef]
- Suehiro, K.; Morikage, N.; Murakami, M.; Yamashita, O.; Ueda, K.; Samura, M.; Nakamura, K.; Hamano, K. Subcutaneous tissue ultrasonography in legs with dependent edema and secondary lymphedema. Ann. Vasc. Dis. 2014, 7, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Ikuta, E.; Watanabe, Y.; Yanagisawa, N.; Nakagawa, M.; Ono, A.; Seki, K.; Oowaki, M.; Koshiyama, M.; Sakamoto, S. Measurement of women’s leg edema using ultrasonography. Women’s Health Open J. 2020, 6, 5–7. [Google Scholar] [CrossRef]
- Seo, D.K.; Kang, H.W.; Ahn, D.S.; Song, J.S. Effect of leg elevation height on reduced swelling of patients of postoperative acute ankle fractures. J. Korean Foot Ankle Coc. 2020, 24, 31–36. [Google Scholar] [CrossRef]
- Ҫoban, A.; Şiri, A. Effect of foot massage to decrease physiological lower leg oedema in late pregnancy: A randomized controlled trial in Turkey. Int. J. Nurs. Pract. 2010, 16, 454–460. [Google Scholar]
- Morris, R.J. Intermittent pneumatic compression-systems and applications. J. Med. Eng. Technol. 2008, 32, 179–188. [Google Scholar] [CrossRef]
- Olszewski, W.L.; Cwikla, J.; Zaleska, M.; Domaszewska-Szostek, A.; Gradalski, T.; Szopinska, S. Pathways of lymph and tissue fluid flow during intermittent pneumatic massage of lower limbs with obstructive lymphedema. Lymphology 2011, 44, 54–64. [Google Scholar]
- Tiran, D. The use of complementary therapies in midwifery practice: A focus on reflexsology. Complement. Ther. Nurs. Midwifery 1996, 2, 32–37. [Google Scholar] [CrossRef]
- Mollart, L. Single-blind trial addressing the differential effects of two reflexology techniques versus rest, on ankle and foot oedema in late pregnancy. Complement. Ther. Nurs. Midwifery 2003, 9, 203–208. [Google Scholar] [CrossRef]
- Kent, T.; Gregor, J.; Deardorff, L.; Katz, V. Edema of pregnancy: A comparison of water aerobics and static immersion. Obstet. Gynecol. 1999, 94, 726–729. [Google Scholar] [CrossRef]
- Hartmann, S.; Huch, R. Response of pregnancy leg edema to a single immersion exercise session. Acta Obstet. Gynecol. Scand. 2005, 84, 1150–1153. [Google Scholar] [CrossRef]
- Bergstein, N.A. Clinical study on the efficacy of o-(beta-hydroxyethyl) rutoside (HR) in varicosis of pregnancy. J. Int. Med. Res. 1975, 3, 189–193. [Google Scholar] [CrossRef]
- Damstra, R.J.; Brouwer, E.R.; Partsch, H. Controlled, comparative study of relation between volume changes and interface pressure under short-stretch bandages in leg lymphedema patients. Dermatal. Surg. 2008, 34, 773–778. [Google Scholar]
- Mosti, G.; Partsch, H. Bandages or double stockings for the initial therapy of venous oedema? A randomized, controlled pilot study. Eur. J. Endovasc. Surg. 2013, 46, 142–148. [Google Scholar] [CrossRef]
- de Godoy, J.M.; Braile, D.M.; Perez, F.B.; de Fátima Guerreiro Godoy, M. Effect of walking on pressure variation that occur at the interface between elastic stocking and the skin. Int. Wound J. 2010, 7, 191–193. [Google Scholar] [CrossRef]
- Carvalho, C.A.; Pinto, R.L.; Godoy, M.F.; de Godoy, J.M. Reduction of pain and edema of the legs by walking wearing elastic stockings. Int. J. Vasc. Med. 2015, 2015, 648074. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| At 36 Weeks | At 37 Weeks | At 38 Weeks | |
|---|---|---|---|
| pitting edema method | on the thigh and lower leg | on the thigh and lower leg | on the thigh and lower leg |
| measurments of the skin thickness | in lower leg | in lower leg | in lower leg |
| wearing elastic compression stockings | put on | pull off |
| Grade of Skin Edema | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| status of pitting edema | negative for edema | pitting edema that disappeared within 10 s | pitting edema that disappeared after 10–15 s | pitting edema that lasted for more than 15 s |
| Thigh | Lower Leg | |||||||
|---|---|---|---|---|---|---|---|---|
| grade of edema | 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 |
| no. of legs at 36 weeks gestation | 48 | 0 | 0 | 0 | 0 | 24 | 11 | 13 |
| no. of legs at 37 weeks gestation | 48 | 0 | 0 | 0 | 0 | 20 | 18 | 10 * |
| no. of legs at 38 weeks gestation | 48 | 0 | 0 | 0 | 10 | 28 | 8 | 2 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banba, A.; Koshiyama, M.; Watanabe, Y.; Makino, K.; Ikuta, E.; Yanagisawa, N.; Ono, A.; Nakagawa, M.; Seki, K.; Sakamoto, S.-i.; et al. Measurement of Skin Thickness Using Ultrasonography to Test the Usefulness of Elastic Compression Stockings for Leg Edema in Pregnant Women. Healthcare 2022, 10, 1754. https://doi.org/10.3390/healthcare10091754
Banba A, Koshiyama M, Watanabe Y, Makino K, Ikuta E, Yanagisawa N, Ono A, Nakagawa M, Seki K, Sakamoto S-i, et al. Measurement of Skin Thickness Using Ultrasonography to Test the Usefulness of Elastic Compression Stockings for Leg Edema in Pregnant Women. Healthcare. 2022; 10(9):1754. https://doi.org/10.3390/healthcare10091754
Chicago/Turabian StyleBanba, Airi, Masafumi Koshiyama, Yumiko Watanabe, Koji Makino, Eri Ikuta, Nami Yanagisawa, Ayumi Ono, Miwa Nakagawa, Keiko Seki, Shin-ichi Sakamoto, and et al. 2022. "Measurement of Skin Thickness Using Ultrasonography to Test the Usefulness of Elastic Compression Stockings for Leg Edema in Pregnant Women" Healthcare 10, no. 9: 1754. https://doi.org/10.3390/healthcare10091754