
Acute Supplementation with Cannabidiol Does Not Attenuate Inflammation or Improve Measures of Performance following Strenuous Exercise

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Protocol
2.2.1. Visits 1 and 4: Muscle Damaging Sessions
Muscle Damaging Protocol
2.2.2. Visits 2, 3, 5, and 6: Performance Measure Sessions
Performance Measures
2.2.3. Blood Collection
2.2.4. Biochemical Analysis
2.2.5. Supplementation
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
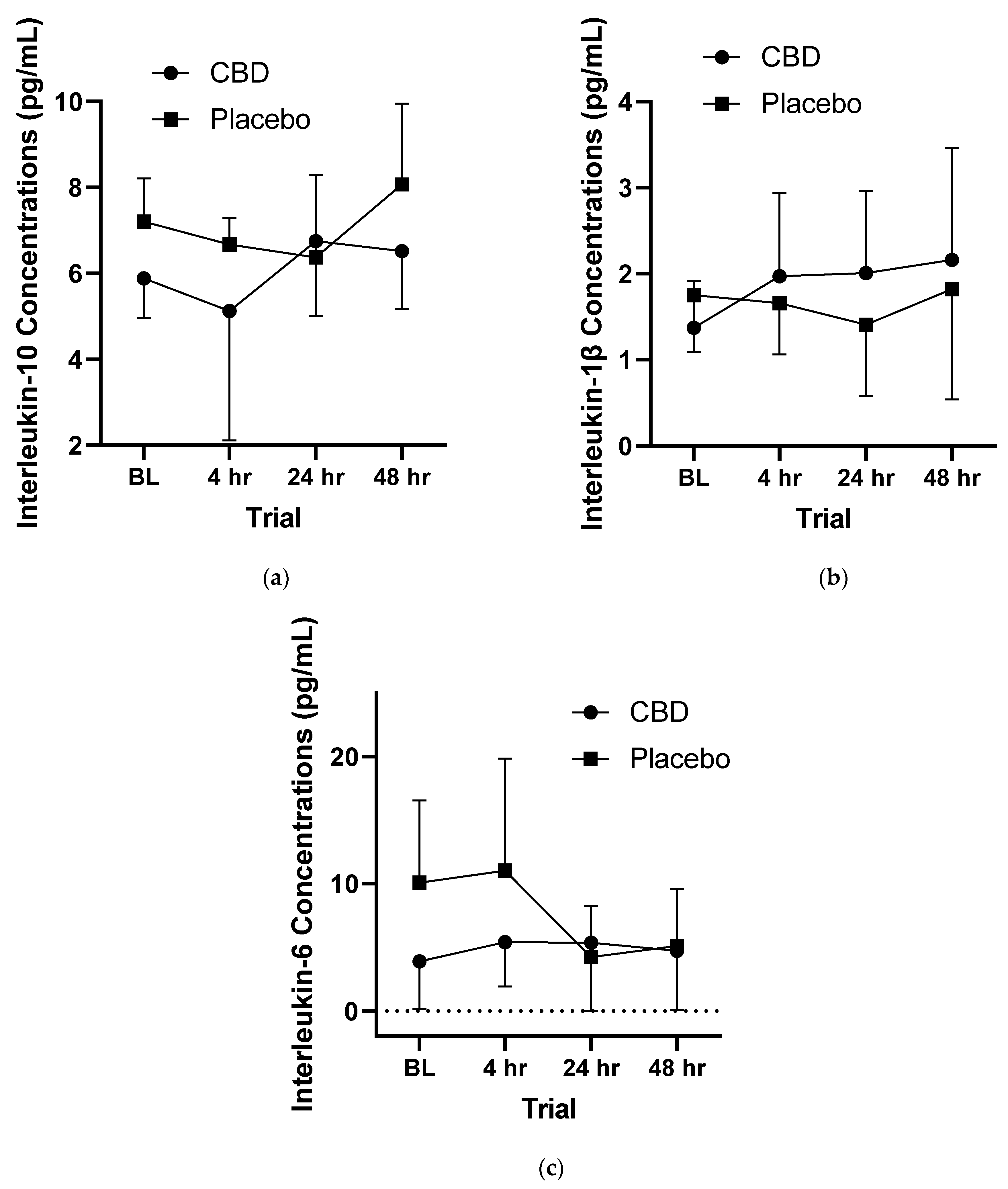
3.2. Inflammatory Responses
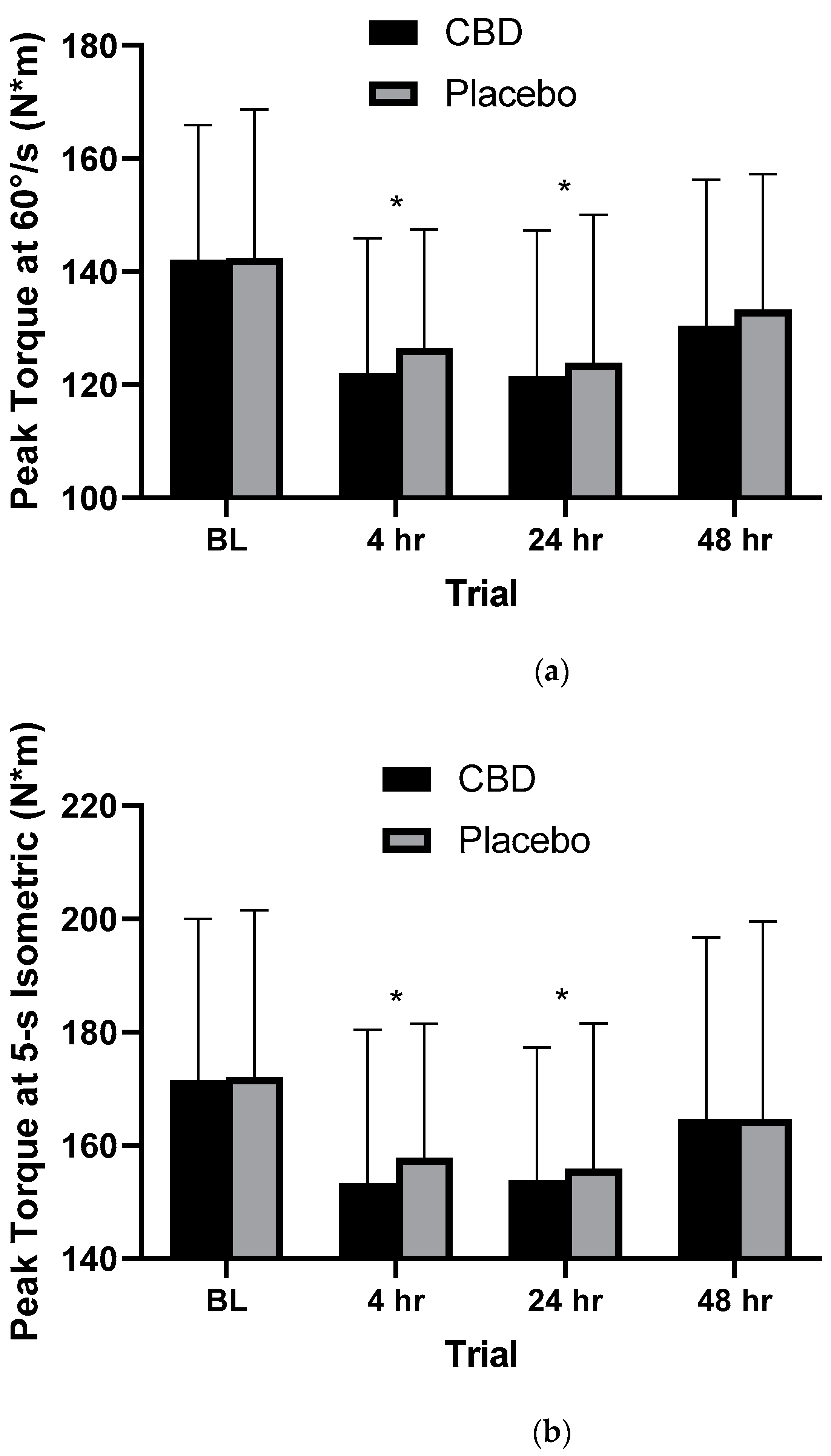
3.3. Performance Measures
3.4. Myoglobin
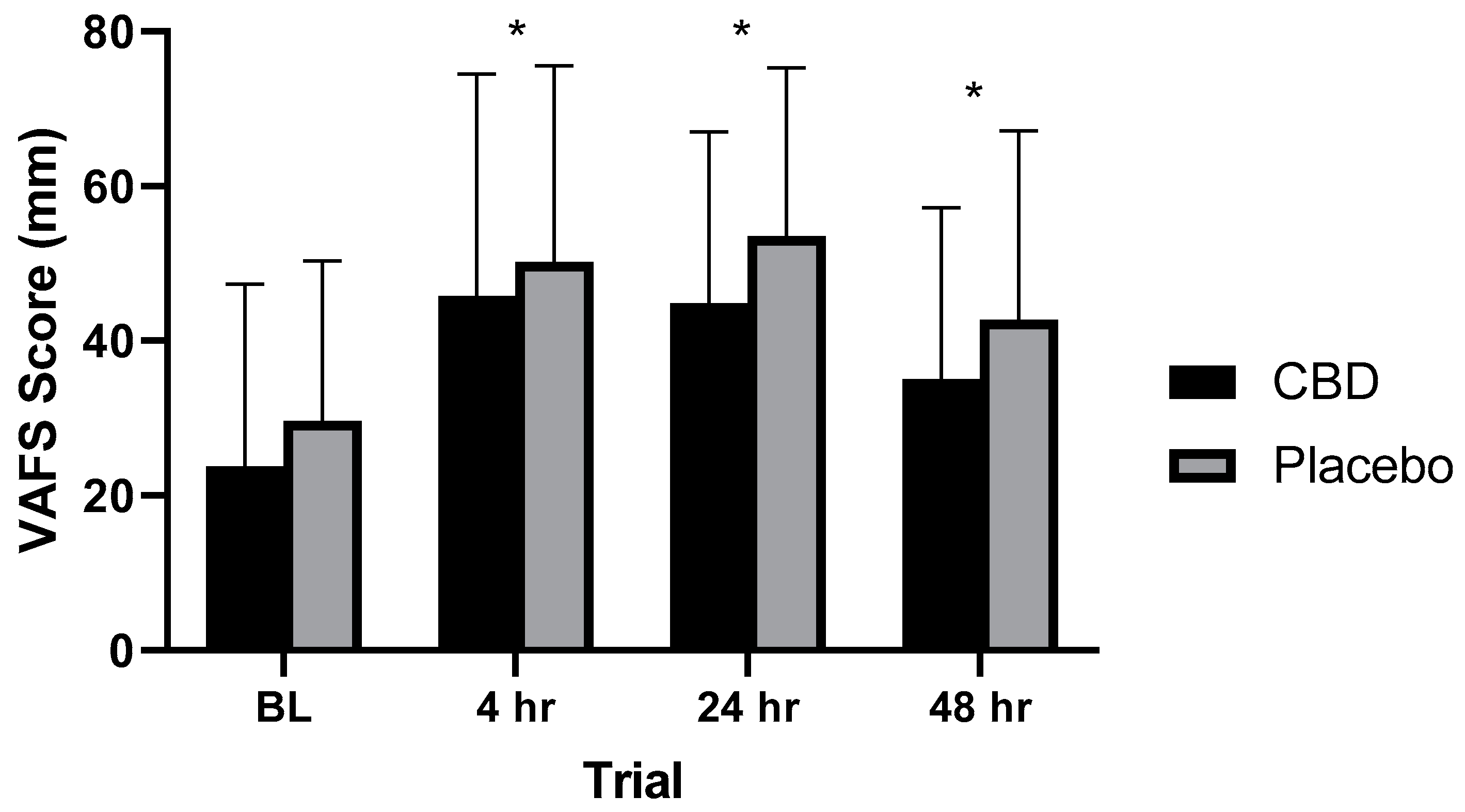
3.5. Visual Analog Fatigue Scale Scores
4. Discussion
4.1. Participants
4.2. Study Protocol
4.2.1. Dose Amount
4.2.2. Timing of Dose
4.3. Cannabidiol Supplementation and Exercise
4.4. Inflammation and Exercise
4.5. Performance
4.6. Muscle Damage and Fatigue
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. Cmaj 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ament, W.; Verkerke, G.J. Exercise and fatigue. Sports Med. 2009, 39, 389–422. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.B.; Warren, G.L.; Warren, J.A. Mechanisms of exercise-induced muscle fiber injury. Sports Med. 1991, 12, 184–207. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Houmard, J.; Fraser, D.; Dudek, R.; Lambert, J.; Tracy, J. Normal forces and myofibrillar disruption after repeated eccentric exercise. J. Appl. Physiol. 1998, 84, 492–498. [Google Scholar] [CrossRef]
- Cleak, M.J.; Eston, R.G. Muscle soreness, swelling, stiffness and strength loss after intense eccentric exercise. Br. J. Sports Med. 1992, 26, 267–272. [Google Scholar] [CrossRef] [Green Version]
- Ebbeling, C.B.; Clarkson, P.M. Muscle adaptation prior to recovery following eccentric exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 26–31. [Google Scholar] [CrossRef]
- Dekkers, J.C.; van Doornen, L.J.; Kemper, H.C. The role of antioxidant vitamins and enzymes in the prevention of exercise-induced muscle damage. Sports Med. 1996, 21, 213–238. [Google Scholar] [CrossRef]
- Hyldahl, R.D.; Hubal, M.J. Lengthening our perspective: Morphological, cellular, and molecular responses to eccentric exercise. Muscle Nerve 2014, 49, 155–170. [Google Scholar] [CrossRef]
- Peake, J.M.; Neubauer, O.; Della Gatta, P.A.; Nosaka, K. Muscle damage and inflammation during recovery from exercise. J. Appl. Physiol. 2017, 3, 559–570. [Google Scholar] [CrossRef]
- Soligard, T.; Schwellnus, M.; Alonso, J.M.; Bahr, R.; Clarsen, B.; Dijkstra, H.P. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br. J. Sports Med. 2016, 50, 1030–1041. [Google Scholar] [CrossRef] [Green Version]
- Byrne, C.; Eston, R. Maximal-intensity isometric and dynamic exercise performance after eccentric muscle actions. J. Sports Sci. 2002, 20, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Sargeant, A.J.; Dolan, P. Human muscle function following prolonged eccentric exercise. Eur. J. Appl. Physiol. 1987, 56, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Hemmings, B.; Smith, M.; Graydon, J.; Dyson, R. Effects of massage on physiological restoration, perceived recovery, and repeated sports performance. Br. J. Sports Med. 2000, 34, 109–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, R.; Pinho, F.; Duarte, J.A.; Cabri, J.M. Effect of single bout versus repeated bouts of stretching on muscle recovery following eccentric exercise. J. Sci. Med. Sport. 2013, 16, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Leeder, J.; Gissane, C.; van Someren, K.; Gregson, W.; Howatson, G. Cold water immersion and recovery from strenuous exercise: A meta-analysis. Br. J. Sports Med. 2012, 46, 233–240. [Google Scholar] [CrossRef]
- Kreider, R.B.; Wilborn, C.D.; Taylor, L.; Campbell, B.; Almada, A.L.; Collins, R.; Cooke, M.; Earnest, C.P.; Greenwood, M.; Kalman, D.S.; et al. ISSN exercise & sport nutrition review: Research & recommendations. J. Int. Soc. Sports Nutr. 2010, 7, 7. [Google Scholar]
- Calleja-González, J.; Terrados, N.; Mielgo-Ayuso, J.; Delextrat, A.; Jukic, I.; Vaquera, A.; Torres, L.; Schelling, X.; Stojanovic, M.; Ostojic, S.M. Evidence-based post-exercise recovery strategies in basketball. Phys. Sportsmed. 2016, 44, 74–78. [Google Scholar] [CrossRef]
- Verified Market Research. Sports Nutrition Market Size and Forecast. Available online: https://www.verifiedmarketresearch.com/product/sports-nutrition-market/ (accessed on 26 May 2022).
- Jonvik, K.; King, M.; Rollo, I.; Stellingwerff, T.; Pitsiladis, Y. New opportunities to advance the field of sports nutrition. Front. Sports Act. Living 2022, 4, 852230. [Google Scholar] [CrossRef]
- Hormoznejad, R.; Javid, A.Z.; Mansoori, A. Effect of BCAA supplementation on central fatigue, energy metabolism substrate and muscle damage to the exercise: A systematic review with meta-analysis. Sport Sci. Health 2019, 15, 265–279. [Google Scholar] [CrossRef]
- Cockburn, E.; Stevenson, E.; Hayes, P.R.; Robson-Ansley, P.; Howatson, G. Effect of milk-based carbohydrate-protein supplement timing on the attenuation of exercise-induced muscle damage. Appl. Physiol. Nutr. Metab. 2010, 35, 270–277. [Google Scholar] [CrossRef]
- Cooke, M.B.; Rybalka, E.; Stathis, C.G.; Cribb, P.J.; Hayes, A. Whey protein isolate attenuates strength decline after eccentrically-induced muscle damage in healthy individuals. J. Int. Soc. Sports Nutr. 2010, 7, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, A.M. CBD and Exercise: Risks and Benefits. Available online: https://health.usnews.com/wellness/fitness/articles/cbd-and-exercise-risks-and-benefits (accessed on 16 December 2019).
- Mead, A. Legal and regulatory issues governing cannabis and cannabis-derived products in the United States. Front. Plant Sci. 2019, 10, 697. [Google Scholar] [CrossRef] [PubMed]
- Holler, J.M.; Bosy, T.Z.; Dunkley, C.S.; Levine, B.; Past, M.R.; Jacobs, A. Δ9-Tetrahydrocannabinol content of commercially available hemp products. J. Anal. Toxicol. 2008, 32, 428–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, T.; Kawa, K.; Eckl, V.; Morton, C.; Stredney, R. Herbal supplement sales in US increased 8.5% in 2017, topping $8 billion. HerbalGram 2018, 119, 62–71. [Google Scholar]
- Benson, D. Should CBD Be Part of My Patients’ Treatment? Altern. Ther. Health Med. 2019, 25, 8–11. [Google Scholar] [PubMed]
- Corroon, J.; Kight, R. Regulatory Status of Cannabidiol in the United States: A Perspective. Cannabis Cannabinoid Res. 2018, 3, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Sawler, J.; Stout, J.M.; Gardner, K.M.; Hudson, D.; Vidmar, J.; Butler, L.; Page, J.; Myles, S. The genetic structure of marijuana and hemp. PLoS ONE 2015, 10, e0133292. [Google Scholar] [CrossRef] [Green Version]
- Maroon, J.; Bost, P.A.C.; Mathyssek, C.; Steelers, N.P. Nutritional & Medical Applications for Cannabidiol: Hemp Health Benefits without THC. In Anti-Aging Therapeutics; Klatz, R., Goldman, R., Eds.; American Academy of Anti-Aging: Chicago, IL, USA, 2015; Volume 17, p. 17. [Google Scholar]
- Millar, S.A.; Stone, N.L.; Yates, A.S.; O’Sullivan, S.E. A systematic review on the pharmacokinetics of cannabidiol in humans. Front. Pharmacol. 2018, 9, 1365. [Google Scholar] [CrossRef]
- Devinsky, O.; Marsh, E.; Friedman, D.; Thiele, E.; Laux, L.; Sullivan, J. Cannabidiol in patients with treatment-resistant epilepsy: An open-label interventional trial. Lancet Neurol. 2016, 15, 270–278. [Google Scholar] [CrossRef]
- Devinsky, O.; Patel, A.D.; Thiele, E.A.; Wong, M.H.; Appleton, R.; Harden, C.L.; Greenwood, S.; Morrison, G.; Sommervile, K. Randomized, dose-ranging safety trial of cannabidiol in Dravet syndrome. Neurology 2018, 90, e1204–e1211. [Google Scholar] [CrossRef] [Green Version]
- Devinsky, O.; Patel, A.D.; Cross, J.H.; Villanueva, V.; Wirrell, E.C.; Privier, M.; Greenwood, S.M.; Roberts, C.; Checketts, D.; VanLandingham, K.E.; et al. Effect of cannabidiol on drop seizures in the Lennox-Gastaut syndrome. N. Engl. J. Med. 2018, 378, 1888–1897. [Google Scholar] [CrossRef] [Green Version]
- Cheng, D.; Spiro, A.S.; Jenner, A.M.; Garner, B.; Karl, T. Long-term cannabidiol treatment prevents the development of social recognition memory deficits in Alzheimer’s disease transgenic mice. J. Alzheimers Dis. 2014, 42, 1383–1396. [Google Scholar] [CrossRef]
- Fernández-Ruiz, J.; Sagredo, O.; Pazos, M.R.; García, C.; Pertwee, R.; Mechoulam, R.; Martínez-Orgado, J. Cannabidiol for neurodegenerative disorders: Important new clinical applications for this phytocannabinoid? Br. J. Clin. Pharmacol. 2013, 75, 323–333. [Google Scholar] [CrossRef]
- Durst, R.; Danenberg, H.; Gallily, R.; Mechoulam, R.; Meir, K.; Grad, E.; Beeri, R.; Pugatsch, T.; Tarish, E.; Lotan, C. Cannabidiol, a nonpsychoactive Cannabis constituent, protects against myocardial ischemic reperfusion injury. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H3602–H3607. [Google Scholar] [CrossRef] [Green Version]
- Rajesh, M.; Mukhopadhyay, P.; Bátkai, S.; Patel, V.; Saito, K.; Matsumoto, S. Cannabidiol attenuates cardiac dysfunction, oxidative stress, fibrosis, and inflammatory and cell death signaling pathways in diabetic cardiomyopathy. J. Am. Coll. Cardiol. 2010, 56, 2115–2125. [Google Scholar] [CrossRef] [Green Version]
- Vitti, S.; Bruneau, M.; Leyshon, K.; Sotir, S.; Headley, S.; O’Neill, E. The effects of betalain-rich concentrate supplementation in attenuating muscle damage following eccentric exercise. J. Hum. Sport. Exerc. 2021, 16, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Nicol, L.; Rowlands, D.; Fazakerly, R.; Kellett, J. Curcumin supplementation likely attenuates delayed onset muscle soreness (DOMS). Eur. J. Appl. Physiol. 2015, 115, 1769–1777. [Google Scholar] [CrossRef]
- Willoughby, D.S.; McFarlin, B.; Bois, C. Interleukin-6 expression after repeated bouts of eccentric exercise. Int. J. Sports Med. 2003, 24, 15–21. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Malfait, A.M.; Gallily, R.; Sumariwalla, P.F.; Malik, A.S.; Andreakos, E.; Mechoulam, R.; Feldmann, M. The nonpsychoactive cannabis constituent cannabidiol is an oral anti-arthritic therapeutic in murine collagen-induced arthritis. Proc. Natl. Acad. Sci. USA 2000, 97, 9561–9566. [Google Scholar] [CrossRef] [Green Version]
- Borrelli, F.; Aviello, G.; Romano, B.; Orlando, P.; Capasso, R.; Maiello, F.; Guadagno, F.; Petrosino, S.; Capasso, F.; Di Marzo, V.; et al. Cannabidiol, a safe and non-psychotropic ingredient of the marijuana plant Cannabis sativa, is protective in a murine model of colitis. J. Mol. Med. 2009, 87, 1111–1121. [Google Scholar] [CrossRef]
- Mecha, M.; Feliú, A.; Iñigo, P.M.; Mestre, L.; Carrillo-Salinas, F.J.; Guaza, C. Cannabidiol provides long-lasting protection against the deleterious effects of inflammation in a viral model of multiple sclerosis: A role for A2A receptors. Neurobiol. Dis. 2013, 59, 141–150. [Google Scholar] [CrossRef]
- Gallily, R.; Yekhtin, Z.; Hanuš, L.O. The anti-inflammatory properties of terpenoids from cannabis. Cannabis Cannabinoid Res. 2018, 3, 282–290. [Google Scholar] [CrossRef] [Green Version]
- Cochrane-Snyman, K.C.; Cruz, C.; Morales, J.; Coles, M. The effects of cannabidiol oil on noninvasive measures of muscle damage in men. Med. Sci. Sports Exerc. 2021, 53, 1460–1472. [Google Scholar] [CrossRef]
- Isenmann, E.; Veit, S.; Starke, L.; Flenker, U.; Diel, P. Effects of cannabidiol supplementation on skeletal muscle regeneration after intensive resistance training. Nutrients 2021, 13, 3028. [Google Scholar] [CrossRef]
- Hatchett, A.; Armstrong, K.; Hughes, B.; Parr, B. The influence cannabidiol on delayed onset of muscle soreness. Int. J. Phys. Educ. Sports Health 2020, 7, 89–94. [Google Scholar]
- Kim, J.; So, W.-Y. Effects of acute grape seed extract supplementation on muscle damage after eccentric exercise: A randomized, controlled clinical trial. J. Exerc. Sci. Fit. 2019, 17, 77–79. [Google Scholar] [CrossRef]
- Mason, J.; Rahlf, A.L.; Groll, A.; Wellmann, K.; Junge, A.; Zech, A. The interval between matches significantly influences injury risk in field hockey. Int. J. Sports Med. 2021, 43, 262–268. [Google Scholar] [CrossRef]
- Ascensão, A.; Rebelo, A.; Oliveira, E.; Marques, F.; Pereira, L.; Magalhães, J. Biochemical impact of a soccer match—Analysis of oxidative stress and muscle damage markers throughout recovery. Clin. Biochem. 2008, 41, 841–851. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, L.; Joo, D.; Sun, S.C. NF-κB signaling in inflammation. Signal Transduct. Target Ther. 2017, 2, 17023. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Cabrera, M.C.; Martínez, A.; Santangelo, G.; Pallardó, F.V.; Sastre, J.; Vina, J. Oxidative stress in marathon runners: Interest of antioxidant supplementation. Br. J. Nutr. 2006, 96, S31–S33. [Google Scholar] [CrossRef] [PubMed]
- Kozela, E.; Pietr, M.; Juknat, A.; Rimmerman, N.; Levy, R.; Vogel, Z. Cannabinoids Δ9-tetrahydrocannabinol and cannabidiol differentially inhibit the lipopolysaccharide-activated NF-κB and interferon-β/STAT proinflammatory pathways in BV-2 microglial cells. J. Biol. Chem. 2010, 285, 1616–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mammana, S.; Cavalli, E.; Gugliandolo, A.; Silvestro, S.; Pollastro, F.; Bramanti, P.; Mazzon, E. Could the combination of two non-psychotropic cannabinoids counteract neuroinflammation? Effectiveness of cannabidiol associated with cannabigerol. Medicina 2019, 55, 747. [Google Scholar] [CrossRef] [Green Version]
- Peake, J.; Nosaka, K.; Suzuki, K. Characterization of inflammatory responses to eccentric exercise in humans. Exerc. Immunol. Rev. 2005, 11, 64–85. [Google Scholar] [PubMed]
- Lopez-Castejon, G.; Brough, D. Understanding the mechanism of IL-1β secretion. Cytokine Growth Factor Rev. 2011, 22, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Passos, B.N.; Lima, M.C.; Sierra, A.P.; Oliveira, R.A.; Maciel, J.F.; Manoel, R.; Rogante, J.; Pesquero, J.; Cury-Boaventura, M.F. Association of daily dietary intake and inflammation induced by marathon race. Mediat. Inflamm. 2019, 2019, 1537274. [Google Scholar] [CrossRef] [Green Version]
- Pournot, H.; Bieuzen, F.; Louis, J.; Fillard, J.R.; Barbiche, E.; Hausswirth, C. Time-course of changes in inflammatory response after whole-body cryotherapy multi exposures following severe exercise. PLoS ONE 2011, 6, e22748. [Google Scholar] [CrossRef]
- Vassilakopoulos, T.; Karatza, M.H.; Katsaounou, P.; Kollintza, A.; Zakynthinos, S.; Roussos, C. Antioxidants attenuate the plasma cytokine response to exercise in humans. J. Appl. Physiol. 2003, 94, 1025–1032. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K. Exercise and cytokines. Immunol. Cell Biol. 2000, 78, 532–535. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Fischer, C.P. Beneficial health effects of exercise—The role of IL-6 as a myokine. Trends Pharmacol. Sci. 2007, 28, 152–156. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Steensberg, A.; Schjerling, P. Muscle-derived interleukin-6: Possible biological effects. J. Physiol. 2001, 536, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.L.; Anwar, A.; Fragen, M.; Rananto, C.; Johnson, R.; Holbert, D. Cytokines and cell adhesion molecules associated with high-intensity eccentric exercise. Eur. J. Appl. Physiol. 2000, 82, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Wilborn, C.; Hayward, S.; Taylor, L.; Urbina, S.; Foster, C.; Deshpande, P.; Mohan, V.; Thakurdesai, P. Effects of a proprietary blend rich in glycoside based standardized fenugreek seed extract (IBPR) on inflammatory markers during acute eccentric resistance exercise in young subjects. Asian J. Pharm. Clin. Res. 2017, 10, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Cornish, S.M.; Johnson, S.T. Systemic cytokine response to three bouts of eccentric exercise. Results Immunol. 2014, 4, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Cabral-Santos, C.; de Lima Junior, E.A.; Fernandes, I.; Pinto, R.Z.; Rosa-Neto, J.C.; Bishop, N.C.; Lira, F.S. Interleukin-10 responses from acute exercise in healthy subjects: A systematic review. J. Cell Physiol. 2019, 234, 9956–9965. [Google Scholar] [CrossRef] [Green Version]
- Deng, B.; Wehling-Henricks, M.; Villalta, S.A.; Wang, Y.; Tidball, J.G. IL-10 triggers changes in macrophage phenotype that promote muscle growth and regeneration. J. Immunol. 2012, 189, 3669–3680. [Google Scholar] [CrossRef] [Green Version]
- Rodas, L.; Martinez, S.; Aguilo, A.; Tauler, P. Caffeine supplementation induces higher IL-6 and IL-10 plasma levels in response to a treadmill exercise test. J. Int. Soc. Sports Nutr. 2020, 17, 47. [Google Scholar] [CrossRef]
- Hirose, L.; Nosaka, K.; Newton, M.; Laveder, A.; Kano, M.; Peake, J.; Suzuki, K. Changes in inflammatory mediators following eccentric exercise of the elbow flexors. Exerc. Immunol. Rev. 2004, 10, 20. [Google Scholar]
- Halson, S.L. Monitoring training load to understand fatigue in athletes. Sports Med. 2014, 44, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Newham, D.J.; McCarthy, T.; Turner, J. Voluntary activation of human quadriceps during and after isokinetic exercise. J. Appl. Physiol. 1991, 71, 2122–2126. [Google Scholar] [CrossRef]
- Carroll, T.J.; Taylor, J.L.; Gandevia, S.C. Recovery of central and peripheral neuromuscular fatigue after exercise. J. Appl. Physiol. 2017, 122, 1068–1076. [Google Scholar] [CrossRef] [Green Version]
- Malm, C. Exercise-induced muscle damage and inflammation: Fact or fiction? Acta Physiol. Scand. 2001, 171, 233–239. [Google Scholar] [CrossRef]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical markers of muscular damage. Clin. Chem. Lab. Med. 2010, 48, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Driessen-Kletter, M.F.; Amelink, G.J.; Bär, P.R.; Van Gijn, J. Myoglobin is a sensitive marker of increased muscle membrane vulnerability. J. Neurol. 1990, 237, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Cheshier, B.C.; Jacobson, B.H. The effectiveness of natural supplements on prevention and treatment of delayed onset muscle soreness and markers of muscle damage: A review of literature. AUC Kinanthropologica 2021, 57, 26–50. [Google Scholar] [CrossRef]
- Sousa, M.; Teixeira, V.H.; Soares, J. Dietary strategies to recover from exercise-induced muscle damage. Int. J. Food Sci. Nutr. 2014, 65, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Tee, J.C.; Bosch, A.N.; Lambert, M.I. Metabolic consequences of exercise-induced muscle damage. Sports Med. 2007, 37, 827–836. [Google Scholar] [CrossRef]
- Kanda, K.; Sugama, K.; Hayashida, H.; Sakuma, J.; Kawakami, Y.; Miura, S.; Yoshioka, H.; Mori, Y.; Suzuki, K. Eccentric exercise-induced delayed-onset muscle soreness and changes in markers of muscle damage and inflammation. Exerc. Immunol. Rev. 2013, 19, 72–85. [Google Scholar]
- Tartibian, B.; Maleki, B.H.; Abbasi, A. Omega-3 fatty acids supplementation attenuates inflammatory markers after eccentric exercise in untrained men. Clin. J. Sports Med. 2011, 21, 131–137. [Google Scholar] [CrossRef]
- Takarada, Y. Evaluation of muscle damage after a rugby match with special reference to tackle plays. Br. J. Sports Med. 2003, 37, 416–419. [Google Scholar] [CrossRef] [Green Version]
- Chase, J.E.; Peeler, J.D.; Barr, M.J.; Gardiner, P.F.; Cornish, S.M. The impact of a single bout of intermittent pneumatic compression on performance, inflammatory markers, and myoglobin in football athletes. J. Trainology 2020, 9, 33–38. [Google Scholar] [CrossRef]
- Chalchat, E.; Charlot, K.; Garcia-Vicencio, S.; Hertert, P.; Baugé, S.; Bourdon, S.; Bompard, J.; Farges, C.; Martin, V.; Bourrilhon, C.; et al. Circulating microRNAs after a 24-h ultramarathon run in relation to muscle damage markers in elite athletes. Scand. J. Med. Sci. Sports 2021, 9, 1782–1795. [Google Scholar] [CrossRef]
- Kostopoulos, N.; Fatouros, I.G.; Siatitsas, I.; Baltopoulos, P.; Kambas, A.; Jamurtas, A.Z.; Fotinakis, P. Intense basketball-simulated exercise induces muscle damage in men with elevated anterior compartment pressure. J. Strength Cond. Res. 2004, 18, 451–458. [Google Scholar] [PubMed]
- Machin, D.R.; Christmas, K.M.; Chou, T.H.; Hill, S.C.; Van Pelt, D.W.; Trombold, J.R.; Coyle, E.F. Effects of differing dosages of pomegranate juice supplementation after eccentric exercise. Physiol. J. 2014, 2014, 271959. [Google Scholar] [CrossRef] [Green Version]
- De Souza Crippa, J.A.; Zuardi, A.W.; Garrido, G.E.; Wichert-Ana, L.; Guarnieri, R.; Ferrari, L.; Azevedo-Marques, P.M.; Hallak, J.E.; McGuire, P.K.; Filho Busatto, G. Effects of cannabidiol (CBD) on regional cerebral blood flow. Neuropsychopharmacology 2004, 29, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Dannecker, E.A.; Liu, Y.; Rector, R.S.; Thomas, T.R.; Fillingim, R.B.; Robinson, M.E. Sex differences in exercise-induced muscle pain and muscle damage. J. Pain 2012, 13, 1242–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.K.; Oikawa, S.Y.; Halson, S.; Tephens, J.; O’Riordan, S.; Luhrs, K.; Sopena, B.; Baker, L.B. In-Season Nutrition Strategies and Recovery Modalities to Enhance Recovery for Basketball Players: A Narrative Review. Sports Med. 2021, 52, 971–993. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | 21.2 ± 1.8 |
| Height (cm) | 166.4 ± 8.0 |
| Weight (kg) | 64.9 ± 9.1 |
| BMI (kg/m2) | 23.7 ± 2.4 |
| Vertical Jump Performance (cm) | 49.3 ± 8.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crossland, B.W.; Rigby, B.R.; Duplanty, A.A.; King, G.A.; Juma, S.; Levine, N.A.; Clark, C.E.; Ramirez, K.P.; Varone, N.L. Acute Supplementation with Cannabidiol Does Not Attenuate Inflammation or Improve Measures of Performance following Strenuous Exercise. Healthcare 2022, 10, 1133. https://doi.org/10.3390/healthcare10061133
Crossland BW, Rigby BR, Duplanty AA, King GA, Juma S, Levine NA, Clark CE, Ramirez KP, Varone NL. Acute Supplementation with Cannabidiol Does Not Attenuate Inflammation or Improve Measures of Performance following Strenuous Exercise. Healthcare. 2022; 10(6):1133. https://doi.org/10.3390/healthcare10061133
Chicago/Turabian StyleCrossland, Brett W., B. Rhett Rigby, Anthony A. Duplanty, George A. King, Shanil Juma, Nicholas A. Levine, Cayla E. Clark, Kyndall P. Ramirez, and Nicole L. Varone. 2022. "Acute Supplementation with Cannabidiol Does Not Attenuate Inflammation or Improve Measures of Performance following Strenuous Exercise" Healthcare 10, no. 6: 1133. https://doi.org/10.3390/healthcare10061133