
Telehome Monitoring of Symptoms and Lung Function in Children with Asthma


Abstract
:1. Introduction
2. Materials and Methods
2.1. Context and Ethics
2.2. Sample
2.3. Objectives
2.4. Conduct of the Study
2.5. Statistical Analysis
3. Results
3.1. Study Flow Diagram
3.2. Demographic Characteristics of the Study Population
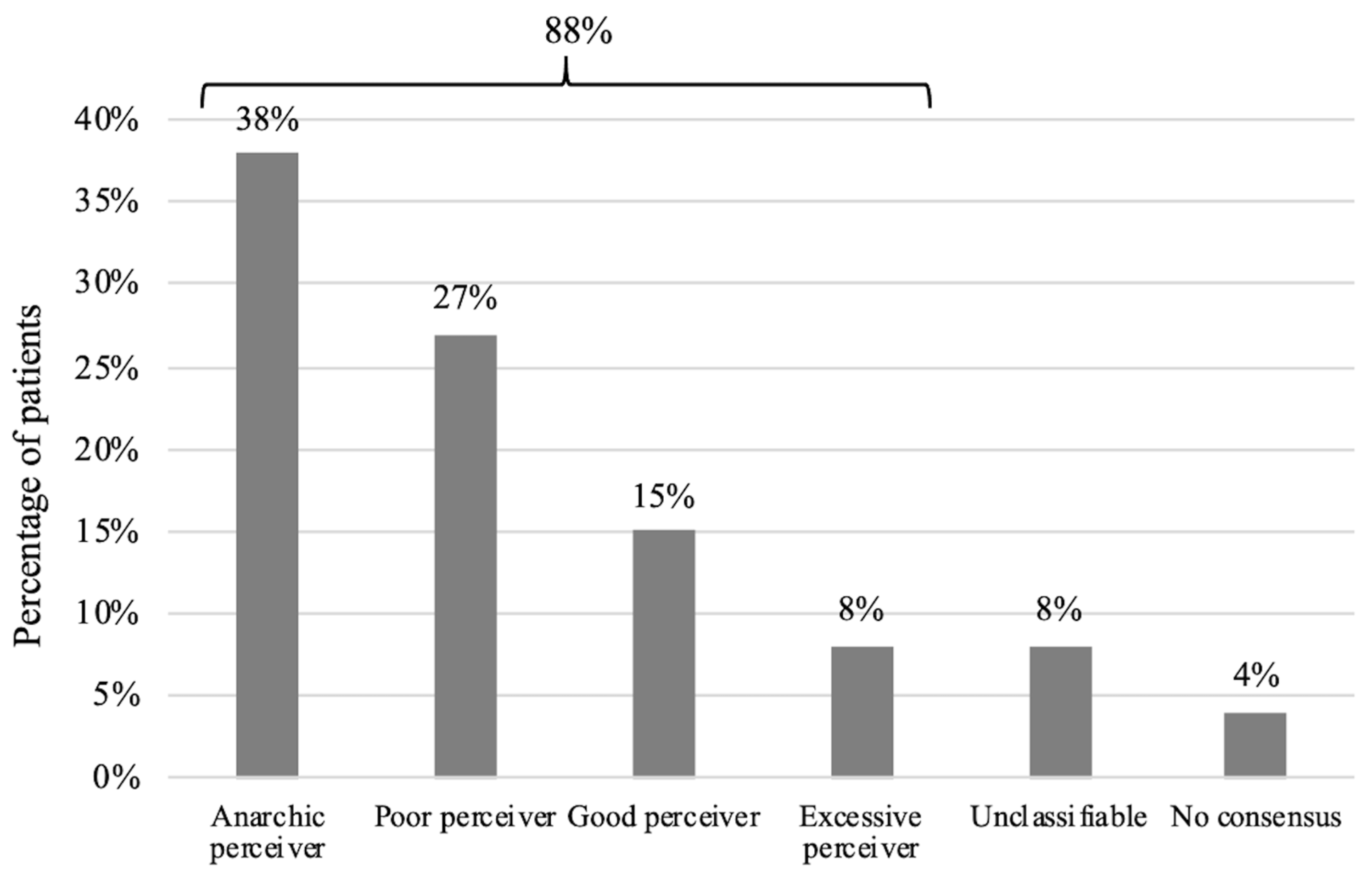
3.3. Main Objective: Brouwer’s Asthma Profile
3.4. Secondary Objectives
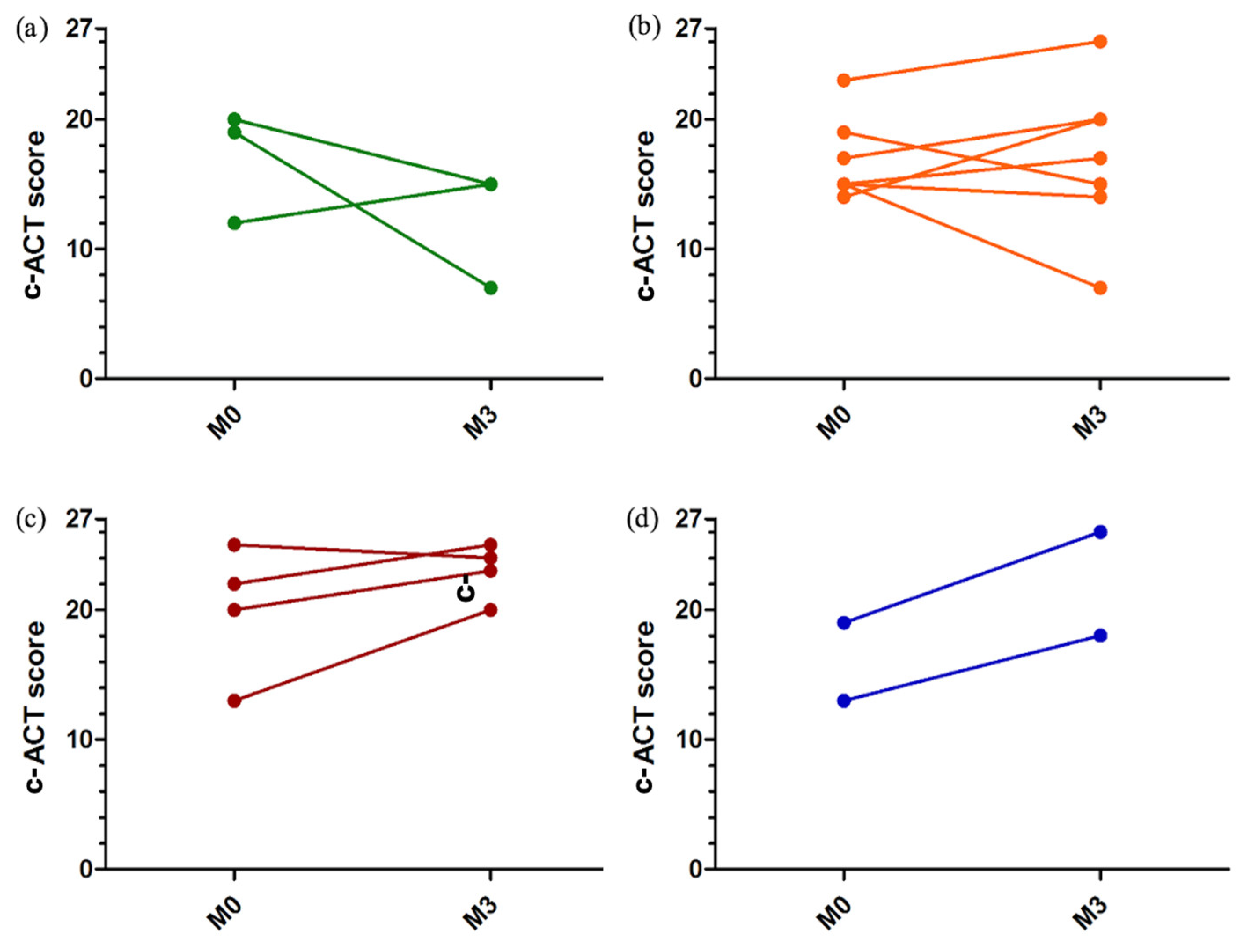
3.4.1. Asthma Control
3.4.2. Therapeutic Optimization
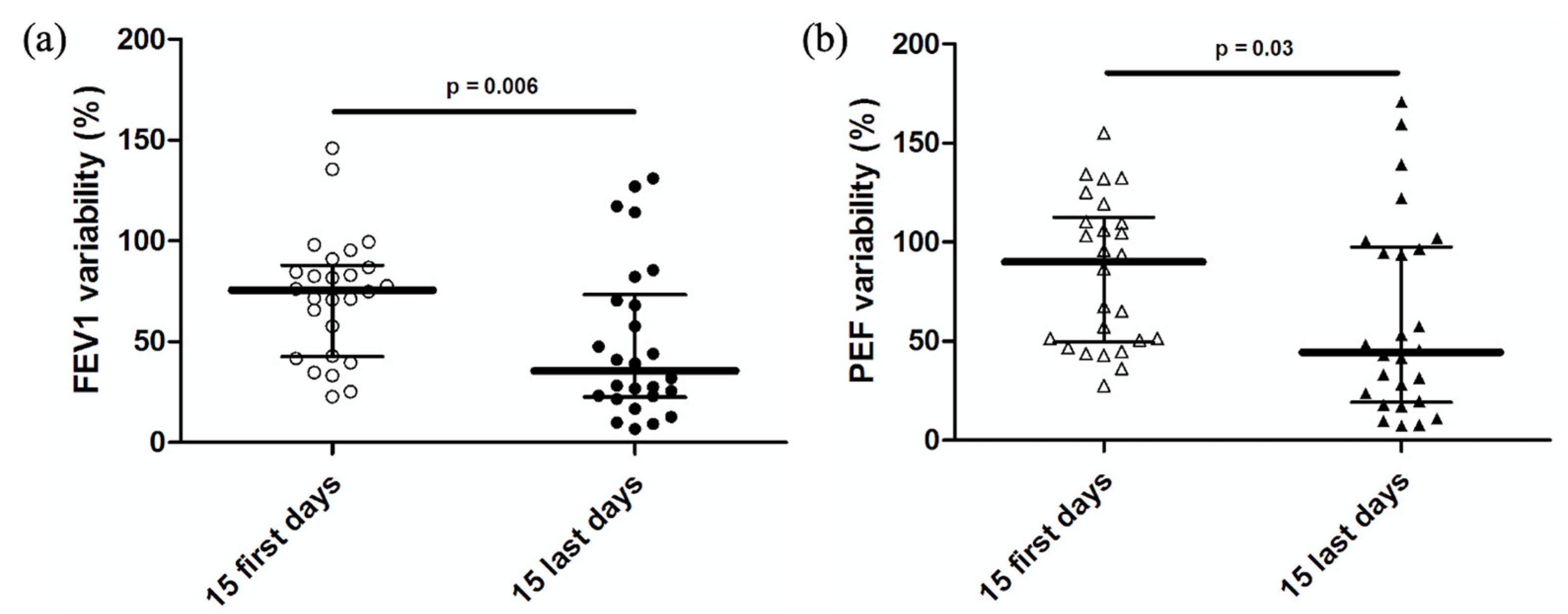
3.4.3. FEV1 and PEF Variability
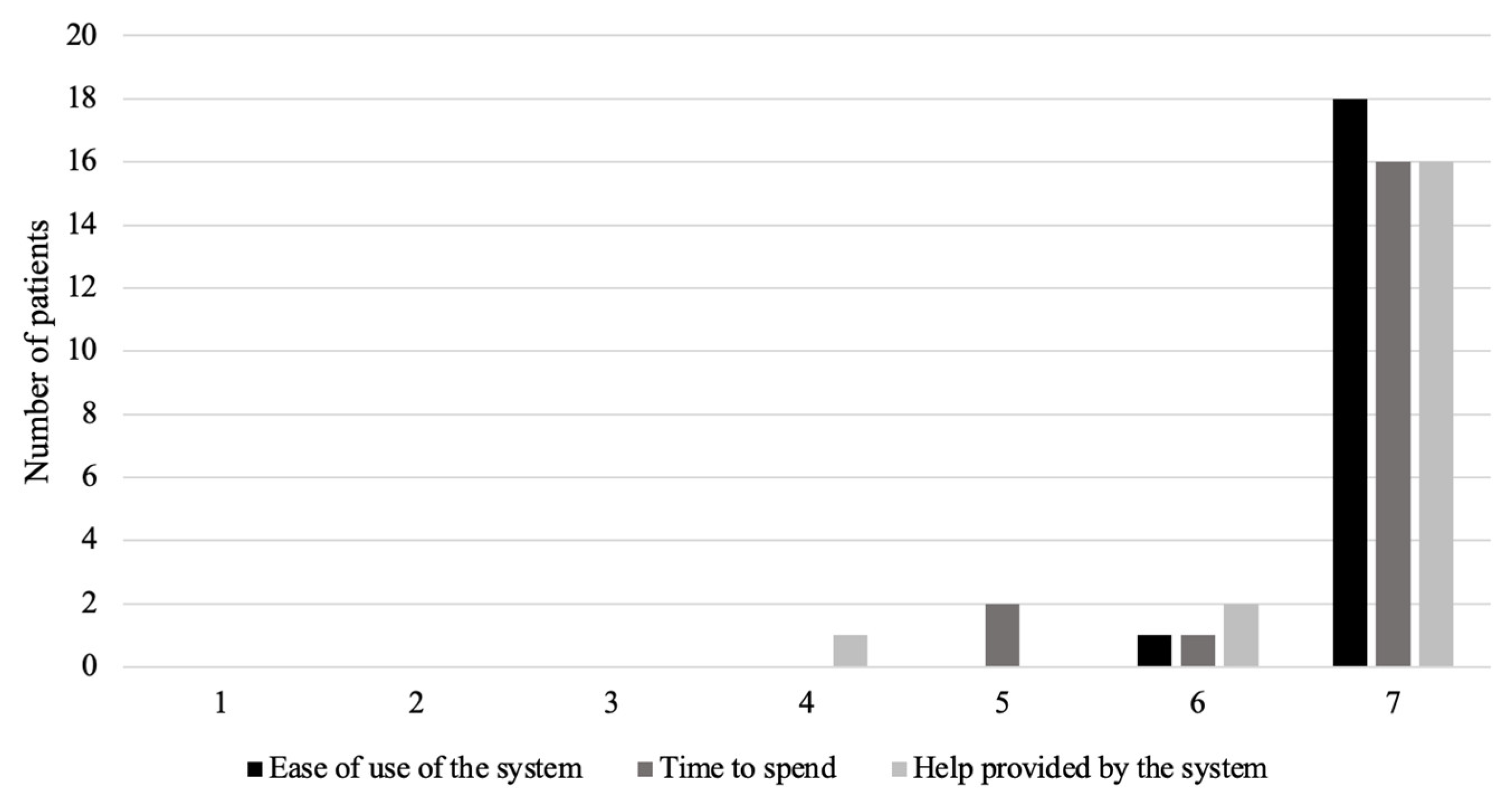
3.4.4. Tool Observance and Acceptability
3.4.5. Qualitative Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davies, B.; Kenia, P.; Nagakumar, P.; Gupta, A. Paediatric and adolescent asthma: A narrative review of telemedicine and emerging technologies for the post-COVID-19 era. Clin. Exp. Allergy 2021, 51, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Loeb, A.E.; Rao, S.S.; Ficke, J.R.; Morris, C.D.; Riley, L.H., III; Levin, A.S. Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J. Am. Acad. Orthop. Surg. 2020, 28, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Perry, T.T.; Margiotta, C.A. Implementing Telehealth in Pediatric Asthma. Pediatr. Clin. 2020, 67, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Haynes, S.C.; Kamerman-Kretzmer, R.; Khan, S.S.; Crossen, S.; Lieng, M.K.; Marcin, J.P.; Kenyon, N.J.; Kim, C.H. Telemedicine use for pediatric asthma care: A mixed methods study. J. Asthma 2022. online ahead of print. [Google Scholar] [CrossRef]
- World Health Organization. Draft Global Strategy on Digital Health 2020–2024; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Haute Autorité de Santé. Efficience de la Télémédecine: État des Lieux de la Littérature Internationale et cadre D’évaluation. Rapport D’évaluation Médico-Economique; Haute Autorité de Santé: Paris, France, 2013.
- Ahmed, S.S.T.; Thanuja, K.; Guptha, N.S.; Narasimha, S. Telemedicine approach for remote patient monitoring system using smart phones with an economical hardware kit. In Proceedings of the 2016 International Conference on Computing Technologies and Intelligent Data Engineering (ICCTIDE’16), Kovilpatti, India, 7–9 January 2016; pp. 1–4. [Google Scholar]
- Nittari, G.; Khuman, R.; Baldoni, S.; Pallotta, G.; Battineni, G.; Sirignano, A.; Amenta, F.; Ricci, G. Telemedicine practice: Review of the current ethical and legal challenges. Telemed. e-Health 2020, 26, 1427–1437. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.T.; Sandhya, M.; Sankar, S. A dynamic MooM dataset processing under TelMED protocol design for QoS improvisation of telemedicine environment. J. Med. Syst. 2019, 43, 257. [Google Scholar] [CrossRef]
- Paré, G.; Jaana, M.; Sicotte, C. Systematic review of home telemonitoring for chronic diseases: The evidence base. J. Am. Med. Inform. Assoc. 2007, 14, 269–277. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, P.; Daines, L.; Campbell, C.; McKinstry, B.; Weller, D.; Pinnock, H. Telehealth Interventions to Support Self-Management of Long-Term Conditions: A Systematic Metareview of Diabetes, Heart Failure, Asthma, Chronic Obstructive Pulmonary Disease, and Cancer. J. Med. Internet Res. 2017, 19, 172. [Google Scholar] [CrossRef]
- Douros, K.; Boutopoulou, B.; Papadopoulos, M.; Fouzas, S. Perception of dyspnea in children with asthma. Front. Biosci. 2015, 7, 469–477. [Google Scholar] [CrossRef]
- Still, L.; Dolen, W.K. The Perception of Asthma Severity in Children. Curr. Allergy Asthma Rep. 2016, 16, 50. [Google Scholar] [CrossRef]
- Douros, K.; Boutopoulou, B.; Priftis, K.N. Blunted perception of dyspnea in asthmatic children: A potential misleading criterion. World J. Clin. Pediatr. 2015, 4, 38–40. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, A.H.; Higgs, C.M.; Whitfield, M.J.; Laszlo, G. Accuracy of perception of severity of asthma: Patients treated in general practice. Br. Med. J. 1993, 307, 422–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, N.J.; Crichton, N.J.; Emerson, P.A.; Morgan, A.D. Quantitative assessment of the value of spirometry. Thorax 1986, 41, 360–363. [Google Scholar] [CrossRef] [Green Version]
- Feldman, J.M.; Steinberg, D.; Kutner, H.; Eisenberg, N.; Hottinger, K.; Sidora-Arcoleo, K.; Warman, K.; Serebrisky, D. Perception of pulmonary function and asthma control: The differential role of child versus caregiver anxiety and depression. J. Pediatr. Psychol. 2013, 38, 1091–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, R.R.; Mishoe, S.C.; Zaitoun, F.H.; Arant, C.B.; Lucas, J.; Rupp, N.T. Poor perception of airway obstruction in children with asthma. J. Asthma 2000, 37, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, A.F.J.; Roorda, R.J.; Brand, P.L.P. Home spirometry and asthma severity in children. Eur. Respir. J. 2006, 28, 1131–1137. [Google Scholar] [CrossRef] [Green Version]
- Magadle, R.; Berar-Yanay, N.; Weiner, P. The risk of hospitalization and near-fatal and fatal asthma in relation to the perception of dyspnea. Chest 2002, 121, 329–333. [Google Scholar] [CrossRef] [Green Version]
- Rhee, H.; Belyea, M.J.; Halterman, J.S. Adolescents’ Perception of Asthma Symptoms and Health Service Utilization. J. Pediatr. Health Care 2011, 25, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.J.; Szefler, S.J.; Reddel, H.K.; Chipps, B.E. Symptoms and perception of airway obstruction in asthmatic patients: Clinical implications for use of reliever medications. J. Allergy Clin. Immunol. 2019, 144, 1180–1186. [Google Scholar] [CrossRef] [Green Version]
- Deschildre, A.; Béghin, L.; Salleron, J.; Iliescu, C.; Thumerelle, C.; Santos, C.; Hoorelbeke, A.; Scalbert, M.; Pouessel, G.; Gnansounou, M.; et al. Home telemonitoring (forced expiratory volume in 1 s) in children with severe asthma does not reduce exacerbations. Eur. Respir. J. 2012, 39, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Honkoop, P.J.; Taylor, D.R.; Smith, A.D.; Snoeck-Stroband, J.B.; Sont, J.K. Early detection of asthma exacerbations by using action points in self-management plans. Eur. Respir. J. 2013, 41, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.R. IBM computer usability satisfaction questionnaires: Psychometric evaluation and instructions for use. Int. J. Hum. Comput. Interact. 1995, 7, 57–78. [Google Scholar] [CrossRef] [Green Version]
- Randolph, J.J. Free-marginal multirater kappa (multirater K [free]): An alternative to Fleiss’ fixed-marginal multirater kappa. In Proceedings of the Joensuu Learning and Instruction Symposium, Joensuu, Finland, 14–15 October 2005; Volume 2005. [Google Scholar]
- Eatough, V.; Smith, J. Interpretative phenomenological analysis. In The SAGE Handbook of Qualitative Research in Psychology; SAGE Publications Ltd.: London, UK, 2017; pp. 193–209. [Google Scholar]
- Pringle, J.; Drummond, J.; McLafferty, E.; Hendry, C. Interpretative phenomenological analysis: A discussion and critique. Nurse Res. 2011, 18, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Kew, K.M.; Cates, C.J. Home telemonitoring and remote feedback between clinic visits for asthma. Cochrane Database Syst Rev. 2016, 8, 1–72. [Google Scholar] [CrossRef] [Green Version]
- Katwa, U.; Rivera, E. Asthma Management in the Era of Smart-Medicine: Devices, Gadgets, Apps and Telemedicine. Indian J Pediatr. 2018, 85, 757–762. [Google Scholar] [CrossRef]
- Oppelaar, M.C.; van den Wijngaart, L.S.; Merkus, P.J.F.M.; Croonen, E.A.; Hugen, C.A.C.; Brouwer, M.L.; Roukema, J. It Is Not Just the FEV1 That Matters, but the Personal Goals We Reach Along the Way: Qualitative, Multicenter, Prospective, Observational Study. J. Med. Internet Res. 2021, 23, e29218. [Google Scholar] [CrossRef]
- Mougeot, F.; Robelet, M.; Rambaud, C.; Occelli, P.; Buchet-Poyau, K.; Touzet, S.; Michel, P. Emergence of the patient-actor in patient safety in France. A narrative review in social sciences and public health. Santé Publique 2018, 30, 73–81. [Google Scholar]
- Simpson, A.J.; Honkoop, P.J.; Kennington, E.; Snoeck-Stroband, J.B.; Smith, I.; East, J.; Coleman, C.; Caress, A.; Fan Chung, K.; Sont, J.K.; et al. Perspectives of patients and healthcare professionals on mHealth for asthma self-management. Eur. Respir. J. 2017, 49, 1601966. [Google Scholar] [CrossRef] [Green Version]
- Côté, J.; Cartier, A.; Malo, J.L.; Rouleau, M.; Boulet, L.P. Compliance with peak expiratory flow monitoring in home management of asthma. Chest 1998, 113, 968–972. [Google Scholar] [CrossRef]
- Wensley, D.C.; Silverman, M. The quality of home spirometry in school children with asthma. Thorax 2001, 56, 183–185. [Google Scholar] [CrossRef] [Green Version]
- Basharat, S.; Jabeen, U.; Zeeshan, F.; Bano, I.; Bari, A.; Rathore, A.W. Adherence to asthma treatment and their association with asthma control in children. J. Pak. Med. Assoc. 2018, 68, 725–728. [Google Scholar] [PubMed]
- Jochmann, A.; Artusio, L.; Jamalzadeh, A.; Nagakumar, P.; Delgado-Eckert, E.; Saglani, S.; Bush, A.; Frey, U.; Fleming, L.J. Electronic monitoring of adherence to inhaled corticosteroids: An essential tool in identifying severe asthma in children. Eur. Respir. J. 2017, 50, 1700910. [Google Scholar] [CrossRef] [PubMed] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Result | |
|---|---|---|
| Sex | Female | 13/26 (50) |
| Age (years) | 9.5 [8.0; 11.5] (min 6–max 18) | |
| Overweight/obesity (IOTF criteria > 25) | 6/26 (23) | |
| Age at 1st wheezing episode (years) | 1.4 [0.5; 3.6] | |
| Environment | ||
| Smoking during pregnancy | 5/26 (19) | |
| Post-natal passive smoking | 10/26 (38) | |
| Living area | Rural | 7/26 (27) |
| Semi-rural | 9/26 (35) | |
| Urban | 10/26 (38) | |
| Mold, dust at home | 6/26 (23) | |
| Pets | Cat | 10/26 (38) |
| Dog | 12/26 (46) | |
| Rabbit | 3/26 (12) | |
| Chicken | 2/26 (8) | |
| Hamster | 1/26 (4) | |
| Co-morbidities | ||
| Gastro-esophagal reflux disease (GERD) | 1/26 (4) | |
| Ear-nose-throat involvement (polyps, nasal obstruction, otitis media) | 4/26 (15) | |
| Obstructive Sleep Apnea Syndrome | 3/26 (12) | |
| Atopy-allergy | ||
| Family History | 24/26 (92) | |
| Prick-test or serum IgE (positive for pneum-allergens) | House Dust Mite | 14/26 (48) |
| Pollen | 10/26 (38) | |
| Mold | 2/26 (8) | |
| Dog dander | 5/26 (19) | |
| Cat dander | 4/26 (15) | |
| Atopic dermatitis | 11/26 (42) | |
| Allergic rhino-conjunctivitis | 16/26 (62) | |
| Food Allergy | 8/26 (31) | |
| Treatment | ||
| SABA (as required) | 26/26 (100) | |
| ICS only | 2/26 (8) | |
| LTRA | 13/26 (50) | |
| Combined ICS + LABA | 24/26 (92) | |
| Omalizumab | 3/26 (12) | |
| Theophylline | 1/26 (4) | |
| Severity (GINA level) | ||
| Moderate persistent, Level 3 | 4/26 (15.4) | |
| Severe persistent, Level 4 | 17/26 (65.4) | |
| Severe persistent, Level 5 | 5/26 (19.2) | |
| Asthma Control | ||
| ≥1 medical consultation for asthma exacerbation in the previous year | 19/23 (83) | |
| ≥1 hospitalization for asthma in the previous year | 12/24 (50) | |
| ≥1 hospitalization in intensive care for asthma, ever | 2/25 (8) | |
| Control according to GINA score | Well controlled | 2/25 (8) |
| Partly controlled | 11/25 (44) | |
| Uncontrolled | 12/25 (48) | |
| c-ACT score < 20 (uncontrolled) | 15/25 (60) | |
| Baseline FEV1 < 80% of predicted value | 4/26 (15) |
| Profile | Obs 1 | Obs 2 | Obs 3 | Results for All Patients after the Delphi Approach | Final Results for Classifiable Profiles after the Delphi Approach |
|---|---|---|---|---|---|
| Anarchic perceiver | 11/26 § | 4/26 ¤ | 8/26 ¤§ | 10/26 (38) | 10/23 (44) |
| Poor perceiver | 5/26 *§ | 13/26 *¤ | 10/26 §¤ | 7/26 (27) | 7/23 (30) |
| Good perceiver | 7/26 *§ | 9/26 *¤ | 5/26 §¤ | 4/26 (15) | 4/23 (17) |
| Excessive perceiver | 2/26 NA | 0/26 NA | 2/26 NA | 2/26 (8) | 2/23 (9) |
| Unclassifiable | 1/26 NA | 0/26 NA | 1/26 NA | 2/26 (8) | - |
| No consensus | - | - | - | 1/26 (4) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fossati, A.; Challier, C.; Dalhoumi, A.A.; Rose, J.; Robinson, A.; Perisson, C.; Galode, F.; Luaces, B.; Fayon, M. Telehome Monitoring of Symptoms and Lung Function in Children with Asthma. Healthcare 2022, 10, 1131. https://doi.org/10.3390/healthcare10061131
Fossati A, Challier C, Dalhoumi AA, Rose J, Robinson A, Perisson C, Galode F, Luaces B, Fayon M. Telehome Monitoring of Symptoms and Lung Function in Children with Asthma. Healthcare. 2022; 10(6):1131. https://doi.org/10.3390/healthcare10061131
Chicago/Turabian StyleFossati, Audrey, Caroline Challier, Aman Allah Dalhoumi, Javier Rose, Annick Robinson, Caroline Perisson, François Galode, Baptiste Luaces, and Michael Fayon. 2022. "Telehome Monitoring of Symptoms and Lung Function in Children with Asthma" Healthcare 10, no. 6: 1131. https://doi.org/10.3390/healthcare10061131