
Virtual Faculty and Peer Mentoring to Promote Social Belonging among Minoritized Physical Therapist and Nursing Students

 ,
,  , ,
, ,
Abstract
:1. Introduction
Theoretical Frameworks
2. Materials and Methods
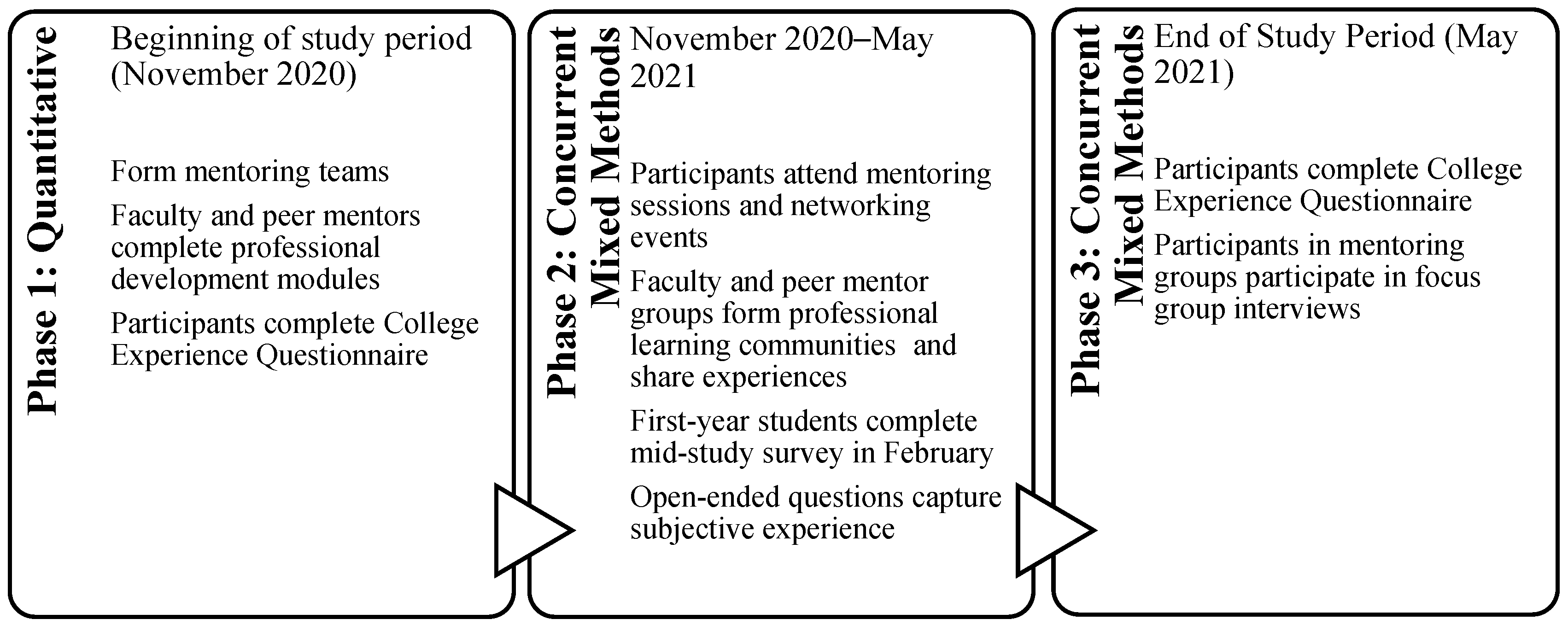
2.1. Study Design and Context
2.2. Participants
2.3. Intervention
2.4. Mentoring Teams
2.5. Networking Events
2.6. Comparison Group
2.7. Measures
2.8. Analysis
2.9. Trustworthiness
3. Results
“Both [faculty and peer] mentors helped me because I was getting stressed out about possibly wanting to switch my specialty, and it was something that had been on my mind for a long time… I did end up changing my specialty, because of their advice, so I think both of them helped me in terms of my future and just in general.”(FG 4, P2)
“I’m not saying that I am just my race, I am just my culture, but like you can’t ignore it, and you can’t ignore what is going on outside in the world. We’re not in our own little bubble, I wish we were sometimes.”(FG4, P2)
“There was a patient who I had a really hard time with, who was really inappropriate, used the “n-word” all the time, and it was really draining to keep interacting with this person on a constant basis. When I had brought it up to other people, they tried to always give me advice on how to steer clear from it or kind of dismiss it and say, “It’s this person’s illness.” … which is true. But I think that those are all answers which centered the patient.”(FG 2, P1)
“My peer mentor shared some of his own experiences working in health care and interacting with patients who were being racist. It felt really personally validating and made me feel like it’s okay, not everything is always about the patient. When I am removed from the situation, when I am at home, I can make it about myself.”(FG 1, P2)
“[The mentors] have personal experiences that make them who they are, and overcoming some challenges, and making me feel like I am not alone and I can do it too. They are smart, intelligent people, and resilient. Learning from their personal experiences I felt a little more confident too, that I can do this.”(FG 1, P2)
“We’re all not going to be able to have mentors of people exactly from your background. It’s nice when it happens because they share that perspective with you, but as we’re going to be moving through life, having to build relationships with people of other backgrounds, having to be comfortable in White spaces. I think that was still helpful.”(FG 4, P1)
“I definitely did not feel any sort of attachment to school at all prior just because of everything being remote and not being able to connect with any other students and I think the mentorship program definitely helped me feel some attachment to school.”(FG 2, P1)
“This was a wonderful experience for me, and this experience, for other students, to make it more sustainable, I worry about faculty of color and students of color, their invisible labor or the time and energy. This is energy consuming too, listening to what I have to go through, the challenges.”(FG 1, P2)
“I think it’s important for faculty of any background to take part in these types of studies because it allows them to meet and understand and start to just talk to students from different backgrounds and start building those relationships that might not be built in the classroom.”(FG 4, P1)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Mentee Interview Protocol
- What has your experience at this institution been like? How has the intervention shaped feelings of connectedness or alienation within the university community?
- Did this mentoring program enhance your educational and social experience as a first-year graduate student? If so, how?
- In what ways do you feel that the mentoring program facilitates first-year graduate students’ successful transition to graduate school?
- What is the greatest strength of this program?
- What has been your most positive experience in the mentoring program?
- What was your favorite program activity provided by the mentorship program?
- What components of the program were more effective than others?
- What are the challenges of being in a mentoring relationship?
- What suggestions do you have to make the mentorship program more effective and beneficial for faculty, peer mentors, and mentees?
- Is there anything else that you would like to mention about your experience in the mentorship program that I haven’t already covered?
References
- HHS Advisory Committee on Minority Health. Reflecting America’s Population. Diversifying a Competent Health Care Workforce for the 21st Century. 2011. Available online: https://minorityhealth.hhs.gov/Assets/pdf/Checked/1/FinalACMHWorkforceReport.pdf (accessed on 22 February 2022).
- U.S. Census Bureau Quick Facts. 2019. Available online: https://www.census.gov/quickfacts/fact/table/US/RHI125219 (accessed on 19 November 2021).
- National Conference of State Legislatures. Racial and Ethnic Health Disparities: Workforce Diversity. 2014. Available online: https://www.ncsl.org/documents/health/Workforcediversity814.pdf (accessed on 19 November 2021).
- Snyder, C.R.; Frogner, B.K.; Skillman, S.M. Facilitating racial and ethnic diversity in the health workforce. J. Allied Health 2018, 47, 58–69. [Google Scholar] [PubMed]
- Health Resources and Services Administration Bureau of Health Professions National Center for Health Workforce Analysis. The UE Nursing Workforce: Trends in Supply and Education. 2013. Available online: https://www.ruralhealthinfo.org/assets/1206-4974/nursing-workforce-nchwa-report-april-2013.pdf (accessed on 19 November 2021).
- American Physical Therapy Association. Physical Therapy Workforce Analysis: A Report from the American Physical Therapy Association. 2020. Available online: https://www.apta.org/your-career/careers-in-physical-therapy/workforce-data/apta-physical-therapy-workforce-analysis (accessed on 19 November 2021).
- Commission on Accreditation of Physical Therapy Education. Aggregate Program Data. 2019. Available online: http://www.capteonline.org/AggregateProgramData/ (accessed on 19 November 2021).
- Naidoo, K.; Yuhaniak, H.; Abel, Y. An ecological systems approach to exploring facilitators and barriers to success for minority students enrolled in a Doctor of Physical Therapy Program. Health Prof. Educ. 2020, 6, 394–405. [Google Scholar] [CrossRef]
- Utzman, R.R.; Riddle, D.L.; Jewell, D.V. Use of demographic and quantitative admissions data to predict academic difficulty among professional physical therapist students. Phys. Ther. 2007, 87, 1164–1180. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Norris, M.; Cassidy, E.; Naylor, S.; Marston, L.; Shiers, P. An investigation of the relationship between ethnicity and success in a BSc (hons) physiotherapy degree programme in the UK. Physiotherapy 2015, 101, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, R.; Birk, S.B.; Sherman, J. E-mentoring for Doctor of Nursing Practice students: A pilot program. J. Nurs. Educ. 2016, 55, 458–462. [Google Scholar] [CrossRef]
- Pryjmachuk, S.; Easton, K.; Littlewood, A. Nurse education: Factors associated with attrition. J. Adv. Nurs. 2009, 65, 149–160. [Google Scholar] [CrossRef]
- Utzman, R.R.; Riddle, D.L.; Jewell, D.V. Use of demographic and quantitative admissions data to predict performance on the national physical therapy examination. Phys. Ther. 2007, 87, 1181–1193. [Google Scholar] [CrossRef]
- Naidoo, K.; Clock, C.R.; Rimmel, L.M.; Wong, J.; Plummer, L.S. Navigating without a compass: How culturally and linguistically diverse physical therapist students persist in higher education. J. Best Pract. Health Prof. Divers. Educ. Res. Policy 2020, 13, 120–142. [Google Scholar]
- Diefenbeck, C.; Michalec, B.; Alexander, R. Lived experiences of racially and ethnically underrepresented minority BSN students: A case study specifically exploring issues related to recruitment and retention. Nurs. Educ. Perspect. 2016, 37, 41. [Google Scholar] [CrossRef]
- Edgoose, J.Y.C.; Steinkamp, L.; Vang, K.; Hampton, A.; Dosch, N. A qualitative study of undergraduate racial and ethnic minority experiences and perspectives on striving to enter careers in the health professions. WMJ 2019, 118, 60–64. [Google Scholar]
- Mikkonen, K.; Elo, S.; Kuivila, H.; Tuomikoski, A.; Kääriäinen, M. Culturally and linguistically diverse healthcare students’ experiences of learning in a clinical environment: A systematic review of qualitative studies. Int. J. Nurs. Stud. 2016, 54, 173–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naidoo, K.; Yuhaniak, H.; Borkoski, C.; Levangie, P.; Abel, Y. Networked mentoring to promote social belonging among minority physical therapist students and develop faculty cross-cultural psychological capital. Mentor. Tutoring Partnersh. Learn. 2021, 29, 586–606. [Google Scholar] [CrossRef]
- Cullen, D.L.; Rodak, B.; Fitzgerald, N.; Baker, S. Minority students benefit from mentoring programs. Radiol. Technol. 1993, 64, 226–231. [Google Scholar] [PubMed]
- Holloway, I.W.; Miyashita Ochoa, A.; Wu, E.S.; Himmelstein, R.; Wong, J.O.; Wilson, B.D. Perspectives on academic mentorship from sexual and gender minority students pursuing careers in the health sciences. Am. J. Orthopsyc. 2019, 89, 343–353. [Google Scholar] [CrossRef]
- Lewis, V.; Martina, C.A.; McDermott, M.P.; Trief, P.; Goodman, S.R.; Morse, G.D.; LaGuardia, J.G.; Sharp, D.; Ryan, R.M. A randomized controlled trial of mentoring interventions for underrepresented minorities. Acad Med. 2016, 91, 994. [Google Scholar] [CrossRef] [Green Version]
- Tram, J.M.; Nwankwo, N.; Khan, A.N.; Sabado, J.A. Impact of faculty mentoring on ethnic and racial minority student program satisfaction. Scholarsh. Teach. Learn. Psychol. 2020, 1–13. [Google Scholar] [CrossRef]
- Davis, D.J. Access to academe: The importance of mentoring to Black students. Negro Educ. Rev. 2007, 58, 217–231. [Google Scholar]
- Mireles-Rios, R.; Garcia, N.M. What would your ideal graduate mentoring program look like? Latina/o student success in higher education. J. Lat. Educ. 2019, 18, 376–386. [Google Scholar] [CrossRef]
- Columbaro, N.L. E-mentoring possibilities for online doctoral students: A literature review. Adult Learn. 2009, 20, 9–15. [Google Scholar] [CrossRef]
- Fayram, J.; Boswood, N.; Kan, Q.; Motzo, A.; Proudfoot, A. Investigating the benefits of online peer mentoring for student confidence and motivation. Int. J. Ment. 2018, 7, 312–328. [Google Scholar] [CrossRef] [Green Version]
- Owen, H.D. Making the most of mobility: Virtual mentoring and education practitioner professional development. Res. Learn. Technol. 2015, 23, 25566. [Google Scholar] [CrossRef] [Green Version]
- Clement, S.A.; Welch, S. Virtual mentoring in nursing education: A scoping review of the literature. J. Nurs. Educ. Pract. 2018, 8, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Tinto, V. Stages of student departure: Reflections on the longitudinal character of student leaving. J. High. Educ. 1988, 59, 438–455. [Google Scholar] [CrossRef]
- Sue, D.W.; Sue, D. Racial/Cultural Identity Development in People of Color: Therapeutic Implications. In Counseling the Culturally Diverse: Theory and Practice; Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 287–310. [Google Scholar]
- Leech, N.L.; Onwuegbuzie, A.J. A typology of mixed methods research designs. Qual. Quant. 2009, 43, 265–275. [Google Scholar] [CrossRef]
- Omatsu, G. Mentoring on the Run: CSUN’s Response to the Challenge of Mentoring at a Large, Commuter Campus. 2002. Available online: https://www.csun.edu/sites/default/files/mentorontherun.pdf (accessed on 19 November 2021).
- Wright-Harp, W.; Cole, P.A. A mentoring model for enhancing success in graduate education. Contemp. Issues Commun. Sci. Disord. 2008, 35, 4–16. [Google Scholar] [CrossRef]
- Chan, A.W. Mentoring ethnic minority, pre-doctoral students: An analysis of key mentor practices. Mentor. Tutoring Partnersh. Learn. 2008, 16, 263–277. [Google Scholar] [CrossRef]
- Spivey-Mooring, T. Cultural Alienation, Mental Health and Attitudes toward Seeking Psychological Help among Students of Color at Predominantly White Universities. Ph.D. Thesis, Lehigh University, Bethlehem, PA, USA, 2008. [Google Scholar]
- Spivey-Mooring, T.; Apprey, C.B. University of Virginia graduate mentoring institute: A model program for graduate student success. Peabody, J. Educ. 2014, 89, 393–410. [Google Scholar] [CrossRef]
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis: A Methods Sourcebook; Sage: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Guba, E.G. Criteria for assessing the trustworthiness of naturalistic inquiries. ECTJ 1981, 29, 75–91. [Google Scholar] [CrossRef]
- Denzin, N.K.; Lincoln, Y.S. Introduction: Entering the Field of Qualitative Research. In Handbook of Qualitative Research; Denzin, N.K., Lincoln, Y.S., Eds.; Sage: Thousand Oaks, CA, USA, 1994; pp. 1–17. [Google Scholar]
- Chong, J.Y.; Ching, A.H.; Renganathan, Y.; Lim, W.Q.; Toh, Y.P.; Mason, S.; Krishna, L.K. Enhancing mentoring experiences through E-mentoring: A systematic scoping review of E-mentoring programs between 2000 and 2017. Adv. Health Sci. Educ. 2020, 25, 195–226. [Google Scholar] [CrossRef]
- McConnell, K.R.; Geesa, R.L. Filling the gaps: How the non-faculty mentor role contributes to the doctoral program support structure. Int. J. Ment. 2021, 27, 188–202. [Google Scholar] [CrossRef]
- Hill, K.A.; Samuels, E.A.; Gross, C.P.; Desai, M.M.; Zelin, N.S.; Latimore, D.; Huot, S.J.; Cramer, L.D.; Wong, A.H.; Boatright, D. Assessment of the prevalence of medical student mistreatment by sex, race/ethnicity, and sexual orientation. JAMA Int. Med. 2020, 180, 653–665. [Google Scholar] [CrossRef]
- McGee, E.; Bentley, L. The equity ethic: Black and Latinx college students reengineering their STEM careers toward justice. Am. J. Educ. 2017, 124, 1–36. [Google Scholar] [CrossRef]
- Fullick, J.M.; Smith-Jentsch, K.; Yarbrough, C.S.; Scielzo, S.A. Mentor and protege goal orientations as predictors of newcomer stress. J. Scholarsh. Teach. Learn. 2012, 12, 59–73. [Google Scholar]
- Walton, G.M.; Cohen, G.L.; Cwir, D.; Spencer, S.J. Mere belonging: The power of social connections. J. Pers. Soc. Psychol. 2012, 102, 513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yomtov, D.; Plunkett, S.W.; Efrat, R.; Marin, A.G. Can peer mentors improve first-year experiences of university students? J. Coll. Stud. Retent. Res. Theory Pract. 2017, 19, 25. [Google Scholar] [CrossRef]
- Dickson, T.; Zafereo, J. Faculty and programmatic influences on the percentage of graduates of color from professional physical therapy programs in the United States. Adv. Health Sci. Educ. 2021, 26, 215–235. [Google Scholar] [CrossRef] [PubMed]
- Matthews, A.K.; Allen-Meares, P.; Watson, K.; Crooks, N.; Smith, A.; Hart, A.; Estrella, M.L.; Kim, S. The use of strategies from the social sciences to inform pipeline development programs for under-represented minority faculty and students in the health sciences. J. Clin. Transl. Sci. 2020, 5, e73. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Data | First Year Graduate Students (All) (N = 336) | Intervention Group (n = 8) | Comparison Group (n = 16) |
|---|---|---|---|
| Program | |||
| CSD | 63 | -- | 6 |
| DPT | 72 | 4 | 3 |
| GC | 20 | -- | 1 |
| NS | 101 | 4 | 4 |
| OTD | 36 | -- | 1 |
| PA | 44 | -- | 1 |
| Ethnicity | |||
| Asian | 44 (13.1%) | 2 (25%) | 2 (12.5%) |
| Black/African American | 23 (6.8%) | 4 (50%) | -- |
| Hispanic | 24 (7.1%) | 2 (25%) | -- |
| White | 223 (66.4%) | -- | 13 (81.3%) |
| Mixed Race | 17 (5.1%) | -- | 1 (6.3%) |
| Unknown | 5 (1.5%) | -- | -- |
| Critical Elements and Number of Participants Who Agreed That Their Faculty Advisor Reviewed the Following Areas during Meetings | Intervention Group (n = 8) | Comparison Group (n = 15) | ||
|---|---|---|---|---|
| Mid-Study | End of Study | Mid-Study | End of Study | |
| Coursework | 7 (87.5%) | 7 (87.5%) | 9 (56.3%) | 12 (75%) |
| Clinical education experiences | 5 (62.5%) | 7 (87.5%) | 6 (37.5%) | 8 (50%) |
| Professional development | 6 (75%) | 4 (50%) | 4 (25%) | 7 (43.8%) |
| My challenges thus far in the program | 7 (87.5%) | 8 (100%) | 11 (68.8%) | 11 (68.8%) |
| My successes thus far in the program | 4 (50%) | 6 (75%) | 7 (43.8%) | 10 (62.5%) |
| My concerns | 7 (87.5%) | 8(100%) | 12 (75%) | 10 (62.5%) |
| College Experience Questionnaire (CEQ) | Intervention Group Mean (SD) | Comparison Group Mean (SD) | ||
|---|---|---|---|---|
| Mid-Study | End of Study | Mid-Study | End of Study | |
| Total score | 70.25 (7.62) | 66.00 (11.11) | 72.73 (8.52) | 70.80 (4.96) |
| Subscales: | ||||
| University connectedness | 32.38 (4.93) | 30.75 (4.77) | 33.4 (4.67) | 31.67 (4.85) |
| University environment | 29.38 (5.32) | 27.13 (7.75) | 33.00 (4.38) | 32.47 (3.11) |
| University alienation | 8.50 (3.21) | 8.13 (2.85) | 6.33 (1.54) | 6.67 (2.32) |
| Sample individual CEQ items: | ||||
| I feel fully entitled to all of the resources available on campus | 3.6 | 3.9 | 2.8 | 3.1 |
| I feel socially alienated at this institution | 2.6 | 2.3 | 2.4 | 2.4 |
| I feel racially isolated | 3.0 | 2.7 | 1.6 | 1.5 |
| I believe that there are enough resources on campus to deal with any racial or cultural issue a student may have | 3.1 | 3.3 | 3.6 | 3.1 |
| There are sufficient minority faculty and staff to serve as resources for students | 2.5 | 2.4 | 2.8 | 2.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naidoo, K.; Plummer, L.; McKean, M.; Mack, A.; Bowdle, G.K.; Mullins, M.A.; Gore, S. Virtual Faculty and Peer Mentoring to Promote Social Belonging among Minoritized Physical Therapist and Nursing Students. Healthcare 2022, 10, 416. https://doi.org/10.3390/healthcare10030416
Naidoo K, Plummer L, McKean M, Mack A, Bowdle GK, Mullins MA, Gore S. Virtual Faculty and Peer Mentoring to Promote Social Belonging among Minoritized Physical Therapist and Nursing Students. Healthcare. 2022; 10(3):416. https://doi.org/10.3390/healthcare10030416
Chicago/Turabian StyleNaidoo, Keshrie, Laura Plummer, Martha McKean, Amanda Mack, Garrett Kelley Bowdle, Margaret Anne Mullins, and Shweta Gore. 2022. "Virtual Faculty and Peer Mentoring to Promote Social Belonging among Minoritized Physical Therapist and Nursing Students" Healthcare 10, no. 3: 416. https://doi.org/10.3390/healthcare10030416