
Establishing a New ECMO Referral Center Using an ICU-Based Approach: A Feasibility and Safety Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
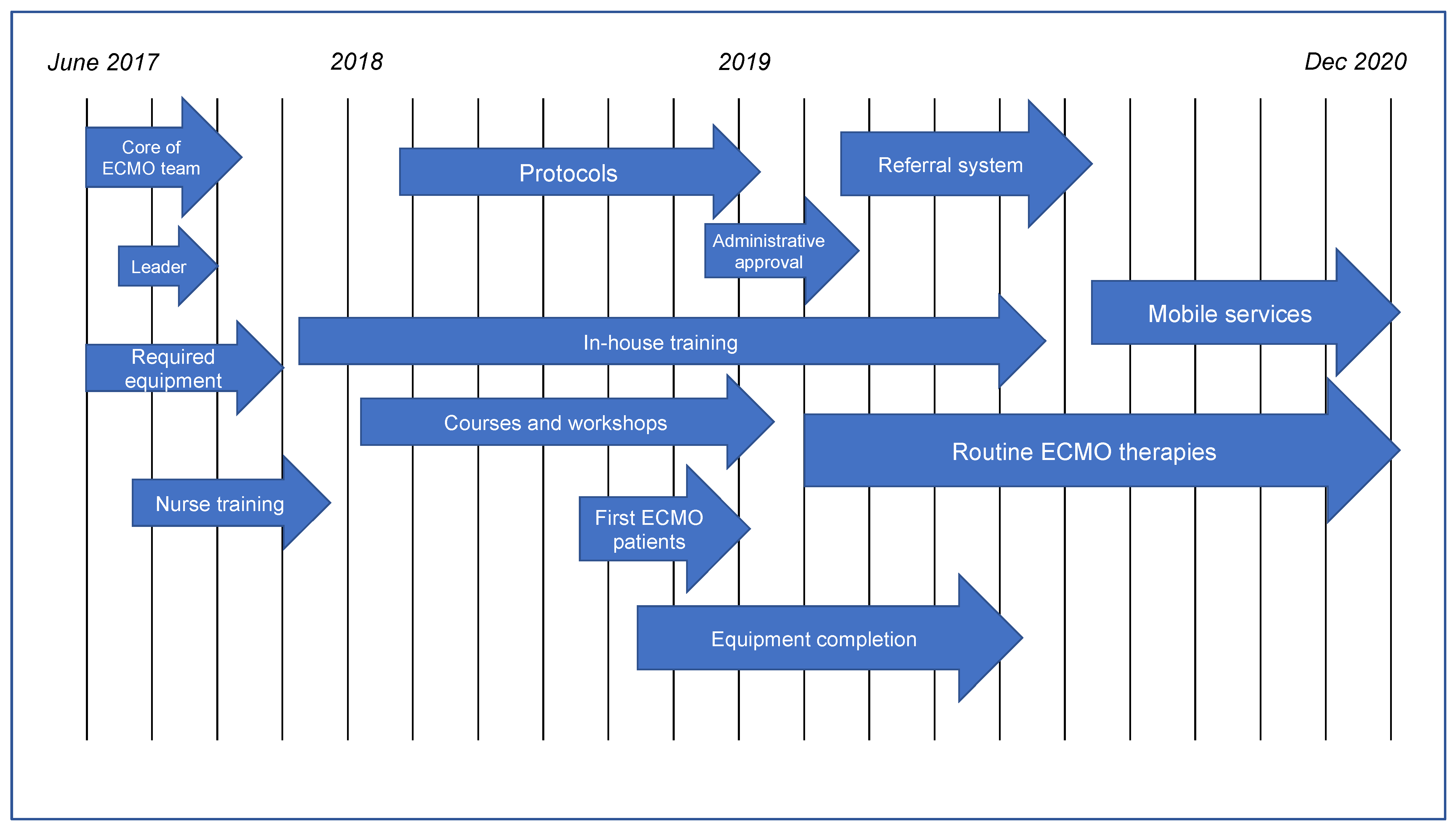
2.1. Initialization
2.2. Training
2.3. Preparation
2.4. Activation
2.5. Protocols
2.6. Patient Treatment
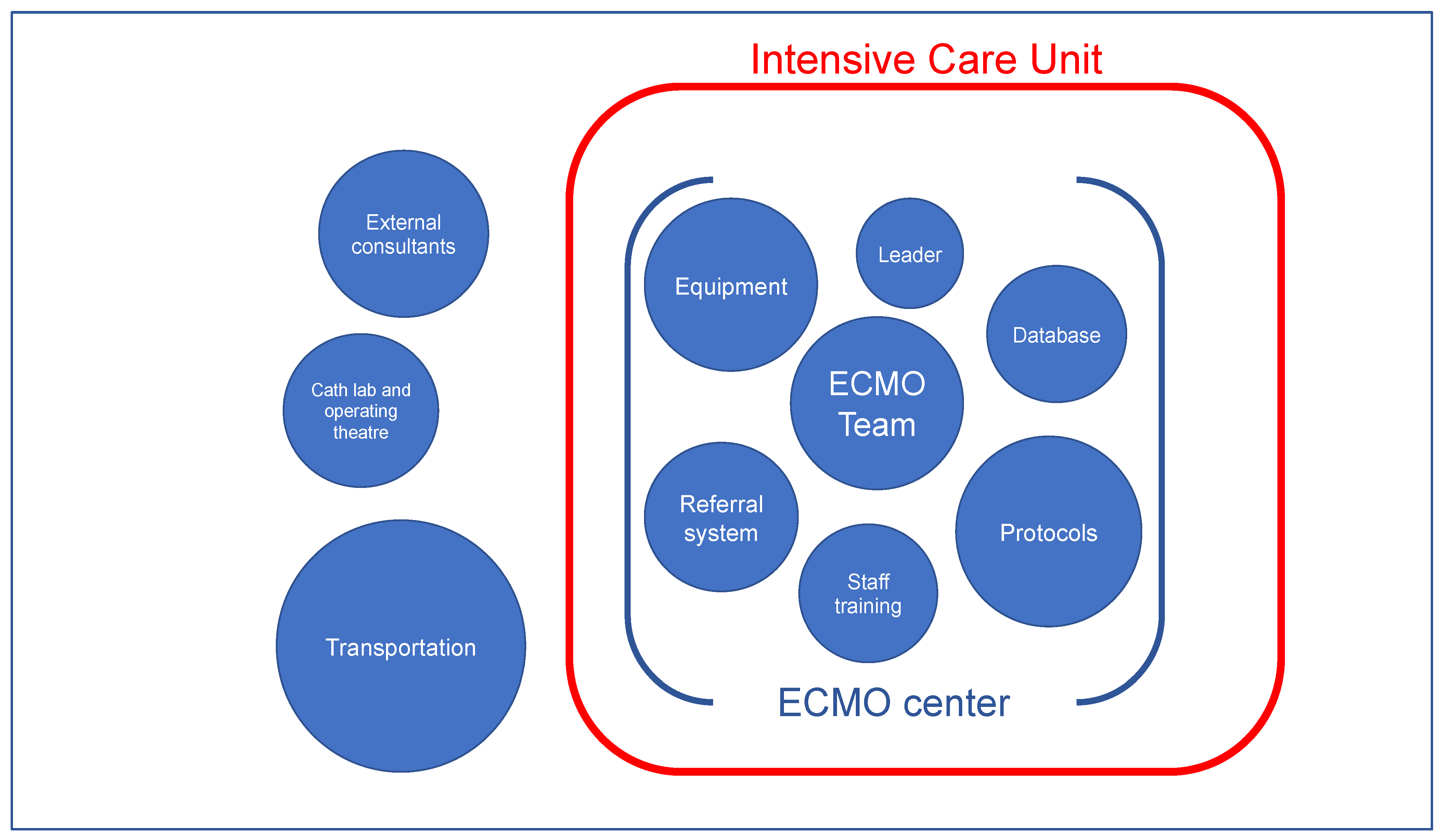
2.7. Staff and Equipment
2.8. Referral System
2.9. ECMO Transportation
2.10. Database
2.11. Statistical Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ratnani, I.; Tuazon, D.; Zainab, A.; Uddin, F. The role and impact of extracorporeal membrane oxygenation in critical care. Methodist Debakey Cardiovasc. J. 2018, 14, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Extracorporeal Life Support Organization: ECLS Registry Report. Available online: https://www.elso.org/Registry/Statistics.aspx (accessed on 21 September 2021).
- Barbaro, R.P.; Odetola, F.O.; Kidwell, K.M.; Paden, M.L.; Bartlett, R.H.; Davis, M.M.; Annich, G.M. Association of hospital-level volume of extracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry. Am. J. Respir. Crit. Care 2015, 191, 894–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becher, P.M.; Goßling, A.; Schrage, B.; Twerenbold, R.; Fluschnik, N.; Seiffert, M.; Bernhardt, A.M.; Reichenspurner, H.; Blankenberg, S.; Westermann, D. Procedural volume and outcomes in patients undergoing VA-ECMO support. Crit. Care 2020, 24, 291. [Google Scholar] [CrossRef] [PubMed]
- Friedrichson, B.; Mutlak, H.; Zacharowski, K.; Piekarski, F. Insight into ECMO, mortality and ARDS: A nationwide analysis of 45,647 ECMO runs. Crit. Care 2021, 25, 38. [Google Scholar] [CrossRef]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Bartlett, R.H.; Tonna, J.E.; Hyslop, R.; Fanning, J.J.; et al. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the extracorporeal life support organization registry. Lancet 2020, 396, 1071–1078. [Google Scholar] [CrossRef]
- ELSO. ELSO Guidelines for ECMO Centers. Available online: https://www.elso.org/Resources/Guidelines.aspx (accessed on 21 September 2021).
- Abrams, D.; Garan, A.R.; Abdelbary, A.; Bacchetta, M.; Bartlett, R.H.; Beck, J.; Belohlavek, J.; Chen, Y.S.; Fan, E.; Ferguson, N.D.; et al. Position paper for the organization of ECMO programs for cardiac failure in adults. Intensive Care Med. 2018, 44, 717–729. [Google Scholar] [CrossRef]
- Combes, A.; Brodie, D.; Bartlett, R.; Brochard, L.; Brower, R.; Conrad, S.; De Backer, D.; Fan, E.; Ferguson, N.; Fortenberry, J.; et al. Position paper for the organization of extracorporeal membrane oxygenation programs for acute respiratory failure in adult patients. Am. J. Respir. Crit. Care 2014, 190, 488–496. [Google Scholar] [CrossRef]
- DellaVolpe, J.; Barbaro, R.P.; Cannon, J.W.; Fan, E.; Greene, W.R.; Gunnerson, K.J.; Napolitano, L.M.; Ovil, A.; Pamplin, J.C.; Schmidt, M.; et al. Joint society of critical care medicine-extracorporeal life support organization task force position paper on the role of the intensivist in the initiation and management of extracorporeal membrane oxygenation. Crit. Care Med. 2020, 48, 838–846. [Google Scholar] [CrossRef]
- Elkhwad, M.; More, K.S.; Anand, D.; Al-Maraghi, S.; Crowe, M.; Wong, D.; Metcalf, J.; Yadav, S.K.; Sigalet, D. Successful establishment of the first neonatal respiratory extracorporeal membrane oxygenation (ECMO) program in the middle east, in collaboration with pediatric services. Front. Pediatr. 2020, 8, 506. [Google Scholar] [CrossRef]
- Cianchi, G.; Lazzeri, C.; Bonizzoli, M.; Batacchi, S.; Cozzolino, M.; Ciapetti, M.; Bernardo, P.; Franci, A.; Chiostri, M.; Peris, A. The 8-year experience of the florence referral ECMO center and retrieval team for acute respiratory failure. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1142–1150. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef] [PubMed]
- Shekar, K.; Badulak, J.; Peek, G.; Boeken, U.; Dalton, H.J.; Arora, L.; Zakhary, B.; Ramanathan, K.; Starr, J.; Akkanti, B.; et al. Extracorporeal life support organization coronavirus disease 2019 interim guidelines: A consensus document from an international group of interdisciplinary extracorporeal membrane oxygenation providers. Asaio J. 2020, 66, 707–721. [Google Scholar] [CrossRef] [PubMed]
- Cotza, M.; Carboni, G.; Ballotta, A.; Kandil, H.; Isgrò, G.; Carlucci, C.; Varrica, A.; Garatti, A.; Giamberti, A.; Ranucci, M. Modern ECMO: Why an ECMO programme in a tertiary care hospital. Eur. Heart J. Suppl. 2016, 18 (Suppl. E), E79–E85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shih, E.; DiMaio, J.M.; Squiers, J.J.; Banwait, J.K.; Meyer, D.M.; George, T.J.; Schwartz, G.S.; Baylor Scott & White ECMO for COVID Group. Venovenous extracorporeal membrane oxygenation for patients with refractory Covid-19: Multicenter experience of referral hospitals in a large healthcare system. J. Thorac. Cardiovasc. Surg. 2020, 163, 1071–1079.e3. [Google Scholar] [CrossRef] [PubMed]
- Patroniti, N.; Zangrillo, A.; Pappalardo, F.; Peris, A.; Cianchi, G.; Braschi, A.; Iotti, G.A.; Arcadipane, A.; Panarello, G.; Ranieri, V.M.; et al. The Italian ECMO network experience during the 2009 influenza A(H1N1) pandemic: Preparation for severe respiratory emergency outbreaks. Intensive Care Med. 2011, 37, 1447. [Google Scholar] [CrossRef]
- Belohlávek, J.; Rohn, V.; Tosovsky, J.; Kunstyr, J.; Semrád, M.; Horák, J.; Lips, M.; Mlejnsky, F.; Vykydal, I.; Balík, M.; et al. A review of a newly established ECMO program in a university affiliated cardiac center. J. Cardiovasc. Surg. 2011, 52, 445–451. [Google Scholar]
- Tipograf, Y.; Liou, P.; Oommen, R.; Agerstrand, C.; Abrams, D.; Brodie, D.; Bacchetta, M. A decade of interfacility extracorporeal membrane oxygenation transport. J. Thorac. Cardiovasc. Surg. 2019, 157, 1696–1706. [Google Scholar] [CrossRef]
- Vaja, R.; Chauhan, I.; Joshi, V.; Salmasi, Y.; Porter, R.; Faulkner, G.; Harvey, C. Five-year experience with mobile adult extracorporeal membrane oxygenation in a tertiary referral center. J. Crit. Care 2015, 30, 1195–1198. [Google Scholar] [CrossRef]
- Bonadonna, D.; Barac, Y.D.; Ranney, D.N.; Rackley, C.R.; Mumma, K.; Schroder, J.N.; Milano, C.A.; Daneshmand, M.A. Interhospital ECMO transport: Regional focus. Semin. Thorac. Cardiovasc. Surg. 2019, 31, 327–334. [Google Scholar] [CrossRef]
- Na, S.J.; Chung, C.R.; Choi, H.J.; Cho, Y.H.; Sung, K.; Yang, J.H.; Suh, G.Y.; Jeon, K. The effect of multidisciplinary extracorporeal membrane oxygenation team on clinical outcomes in patients with severe acute respiratory failure. Ann. Intensive Care 2018, 8, 31. [Google Scholar] [CrossRef]
- Hong, D.; Choi, K.H.; Cho, Y.H.; Cho, S.H.; Park, S.J.; Kim, D.; Park, T.K.; Lee, J.M.; Song, Y.B.; Choi, J.O.; et al. Multidisciplinary team approach in acute myocardial infarction patients undergoing veno-arterial extracorporeal membrane oxygenation. Ann. Intensive Care 2020, 10, 83. [Google Scholar] [CrossRef]
- Komindr, A.; Abe, R.; Tateishi, Y.; Takahashi, Y.; Goto, J.; Wada, K.; Furukawa, Y.; Sugiura, A.; Imaeda, T.; Suga, N.; et al. Establishing extracorporeal membrane oxygenation team increased number of patients and improved data recording. J. Intensive Care 2019, 7, 11. [Google Scholar] [CrossRef]
- Bellomo, R.; Cole, L.; Reeves, J.; Silvester, W. Who should manage CRRT in the ICU? The intensivist’s viewpoint. Am. J. Kidney Dis. 1997, 30, S109–S111. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | All Patients (n = 33) | VV-ECMO (n = 22) | VA-ECMO (n = 11) | p Value |
|---|---|---|---|---|
| Age, years | 52 (40–59) | 52 (39–58) | 53 (44–68) | 0.2381 |
| Female sex, n (%) | 8 (24.2) | 4 (18.2) | 4 (36.4) | 0.4727 |
| Weight, kg | 80 (70–99) | 85 (70–99) | 72 (68–89) | 0.1516 |
| BMI, kg/cm2 | 26 (23–31) | 26 (23–33) | 25 (24–28) | 0.1799 |
| SOFA score | 9 (7–12), n = 30 | 7 (6–12) | 11 (10–14), n = 8 | 0.0051 |
| CRRT, n (%) | 16 (48.5) | 11 (50) | 5 (45.5) | 0.9020 |
| ECMO duration, hours | 277 (56–464) | 365 (218–496) | 49 (12–113) | 0.0006 |
| ICU length of stay, days | 17 (6–33) | 19 (9–37) | 6 (2–20) | 0.0355 |
| All Patients (n = 22) | Status at 90 Days after ECMO | p Value | ||
|---|---|---|---|---|
| Alive (n = 13) | Dead (n = 9) | |||
| Mode of circuit | ||||
| Jugulo-femoral, n (%) | 17 (77.3) | 10 (76.9) | 7 (77.8) | 0.6381 |
| Femoro-femoral, n (%) | 5 (22.7) | 3 (23.1) | 2 (22.2) | 0.6381 |
| Admission cannula, Fr | 25 (23–25); n = 15 | 25 (23–25); n = 8 | 25 (24–25); n = 7 | 0.6754 |
| Return cannula, Fr | 23 (22–24); n = 15 | 23 (22–25); n = 8 | 23 (21–23); n = 7 | 0.2238 |
| Indications for ECMO | ||||
| ARDS of viral etiology, n (%) | 10 (45.5) | 6 (46.1) | 4 (44.4) | 0.4789 |
| ARDS of bacterial etiology, n (%) | 8 (36.4) | 5 (38.4) | 3 (33.3) | 0.4423 |
| ARDS of unknown etiology, n (%) | 4 (18.2) | 2 (15.4) | 2 (22.2) | 0.4309 |
| Ventilation before ECMO | ||||
| Peak pressure, cm H2O | 31 (29–34); n = 20 | 33 (30–35); n = 12 | 30 (28–32); n = 8 | 0.3788 |
| Plateau pressure, cm H2O | 29 (26–32); n = 16 | 30 (27–34); n = 9 | 26 (26–30); n = 7 | 0.3350 |
| Driving pressure, cm H2O | 16 (13–18); n = 19 | 16 (14–19); n = 11 | 15 (12–17); n = 8 | 0.4101 |
| PEEP, cm H2O | 12 (12–14) | 14 (12–15) | 12 (11–14) | 0.1794 |
| FiO2 | 0.8 (0.7–1) | 0.8 (0.6–1) | 0.8 (0.8–1) | 0.3294 |
| Tidal volume, mL/kg PBW | 5 (4–5); n = 13 | 5.7 (4–6); n = 7 | 4.9 (4–5); n = 6 | 0.2644 |
| Prone position, n (%) | 8 (36.4) | 6 (46.1) | 2 (22.2) | 0.4861 |
| Intervention on ECMO | ||||
| Mechanical ventilation, hours | 365 (179–496) | 336 (168–500) | 432 (215–476) | 0.7528 |
| Sedation, hours | 306 (132–470); n = 19 | 306 (132–458); n = 11 | 336 (170–467); n = 8 | 0.9099 |
| Neuromuscular blockade, n (%) | 14 (63.6) | 9 (69.2) | 5 (55.5) | 0.8377 |
| Tracheostomy, n (%) | 13 (59.1) | 8 (61.5) | 5 (55.5) | 0.8726 |
| VA-ECMO (n = 11) | |
|---|---|
| Mode of circuit | |
| Femoro-femoral, n (%) | 8 (72.7) |
| Jugulo-femoral, n (%) | 3 (27.3) |
| Admission cannula, Fr | 25 (25–27); n = 6 |
| Return cannula, Fr | 18 (17–19); n = 6 |
| Indications for ECMO | |
| Myocardial infarction, n (%) | 4 (36.3) |
| Myocarditis, n (%) | 2 (18.2) |
| Cardiac arrest, n (%) | 2 (18.2) |
| High-risk coronary angioplasty, n (%) | 3 (27.3) |
| Parameters before ECMO | |
| MAP, mm Hg | 50 (35–56); n = 8 |
| HR | 96 (86–115); n = 6 |
| EF LV, percentage | 15 (5–20); n = 9 |
| Creatinine, mg/dL | 1.25 (0.8–1.6); n = 10 |
| Arterial, pH | 7.1 (7.1–7.2); n = 6 |
| Lactate, mmol/L | 10 (7–13); n = 5 |
| Medication before ECMO | |
| Norepinephrine, μg/kg/min | 0.2 (0–0.3); n = 10 |
| Dobutamine, mg/kg/min | 0 (0–0); n = 10 |
| Adrenaline, μg/kg/min | 0 (0–0); n = 10 |
| Mode of LV venting | |
| IABP, n (%) | 1 (9.1) |
| Atrial septostomy, n (%) | 1 (9.1) |
| Impella, n (%) | 2 (18.2) |
| Multidisciplinary Approach | ICU-Based Approach | |
|---|---|---|
| Staff | Specialists from different hospital wards | Entirely ICU personnel |
| Leadership | Possibly a director from outside the ICU | Leader from the staff of the ICU |
| Who treat | Purpose-built multidisciplinary team | Intensivists, consultants only upon request |
| Who for | Only ECMO patients | One of the routine modalities in the ICU |
| Administrative structure | A separate structure in the hospital | An integral part of an existing ICU |
| Premises | Possibly external to the ICU | Only premises of the ICU |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gawda, R.; Piwoda, M.; Marszalski, M.; Lyp, K.; Piwoda, J.; Maj, M.; Gawor, M.; Molsa, M.; Pietka, M.; Czarnik, T. Establishing a New ECMO Referral Center Using an ICU-Based Approach: A Feasibility and Safety Study. Healthcare 2022, 10, 414. https://doi.org/10.3390/healthcare10030414
Gawda R, Piwoda M, Marszalski M, Lyp K, Piwoda J, Maj M, Gawor M, Molsa M, Pietka M, Czarnik T. Establishing a New ECMO Referral Center Using an ICU-Based Approach: A Feasibility and Safety Study. Healthcare. 2022; 10(3):414. https://doi.org/10.3390/healthcare10030414
Chicago/Turabian StyleGawda, Ryszard, Maciej Piwoda, Maciej Marszalski, Katarzyna Lyp, Jolanta Piwoda, Magdalena Maj, Maciej Gawor, Maciej Molsa, Marek Pietka, and Tomasz Czarnik. 2022. "Establishing a New ECMO Referral Center Using an ICU-Based Approach: A Feasibility and Safety Study" Healthcare 10, no. 3: 414. https://doi.org/10.3390/healthcare10030414