

An Analysis of Body Language of Patients Using Artificial Intelligence
 ,
,  , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Body Language Analysis
2.1. Overview of Body Language Analysis
2.2. Body Language Analysis in Communication
2.3. Body Language in Public Speaking
2.4. Body Language Analysis in Teaching
2.5. Body Language Analysis in Sport
2.6. Body Language Analysis in Leadership
2.7. Body Language Analysis in Culture
- Eye contact differs by culture.
- Other nonverbal signals vary by culture.
- The right distance between two individuals reveals their distinct attitudes from different civilizations.
2.8. Body Language in Body Motions
2.8.1. Facial Expressions
2.8.2. Gestures
3. Body Language Analysis and AI
3.1. Overview
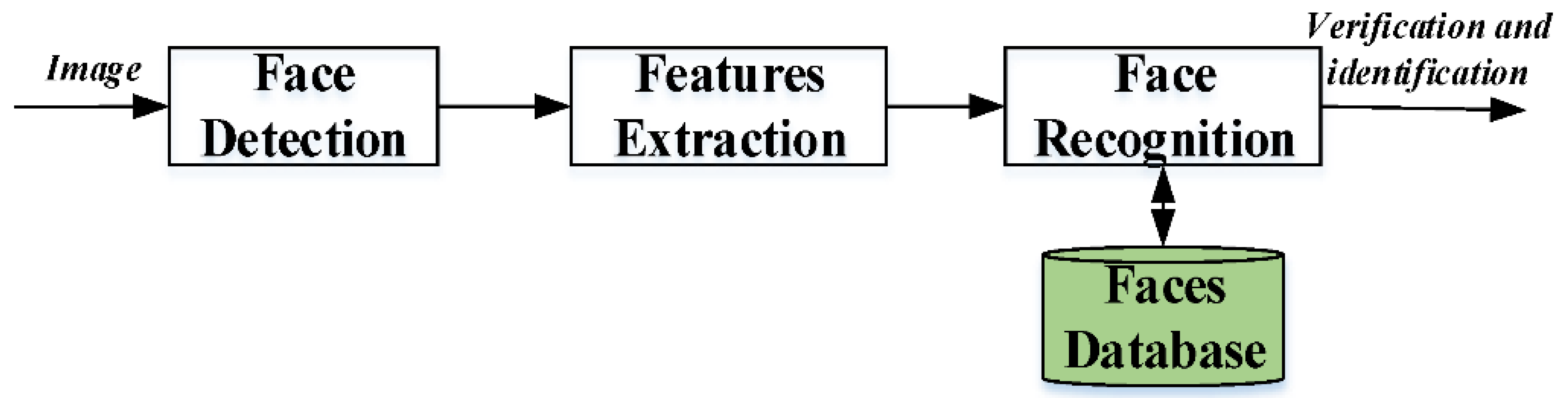
3.2. Recognition of Facial Expressions
3.2.1. Face Detection
3.2.2. Feature Extraction
3.2.3. Face Recognition
3.3. Face Recognition Techniques
3.3.1. D Facial Recognition
3.3.2. Multimodal Facial Recognition
3.3.3. Deep Learning Facial Recognition
3.4. Recognition of Gestures
3.4.1. Convolutional Neural Networks in 2D
3.4.2. Features That Are Dependent on Motion
3.4.3. Convolutional Neural Networks in 3D
3.4.4. RNN and LSTM Models for Temporal Deep Learning
4. Body Language Analysis of Patients and AI
4.1. Overview
4.2. Facial Recognition
4.3. Fall Detection
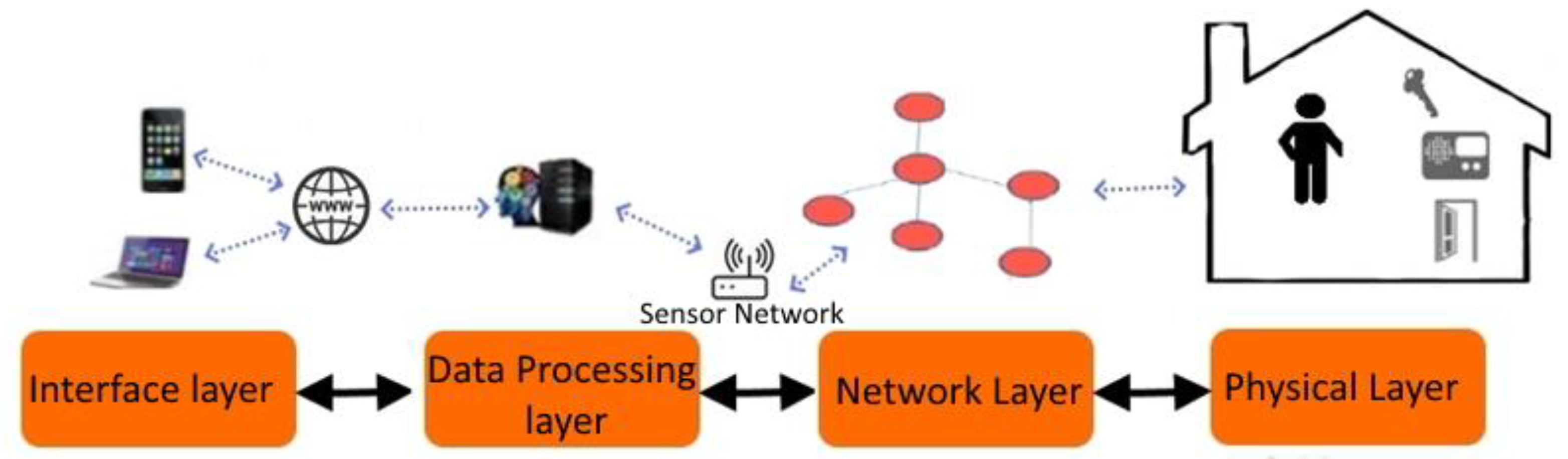
4.4. Smart Homes in Health Care
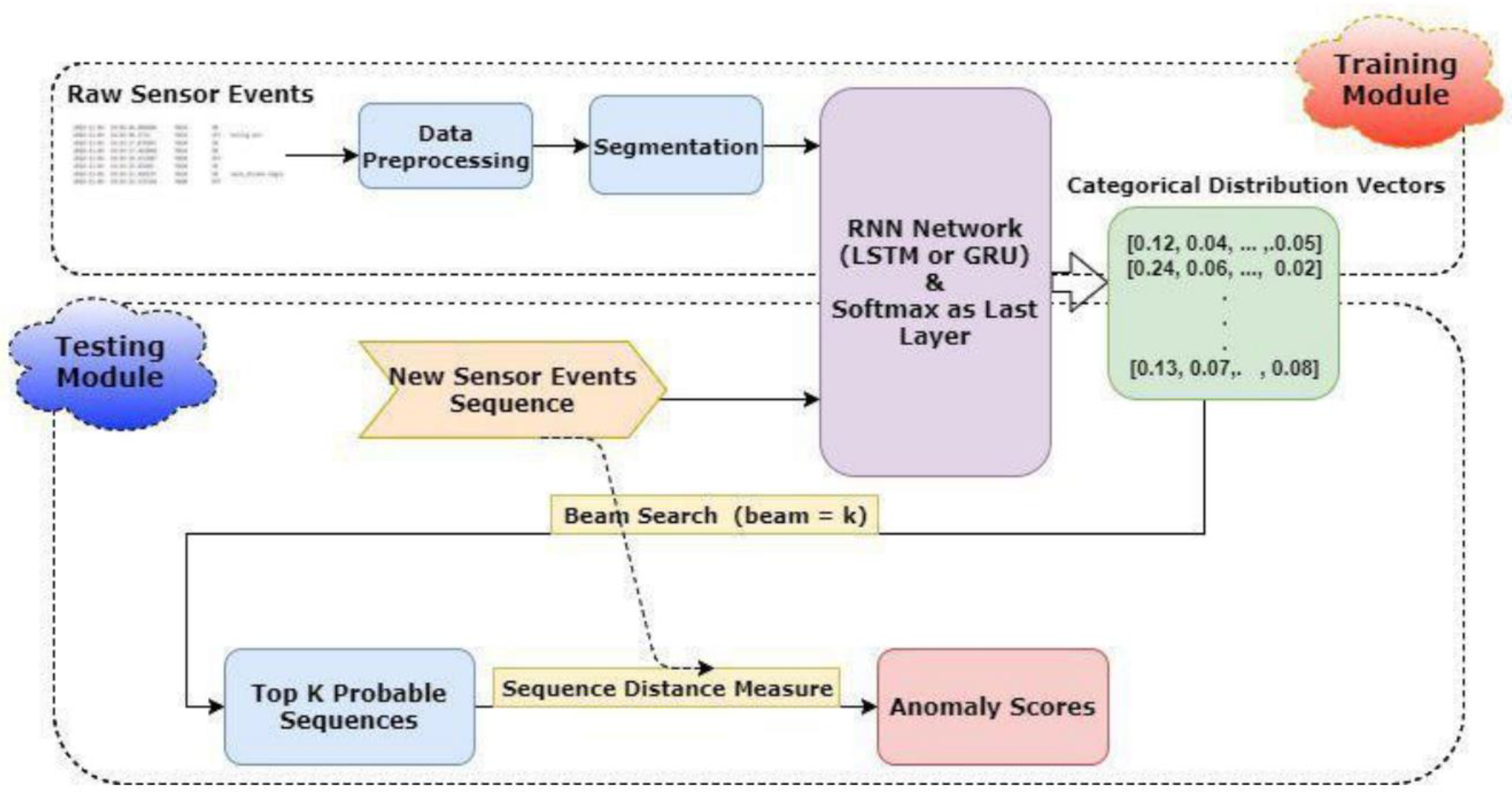
4.4.1. Anomaly Detection Using Deep Learning
- The SA value is derived by adding the S and A values together.
- SA’s character string has been encoded. This encoding can be done in one of two ways: one-hot encoding or word embedding.
- D is determined by subtracting the current and previous event timestamps.
- The return of time, periodicity, and cycle are all taken into account while converting timestamps.
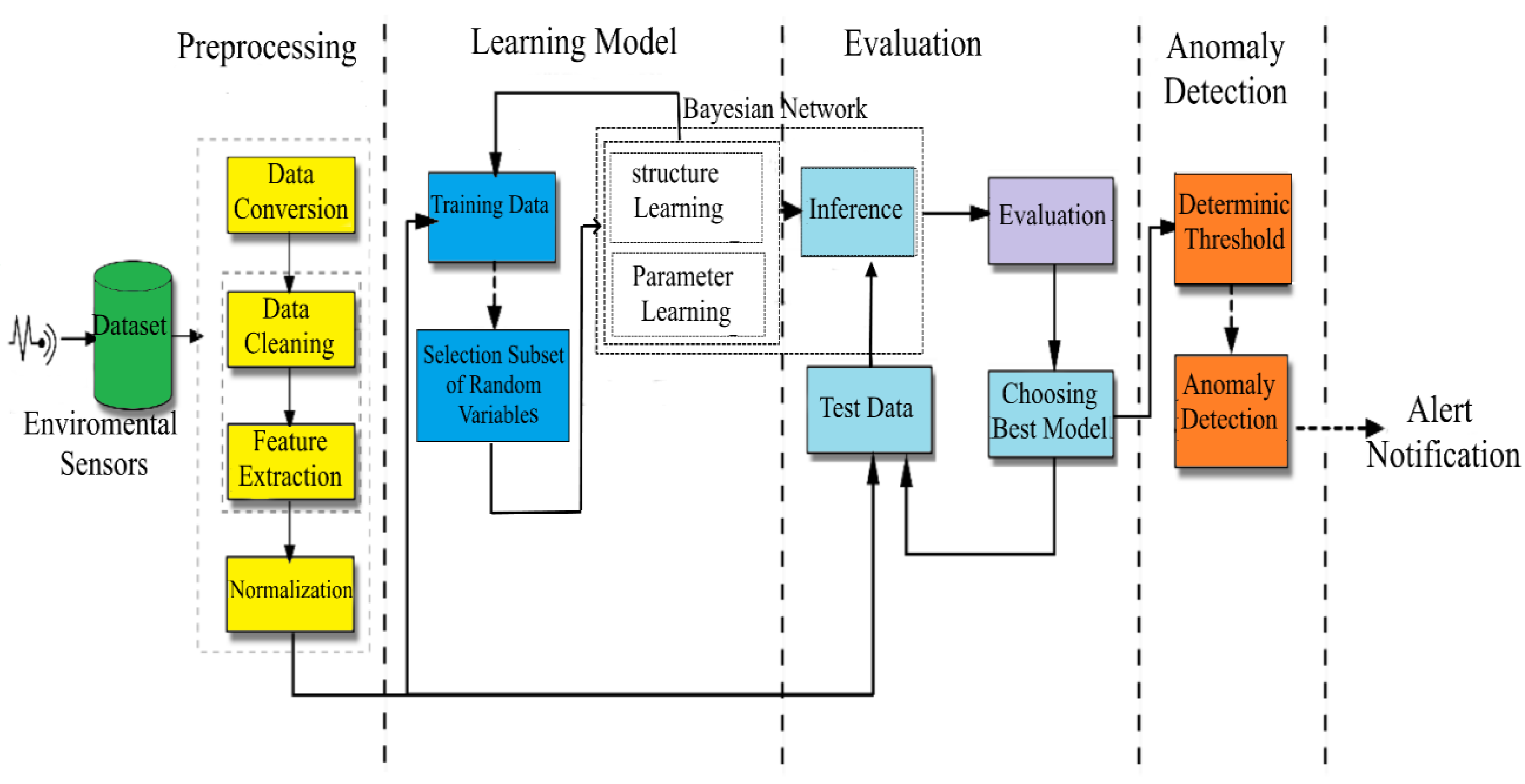
4.4.2. Anomaly Detection Using Bayesian Networks
4.4.3. Anomaly Detection Using a Graph-Based Approach
4.5. AI for Localizing Neural Posture
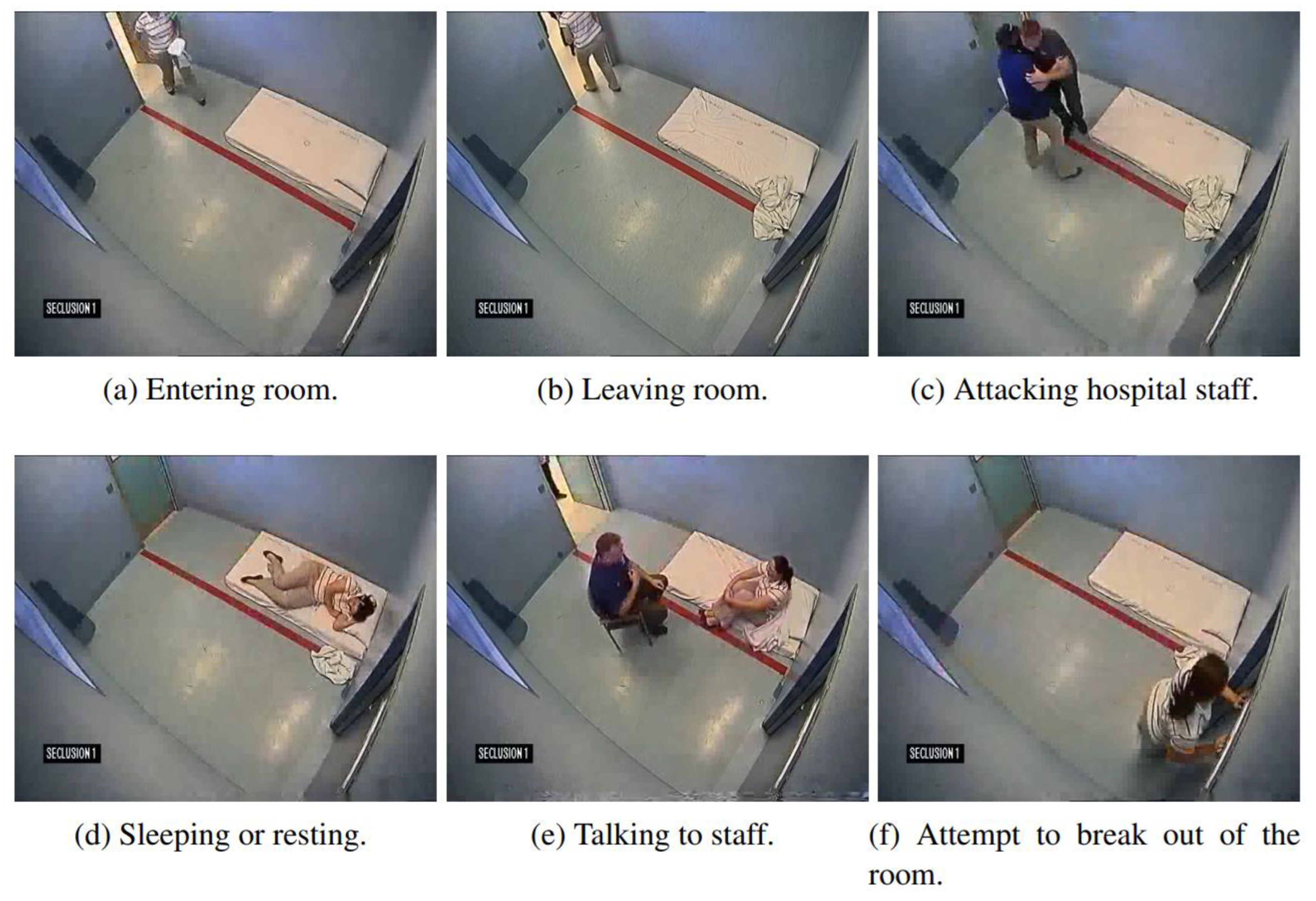
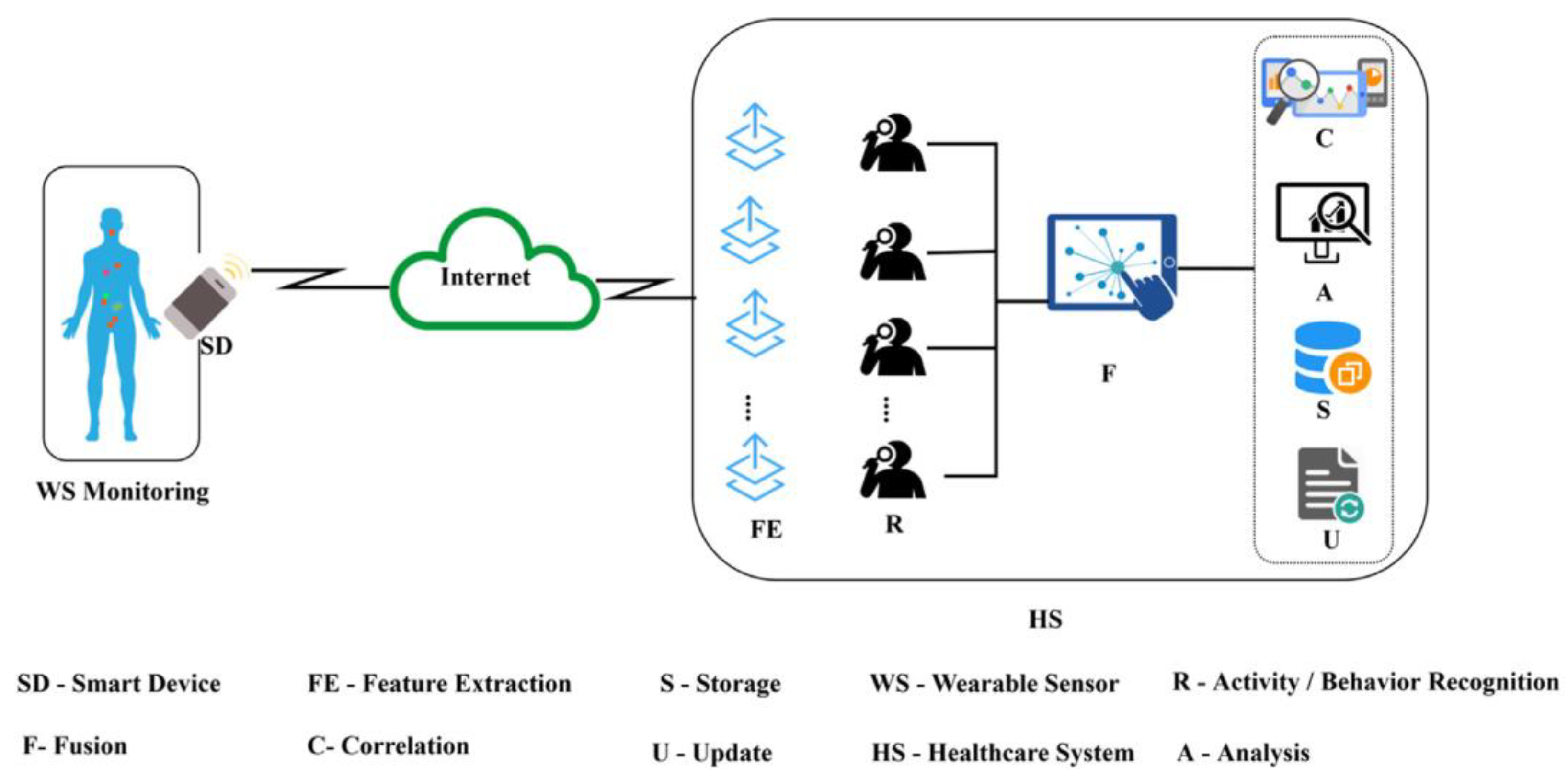
4.6. AI for Monitoring Patients
4.7. AI and Patient’s Lower Limb Movement
4.7.1. Evaluation of Paraplegics’ Legged Mobility
4.7.2. Estimating Clinically of Strokes in Gait Speed Changing
4.7.3. Measuring Parkinson’s Gait Quality
4.8. Remark
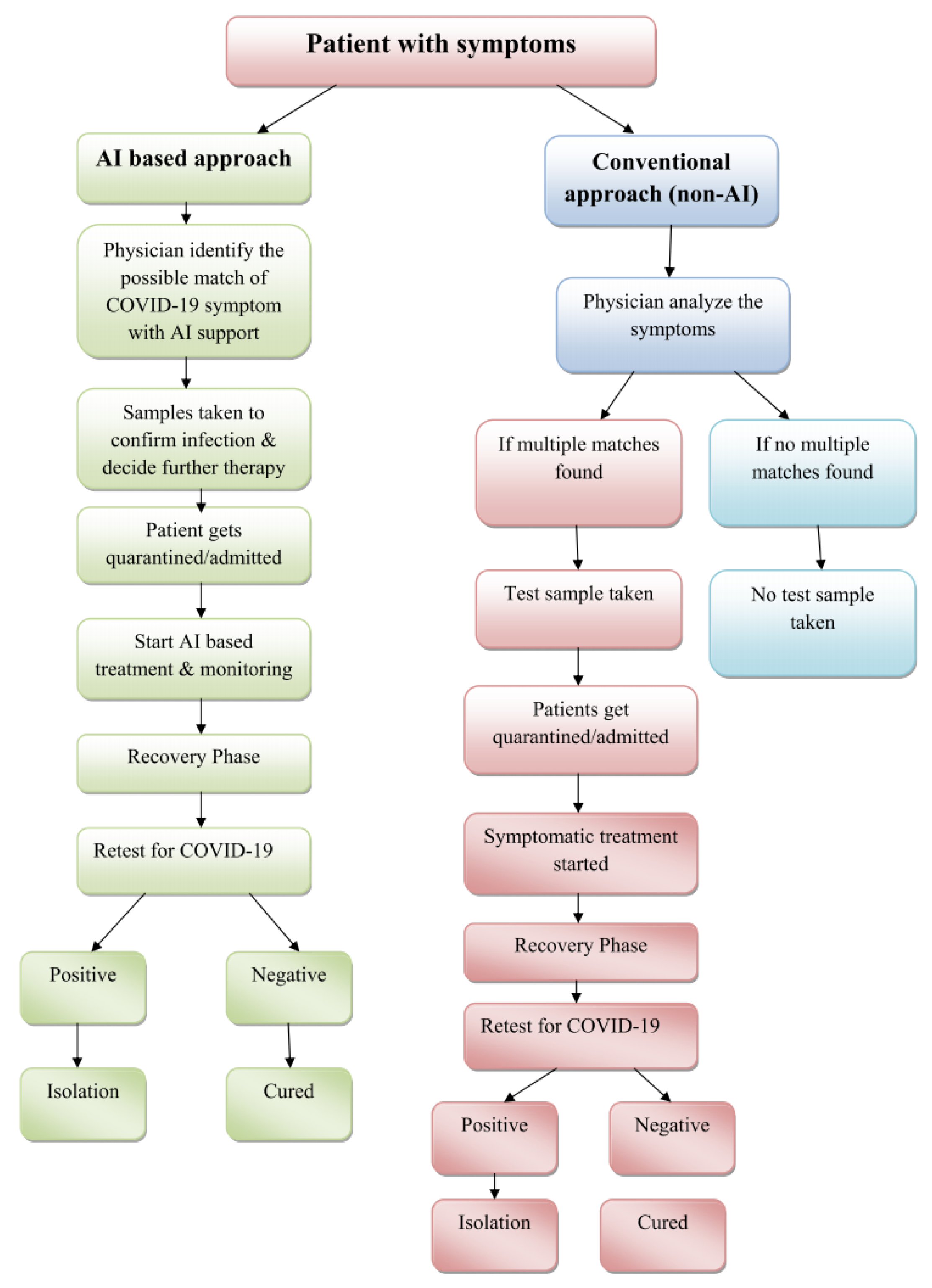
5. AI and COVID-19
5.1. Overview
5.2. AI Training Techniques
5.2.1. Supervised Learning
5.2.2. Unsupervised Learning
5.3. Real World Use Cases
5.3.1. Early Warnings and Alerts
5.3.2. Prediction and Tracking
5.3.3. Data Dashboards
5.3.4. Diagnosis
5.3.5. Faster Cure Discovery
5.3.6. Repurposing Existing Drugs
5.4. AI and Health Care Workers’ Workloads Reduction
5.5. Remark
6. Significance of the Study (Body Language Symptoms for COVID-19)
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iaccino, J. Left Brain—Right Brain Differences: Inquiries, Evidence, and New Approaches, 1st ed.; Psychology Press: London, UK, 2014. [Google Scholar] [CrossRef]
- Ruthrof, H. The Body in Language; Bloomsbury Academic: London, UK, 2015. [Google Scholar] [CrossRef]
- Molchanov, P.; Gupta, S.; Kim, K.; Kautz, J. Hand gesture recognition with 3D convolutional neural networks. In Proceedings of theIEEE Conference on Computer Vision and Pattern Recognition Workshops (CVPRW), Boston, MA, USA, 7–12 June 2015; pp. 1–7. [Google Scholar] [CrossRef]
- Pease, A. Definitive Book of Body Language; Orion Paperbacks: London, UK, 2017. [Google Scholar]
- Wilson, P.A.; Lewandowska-Tomaszczyk, B. Affective Robotics: Modelling and Testing Cultural Prototypes. Cognit. Comput. 2014, 6, 814–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vishwakarma, S.; Agrawal, A. A survey on activity recognition and behavior understanding in video surveillance. Vis. Comput. 2012, 29, 983–1009. [Google Scholar] [CrossRef]
- Hondori, H.M.; Khademi, M. A Review on Technical and Clinical Impact of Microsoft Kinect on Physical Therapy and Rehabilitation. J. Med. Eng. 2014, 2014, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharcanski, J.; Celebi, E. Computer Vision Techniques for the Diagnosis of Skin Cancer, 2014th ed.; Series in BioEngineering; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Kumar, A.; Kumar, S.; Singh, S.; Jha, V. Sign Language Recognition Using Convolutional Neural Network. Lect. Notes Netw. Syst. 2022, 314, 915–922. [Google Scholar] [CrossRef]
- Lueth, J.; Reddy, A.; Garnet, W.; Hankla, D. Systemand Method for Providinga Real-Time Three-Dimiensional Digital Impact Virtual Audience. U.S. Patent 9,462,030, 4 October 2016. [Google Scholar]
- Feichtenhofer, C.; Pinz, A.; Zisserman, A. Convolutional Two-Stream Network Fusion for Video Action Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef] [Green Version]
- Simonyan, K.; Zisserman, A.; Simonyan, K.; Zisserman, A. Two-Stream Convolutional Networks for Action Recognition in Videos. NIPS 2014, 1, 568–576. Available online: https://www.robots.ox.ac.uk/~vgg/publications/2014/Simonyan14b/simonyan14b.pdf (accessed on 20 December 2014).
- Deng, Z.; Vahdat, A.; Hu, H.; Mori, G. Structure Inference Machines: Recurrent Neural Networks for Analyzing Relations in Group Activity Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.S.; Muralidharan, S.; Deng, Z.; Vahdat, A.; Mori, G. A Hierarchical Deep Temporal Model for Group Activity Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef]
- Araujo, R.; Kamel, M.S. A semi-supervised temporal clustering method for facial emotion analysis. In Proceedings of the 2014 IEEE International Conference on Multimedia and Expo Workshops (ICMEW), Chengdu, China, 14–18 July 2014; pp. 1–6. [Google Scholar] [CrossRef]
- Joo, J.; Li, W.; Steen, F.F.; Zhu, S.-C. Visual Persuasion: Inferring Communicative Intents of Images. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition 2014, Columbus, OH, USA, 23–28 June 2014; pp. 216–223. [Google Scholar] [CrossRef] [Green Version]
- Brown, K. Encyclopedia of Language and Linguistics, 2nd ed.; Elsevier Science: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Mast, M.S. On the Importance of Nonverbal Communication in the Physician-Patient Interaction. Available online: https://pubmed.ncbi.nlm.nih.gov/17478072/ (accessed on 2 May 2022).
- Singh, V.P. Language and Body Language; ResearchGate: Berlin, Germany, 2018; p. 2. Available online: https://www.researchgate.net/publication/324246401_Language_and_Body_Language#fullTextFileContent (accessed on 30 November 2022).
- Surkamp, C. Non-Verbal Communication: Why We Need It in Foreign Language Teaching and How We Can Foster It with Drama Activities. Scenar. A J. Performative Teach. Learn. Res. 2014, VIII, 28–43. [Google Scholar] [CrossRef]
- Mandal, F.B. Nonverbal Communication in Humans. J. Hum. Behav. Soc. Environ. 2014, 24, 417–421. [Google Scholar] [CrossRef]
- Uzun, G.Ö. A Review of Communication, Body Language and Communication Conflict. Int. J. Psychosoc. Rehabil. 2020, 24, 9. Available online: https://www.researchgate.net/publication/351057431_A_Review_of_Communication_Body_Language_and_Communication_Conflict#fullTextFileContent (accessed on 30 November 2022).
- Tandon, R. Importance of body language in public speaking. IJISET 2015, 2, 114–120. Available online: http://ijiset.com/vol2/v2s3/IJISET_V2_I3_18.pdf (accessed on 30 November 2022).
- Bambaeeroo, F.; Shokrpour, N. The impact of the teachers’ non-verbal communication on success in teaching. J. Adv. Med. Educ. Prof. 2017, 5, 51–59. [Google Scholar]
- White, J.; Gardner, J. The Classroom X-Factor: The Power of Body Language and Non-Verbal Communication in Teaching, 1st ed.; Routledge: Oxfordshire, UK, 2011. [Google Scholar] [CrossRef]
- Matsumoto, D.; Frank, M.G.; Hwang, H.S. Nonverbal communication: Science and applications. Nonverbal Commun. Sci. Appl. 2012, 1, 1–283. [Google Scholar] [CrossRef] [Green Version]
- Valster, L. Gender differences in nonverbal behaviour of effective leaders: An explorative Study. Bachelor’s Thesis, University of Twente, Enschede, The Netherlands, 2015; pp. 22–26. [Google Scholar]
- Zhi-Peng, R. Body Language in Different Cultures. US-China Foreign Lang. 2014, 12, 1029–1033. [Google Scholar] [CrossRef]
- Soegiono, C.L.; Harti, L.M.S.; Sueb, S. Body Language and Gestures as a Lingua Franca among Multilingual Interlocutors: Multimodal Transcription Study. In Proceedings of the International Joint Conference on Arts and Humanities (IJCAH 2021), Surabaya, Indonesia, 3–4 October 2022. [Google Scholar] [CrossRef]
- Hareli, S.; Hess, U. Facial Expressions and Emotion. Encycl. Personal. Individ. Differ. 2017, 1–7. [Google Scholar] [CrossRef]
- Wolf, K. Measuring facial expression of emotion. Dialogues Clin. Neurosci. 2015, 17, 457–462. [Google Scholar] [CrossRef]
- Kinsbourne, M. Gestures as embodied cognition. Gesture Ritual Mem. 2006, 6, 205–214. [Google Scholar] [CrossRef]
- Carlson, R.A.; Avraamides, M.N.; Cary, M.; Strasberg, S. What do the hands externalize in simple arithmetic? J. Exp. Psychol. Learn. Mem. Cogn. 2007, 33, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Kay, A.; Li, Y.; Cross, W.; Luo, J. Pose-based Body Language Recognition for Emotion and Psychiatric Symptom Interpretation. In Proceedings of the IEEE International Conference on Pattern Recognition (ICPR), Milan, Italy, 10–15 January 2021. [Google Scholar] [CrossRef]
- Beyan, C.; Katsageorgiou, V.-M.; Murino, V. Moving as a Leader. In Proceedings of the 25th ACM International Conference on Multimedia, Mountain View, CA, USA, 23–27 October 2017; pp. 1425–1433. [Google Scholar] [CrossRef]
- Du, H.; Shi, H.; Zeng, D.; Zhang, X.-P.; Mei, T. The Elements of End-to-end Deep Face Recognition: A Survey of Recent Advances. ArXiv arXiv:2009.13290. [CrossRef]
- Napoléon, T.; Alfalou, A. Pose invariant face recognition: 3D model from single photo. Opt. Lasers Eng. 2017, 89, 150–161. [Google Scholar] [CrossRef]
- Vinay, A.; Hebbar, D.; Shekhar, V.S.; Murthy, K.N.B.; Natarajan, S. Two Novel Detector-Descriptor Based Approaches for Face Recognition Using SIFT and SURF. Procedia Comput. Sci. 2015, 70, 185–197. [Google Scholar] [CrossRef] [Green Version]
- Kortli, Y.; Jridi, M.; al Falou, A.; Atri, M. Face Recognition Systems: A Survey. Sensors 2020, 20, 342. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Wang, X.A. Cascade classifier for face detection. J. Algorithm. Comput. Technol. 2016, 10, 187–197. [Google Scholar] [CrossRef] [Green Version]
- Ranjan, A.; Jampani, V.; Balles, L.; Kim, K.; Sun, D.; Wulff, J.; Black, M.J. Competitive Collaboration: Joint Unsupervised Learning of Depth, Camera Motion, Optical Flow and Motion Segmentation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019. [Google Scholar] [CrossRef]
- Kortli, Y.; Jridi, M.; al Falou, A.; Atri, M. A novel face detection approach using local binary pattern histogram and support vector machine. In Proceedings of the International Conference on Advanced Systems and Emergent Technologies, Hammamet, Tunisia, 22–25 March 2018; pp. 28–33. [Google Scholar] [CrossRef]
- Annalakshmi, M.; Roomi, S.M.M.; Naveedh, A.S. A hybrid technique for gender classification with SLBP and HOG features. Cluster Comput. 2018, 22, 11–20. [Google Scholar] [CrossRef]
- Wang, Q.; Alfalou, A.; Brosseau, C. New perspectives in face correlation research: A tutorial. Adv. Opt. Photonics 2017, 9, 1–78. [Google Scholar] [CrossRef]
- Molchanov, P.; Yang, X.; Gupta, S.; Kim, K.; Tyree, S.; Kautz, J. Online Detection and Classification of Dynamic Hand Gestures with Recurrent 3D Convolutional Neural Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef]
- Schroff, F.; Kalenichenko, D.; Philbin, J. FaceNet: A unified embedding for face recognition and clustering. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 815–823. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, S. Discussion of “An epidemiological forecast model and software assessing interventions on the COVID-19 epidemic in China”. J. Data Sci. 2021, 18, 437. [Google Scholar] [CrossRef]
- John, V.; Boyali, A.; Mita, S.; Imanishi, M.; Sanma, N. Deep Learning-Based Fast Hand Gesture Recognition Using Representative Frames. In Proceedings of the International Conference on Digital Image Computing: Techniques and Applications (DICTA), Gold Coast, QLD, Australia, 30 November–2 December 2016; pp. 1–8. [Google Scholar] [CrossRef]
- Boukamcha, H.; Hallek, M.; Smach, F.; Atri, M. Automatic landmark detection and 3D Face data extraction. J. Comput. Sci. 2017, 21, 340–348. [Google Scholar] [CrossRef]
- Mian, A.; Bennamoun, M.; Owens, R. An Efficient Multimodal 2D-3D Hybrid Approach to Automatic Face Recognition. IEEE Trans. Pattern Anal. Mach. Intell. 2007, 29, 1927–1943. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Wang, Z.; Liu, X.; Zeng, N.; Liu, Y.; Alsaadi, F.E. A survey of deep neural network architectures and their applications. Neurocomputing 2017, 234, 11–26. [Google Scholar] [CrossRef]
- Koshy, R.; Mahmood, A. Optimizing Deep CNN Architectures for Face Liveness Detection. Entropy 2019, 21, 423. [Google Scholar] [CrossRef] [Green Version]
- Jain, A.; Tompson, J.; Andriluka, M.; Bregler, C. Learning Human Pose Estimation Features with Convolutional Networks. Arxiv 2014. [Google Scholar] [CrossRef]
- Li, S.; Liu, Z.-Q.; Chan, A.B. Heterogeneous Multi-task Learning for Human Pose Estimation with Deep Convolutional Neural Network. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 23–28 June 2014; 113, pp. 19–36. [Google Scholar] [CrossRef] [Green Version]
- Neverova, N.; Wolf, C.; Taylor, G.W.; Nebout, F. Hand Segmentation with Structured Convolutional Learning. Comput. Vis. ACCV 2015, 2014, 687–702. [Google Scholar] [CrossRef] [Green Version]
- Oyedotun, O.K.; Khashman, A. Deep learning in vision-based static hand gesture recognition. Neural Comput. Appl. 2016, 28, 3941–3951. [Google Scholar] [CrossRef]
- Liang, C.; Song, Y.; Zhang, Y. Hand gesture recognition using view projection from point cloud. In Proceedings of the IEEE International Conference on Image Processing, Phoenix, AZ, USA, 25–28 September 2016; pp. 4413–4417. [Google Scholar] [CrossRef]
- Lin, H.-I.; Hsu, M.-H.; Chen, W.-K. Human hand gesture recognition using a convolution neural network. In Proceedings of the IEEE International Conference on Automation Science and Engineering (CASE), New Taipei, Taiwan, 8–22 August 2014; pp. 1038–1043. [Google Scholar] [CrossRef]
- Tompson, J.; Stein, M.; Lecun, Y.; Perlin, K. Real-Time Continuous Pose Recovery of Human Hands Using Convolutional Networks. ACM Trans. Graph. 2014, 33, 1–10. [Google Scholar] [CrossRef]
- Wu, J.; Ishwar, P.; Konrad, J. Two-Stream CNNs for Gesture-Based Verification and Identification: Learning User Style. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 1–26 June 2016. [Google Scholar] [CrossRef]
- Jain, A.; Tompson, J.; LeCun, Y.; Bregler, C. MoDeep: A Deep Learning Framework Using Motion Features for Human Pose Estimation. Comput. Vis.-ACCV 2015, 2014, 302–315. [Google Scholar] [CrossRef]
- Huang, J.; Zhou, W.; Li, H.; Li, W. Sign Language Recognition using 3D convolutional neural networks. In Proceedings of the IEEE International Conference on Multimedia and Expo, Turin, Italy, 29 June–3 July 2015. [Google Scholar] [CrossRef]
- Li, Y.; Miao, Q.; Tian, K.; Fan, Y.; Xu, X.; Li, R.; Song, J. Large-Scale Gesture Recognition with a Fusion of RGB-D Data Based on Saliency Theory and C3D Model. IEEE Trans. Circuits Syst. Video Technol. 2018, 28, 2956–2964. [Google Scholar] [CrossRef]
- Camgoz, N.C.; Hadfield, S.; Koller, O.; Bowden, R. Using Convolutional 3D Neural Networks for User-independent continuous gesture recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef] [Green Version]
- Neverova, N.; Wolf, C.; Paci, G.; Sommavilla, G.; Taylor, G.W.; Nebout, F. A Multi-scale Approach to Gesture Detection and Recognition. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Sydney, Australia, 2–8 December 2013; pp. 484–491. [Google Scholar] [CrossRef]
- Tran, D.; Bourdev, L.; Fergus, R.; Torresani, L.; Paluri, M. Learning Spatiotemporal Features with 3D Convolutional Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 4489–4497. [Google Scholar] [CrossRef] [Green Version]
- Chai, X.; Liu, Z.; Yin, F.; Liu, Z.; Chen, X. Two streams Recurrent Neural Networks for Large-Scale Continuous Gesture Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar] [CrossRef]
- Eleni, T. Gesture Recognition with a Convolutional Long Short Term Memory Recurrent Neural Network. In Proceedings of the ESANN 2015, Bruges, Belgium, 22–23 April 2015; Available online: https://books.google.cl/books?id=E8qMjwEACAAJ. (accessed on 30 November 2022).
- Nishida, N.; Nakayama, H. Multimodal Gesture Recognition Using Multi-stream Recurrent Neural Network. Image Video Technol. 2016, 9431, 682–694. [Google Scholar] [CrossRef]
- Koller, O.; Ney, H.; Bowden, R. Deep Hand: How to Train a CNN on 1 Million Hand Images When Your Data is Continuous and Weakly Labelled. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 3793–3802. [Google Scholar] [CrossRef] [Green Version]
- Hamm, J.; Kohler, C.G.; Gur, R.C.; Verma, R. Automated Facial Action Coding System for dynamic analysis of facial expressions in neuropsychiatric disorders. J. Neurosci. Methods 2011, 200, 237–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- haq, I.; Jalil, A. Real-Time Gait Analysis Algorithm for Patient Activity Detection to Understand and Respond to the Movements. School of Computing, Blekinge Institute of Technology, SE – 371 79 Karlskrona, Sweden. 2012. Available online: http://www.diva-portal.org/smash/get/diva2:829264/FULLTEXT01 (accessed on 30 November 2022).
- Ajerla, D.; Mahfuz, S.; Zulkernine, F. A Real-Time Patient Monitoring Framework for Fall Detection. Wirel. Commun. Mob. Comput. 2019, 2019, 1–13. [Google Scholar] [CrossRef]
- Bhowmik, P.; Pantho, M.J.H.; Bobda, C. HARP: Hierarchical Attention Oriented Region-Based Processing for High-Performance Computation in Vision Sensor. Sensors 2021, 21, 1757. [Google Scholar] [CrossRef]
- Saqaeeyan, S.; Amirkhani, H.; Javadi, H. Anomaly Detection in Smart Homes Using Bayesian Networks. KSII Trans. Internet Inf. Syst. 2020, 14, 1796–1813. [Google Scholar] [CrossRef]
- Moallem, M.; Hassanpour, H.; Pouyan, A.; Moallem, M.; Hassanpour, H.; Pouyan, A. Anomaly Detection in Smart Homes Using Deep Learning. Iran. J. Energy Environ. 2019, 10, 126–135. [Google Scholar] [CrossRef]
- Horný, M. Bayesian Networks. 2014. Available online: https://www.bu.edu/sph/files/2014/05/bayesian-networks-final.pdf (accessed on 30 November 2022).
- Paudel, R.; Eberle, W.; Holder, L. Anomaly Detection of Elderly Patient Activities in Smart Homes Using a Graph-Based Approach; ICDATA’18; CSREA Press: Providence, RI, USA, 2018; pp. 163–169. [Google Scholar]
- Luštrek, M.; Kaluža, B. Fall Detection and Activity Recognition with Machine Learning. Informatica 2009, 33, 205–212. Available online: https://www.academia.edu/552485/Fall_detection_and_activity_recognition_with_machine_learning (accessed on 30 November 2022).
- Roh, J.; Park, H.; Lee, K.; Hyeong, J.; Kim, S.; Lee, B. Sitting Posture Monitoring System Based on a Low-Cost Load Cell Using Machine Learning. Sensors 2018, 18, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matar, G.; Lina, J.-M.; Kaddoum, G. Artificial Neural Network for in-Bed Posture Classification Using Bed-Sheet Pressure Sensors. IEEE J. Biomed. Heal. Inform. 2020, 24, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.; Kim, K.H.; Song, C.; Lee, I.; Lee, K.; Kang, J.; Kang, Y.K. Electrodiagnosis support system for localizing neural injury in an upper limb. J. Am. Med. Inform. Assoc. 2010, 17, 345–347. [Google Scholar] [CrossRef] [Green Version]
- Borges, P.; Nourani-Vatani, N. Vision-based detection of unusual patient activity. Stud. Health Technol. Inf. 2011, 168, 16–23. [Google Scholar]
- Tolba, A.; Said, O.; Al-Makhadmeh, Z. MDS: Multi-level decision system for patient behavior analysis based on wearable device information. Comput. Commun. 2019, 147, 180–187. [Google Scholar] [CrossRef]
- Pirouz, B.; Haghshenas, S.S.; Haghshenas, S.S.; Piro, P. Investigating a Serious Challenge in the Sustainable Development Process: Analysis of Confirmed cases of COVID-19 (New Type of Coronavirus) through a Binary Classification Using Artificial Intelligence and Regression Analysis. Sustainability 2020, 12, 2427. [Google Scholar] [CrossRef] [Green Version]
- Farris, R.J.; Quintero, H.A.; Murray, S.A.; Ha, K.H.; Hartigan, C.; Goldfarb, M. A Preliminary Assessment of Legged Mobility Provided by a Lower Limb Exoskeleton for Persons with Paraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Fulk, G.D.; Ludwig, M.; Dunning, K.; Golden, S.; Boyne, P.; West, T. Estimating Clinically Important Change in Gait Speed in People with Stroke Undergoing Outpatient Rehabilitation. J. Neurol. Phys. Ther. 2011, 35, 82–89. [Google Scholar] [CrossRef]
- Mileti, I.; Germanotta, M.; di Sipio, E.; Imbimbo, I.; Pacilli, A.; Erra, C.; Petracca, M.; Rossi, S.; del Prete, Z.; Bentivoglio, A.; et al. Measuring Gait Quality in Parkinson’s Disease through Real-Time Gait Phase Recognition. Sensors 2018, 18, 919. [Google Scholar] [CrossRef] [Green Version]
- Horak, F.; King, L.; Mancini, M. Role of Body-Worn Movement Monitor Technology for Balance and Gait Rehabilitation. Phys. Ther. 2015, 95, 461–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaishya, R.; Javaid, M.; Khan, I.H.; Haleem, A. Artificial Intelligence (AI) applications for COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017. [Google Scholar] [CrossRef] [Green Version]
- Bank, D.; Koenigstein, N.; Giryes, R. Autoencoders. ArXiv 2020. [Google Scholar] [CrossRef]
- Mannor, S.; Jin, X.; Han, J.; Jin, X.; Han, J.; Jin, X.; Zhang, X. K-Means Clustering. In Encyclopedia of Machine Learning; Springer: New York, NY, USA, 2011; pp. 563–564. [Google Scholar] [CrossRef]
- Browning, P.; Siegel, E.; Greenspan, H.; Gozes, O.; Zhang, H.; Frid-Adar, M.; Ji, W.; Bernheim, A. Rapid AI Development Cycle for the Coronavirus (COVID-19) Pandemic: Initial Results for Automated Detection & Patient Monitoring using Deep Learning CT Image Analysis. ArXiv 2020. Available online: https://arxiv.org/abs/2003.05037 (accessed on 30 November 2022).
- Zhu, A.Z.; Yuan, L.; Chaney, K.; Daniilidis, K. Live Demonstration: Unsupervised Event-Based Learning of Optical Flow, Depth and Egomotion. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 16–17 June 2019. [Google Scholar] [CrossRef]
- Naudé, W. Artificial Intelligence Against Covid-19: An Early Review. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- BlueDot. BlueDot: Outbreak Intelligence Platform. 2021. Available online: https://bluedot.global/ (accessed on 30 November 2022).
- Bogoch, I.I.; Watts, A.; Thomas-Bachli, A.; Huber, C.; Kraemer, M.U.G.; Khan, K. Pneumonia of unknown aetiology in Wuhan, China: Potential for international spread via commercial air travel. J. Travel Med. 2020, 27, 2. [Google Scholar] [CrossRef]
- About. The Disease Daily. 2022. Available online: https://www.diseasedaily.org/about/ (accessed on 30 November 2022).
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet Infect. Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Akhtar, M.; Kraemer, M.U.G.; Gardner, L.M. A dynamic neural network model for predicting risk of Zika in real time. BMC Med. 2019, 17, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Lazer, D.; Kennedy, R.; King, G.; Vespignani, A. The Parable of Google Flu: Traps in Big Data Analysis. Science 2014, 343, 1203–1205. [Google Scholar] [CrossRef]
- GLEAMviz.org. 2021. Available online: http://www.gleamviz.org/ (accessed on 30 November 2022).
- Home|Metabiota. 2020. Available online: https://www.metabiota.com/ (accessed on 30 November 2022).
- Crawford, T. Oxford Mathematician Explains SIR Disease Model for COVID-19 (Coronavirus). 2020. Available online: https://www.youtube.com/watch?v=NKMHhm2Zbkw (accessed on 30 November 2022).
- Maier, B.F.; Brockmann, D. Effective containment explains subexponential growth in recent confirmed COVID-19 cases in China. Science 2020, 368, 742–746. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Zhou, Y.; He, J.; Zhu, B.; Wang, F.; Tang, L.; Kleinsasser, M.; Barker, D.; Eisenberg, M.C.; Song, P.X.K. Rejoinder: An epidemiological forecast model and software assessing interventions on COVID-19 epidemic in China. J. Data Sci. 2021, 18, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Patel, N. The Best, and the Worst, of the Coronavirus Dashboards. 2020. Available online: https://www.technologyreview.com/2020/03/06/905436/best-worst-coronavirus-dashboards/ (accessed on 30 November 2022).
- TABLEAU. COVID 19 ZA Dashboard, Atlassian Statuspage. 2021. Available online: https://datastudio.google.com/u/0/reporting/1b60bdc7-bec7-44c9-ba29-be0e043d8534/page/hrUIB (accessed on 30 November 2022).
- Data, World Coronavirus (COVID-19) Data Resource Hub. 2020. Available online: https://data.world/resources/coronavirus/%0A (accessed on 30 November 2022).
- Bullock, J.; Luccioni, A.; Pham, K.H.; Lam, C.S.N.; Luengo-Oroz, M. Mapping the landscape of Artificial Intelligence applications against COVID-19. J. Artif. Intell. Res. 2020, 69, 807–845. [Google Scholar] [CrossRef]
- Rosebrock, A. Detecting COVID-19 in X-Ray Images with Keras, TensorFlow, and Deep Learning, PyImageSearch. 2020. Available online: https://www.pyimagesearch.com/2020/03/16/detecting-covid-19-in-x-ray-images-with-keras-tensorflow-and-deep-learning/ (accessed on 30 November 2022).
- Maghded, H.S.; Ghafoor, K.Z.; Sadiq, A.S.; Curran, K.; Rawat, D.B.; Rabie, K. A Novel AI-enabled Framework to Diagnose Coronavirus COVID-19 using Smartphone Embedded Sensors: Design Study. In Proceedings of the IEEE International Conference on Information Reuse and Integration for Data Science, Las Vegas, NV, USA, 11–13 August 2020; pp. 180–187. [Google Scholar] [CrossRef]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef] [PubMed]
- Rawat, W.; Wang, Z. Deep Convolutional Neural Networks for Image Classification: A Comprehensive Review. Neural Comput. 2017, 29, 2352–2449. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wu, L.; Zhang, J.; Zhang, L.; Gong, D.; Zhao, Y.; Hu, S.; Wang, Y.; Hu, X.; Zheng, B.; et al. Deep learning-based model for detecting 2019 novel coronavirus pneumonia on high-resolution computed tomography: A prospective study. MedRxiv 2020. [Google Scholar] [CrossRef]
- Imaging Technologies News. Artificial Intelligence Assisted Radiology Technologies Aid COVID-19 Fight in China; ITN Online: Lincolnshire, IL, USA, 2020; Available online: https://www.itnonline.com/article/artificial-intelligence-assisted-radiology-technologies-aid-covid-19-fight-china (accessed on 30 November 2022).
- Yan, L.; Zhang, H.-T.; Goncalves, J.; Xiao, Y.; Wang, M.; Guo, Y.; Sun, C.; Tang, X.; Jin, L.; Zhang, M.; et al. A machine learning-based model for survival prediction in patients with severe COVID-19 infection. Medrxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Coffee, M.; Bari, A.; Wang, J.; Jiang, X.; Huang, J.; Shi, J.; Dai, J.; Cai, J.; Zhang, T.; et al. Towards an artificial intelligence framework for data-driven prediction of coronavirus clinical severity. Comput. Mater. Contin. 2020, 63, 537–551. [Google Scholar] [CrossRef]
- Segler, M.H.S.; Preuss, M.; Waller, M.P. Planning chemical syntheses with deep neural networks and symbolic AI. Nature 2018, 555, 604–610. [Google Scholar] [CrossRef] [Green Version]
- Silver, D.; Hubert, T.; Schrittwieser, J.; Antonoglou, I.; Lai, M.; Guez, A.; Lanctot, M.; Sifre, L.; Kumaran, D.; Graepel, T.; et al. A general reinforcement learning algorithm that masters chess, shogi, and Go through self-play. Science 2018, 362, 1140–1144. [Google Scholar] [CrossRef] [Green Version]
- Beck, B.R.; Shin, B.; Choi, Y.; Park, S.; Kang, K. Predicting commercially available antiviral drugs that may act on the novel coronavirus (2019-nCoV), Wuhan, China through a drug-target interaction deep learning model. BioRexiv 2020. [Google Scholar] [CrossRef]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Bobdey, S.; Ray, S. Going viral—Covid-19 impact assessment: A perspective beyond clinical practice. J. Mar. Med. Soc. 2020, 22, 9. [Google Scholar] [CrossRef]
- Gupta, R.; Misra, A. Contentious issues and evolving concepts in the clinical presentation and management of patients with COVID-19 infectionwith reference to use of therapeutic and other drugs used in Co-morbid diseases (Hypertension, diabetes etc). Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Chahal, K.K. How Your Body Language Affects Patient Care. Curr. Psychiatr. 2017, 42, 41–42. [Google Scholar]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdulghafor, R.; Abdelmohsen, A.; Turaev, S.; Ali, M.A.H.; Wani, S. An Analysis of Body Language of Patients Using Artificial Intelligence. Healthcare 2022, 10, 2504. https://doi.org/10.3390/healthcare10122504
Abdulghafor R, Abdelmohsen A, Turaev S, Ali MAH, Wani S. An Analysis of Body Language of Patients Using Artificial Intelligence. Healthcare. 2022; 10(12):2504. https://doi.org/10.3390/healthcare10122504
Chicago/Turabian StyleAbdulghafor, Rawad, Abdelrahman Abdelmohsen, Sherzod Turaev, Mohammed A. H. Ali, and Sharyar Wani. 2022. "An Analysis of Body Language of Patients Using Artificial Intelligence" Healthcare 10, no. 12: 2504. https://doi.org/10.3390/healthcare10122504