

Dental Prosthetic Rehabilitation Interventions in Elderly Patients Hospitalized in the Nursing Homes of the Lombardy Region: A Retrospective Study
 ,
,
Abstract
:1. Introduction
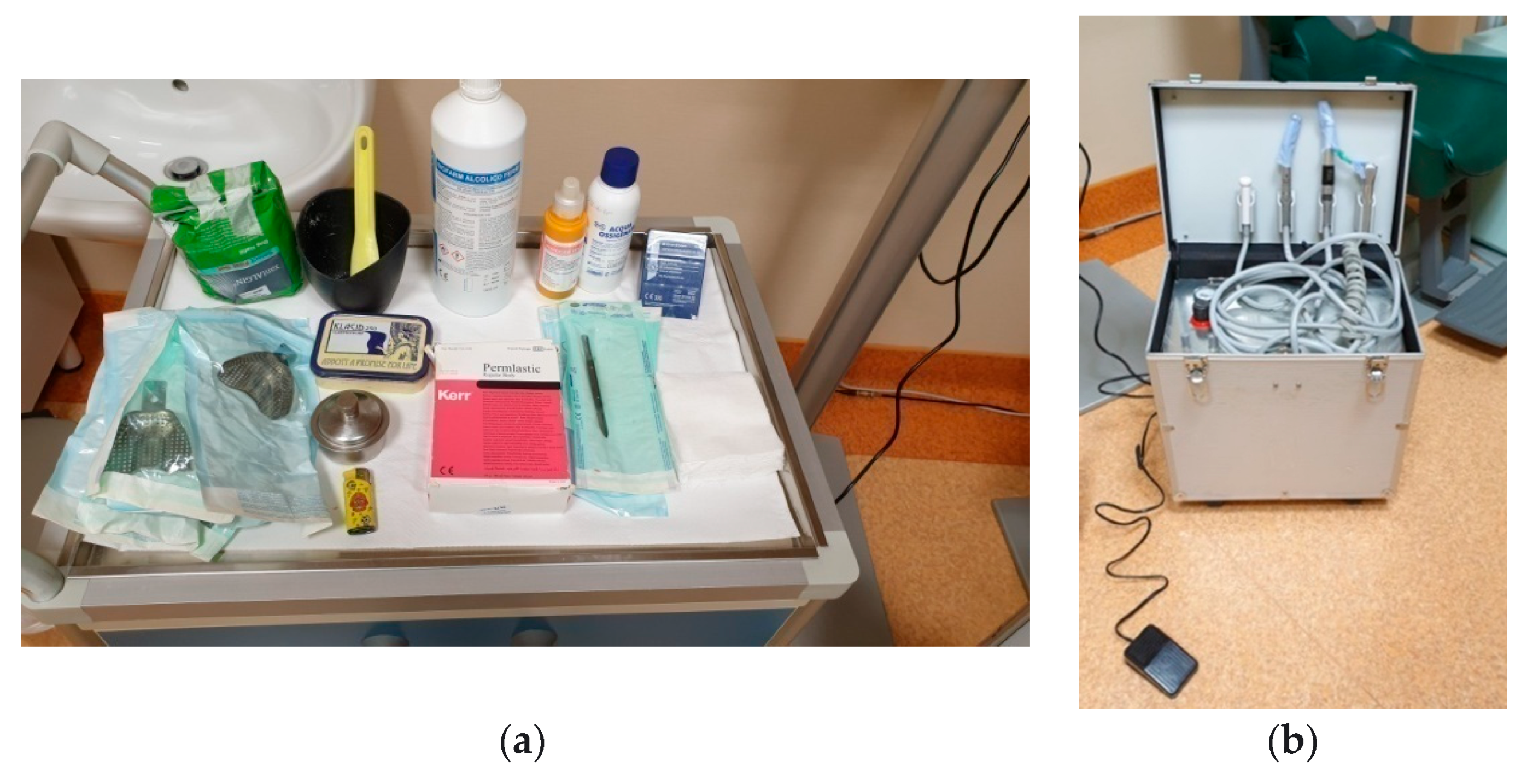
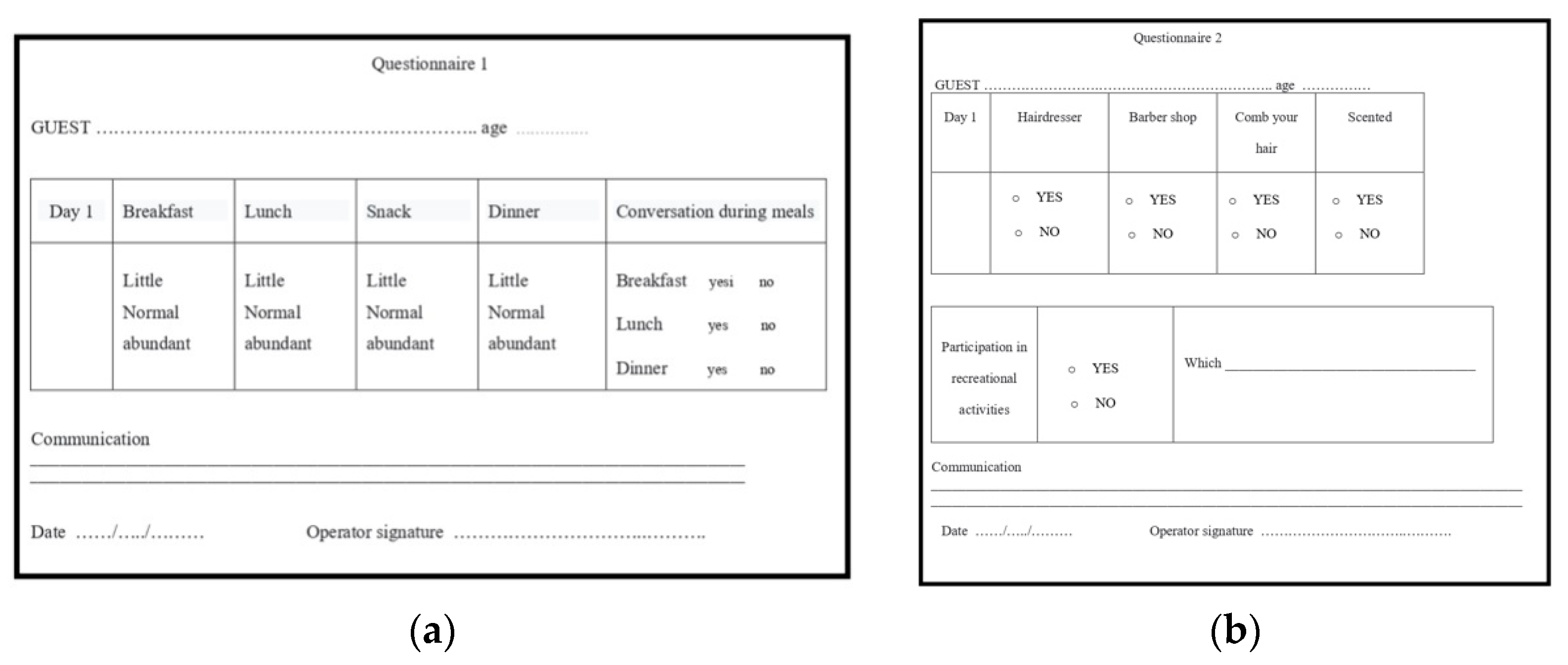
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Nascimento, C.M.; Ingles, M.; Salvador-Pascual, A.; Cominetti, M.R.; Gomez-Cabrera, M.C.; Viña, J. Sarcopenia, frailty and their prevention by exercise. Free Radic. Biol. Med. 2019, 132, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Erdinçler, D.S.; Avcı, S. Kardiyovaskülerhastalığıolanyaşlıdabeslenme [Nutrition in elderly patients with cardiovascular diseases]. Turk Kardiyol. Dern. Ars. 2017, 45 (Suppl. 5), 113–116. (In Turkish) [Google Scholar] [CrossRef] [PubMed]
- Bahat, G.; Tufan, F.; Bahat, Z.; Tufan, A.; Aydin, Y.; Akpinar, T.S.; Nadir, S.; Erten, N.; Karan, M.A. Comorbidities, polypharmacy, functionality and nutritional status in Turkish community-dwelling female elderly. Aging Clin. Exp. Res. 2014, 26, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Okada, K.; Kondo, M.; Matsushita, T.; Nakazawa, S.; Yamazaki, Y. Oral health for achieving longevity. Geriatr. Gerontol. Int. 2020, 20, 526–538. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Iinuma, T.; Sato, S. Relationship between the oral cavity and respiratory diseases: Aspiration of oral bacteria possibly contributes to the progression of lower airway inflammation. Jpn. Dent. Sci. Rev. 2021, 57, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Azzolino, D.; Passarelli, P.C.; de Angelis, P.; Piccirillo, G.B.; D’Addona, A.; Cesari, M. Poor Oral Health as a Determinant of Malnutrition and Sarcopenia. Nutrients 2019, 11, 2898. [Google Scholar] [CrossRef] [Green Version]
- De Sire, A.; Ferrillo, M.; Lippi, L.; Agostini, F.; de Sire, R.; Ferrara, P.E.; Raguso, G.; Riso, S.; Roccuzzo, A.; Ronconi, G.; et al. Sarcopenic Dysphagia, Malnutrition, and Oral Frailty in Elderly: A Comprehensive Review. Nutrients 2022, 14, 982. [Google Scholar] [CrossRef]
- Ceraulo, S.; Caccianiga, P.; Casto, C.; Baldoni, M.; Caccianiga, G. COVID-19 and Prosthetic Emergencies, Home Care in Fragile Patients: A Case Report. Healthcare 2022, 10, 1407. [Google Scholar] [CrossRef]
- Pan, Y.; Liu, H.; Chu, C.; Li, X.; Liu, S.; Lu, S. Transmission routes of SARS-CoV-2 and protective measures in dental clinics during the COVID-19 pandemic. Am. J. Dent. 2020, 33, 129–134. [Google Scholar]
- Ceraulo, S.; Lauritano, D.; Caccianiga, G.; Baldoni, M. Reduce the spread of COVID-19 within the dental practice: The era of single use. Minerva Stomatol. 2020. epub ahead of print. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef]
- Manresa, C.; Sanz-Miralles, E.C.; Twigg, J.; Bravo, M. Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst. Rev. 2018, 1, CD009376. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Laser Management of Peri-Implantitis: A Comparison between Photodynamic Therapy Combined with Hydrogen Peroxide (OHLLT) and OHLLT + Er:YAG Laser. A Retrospective Controlled Study. Appl. Sci. 2021, 11, 6771. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Caccianiga, P.; Baldoni, A.; Ceraulo, S. Periodontal Decontamination Induced by Light and Not by Heat: Comparison between Oxygen High Level Laser Therapy (OHLLT) and LANAP. Appl. Sci. 2021, 11, 4629. [Google Scholar] [CrossRef]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition Management in Older Adults with Diabetes: A Review on the Importance of Shifting Prevention Strategies from Metabolic Syndrome to Frailty. Nutrients 2020, 12, 3367. [Google Scholar] [CrossRef]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- Khanagar, S.B.; Al-Ehaideb, A.; Shivanna, M.M.; UlHaq, I.; Al Kheraif, A.A.; Naik, S.; Maganur, P.; Vishwanathaiah, S. Age-related Oral Changes and Their Impact on Oral Health-related Quality of Life among Frail Elderly Population: A Review. J. Contemp. Dent. Pract. 2020, 21, 1298–1303. [Google Scholar]
- Lauritano, D.; Moreo, G.; Carinci, F.; Borgia, R.; Lucchese, A.; Contaldo, M.; Della Vella, F.; Bernardelli, P.; Moreo, G.; Petruzzi, M. Aging and Oral Care: An Observational Study of Characteristics and Prevalence of Oral Diseases in an Italian Cohort. Int. J. Environ. Res. Public Health 2019, 16, 3763. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Clark, J.J.J.; Naorungroj, S. Oral health in nursing home residents with different cognitive statuses. Gerodontology 2013, 30, 49–60. [Google Scholar] [CrossRef]
- Lauritano, D.; Moreo, G.; Della Vella, F.; Di Stasio, D.; Carinci, F.; Lucchese, A.; Petruzzi, M. Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4558. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Sabbah, W. Association between number of teeth, use of dentures and musculoskeletal frailty among older adults. Geriatr. Gerontol. Int. 2018, 18, 592–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suma, S.; Furuta, M.; Takeuchi, K.; Tomioka, M.; Iwasa, Y.; Yamashita, Y. Number of teeth, denture wearing and cognitive function in relation to nutritional status in residents of nursing homes. Gerodontology 2022, 39, 197–203. [Google Scholar] [CrossRef] [PubMed]
- da Rosa, R.S.; Garcia, R.C.; Cury, A.A.; Faot, F. Management of the oral manifestations of senile purpura in an edentulous patient: A case report. Spec. Care Dentist. 2011, 31, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Radwan-Oczko, M.; Bandosz, K.; Rojek, Z.; Owczarek-Drabińska, J.E. Clinical Study of Oral Mucosal Lesions in the Elderly-Prevalence and Distribution. Int. J. Environ. Res. Public Health 2022, 19, 2853. [Google Scholar] [CrossRef]
- Vasilyeva, D.; Lee, K.C.; Alex, G.; Peters, S.M. Painful palatal lesion in a 90-year-old female. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 626–630. [Google Scholar] [CrossRef]
- Azzolino, D.; Marzetti, E.; Proietti, M.; Calvani, R.; de Souto Barreto, P.; Rolland, Y.; Cesari, M. Lack of energy is associated with malnutrition in nursing home residents: Results from the INCUR study. J. Am. Geriatr. Soc. 2021, 69, 3242–3248. [Google Scholar] [CrossRef]
- Damanti, S.; de Souto Barreto, P.; Rolland, Y.; Astrone, P.; Cesari, M. Malnutrition and physical performance in nursing home residents: Results from the INCUR study. Aging Clin. Exp. Res. 2021, 33, 2299–2303. [Google Scholar] [CrossRef]
- Duray-Parmentier, C.; Lafontaine, J.B.; Nielens, N.; Janne, P.; Gourdin, M. Aspect médico-psychologiquerelatif à l’épidémie du coronavirus: Mise en place d’unestratégie de soutien pour le personnel soignant par les médecinscoordinateurs dans les maisons de repos et de soinsen Belgique ouEhpaden France et impact psychologique pour les résidents de cesmaisons de repos et de soinsprivées et publiques [Medico-psychological aspect relating to the coronavirus epidemic: Implementation of a support strategy for nursing staff by coordinating doctors in rest and care homes in Belgium and in France and psychological impact for the residents of these private and public nursing and care homes]. Geriatr. Psychol. Neuropsychiatr. Vieil. 2021, 19, 359–365 (In French). [Google Scholar] [CrossRef]
- Duray-Parmentier, C.; Lafontaine, J.B.; Nielens, N.; Janne, P.; Gourdin, M. Psychological impact of COVID-19 lockdown on staff and residents of nursing and care homes in Belgium and EHPADs France. Geriatr. Psychol. Neuropsychiatr. Vieil. 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Feng, X.; Todd, T.; Lintzenich, C.R.; Ding, J.; Carr, J.J.; Ge, Y.; Browne, J.D.; Kritchevsky, S.B.; Butler, S.G. Aging-related geniohyoid muscle atrophy is related to aspiration status in healthy older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 853–860. [Google Scholar] [CrossRef] [Green Version]
- Wakabayashi, H.; Takahashi, R.; Watanabe, N.; Oritsu, H.; Shimizu, Y. Prevalence of skeletal muscle mass loss and its association with swallowing function after cardiovascular surgery. Nutrition 2017, 38, 70–73. [Google Scholar] [CrossRef]
- Cormi, C.; Chrusciel, J.; Fayol, A.; van Rechem, M.; Abou-Amsha, K.; Tixier, M.; Lewkowicz, M.; Laplanche, D.; Sanchez, S. The Use of Telemedicine in Nursing Homes: A Mixed-Method Study to Identify Critical Factors When Connecting with a General Hospital. Int. J. Environ. Res. Public Health 2021, 18, 11148. [Google Scholar] [CrossRef]
- Plunger, P.; Eitenberger, M.; Kletecka-Pulker, M.; Wochele-Thoma, T.; Klager, E.; Ruf, A.K.; Eibensteiner, F. Using telemedicine in nursing homes during the COVID-19 pandemic: A multi-perspective view on the implementation process. Nurs. Open 2022, 9, 1155–1163. [Google Scholar] [CrossRef]
- Tan, A.J.; Rusli, K.D.; McKenna, L.; Tan, L.L.; Liaw, S.Y. Telemedicine experiences and perspectives of healthcare providers in long-term care: A scoping review. J. Telemed. Telecare 2021. [CrossRef]
- Aquilanti, L.; Santarelli, A.; Mascitti, M.; Procaccini, M.; Rappelli, G. Dental Care Access and the Elderly: What Is the Role of Teledentistry? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9053. [Google Scholar] [CrossRef]
- Queyroux, A.; Saricassapian, B.; Herzog, D.; Müller, K.; Herafa, I.; Ducoux, D.; Marin, B.; Dantoine, T.; Preux, P.-M.; Tchalla, A. Accuracy of Teledentistry for Diagnosing Dental Pathology Using Direct Examination as a Gold Standard: Results of the Tel-e-dent Study of Older Adults Living in Nursing Homes. J. Am. Med. Dir. Assoc. 2017, 18, 528–532. [Google Scholar] [CrossRef] [Green Version]
- Sacco, G.; Lléonart, S.; Simon, R.; Noublanche, F.; Annweiler, C. TOVID Study Group Communication Technology Preferences of Hospitalized and Institutionalized Frail Older Adults During COVID-19 Confinement: Cross-Sectional Survey Study. JMIR mHealth uHealth 2020, 8, e21845. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 Arch Mobile Prosthesis | 2 Arch Mobile Prosthesis | 1 Arch Skeletonized Prosthesis | 2 Arch Skeletonized Prosthesis | Relining Repair | |
|---|---|---|---|---|---|
| Men | 8 | 2 | 4 | 3 | 9 |
| Women | 11 | 3 | 7 | 5 | 15 |
| Little Power Supply | Normal Feeding | Abundant Nutrition | Conversation | |
|---|---|---|---|---|
| N° Men | 5 | 16 | 5 | 12 out of 26 |
| N° Women | 9 | 30 | 2 | 23 out of 41 |
| Hairdresser | Barber Shop | Combing Hair | Scented | |
|---|---|---|---|---|
| N° Men | -- | 26 | 16 | 20 |
| N° Women | 41 | -- | 41 | 37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceraulo, S.; Caccianiga, P.; Casto, C.; Ceraulo, I.; Caccianiga, G. Dental Prosthetic Rehabilitation Interventions in Elderly Patients Hospitalized in the Nursing Homes of the Lombardy Region: A Retrospective Study. Healthcare 2022, 10, 2328. https://doi.org/10.3390/healthcare10112328
Ceraulo S, Caccianiga P, Casto C, Ceraulo I, Caccianiga G. Dental Prosthetic Rehabilitation Interventions in Elderly Patients Hospitalized in the Nursing Homes of the Lombardy Region: A Retrospective Study. Healthcare. 2022; 10(11):2328. https://doi.org/10.3390/healthcare10112328
Chicago/Turabian StyleCeraulo, Saverio, Paolo Caccianiga, Carmelo Casto, Ignazio Ceraulo, and Gianluigi Caccianiga. 2022. "Dental Prosthetic Rehabilitation Interventions in Elderly Patients Hospitalized in the Nursing Homes of the Lombardy Region: A Retrospective Study" Healthcare 10, no. 11: 2328. https://doi.org/10.3390/healthcare10112328