
Use of Medicinal Plants during Pregnancy, Childbirth and Postpartum in Southern Morocco


Abstract
:1. Introduction
2. Materials and Methods
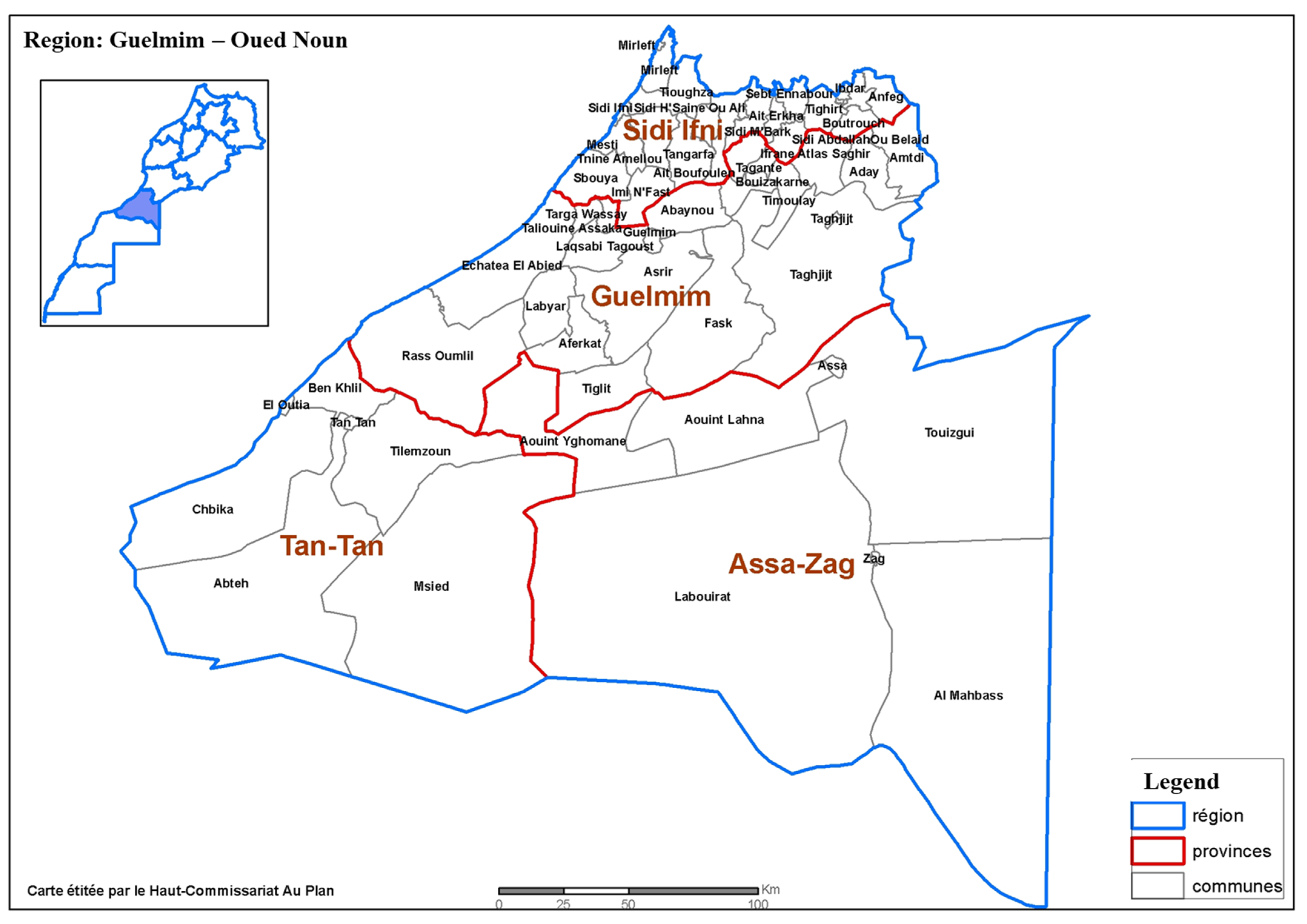
2.1. The Study Area
2.2. Type of Study
2.3. Study Population
2.4. Questionnaire
2.5. Ethical Considerations
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of the Population Surveyed
3.2. Characteristics of the Women Using MPs
3.3. Prevalence and Risk Factors Linked to the Use of MPs
3.4. Monograph of Medicinal Plants Used by Pregnant Women and Reasons for Use
- -
- First trimester of pregnancy: white mugwort, thyme and fenugreek.
- -
- Second trimester: thyme, white mugwort, olive tree and sesame.
- -
- Third trimester: white mugwort, thyme and fenugreek.
- -
- Labor and delivery: white mugwort, thyme, garden cress and saffron.
- -
- Postpartum: garden cress, fenugreek and white mugwort.
3.5. Mode of Preparation and Route of Administration
3.6. Source of Information
4. Discussion
- -
- A. herba-alba Asso (UV = 0.059); it is one of the most used plants in the Mediterranean region to treat various diseases including diabetes, hypertension, spasmodic dysphonia and certain bacterial infections [89]. In this study, A. herba-alba was cited for the treatment of gestational diabetes, hypertension, problems of the digestive tract, certain genital infections and to facilitate childbirth. It has been reported that the aqueous extract of A. herba-alba has hypoglycemic properties [90], antihypertensive activity [91] and antimicrobial and antifungal activities [92]. In addition, a limited number of scientific studies have demonstrated the harmful effect of this plant on pregnancy and the development of the fetus and infant. A study by Laadraoui et al. (2018) [89] highlighted that transplacental exposure of A. herba-alba affects reproduction by increasing infertility, delayed memory function and neuromotor reflex in mouse offspring.
- -
- T. maroccanus Ball. (UV = 0.045); it is a perennial aromatic shrub widely used to treat digestive, respiratory and nervous system diseases, rheumatism, bronchitis, fever, cough, wounds and many infections [93,94,95,96,97,98,99]. Pregnant women in the region of Guelmim use T. maroccanus Ball to treat problems related to pregnancy, namely, digestive disorders (constipation, vomiting, indigestion, etc.), genital infections, coughs, colds, the induction and acceleration of labor and also for good development of the fetus. The antiviral and analgesic activities of T. maroccanus oil have been documented previously [100]. In addition, a study by Belaqziz et al. (2013) [101] showed that the essential oil of T. maroccanus possesses antibacterial potential.
- -
- T. foenum-graecum L. (UV = 0.037); it is used by women in the Gulemim region to treat anemia, facilitate childbirth, promote the production of breast milk, induce labor and prevent and treat genital infections. According to Ulbricht et al. (2008), this herb has been used to treat a range of ailments ranging from labor induction to digestion to cough [102]. Additionally, previous studies have shown that fenugreek seeds increase milk production in lactating women [103]. According to Orief et al. (2014), fenugreek should be consumed with caution during pregnancy as the seeds have the ability to lower blood sugar levels and stimulate uterine contractions [16]. According to Vu (2019), fenugreek is well tolerated without serious side effects. However, it was reported by the same authors that when fenugreek is taken with certain pharmaceutical drugs, it can exacerbate the effect of the drugs [104].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Beaglehole, R. The World Health Report 2003: Shaping the Future; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Rejdali, M. La flore du Maroc: Etat actuel et perspectives de conservation. In Proceeding du Symposium‘Diversité Biologique et Valorisation des Plantes Médicinales. Actes Editions; IAV. Hassan II: Rabat, Morocco, 1996; pp. 17–22. [Google Scholar]
- Bammi, J.; Douira, A. Les plantes médicinales dans la forêt de l’achach (plateau central, Maroc). Acta Bot. Malacit. 2002, 27, 131–145. [Google Scholar] [CrossRef]
- Fakchich, J.; Elachouri, M. Ethnobotanical survey of medicinal plants used by people in Oriental Morocco to manage various ailments. J. Ethnopharmacol. 2014, 154, 76–87. [Google Scholar]
- El Haouari, M.; Bnouham, M.; Bendahou, M.; Aziz, M.; Ziyyat, A.; Legssyer, A.; Mekhfi, H. Inhibition of rat platelet aggregation by Urtica dioica leaves extracts. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2006, 20, 568–572. [Google Scholar]
- Bouiamrine, E.H.; Bachiri, L.; Ibijbijen, J.; Nassiri, L. Fresh medicinal plants in middle atlas of Morocco: Trade and threats to the sustainable harvesting. J. Med. Plants 2017, 5, 123–128. [Google Scholar]
- Hamamouch, N. Use of ethnomedicinal plants by the people living in the middle atlas mountains in Morocco. Med. Aromat. Plants 2020, 9, 349. [Google Scholar] [CrossRef]
- Tahraoui, A.; El-Hilaly, J.; Israili, Z.; Lyoussi, B. Ethnopharmacological survey of plants used in the traditional treatment of hypertension and diabetes in south-eastern Morocco (Errachidia province). J. Ethnopharmacol. 2007, 110, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Lindzon, G.; Sadry, S.; Sharp, J. Obstetric. In Toronto Notes for Medical Students, 27th ed.; Type & Graphics Inc.: Vaughan, ON, Canada, 2011. [Google Scholar]
- Holst, L.; Wright, D.; Nordeng, H.; Haavik, S. Use of herbal preparations during pregnancy: Focus group discussion among expectant mothers attending a hospital antenatal clinic in Norwich, UK. Complement. Ther. Clin. Pract. 2009, 15, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Bhat, R. Medicinal plants and traditional practices of Xhosa people in the Transkei region of Eastern Cape, South Africa. Indian J. Tradit. Knowl. 2014, 13, 292–298. [Google Scholar]
- Tsui, B.; Dennehy, C.E.; Tsourounis, C. A survey of dietary supplement use during pregnancy at an academic medical center. Am. J. Obstet. Gynecol. 2001, 185, 433–437. [Google Scholar] [CrossRef]
- Rajith, N.; Navas, M.; Thaha, A.M.; Manju, M.; Anish, N.; Rajasekharan, S.; George, V. A study on traditional mother care plants of rural communities of South Kerala. Indian J. Tradit. Knowl. 2010, 9, 203–208. [Google Scholar]
- Cuzzolin, L.; Francini-Pesenti, F.; Verlato, G.; Joppi, M.; Baldelli, P.; Benoni, G. Use of herbal products among 392 Italian pregnant women: Focus on pregnancy outcome. Pharmacoepidemiol. Drug Saf. 2010, 19, 1151–1158. [Google Scholar] [CrossRef]
- Dugoua, J.-J. Herbal medicines and pregnancy. J. Popul. Ther. Clin. Pharmacol. 2010, 17, 370–378. [Google Scholar]
- Orief, Y.I.; Farghaly, N.F.; Ibrahim, M.I.A. Use of herbal medicines among pregnant women attending family health centers in Alexandria. Middle East Fertil. Soc. J. 2014, 19, 42–50. [Google Scholar] [CrossRef]
- Malan, D.F.; Neuba, D.F. Traditional practices and medicinal plants use during pregnancy by Anyi-Ndenye women (Eastern Côte d’Ivoire). Afr. J. Reprod. Health 2011, 15, 85–93. [Google Scholar]
- Ernst, E. Herbal medicinal products during pregnancy: Are they safe? BJOG Int. J. Obstet. Gynaecol. 2002, 109, 227–235. [Google Scholar] [CrossRef]
- Illamola, S.M.; Amaeze, O.U.; Krepkova, L.V.; Birnbaum, A.K.; Karanam, A.; Job, K.M.; Bortnikova, V.V.; Sherwin, C.M.; Enioutina, E.Y. Use of herbal medicine by pregnant women: What physicians need to know. Front. Pharmacol. 2020, 10, 1483. [Google Scholar] [CrossRef]
- Holst, L.; Nordeng, H.; Haavik, S. Use of herbal drugs during early pregnancy in relation to maternal characteristics and pregnancy outcome. Pharmacoepidemiol. Drug Saf. 2008, 17, 151–159. [Google Scholar] [CrossRef]
- Bercaw, J.; Maheshwari, B.; Sangi-Haghpeykar, H. The use during pregnancy of prescription, over-the-counter, and alternative medications among Hispanic women. Birth 2010, 37, 211–218. [Google Scholar] [CrossRef]
- Sun, X.; Xue, Z.; Yasin, A.; He, Y.; Chai, Y.; Li, J.; Zhang, K. Colorectal Cancer and Adjacent Normal Mucosa Differ in Apoptotic and Inflammatory Protein Expression. Eng. Regen. 2022, 2, 279–287. [Google Scholar] [CrossRef]
- Balbontín, Y.M.; Stewart, D.; Shetty, A.; Fitton, C.A.; McLay, J.S. Herbal medicinal product use during pregnancy and the postnatal period: A systematic review. Obstet. Gynecol. 2019, 133, 920. [Google Scholar] [CrossRef] [Green Version]
- Seddiki, A.E.; Messaouidi, S.; Amrani, R. Le rôle du fenugrec dans la survenue d’anomalie de fermeture du tube neural: Un signal d’alerte depuis le Maroc. Phytothérapie 2017, 15, 155–158. [Google Scholar] [CrossRef]
- Achour, S.; Saadi, H.; Turcant, A.; Banani, A.; Mokhtari, A.; Soulaymani, A.; Bencheikh, R.S. Intoxication au Peganum harmala L. et grossesse: Deux observations marocaines. Médecine et St. Trop. 2012, 22, 84–86. [Google Scholar]
- Lahsissene, H.; Kahouadji, A.; Hseini, S. Catalogue des Plantes Médicinales Utilisées dans la Région de Zaër (Maroc Occidental). Lejeunia, Revue de Botanique. 2009. Available online: https://popups.uliege.be/0457-4184/index.php?id=701 (accessed on 1 February 2021).
- Boukaici, F. Risque de la Phytothérapie chez la Femme Enceinte: Monographie des Plantes Médicinales Marocaine à Risque. Ph.D. Thesis, Mohammed V University, Rabat, Morocco, 2018. Available online: http://ao.um5s.ac.ma/xmlui/handle/123456789/16333 (accessed on 1 February 2021).
- Elkhoudri, N.; Baali, A.; Amor, H. Maternal morbidity and the use of medicinal herbs in the city of Marrakech, Morocco. Indian J. Tradit. Knowl. 2016, 15, 79–85. [Google Scholar]
- La Région de Guelmim-Oued Noun. Monographie Generale. 2015. Available online: https://www.regions-maroc.ma/wp-content/uploads/2020/10/MONOGRAPHIE-DE-LA-REGION-DE-GUELMIM-OUED-NOUN-FR.pdf (accessed on 1 February 2021).
- Fennane, M.; Ibn Tattou, M. Observations sur la flore vasculaire endémique, rare ou menacée du Maroc. Flora Mediterr. 1999, 9, 113–124. [Google Scholar]
- Fennane, M.; Ibn Tattou, M.; Ouyahya, A.; El Oulaidi, J. Flore pratique du Maroc. Travaux Institut Scientifique, Sér. Botanique 2007, 2, 648. [Google Scholar]
- Fennane, M.; Tattou, M.I.; El Oualidi, J. Flore Pratique du Maroc: Manuel de Détermination des Plantes Vasculaires. Dicotyledones (pp), Monocotyledones/éditeurs Mohamed Fennane, Mohammed Ibn Tattou, Jalal El Oualidi; Service d’édition; Institut Scientifique: Rabat, Morocco, 2014. [Google Scholar]
- Phillips, O.; Gentry, A.H.; Reynel, C.; Wilkin, P.; Gálvez-Durand, B.C. Quantitative ethnobotany and Amazonian conservation. Conserv. Biol. 1994, 8, 225–248. [Google Scholar] [CrossRef]
- Da Silva, V.A.; Andrade, L.D.H.C.; De Albuquerque, U.P. Revising the cultural significance index: The case of the Fulni-ô in northeastern Brazil. Field Methods 2006, 18, 98–108. [Google Scholar] [CrossRef]
- Tardío, J.; Pardo-de-Santayana, M. Cultural importance indices: A comparative analysis based on the useful wild plants of Southern Cantabria (Northern Spain) 1. Econ. Bot. 2008, 62, 24–39. [Google Scholar] [CrossRef]
- Yeh, H.-Y.; Chen, Y.-C.; Chen, F.-P.; Chou, L.-F.; Chen, T.-J.; Hwang, S.-J. Use of traditional Chinese medicine among pregnant women in Taiwan. Int. J. Gynecol. Obstet. 2009, 107, 147–150. [Google Scholar] [CrossRef]
- Forster, D.A.; Denning, A.; Wills, G.; Bolger, M.; McCarthy, E. Herbal medicine use during pregnancy in a group of Australian women. BMC Pregnancy Childbirth 2006, 6, 21. [Google Scholar] [CrossRef] [Green Version]
- Al-Riyami, I.M.; Al-Busaidy, I.Q.; Al-Zakwani, I.S. Medication use during pregnancy in Omani women. Int. J. Clin. Pharm. 2011, 33, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.; Lupattelli, A.; Koren, G.; Nordeng, H. Safety classification of herbal medicines used in pregnancy in a multinational study. BMC Complement. Altern. Med. 2016, 16, 102. [Google Scholar] [CrossRef] [Green Version]
- John, L.J.; Shantakumari, N. Herbal medicines use during pregnancy: A review from the Middle East. Oman Med. J. 2015, 30, 229. [Google Scholar] [CrossRef] [PubMed]
- Amasha, H.; Jarrah, S. The use of home remedies by pregnant mothers as a treatment of pregnancy related complaints: An exploratory study. Med. J. Cairo Univ. 2012, 80, 673–680. [Google Scholar]
- Hashem, D.F.; Abdollahi, F.M.; Shojaei, A.; Kianbakht, S.; Zafarghandi, N.; Goushegir, A. Use and attitude on herbal medicine in a group of pregnant women in Tehran. J. Med. Plants 2012, 11, 22–33. [Google Scholar]
- Kennedy, D.A.; Lupattelli, A.; Koren, G.; Nordeng, H. Herbal medicine use in pregnancy: Results of a multinational study. BMC Complement. Altern. Med. 2013, 13, 355. [Google Scholar] [CrossRef] [Green Version]
- Hall, H.R.; Jolly, K. Women’s use of complementary and alternative medicines during pregnancy: A cross-sectional study. Midwifery 2014, 30, 499–505. [Google Scholar] [CrossRef]
- Laelago, T.; Yohannes, T.; Lemango, F. Prevalence of herbal medicine use and associated factors among pregnant women attending antenatal care at public health facilities in Hossana Town, Southern Ethiopia: Facility based cross sectional study. Arch. Public Health 2016, 74, 7. [Google Scholar] [CrossRef] [Green Version]
- Mawoza, T.; Nhachi, C.; Magwali, T. Prevalence of traditional medicine use during pregnancy, at labour and for postpartum care in a rural area in Zimbabwe. Clin. Mother Child Health 2019, 16, 321. [Google Scholar]
- Inamdar, I.; Sonkar, V.; Aswar, N.; Doibale, M. Drug Utilization Pattern During Pregnancy. Ind. Med. Gaz. 2012, 146, 305–311. [Google Scholar]
- Jaradat, N.; Adawi, D. Use of herbal medicines during pregnancy in a group of Palestinian women. J. Ethnopharmacol. 2013, 150, 79–84. [Google Scholar]
- Abdollahi, F.; Yazdani Chareti, J. The relationship between women’s characteristics and herbal medicines use during pregnancy. Women Health 2019, 59, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Louik, C.; Gardiner, P.; Kelley, K.; Mitchell, A.A. Use of herbal treatments in pregnancy. Am. J. Obstet. Gynecol. 2010, 202, 439.e1–439.e10. [Google Scholar] [CrossRef] [Green Version]
- Sereshti, M.; Azari, P.; Rafieian-Kopaei, M.; Kheiri, S. Use of herbal medicines by pregnant women in Shahr-e-Kord. J. Reprod. Infertil. 2006, 7, 125–131. [Google Scholar]
- Soon, L.; Law, K.; Mohsin, S.; Farid, C. Use of herbal medicine during pregnancy: A cross-sectional survey. Malays. J. Obstet. Gynecol. 2009, 8, 35. [Google Scholar]
- Kim Sooi, L.; Lean Keng, S. Herbal medicines: Malaysian women’s knowledge and practice. Evid.-Based Complement. Altern. Med. 2013, 2013, 438139. [Google Scholar] [CrossRef] [Green Version]
- Tiran, D. The use of herbs by pregnant and childbearing women: A risk–benefit assessment. Complement. Ther. Nurs. Midwifery 2003, 9, 176–181. [Google Scholar] [CrossRef]
- Broussard, C.S.; Louik, C.; Honein, M.A.; Mitchell, A.A. National Birth Defects Prevention Study. Herbal use before and during pregnancy. Am. J. Obstet. Gynecol. 2010, 202, 443.e1–443.e6. [Google Scholar] [CrossRef]
- Bernstein, N.; Akram, M.; Yaniv-Bachrach, Z.; Daniyal, M. Is it safe to consume traditional medicinal plants during pregnancy? Phytother. Res. 2021, 35, 1908–1924. [Google Scholar] [CrossRef]
- Guillot, L. Maux Bénins de la Grossesse: Conseil en Phytothérapie à L’officine. Ph.D. Thesis, Université Aix Marseille, Marseille, France, 2017; p. 116. [Google Scholar]
- Tabatabaee, M. Use of herbal medicine among pregnant women referring to Valiasr Hospital in Kazeroon, Fars, South of Iran. J. Med. Plants 2011, 10, 96–108. [Google Scholar]
- Hashim, M.; Johina, A.; Deyaa, K.; Fareed, M.; Mohamed, H.; Faten, A. Knowledge attitude and practice of complementary and alternative medicine (CAM) among pregnant women: A preliminary survey in Qatar. Middle East J. Fam. Med. 2005, 7, 6–14. [Google Scholar]
- Khadivzadeh, T.; Ghabel, M. Complementary and alternative medicine use in pregnancy in Mashhad, Iran, 2007–2008. Iran. J. Nurs. Midwifery Res. 2012, 17, 263. [Google Scholar] [PubMed]
- Hanafy, S.A.; Sallam, S.A.; Kharboush, I.F.; Wahdan, I.H. Drug utilization pattern during pregnancy in Alexandria, Egypt. Eur. J. Pharm. Med. Res. 2016, 3, 19–29. [Google Scholar]
- Saber, M.; Khanjani, N.; Zamanian, M.; Safinejad, H.; Shahinfar, S.; Borhani, M. Use of medicinal plants and synthetic medicines by pregnant women in Kerman, Iran. Arch. Iran. Med. 2019, 22, 390–393. [Google Scholar] [PubMed]
- Aljofan, M.; Alkhamaiseh, S. Prevalence and factors influencing use of herbal medicines during pregnancy in Hail, Saudi Arabia: A Cross-Sectional Study. Sultan Qaboos Univ. Med. J. 2020, 20, e71. [Google Scholar] [CrossRef]
- Rahman, A.A.; Sulaiman, S.A.; Ahmad, Z.; Daud, W.N.W.; Hamid, A.M. Prevalence and pattern of use of herbal medicines during pregnancy in Tumpat district, Kelantan. Malays. J. Med. Sci. 2008, 15, 40. [Google Scholar]
- Nordeng, H.; Bayne, K.; Havnen, G.C.; Paulsen, B.S. Use of herbal drugs during pregnancy among 600 Norwegian women in relation to concurrent use of conventional drugs and pregnancy outcome. Complement. Ther. Clin. Pract. 2011, 17, 147–151. [Google Scholar] [CrossRef]
- Holst, L.; Wright, D.; Haavik, S.; Nordeng, H. Safety and efficacy of herbal remedies in obstetrics—Review and clinical implications. Midwifery 2011, 27, 80–86. [Google Scholar] [CrossRef]
- Kamatenesi-Mugisha, M.; Oryem-Origa, H. Medicinal plants used to induce labour during childbirth in western Uganda. J. Ethnopharmacol. 2007, 109, 1–9. [Google Scholar] [CrossRef]
- Adusi-Poku, Y.; Vanotoo, L.; Detoh, E.; Oduro, J.; Nsiah, R.; Natogmah, A. Type of herbal medicines utilized by pregnant women attending ante-natal clinic in Offinso north district: Are orthodox prescribers aware? Ghana Med. J. 2015, 49, 227–232. [Google Scholar] [CrossRef] [Green Version]
- El Hajj, M.; Holst, L. Herbal medicine use during pregnancy: A review of the literature with a special focus on sub-Saharan Africa. Front. Pharmacol. 2020, 11, 866. [Google Scholar] [CrossRef] [PubMed]
- Sawalha, A.F. Consumption of prescription and non-prescription medications by pregnant women: A cross sectional study in Palestine. IUG J. Nat. Stud. 2007, 15, 41–57. [Google Scholar]
- Armel Moyabi, A.G.; Amadou Coulibaly, F.; Jules Kouadio, N.; Yao, K.Y.; Witabouna Koné, M. Plantes Médicinales Utilisées Dans L’entretien Des Grossesses Dans Le Département D’Oumé (Centre-Ouest, Côte d’Ivoire). Eur. Sci. J. 2020, 16, 187–203. [Google Scholar]
- Fukunaga, R.; Morof, D.; Blanton, C.; Ruiz, A.; Maro, G.; Serbanescu, F. Factors associated with local herb use during pregnancy and labor among women in Kigoma region, Tanzania, 2014–2016. BMC Pregnancy Childbirth 2020, 20, 122. [Google Scholar] [CrossRef]
- Mugomeri, E.; Chatanga, P.; Seliane, K.; Maibvise, C. Identifying promoters and reasons for medicinal herb usage during pregnancy in Maseru, Lesotho. Afr. J. Nurs. Midwifery 2015, 17, 4–16. [Google Scholar] [CrossRef]
- Nordeng, H.; Havnen, G.C. Impact of socio-demographic factors, knowledge and attitude on the use of herbal drugs in pregnancy. Acta Obstet. Gynecol. Scand. 2005, 84, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Pacifique, M.; De Dieu, M.M.J.; Gentil, I.K.; René, M. Etude Des Plantes Médicinales Utilisées Par Les Femmes Autochtones Pygmées (Batwa) Enceintes Dans L’hinterland Du Parc National De Kahuzi-Biega (Rift albertin, RD. Congo). Eur. Sci. J. 2020, 16, 27. [Google Scholar] [CrossRef]
- Taloubi, L.; Belahcen, A.; Forci, K. Fenugrec et grossesse: Quels risques encourus? Étude prospective au niveau des maternités Soussi et des Orangers CHIS Rabat. Cah. D’abstracts Journées Pédiatrie Fès CO 2015, 10, 123–124. [Google Scholar]
- Kakani, R.; Anwer, M. Fenugreek. In Handbook of Herbs and Spices, 2nd ed.; Woodhead Publishing Series in Food Science Technology and Nutrition; Woodhead Publishing: Cambridge, UK, 2012; Volume 1, pp. 286–298. [Google Scholar]
- Facchinetti, F.; Pedrielli, G.; Benoni, G.; Joppi, M.; Verlato, G.; Dante, G.; Balduzzi, S.; Cuzzolin, L. Herbal supplements in pregnancy: Unexpected results from a multicentre study. Hum. Reprod. 2012, 27, 3161–3167. [Google Scholar] [CrossRef] [Green Version]
- Frawley, J.; Adams, J.; Sibbritt, D.; Steel, A.; Broom, A.; Gallois, C. Prevalence and determinants of complementary and alternative medicine use during pregnancy: Results from a nationally representative sample of Australian pregnant women. Aust. N. Z. J. Obstet. Gynaecol. 2013, 53, 347–352. [Google Scholar] [CrossRef]
- Haruna, D.; Mauki, D.; Shabani, I.; Richard, R. Prevalent use of herbs for reduction of labour duration in Mwanza, Tanzania: Are obstetricians aware? Tanzan. J. Health Res. 2017, 19. [Google Scholar] [CrossRef]
- Hemminki, E.; Mäntyranta, T.; Malin, M.; Koponen, P. A survey on the use of alternative drugs during pregnancy. Scand. J. Soc. Med. 1991, 19, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. Enquête Nationale sur la Population et la Santé Familiale, (Ministère de la Santé, Royaume du Maroc). 2011. Available online: https://www.sante.gov.ma/Publications/Etudes_enquete/Documents/Indicateurs%20regionaux_ENPSF-2011.pdf (accessed on 11 November 2022).
- Ahmed, S.M.; Nordeng, H.; Sundby, J.; Aragaw, Y.A.; de Boer, H.J. The use of medicinal plants by pregnant women in Africa: A systematic review. J. Ethnopharmacol. 2018, 224, 297–313. [Google Scholar] [CrossRef] [PubMed]
- Boudjelal, A.; Henchiri, C.; Sari, M.; Sarri, D.; Hendel, N.; Benkhaled, A.; Ruberto, G. Herbalists and wild medicinal plants in M’Sila (North Algeria): An ethnopharmacology survey. J. Ethnopharmacol. 2013, 148, 395–402. [Google Scholar] [CrossRef]
- Ouhaddou, H.; Boubaker, H.; Msanda, F.; El Mousadik, A. An ethnobotanical study of medicinal plants of the Agadir Ida Ou Tanane province (southwest Morocco). J. Appl. Biosci. 2014, 84, 7707–7722. [Google Scholar] [CrossRef]
- Chermat, S.; Gharzouli, R. Ethnobotanical study of medicinal flora in the North East of Algeria-An empirical knowledge in Djebel Zdimm (Setif). J. Mater. Sci. Eng. 2015, 5, 50–59. [Google Scholar]
- Barkaoui, M.; Katiri, A.; Boubaker, H.; Msanda, F. Ethnobotanical survey of medicinal plants used in the traditional treatment of diabetes in Chtouka Ait Baha and Tiznit (Western Anti-Atlas), Morocco. J. Ethnopharmacol. 2017, 198, 338–350. [Google Scholar] [CrossRef]
- Katiri, A.; Barkaoui, M.; Msanda, F.; Boubaker, H. Ethnobotanical survey of medicinal plants used for the treatment of diabetes in the Tizin’Test region (Taroudant Province, Morocco). J. Pharm. Nat. Prod. 2017, 3, 2472-0992. [Google Scholar]
- Laadraoui, J.; Aboufatima, R.; El Gabbas, Z.; Ferehan, H.; Bezza, K.; Laaradia, M.A.; Marhoume, F.; Wakrim, E.M.; Chait, A. Effect of Artemisia herba-alba consumption during pregnancy on fertility, morphological and behaviors of mice offspring. J. Ethnopharmacol. 2018, 226, 105–110. [Google Scholar] [CrossRef]
- Hamza, N.; Berke, B.; Cheze, C.; Agli, A.-N.; Robinson, P.; Gin, H.; Moore, N. Prevention of type 2 diabetes induced by high fat diet in the C57BL/6J mouse by two medicinal plants used in traditional treatment of diabetes in the east of Algeria. J. Ethnopharmacol. 2010, 128, 513–518. [Google Scholar] [CrossRef]
- Zeggwagh, N.; Farid, O.; Michel, J.; Eddouks, M. Cardiovascular effect of Artemisia herba alba aqueous extract in spontaneously hypertensive rats. Methods Find. Exp. Clin. Pharmacol. 2008, 30, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.E.-H.H.; El-Sayed, M.; Hegazy, M.E.; Helaly, S.E.; Abeer, M.E.; Naglaa, S.M. Chemical constituents and biological activities of Artemisia herba-alba. Rec. Nat. Prod. 2010, 4, 1–25. [Google Scholar]
- El Bouzidi, L.; Jamali, C.A.; Bekkouche, K.; Hassani, L.; Wohlmuth, H.; Leach, D.; Abbad, A. Chemical composition, antioxidant and antimicrobial activities of essential oils obtained from wild and cultivated Moroccan Thymus species. Ind. Crops Prod. 2013, 43, 450–456. [Google Scholar] [CrossRef]
- Belhaj, S.; Dahmani, J.; Belahbib, N.; Zidane, L. Ethnopharmacological and Ethnobotanical study of Medicinal plants in the Central High Atlas, Morocco. Ethnobot. Res. Appl. 2020, 20, 1–40. [Google Scholar] [CrossRef]
- Daoudi, A.; Bammou, M.; Zarkani, S.; Slimani, I.; Ibijbijen, J.; Nassiri, L. Ethnobotanical study of medicinal flora in rural municipality of Aguelmouss-Khenifra province–(Morocco). Phytothérapie 2016, 14, 220–228. [Google Scholar] [CrossRef]
- El Alami, A.; Farouk, L.; Chait, A. Etude ethnobotanique sur les plantes médicinales spontanées poussant dans le versant nord de l’Atlas d’Azilal (Maroc). Alger. J. Nat. Prod. 2016, 4, 271–282. [Google Scholar]
- Fakchich, J.; Elachouri, M. An overview on ethnobotanico-pharmacological studies carried out in Morocco, from 1991 to 2015: Systematic review (part 1). J. Ethnopharmacol. 2021, 267, 113200. [Google Scholar] [CrossRef]
- Najem, M.; Harouak, H.; Ibijbijen, J.; Nassiri, L. Oral disorders and ethnobotanical treatments: A field study in the central Middle Atlas (Morocco). Heliyon 2020, 6, e04707. [Google Scholar] [CrossRef]
- El Yaagoubi, M.; Mechqoq, H.; El Hamdaoui, A.; Mukku, V.J.; El Mousadik, A.; Msanda, F.; El Aouad, N. A review on Moroccan Thymus species: Traditional uses, essential oils chemical composition and biological effects. J. Ethnopharmacol. 2021, 278, 114205. [Google Scholar] [CrossRef]
- Mouhajir, F.; Hudson, J.; Rejdali, M.; Towers, G. Multiple antiviral activities of endemic medicinal plants used by Berber peoples of Morocco. Pharm. Biol. 2001, 39, 364–374. [Google Scholar] [CrossRef]
- Belaqziz, R.; Bahri, F.; Romane, A.; Antoniotti, S.; Fernandez, X.; Duñach, E. Essential oil composition and antibacterial activity of the different parts of Thymus maroccanus Ball: An endemic species in Morocco. Nat. Prod. Res. 2013, 27, 1700–1704. [Google Scholar] [CrossRef] [PubMed]
- Ulbricht, C.; Basch, E.; Burke, D.; Cheung, L.; Ernst, E.; Giese, N.; Foppa, I.; Hammerness, P.; Hashmi, S.; Kuo, G. Fenugreek (Trigonella foenum-graecum L. Leguminosae): An evidence-based systematic review by the natural standard research collaboration. J. Herb. Pharmacother. 2008, 7, 143–177. [Google Scholar] [CrossRef] [PubMed]
- Farnsworth, N.R.; Bingel, A.S.; Cordell, G.A.; Crane, F.A.; Fong, H.H. Potential value of plants as sources of new antifertility agents I. J. Pharm. Sci. 1975, 64, 535–598. [Google Scholar] [CrossRef] [PubMed]
- Vu, A. Navigating the Myths and Truths Behind Pharmacological Drug and Herbal Supplement Use: A Guide for Pregnant Women. Bachelor’s Thesis, Regis University, Weston, MA, USA, 2019. Available online: https://epublications.regis.edu/theses/931 (accessed on 12 November 2022).
- de Boer, H.; Lamxay, V. Plants used during pregnancy, childbirth and postpartum healthcare in Lao PDR: A comparative study of the Brou, Saek and Kry ethnic groups. J. Ethnobiol. Ethnomed. 2009, 5, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nergard, C.S.; Ho, T.P.T.; Diallo, D.; Ballo, N.; Paulsen, B.S.; Nordeng, H. Attitudes and use of medicinal plants during pregnancy among women at health care centers in three regions of Mali, West-Africa. J. Ethnobiol. Ethnomed. 2015, 11, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali-Shtayeh, M.S.; Jamous, R.M.; Jamous, R.M. Plants used during pregnancy, childbirth, postpartum and infant healthcare in Palestine. Complement. Ther. Clin. Pract. 2015, 21, 84–93. [Google Scholar] [CrossRef]
- Bayisa, B.; Tatiparthi, R.; Mulisa, E. Use of herbal medicine among pregnant women on antenatal care at Nekemte Hospital, Western Ethiopia. Jundishapur J. Nat. Pharm. Prod. 2014, 9, e17368. [Google Scholar] [CrossRef] [Green Version]
- Yemele, M.; Telefo, P.; Lienou, L.; Tagne, S.; Fodouop, C.; Goka, C.; Lemfack, M.; Moundipa, F. Ethnobotanical survey of medicinal plants used for pregnant women’s health conditions in Menoua division-West Cameroon. J. Ethnopharmacol. 2015, 160, 14–31. [Google Scholar] [CrossRef]
- Mothupi, M.C. Use of herbal medicine during pregnancy among women with access to public healthcare in Nairobi, Kenya: A cross-sectional survey. BMC Complement. Altern. Med. 2014, 14, 432. [Google Scholar] [CrossRef]
- Alsubaie, S.F.; Alshehri, M.G.; Ghalib, R.H. Awareness, use, and attitude towards herbal medicines among Saudi women-cross sectional study. Imp. J. Interdiscip. Res. 2017, 3, 285–290. [Google Scholar]
- Al Essa, M.; Alissa, A.; Alanizi, A.; Bustami, R.; Almogbel, F.; Alzuwayed, O.; Moti, M.A.; Alsadoun, N.; Alshammari, W.; Albekairy, A. Pregnant women’s use and attitude toward herbal, vitamin, and mineral supplements in an academic tertiary care center, Riyadh, Saudi Arabia. Saudi Pharm. J. 2019, 27, 138–144. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Health Structures | Number of Pregnant Women Interviewed |
|---|---|
| First-level urban health centers | 305 |
| Second-level rural health centers with delivery unit | 127 |
| First-level rural health centers | 28 |
| Maternity hospital | 100 |
| Total | 560 |
| Variables | Total (560) | Use of Medicinal Plants | p-Value | |
|---|---|---|---|---|
| No (185) | Yes (375) | |||
| N (%) | N (%) | N (%) | p = 0.141 | |
| Family situation | ||||
| Divorced | 6 (1.1) | 0 | 6 (1.5) | |
| Married | 554 (98.9) | 148 (100) | 406 (98.5) | |
| Education level | p = 0.004 | |||
| None | 135 (24.5) | 52 (36.1) | 83 (20.4) | |
| Primary | 127 (23.0) | 33 (22.9) | 94 (23.1) | |
| Middle school | 136 (24.7) | 28 (19.4) | 108 (26.5) | |
| High school | 81 (14.7) | 16 (11.1) | 65 (16) | |
| College | 72 (13.1) | 15 (10.4) | 57 (14.0) | |
| Age (Median; Q1–Q3) | 30 years old (25–34.15) | 30.01 years old (25–35) | 29.43 years old (25–34) | p = 0.777 |
| Height (Median; Q1–Q3) | 161.47 cm (1.574–1.657) | 161.02 cm (155.02–165.00) | 161.63 cm (158.00–166.0) | p = 0.057 |
| Weight (Median; Q1–Q3) | 72.00 Kg (60.91–81.02) | 72.20 Kg (61.19–82.27) | 72.00 Kg (60.82–81.00) | p = 0.969 |
| Environment | p = 0.971 | |||
| Nomad | 8 (1.4) | 2 (1.4) | 6 (1.5) | |
| Rural | 182 (32.6) | 49 (33.3) | 133 (32.3) | |
| Urban | 369 (66.0) | 96 (65.3) | 273 (66.3) | |
| Language | p = 0.669 | |||
| Amazigh | 125 (22.5) | 32 (21.8) | 93 (22.8) | |
| Dialectal Arabic | 430 (77.5) | 115 (78.2) | 315 (77.2) | |
| Employment of the woman | ||||
| Employed | 54 (9.75) | 16 (10.60) | 38 (9.43) | p = 0.680 |
| Unemployed | 500 (90.25) | 135 (89.40) | 365 (90.57) | |
| Employment of the husband | p = 0.117 | |||
| Employed | 533 (96.6) | 137 (94.5) | 396 (97.3) | |
| Unemployed | 19 (3.4) | 8 (5.5) | 11 (2.7) | |
| Income level | p = 0.065 | |||
| Poor | 280 (50.1) | 83 (56.5) | 197 (47.8) | |
| Middle class | 220 (39.4) | 46 (31.3) | 174 (42.2) | |
| Rich | 59 (10.6) | 18 (12.2) | 41 (10.0) | |
| Medical insurance | p = 0.056 | |||
| None | 106 (19.4) | 38 (26.4) | 68 (16.9) | |
| RAMED 1 | 276 (50.5) | 71 (49.3) | 205 (50.9) | |
| CNOPS | 111 (20.3) | 27 (18.8) | 84 (20.8) | |
| CNSS | 19 (3.5) | 2 (1.4) | 17 (4.2) | |
| Private insurance | 35 (6.4) | 6 (4.2) | 29 (7.2) | |
| Medical history | p = 0.271 | |||
| No | 454 (81.2) | 124 (84.4) | 330 (80.1) | |
| Yes | 105 (18.8) | 23 (15.6) | 82 (19.9) | |
| Surgical history | p = 0.590 | |||
| No | 526 (94.1) | 137 (93.2) | 389 (94.4) | |
| Yes | 33 (5.9) | 10 (6.8) | 23 (5.6) | |
| Gynecological history | p = 0.489 | |||
| No | 410 (73.3) | 111 (75.5) | 299 (72.6) | |
| Yes | 149 (26.7) | 36 (24.5) | 113 (27.4) | |
| Gestation | p = 0.839 | |||
| 1st trimester | 184 (33) | 53 (35.11) | 131 (31.8) | |
| 2nd trimester | 144 (25.8) | 36 (24.5) | 108 (26.2) | |
| 3rd trimester | 127 (22.7) | 31 (21.1) | 96 (23.3) | |
| ≥4th trimester | 104 (18.6) | 27 (18.4) | 77 (18.7) | |
| Parity | p = 0.190 | |||
| Nulliparity | 64 (11.4) | 17 (11.6) | 47 (11.4) | |
| 1st parity | 161 (28.8) | 45 (30.6) | 116 (28.2) | |
| 2nd parity | 148 (26.5) | 40 (27.2) | 108 (26.2) | |
| 3rd parity | 99 (17.7) | 21 (14.3) | 78 (18.9) | |
| Multiparity > 4 | 87 (15.6) | 24 (16.3) | 63 (15.3) | |
| Pregnancy follow-up | p = 0.028 | |||
| No | 35 (6.3) | 15 (10.2) | 20 (4.9) | |
| Yes | 524 (93.7) | 132 (89.8) | 392 (95.1) | |
| Assessment/ultrasound | p = 0.653 | |||
| No | 65 (11.6) | 15 (10.2) | 50 (12.1) | |
| Yes | 494 (88.4) | 132 (89.8) | 362 (87.9) | |
| Pregnancy at risk | p = 0.188 | |||
| No | 367 (65.7) | 90 (61.2) | 277 (67.2) | |
| Yes | 192 (34.3) | 57 (38.8) | 135 (32.8) | |
| Type of pregnancy at risk | ||||
| Anemia | 102 (46.57) | 34 (50) | 68 (45.03) | |
| Gestational diabetes | 45 (20.54) | 16 (23.53) | 29 (19.21) | |
| High blood pressure | 28 (12.78) | 6 (8.82) | 22 (14.57) | |
| Pre-eclampsia | 6 (2.73) | 0 | 6 (3.97) | |
| Others | 38 (17.5) | 12 (17.64) | 26 (17.21) | |
| Family and Scientific Name | Vernacular Name | Mode of Preparation | Time | Reason for Use | Mode of Administration | FRC 1 | UV 2 |
|---|---|---|---|---|---|---|---|
| Alliaceae | |||||||
| Allium cepa L. | Onion | Raw | TR2 3 | Prevention of miscarriages Vaginal itching/pruritus Prevention and treatment of genital infections | Vaginal | 0.003 | 0.008 |
| Allium sativum L. | Garlic | Raw | TR1 4, TR2, TR3 5 | Urinary burns Pain Uterine involution Cold/flu/cough | Oral | 0.013 | 0.011 |
| Anacardiaceae | |||||||
| Pistacia lentiscus L. | Lentisk | Fumigation | TR1, TR2 | Prevention and treatment of genital infections | Vaginal | 0.002 | 0.003 |
| Apiaceae | |||||||
| Foeniculum vulgare Mill. | Fennel | Powder Raw Decoction Infusion | Childbirth TR1, TR2, TR3 Postpartum | Intestinal bloating Good fetal development Pain Gastric pain Ease childbirth (accelerate labor) Promote the production of breast milk Prevent vomiting | Oral | 0.016 | 0.019 |
| Petroselinum crispum (Mill.) Fuss | Parsley | Raw Decoction | Childbirth TR2, TR3 Postpartum | Promote the production of breast milk Prevention and treatment of genital infections | Oral Vaginal | 0.004 | 0.005 |
| Ammodaucus leucotrichus Coss. Durieu | Hairy cumin or woolly cumin | Infusion Raw Powder | Childbirth TR1, TR2, TR3 | Intestinal bloating Urinary burns Pain Gastric pain Ease childbirth (accelerate labor) Indigestion Induce labor (induction) Prevention and treatment of genital infections Cold/flu/cough Stress/anxiety | Oral | 0.042 | 0.027 |
| Carum carvi L. | Caraway | Infusion | Throughout pregnancy Postpartum | Vaginal itching/pruritus Promote the production of breast milk | Oral Vaginal | 0.002 | 0.005 |
| Cuminum cyminum L. | Cumin | Infusion Raw Powder | Childbirth TR1, TR2, TR3 | Intestinal bloating Heartburn (heartburn) Constipation Diarrhea Pain Gastric pain Prevent miscarriages Ease childbirth (accelerate labor) Promote the production of breast milk Stress/anxiety Vomiting | Oral | 0.029 | 0.032 |
| Daucus carota L. | Carrot | Fumigation Decoction | Childbirth | Ease childbirth (accelerate labor) | Vaginal Oral | 0.001 | 0.003 |
| Pimpinella anisum L. | Green anise | Maceration | Childbirth TR1 | Anemia Intestinal bloating Good fetal development Constipation Gastric pain Ease childbirth (accelerate labor) | Oral | 0.006 | 0.016 |
| Asteraceae | |||||||
| Artemisia herba-alba Asso | White mugwort | Infusion Decoction Fumigation Raw Maceration | Childbirth TR1, TR2, TR3 Postpartum | Intestinal bloating Heartburn (heartburn) Urinary burns Constipation Vaginal itching/pruritus Pain Gastric pain Prevent bleeding Prevent caesarean section Ease childbirth (accelerate labor) Promote the production of breast milk Induce labor (induction) Uterine involution Loss of appetite Prevention and treatment of gestational diabetes Prevention and treatment of genital infections Cold/flu/cough Episiotomy care Treat high blood pressure (toxemia of pregnancy) Vomiting | Vaginal Oral Nasal | 0.195 | 0.059 |
| Artemisia absinthium L. | Absinthe | Infusion Decoction | TR1, TR2, TR3 Postpartum | Pain Ease childbirth (accelerate labor) Stress/anxiety | Oral | 0.014 | 0.008 |
| Atractylis gummifera L. | Slime thistle | Powder | TR3 | Pain | Oral | 0.001 | 0.003 |
| Matricaria chamomilla L. | Chamomile | Infusion Decoction | TR1 | Pain Gastric pain Stress/anxiety | Oral | 0.005 | 0.008 |
| Brassicaceae | |||||||
| Lepidium sativum L. | Garden cress | Infusion Maceration Raw Decoction | Childbirth TR1, TR2, TR3 Postpartum | Anemia Intestinal bloating Pain Prevent bleeding Ease childbirth (accelerate labor) Promote the production of breast milk Induce labor (induction) Uterine involution Loss of appetite Prevention and treatment of genital infections Weight gain Cold/flu/cough | Oral | 0.067 | 0.035 |
| Burseraceae | |||||||
| Commiphora myrrha (Nees) Engl. | Myrrh | Fumigation | Childbirth TR3 | Ease childbirth (accelerate labor) | Vaginal | 0.002 | 0.003 |
| Boswelliasp. | Frankincense | Fumigation | Childbirth | Ease childbirth (accelerate labor) | Vaginal | 0.001 | 0.003 |
| Chenopodiaceae | |||||||
| Dysphania ambrosioides (L.) Mosyakin and Clemants | Anserine | Maceration Decoction Infusion Powder | TR2, TR3 | Fever | Dermal Oral | 0.005 | 0.003 |
| Cupressaceae | |||||||
| Juniperus communis L. | Juniper | Decoction | Postpartum | Uterine involution | Dermal Vaginal | 0.006 | 0.003 |
| Fabaceae | |||||||
| Trigonella foenum-graecum L. | Fenugreek | Decoction Infusion Maceration Raw Powder | Childbirth TR1, TR2, TR3 Postpartum | Anemia Heartburn Pain Gastric pain Ease childbirth (accelerate labor) Promote the production of breast milk Induce labor (induction) Uterine involution Loss of appetite Prevention and treatment of gestational diabetes Prevention and treatment of genital infections Weight gain Cold/flu/cough Vomiting | Oral | 0.081 | 0.037 |
| Vicia faba L. | Bean | Decoction | TR1, TR2 | Anemia Heartburn (heartburn) | Oral | 0.002 | 0.005 |
| Cicer arietinum L. | Chickpea | Decoction | TR1 | Anemia Heartburn (heartburn) | Oral | 0.002 | 0.005 |
| Lens culinaris L. | Lentil | Raw | TR1 | Anemia Loss of appetite | Oral | 0.002 | 0.005 |
| Iridaceae | |||||||
| Crocus sativus L. | Safran | Infusion Decoction Raw | Childbirth TR2, TR3 | Intestinal bloating Pain Ease childbirth (accelerate labor) Stress/anxiety | Oral | 0.021 | 0.011 |
| Lamiaceae | |||||||
| Lavandula angustifolia Mill. | Lavender | Infusion Fumigation Decoction | Childbirth TR1, TR2, TR3 | Good fetal development Urinary burns Pain Gastric pain Induce labor (induction) Uterine involution Prevention and treatment of genital infections Cold/flu/cough Episiotomy care | Oral Vaginal Nasal Rectal | 0.022 | 0.024 |
| Rosmarinus officinalis L. | Rosemary | Decoction Infusion | Childbirth Throughout pregnancy TR1, TR2, TR3 | Pain Ease childbirth (accelerate labor) Induce labor (induction) Prevention and treatment of genital infections Cold/flu/cough Stress/anxiety | Oral Nasal | 0.026 | 0.019 |
| Salvia officinalis L. | Common sage | Decoction Infusion | TR1, TR3 | Good fetal development Pain Hormonal balance | Oral | 0.005 | 0.008 |
| Thymus maroccanus Ball. | Thyme | Infusion Decoction Raw | Childbirth TR1, TR2, TR3 Postpartum | Anemia Angina Intestinal bloating Good fetal development Constipation Pain Gastric pain Avoid perineal tears Ease childbirth (accelerate labor) Indigestion Induce labor (induction) Prevention and treatment of genital infections Cold/flu/cough Stress/anxiety Treat high blood pressure (toxemia of pregnancy) Vomiting | Oral Nasal Vaginal | 0.153 | 0.045 |
| Mentha pulegium L. | Pennyroyal mint | Infusion | TR1, TR2 | Cold/flu/cough | Oral | 0.004 | 0.005 |
| Lauraceae | |||||||
| Cinnamomum verum J. Presl | Cinnamon | Powder Decoction Infusion Maceration | Childbirth TR1, TR2, TR3 Postpartum | Anemia Urinary burns Pain Prevent bleeding Ease childbirth (accelerate labor) Promote the production of breast milk Induce labor (induction) Sore throat Prevention and treatment of genital infections Cold/flu/cough | Oral | 0.019 | 0.027 |
| Linaceae | |||||||
| Linum usitatissimum L. | Lin | Powder Infusion | Childbirth TR1, TR2, TR3 Postpartum | Anemia Good fetal development Pain Promote the production of breast milk Indigestion Loss of appetite | Oral | 0.008 | 0.016 |
| Myrtaceae | |||||||
| Syzygium aromaticum (L.) Merr. and Perry | Clove | Maceration Infusion Decoction Raw | TR1, TR2, TR3 Throughout pregnancy | Good fetal development Pain Gingival bleeding Induce labor (induction) Sore throat Prevention and treatment of genital infections Cold/flu/cough | Oral Nasal | 0.016 | 0.019 |
| Oleaceae | |||||||
| Olea europaea L. | Olive | Decoction Infusion Nature | Childbirth TR1, TR2, TR3 | Anemia Intestinal bloating Constipation Vaginal itching/pruritus Pain Prevent perineal tears Ease childbirth (accelerate labor) Loss of appetite Cold/flu/cough Stretch marks | Oral Vaginal Dermal | 0.040 | 0.027 |
| Palmaceae | |||||||
| Phoenix dactylifera L. | Date | Raw | TR1, TR2 | Urinary burns Loss of appetite | Oral | 0.002 | 0.005 |
| Pedaliaceae | |||||||
| Sesamum indicum L. | Sesame | Powder Decoction Raw | Childbirth TR1, TR2, TR3 Postpartum | Anemia Good fetal development Constipation Gastric pain Prevent bleeding Promote the production of breast milk Loss of appetite Weight gain | Oral | 0.041 | 0.021 |
| Poaceae | |||||||
| Pennisetum typhoides (Burm.f.) Stapf. and C.E. Hubb. | Candle millet | Powder | TR1, TR2 | Anemia Good fetal development Loss of appetite | Oral | 0.003 | 0.008 |
| Ranunculaceae | |||||||
| Nigella sativa L. | Nigella | Powder Decoction | Childbirth TR1, TR3 | Good fetal development Pain Ease childbirth (accelerate labor) Induce labor (induction) Weight gain Cold/flu/cough | Oral | 0.011 | 0.016 |
| Rhamnaceae | |||||||
| Ziziphus lotus (L.) Lam. | Jujube | Infusion | TR1 | Pain | Oral | 0.001 | 0.003 |
| Verbenaceae | |||||||
| Aloysia citriodora Palau | Verbena | Infusion Decoction | Childbirth TR1, TR2, TR3 Postpartum | Good fetal development Constipation Pain Gastric pain Eliminate intestinal gas in infants Ease childbirth (accelerate labor) Insomnia Uterine involution Cold/flu/cough Stress/anxiety Treat high blood pressure (toxemia of pregnancy) Vertigo Vomiting | Oral | 0.097 | 0.037 |
| Vitex agnus-castus L. | Chaste berry | Decoction Infusion | Childbirth | Ease childbirth (accelerate labor) | Oral | 0.006 | 0.003 |
| Zingiberaceae | |||||||
| Aframomum melegueta (Roscoe) K. Schum. | Maniguette | Infusion | Childbirth TR3 | Ease childbirth (accelerate labor) | Oral | 0.001 | 0.003 |
| Zingiber officinale Roscoe | Ginger | Decoction Infusion | Childbirth TR1, TR3 | Vaginal itching/pruritus Pain Induce labor (induction) Cold/flu/cough | Oral | 0.006 | 0.011 |
| Zygophyllaceae | |||||||
| Peganum harmala L. | Harmel | Fumigation Decoction | Childbirth TR1, TR3 Throughout pregnancy | Pain Ease childbirth (accelerate labor) Induce labor (induction) Cold/flu/cough | Nasal Vaginal | 0.011 | 0.011 |
| Application | At Birth % | Postpartum % | TR1% | TR2% | TR3% | Total % |
|---|---|---|---|---|---|---|
| Dermal | 0.20 | 0 | 0 | 1.82 | 0.40 | 2.43 |
| Nasal | 0.20 | 0 | 1.82 | 0.91 | 0.91 | 3.84 |
| Oral | 15.57 | 4.85 | 22.65 | 16.48 | 13.65 | 73.21 |
| Vaginal | 12.74 | 0.20 | 4.65 | 0.71 | 2.22 | 20.53 |
| Total | 28.72 | 5.06 | 29.12 | 19.92 | 17.19 | 100 |
| Mode of Preparation | At Birth % | Immediate Postpartum % | TR1% | TR2% | TR3% | Total % |
|---|---|---|---|---|---|---|
| Decoction | 8.76 | 0.20 | 10.26 | 9.56 | 6.08 | 34.86 |
| Fumigation | 3.69 | 0 | 1.99 | 0.70 | 0.70 | 7.07 |
| Infusion | 10.66 | 4.18 | 8.37 | 1.99 | 6.08 | 31.27 |
| Maceration | 0.10 | 0.10 | 0.60 | 0.20 | 0.10 | 1.10 |
| Raw | 2.19 | 0.50 | 6.27 | 5.98 | 3.39 | 18.33 |
| Unidentified | 3.09 | 0 | 0 | 0.10 | 0.10 | 3.29 |
| Powder | 1.39 | 0 | 1.10 | 1.10 | 0.50 | 4.08 |
| Total | 29.88 | 4.98 | 28.59 | 19.62 | 16.93 | 100 |
| Source of Information | At Birth % | Pregnancy % | Postpartum % | Total % |
|---|---|---|---|---|
| Family | 19 | 23 | 4 | 46 |
| Friends and neighbors | 15 | 16 | 3 | 34 |
| Herbalists | 1 | 2 | 1 | 4 |
| Internet | 1 | 1 | 0 | 3 |
| Health professional | 2 | 3 | 1 | 6 |
| TV media | 1 | 3 | 1 | 6 |
| Total | 41 | 49 | 10 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamel, N.; El Boullani, R.; Cherrah, Y. Use of Medicinal Plants during Pregnancy, Childbirth and Postpartum in Southern Morocco. Healthcare 2022, 10, 2327. https://doi.org/10.3390/healthcare10112327
Kamel N, El Boullani R, Cherrah Y. Use of Medicinal Plants during Pregnancy, Childbirth and Postpartum in Southern Morocco. Healthcare. 2022; 10(11):2327. https://doi.org/10.3390/healthcare10112327
Chicago/Turabian StyleKamel, Nadia, Rachida El Boullani, and Yahia Cherrah. 2022. "Use of Medicinal Plants during Pregnancy, Childbirth and Postpartum in Southern Morocco" Healthcare 10, no. 11: 2327. https://doi.org/10.3390/healthcare10112327