
Pharmacist Preceptor Exposure, Comfort and Awareness of Resources to Address the Social Determinants of Health—A Pilot Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
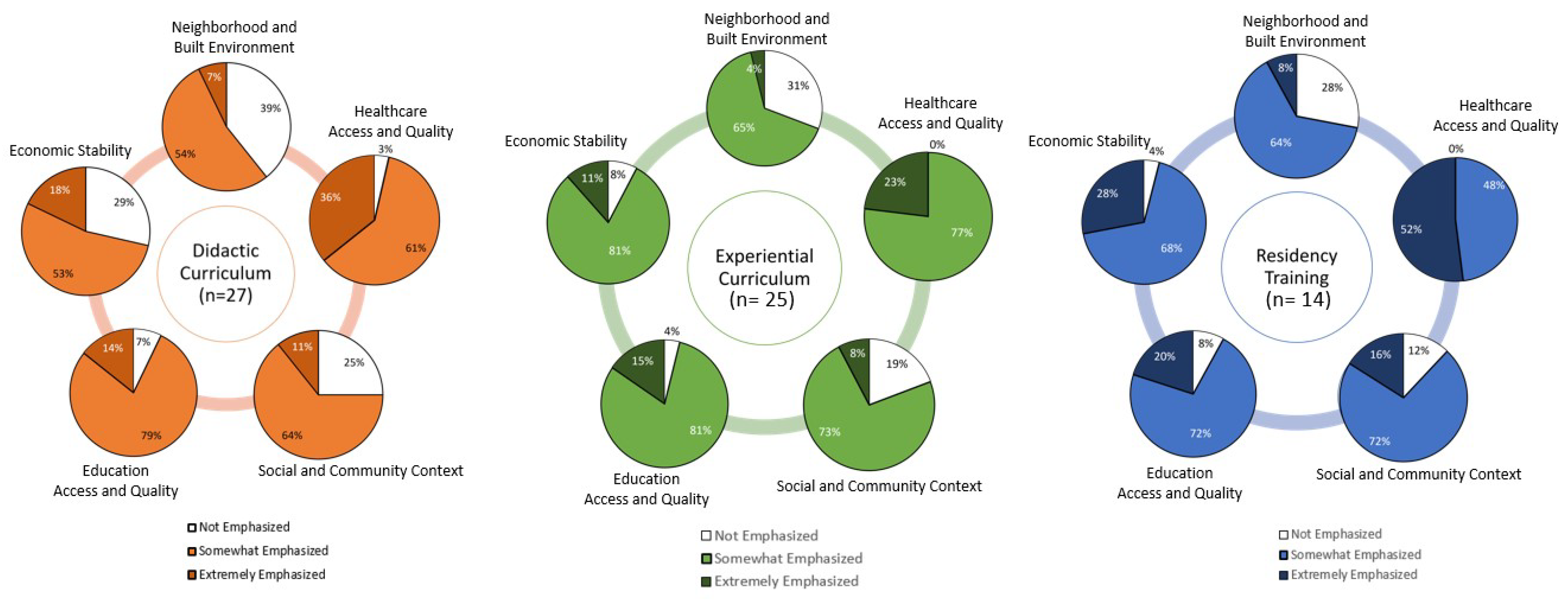
3.1. Exposure to Social Determinants of Health in Pharmacy Education
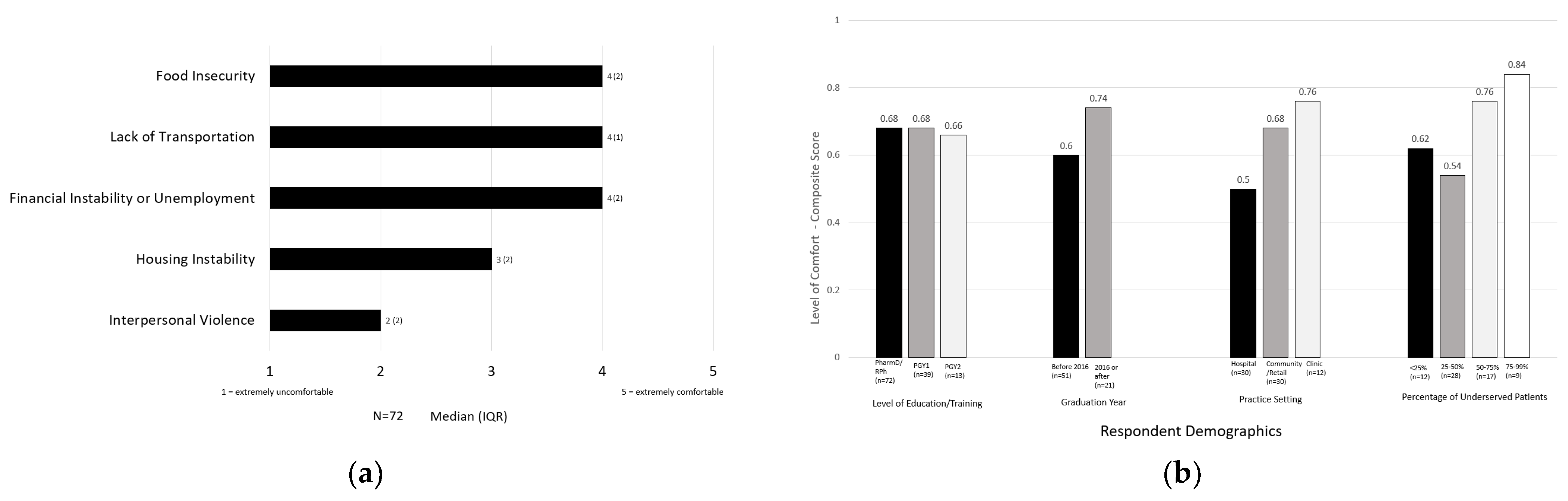
3.2. Comfort Addressing Social Needs
3.3. Awareness of Social Resources
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Item | Awareness Level | Aggregate n (%) | Graduation Year | Practice Setting | % Underserved | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Before 2016 n (%) | After 2016 n (%) | Hospital n (%) | Community/Retail n (%) | Clinic n (%) | <25% n (%) | 25–50% n (%) | 50–75% n (%) | 75–100% n (%) | |||
| Prescription cost assistance | Not at all aware | 3 (4.2) | 3 (5.9) | 0 0.0) | 1 (3.3) | 2 (6.7) | 0 (0.0) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 0 (0.0) |
| Somewhat aware | 19 (26.4) | 15 (29.4) | 4 (19.0) | 9 (30.0) | 8 (26.7) | 2 (16.7) | 5 (41.7) | 9 (33.3) | 3 (17.6) | 0 (0.0) | |
| Very aware | 50 (69.4) | 33 (64.7) | 17 (81.0) | 20 (66.7) | 20 (66.7) | 10 (83.3) | 7 (58.3) | 17 (63.0) | 14 (82.4) | 9 (100.0) | |
| Healthcare Access | Not at all aware | 4 (5.6) | 4 (7.8) | 0 (0.0) | 1 (3.3) | 3 (10.0) | 0 (0.0) | 1 (8.3) | 1 (3.7) | 0 (0.0) | 0 (0.0) |
| Somewhat aware | 34 (47.2) | 26 (51.0) | 8 (38.1) | 17 (56.7) | 14 (46.7) | 3 (25.0) | 6 (50.0) | 15 (55.6) | 8 (47.1) | 2 (22.2) | |
| Very aware | 34 (47.2) | 21 (41.2) | 13 (61.9) | 12 (40.0) | 13 (43.3) | 9 (75.0) | 5 (41.7) | 11 (40.7) | 9 (52.9) | 7 (77.7) | |
| Access to healthy food | Not at all aware | 21 (29.20 | 15 (29.4) | 6 (28.6) | 14 (46.7) | 7 (23.3) | 0 (0.0) | 2 (16.7) | 12 (44.4) | 4 (23.5) | 2 (22.2) |
| Somewhat aware | 35 (48.6) | 28 (54.9) | 7 (33.3) | 14 (46.7) | 11 (36.7) | 10 (83.3) | 8 (66.7) | 10 (37.0) | 7 (41.2) | 4 (44.4) | |
| Very aware | 16 (22.2) | 8 (15.7) | 8 (38.1) | 2 (6.7) | 12 (0.0) | 2 (16.7) | 2 (16.7) | 5 (18.5) | 6 (35.3) | 3 (33.3) | |
| Housing assistance | Not at all aware | 31 (43.1) | 24 (47.1) | 7 (33.3) | 17 (56.7) | 11 (36.7) | 3 (25.0) | 5 (41.7) | 14 (51.9) | 6 (35.3) | 2 (22.2) |
| Somewhat aware | 30 (41.7) | 22 (43.1) | 8 (38.1) | 11 (36.7) | 12 (40.0) | 7 (58.3) | 6 (50.0) | 9 (33.3) | 7 (41.2) | 5 (55.5) | |
| Very aware | 11 (15.3) | 5 (9.8) | 6 (28.6) | 2 (6.7) | 7 (23.3) | 2 (16.7) | 1 (8.3) | 4 (14.8) | 4 (23.5) | 2 (22.2) | |
| Transportation assistance | Not at all aware | 14 (19.4) | 11 (21.6) | 3 (14.3) | 9 30.0) | 5 (16.7) | 0 (0.0) | 3 (25.0) | 7 (25.9) | 0 (0.0) | 2 (22.2) |
| Somewhat aware | 44 (61.1) | 32 (62.7) | 12 (57.1) | 19 (63.3) | 16 (53.3) | 9 (75.0) | 8 (66.7) | 17 (63.0) | 12 (70.6) | 3 (33.3) | |
| Very aware | 14 (19.4) | 8 (15.7) | 6 (28.6) | 2 (6.7) | 9 (30.0) | 3 (25.0) | 1 (8.3) | 3 (11.1) | 5 (29.4) | 4 (44.4) | |
| Access to training and educational advancement | Not at all aware | 35 (48.6) | 27 (52.9) | 8 (38.1) | 19 (63.3) | 9 (30.0) | 7 (58.3) | 5 (41.7) | 17 (63.0) | 6 (35.3) | 2 (22.2) |
| Somewhat aware | 24 (33.3) | 16 (31.4) | 8 (38.1) | 8 (26.7) | 14 (46.7) | 2 (16.7) | 6 (50.0) | 8 (29.6) | 6 (35.3) | 2 (22.2) | |
| Very aware | 13 (18.1) | 8 (15.7) | 5 (23.8) | 3 (10.0) | 7 (23.3) | 3 (25.0) | 1 (8.3) | 2 (7.4) | 5 (29.4) | 5 (55.5) | |
| Employment resources | Not at all aware | 34 (47.2) | 26 (51.0) | 8 (38.1) | 18 (60.0) | 11 (36.7) | 5 (41.7) | 7 (58.3) | 13 (48.1) | 8 (47.1) | 2 (22.2) |
| Somewhat aware | 29 (40.3) | 20 (39.2) | 9 (42.9) | 11 (36.7) | 13 (43.3) | 5 (41.7) | 5 (41.7) | 11 (40.7) | 5 (29.4) | 5 (55.5) | |
| Very aware | 9 (12.5) | 5 (9.8) | 4 (19.0) | 1 (3.3) | 6 (20.0) | 2 (16.7) | 0 (0.0) | 3 (11.1) | 4 (23.5) | 2 (22.2) | |
| Legal assistance | Not at all aware | 43 (59.7) | 31 (60.8) | 12 (57.1) | 23 (76.7) | 12 (40.0) | 8 (66.7) | 7 (58.3) | 19 (70.4) | 9 (52.9) | 5 (55.5) |
| Somewhat aware | 20 (27.8) | 15 (29.4) | 5 (23.8) | 6 (20.0) | 11 (36.7) | 3 (25.0) | 4 (33.3) | 5 (18.5) | 4 (23.5) | 3 (33.3) | |
| Very aware | 9 (12.5) | 5 (9.8) | 4 (19.0) | 1 (3.3) | 7 (23.3) | 1 (8.3) | 1 (8.3) | 3 (11.1) | 4 (23.5) | 1 (11.1) | |
| Translation services/ Language assistance | Not at all aware | 16 (22.2) | 12 (23.5) | 4 (19.0) | 7 (23.3) | 8 (26.7) | 1 (8.3) | 1 (8.3) | 9 (33.3) | 2 (11.8) | 3 (33.3) |
| Somewhat aware | 35 (48.6) | 24 (47.1) | 11 (52.4) | 16 (53.3) | 14 (46.7) | 5 (41.7) | 9 (75.0) | 13 (48.1) | 6 (35.3) | 2 (22.2) | |
| Very aware | 21 (29.2) | 15 (29.4) | 6 (28.6) | 7 (23.3) | 8 (26.7) | 6 (50.0) | 2 (16.7) | 5 (18.5) | 9 (52.9) | 4 (44.4) | |
| Environmental safety | Not at all aware | 36 (50.0) | 28 (54.9) | 8 (38.1) | 19 (63.3) | 12 (40.0) | 5 (41.7) | 4 (33.3) | 18 (66.7) | 8 (47.1) | 4 (44.4) |
| Somewhat aware | 29 (40.3) | 19 (37.3) | 10 (47.6) | 10 (33.3) | 13 (43.3) | 6 (50.0) | 8 (66.7) | 7 (25.9) | 5 (29.4) | 4 (44.4) | |
| Very aware | 7 (9.7) | 4 (7.8) | 3 (14.3) | 1 (3.3) | 5 (16.7) | 1 (8.3) | 0 (0.0) | 2 (7.4) | 4 (23.5) | 1 (11.1) | |
| Social/community engagement | Not at all aware | 30 (41.7) | 22 (43.1) | 8 (38.1) | 18 (60.0) | 7 (23.3) | 5 (41.7) | 4 (33.3) | 13 (48.1) | 8 (47.1) | 4 (44.4) |
| Somewhat aware | 33 (45.8) | 24 (47.1) | 9 (42.9) | 11 (36.7) | 17 (56.7) | 5 (41.7) | 7 (58.3) | 12 (44.4) | 5 (29.4) | 3 (33.3) | |
| Very aware | 9 (12.5) | 5 (9.8) | 4 (19.0) | 1 (3.3) | 6 (20.0) | 2 (16.7) | 1 (8.3) | 2 (7.4) | 4 (23.5) | 2 (22.2) | |
References
- Centers for Disease Control and Prevention. Social Determinants of Health at CDC. Available online: https://www.cdc.gov/about/sdoh/index.html (accessed on 27 February 2023).
- Healthy People 2030, U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Available online: https://health.gov/healthypeople/priority-areas/social-determinants-healthhtml (accessed on 27 February 2023).
- World Health Organization. Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1. (accessed on 4 May 2023).
- Hood, C.M.; Gennuso, K.P.; Swain, G.R.; Catlin, B.B. County health rankings: Relationships between determinant factors and health outcomes. Am. J. Prev. Med. 2016, 50, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Kiles, T.M.; Peroulas, D.; Borja-Hart, N. Defining the role of pharmacists in addressing the social determinants of health. Res. Soc. Admin. Pharm. 2022, 18, 3699–3703. [Google Scholar] [CrossRef] [PubMed]
- Accreditation Council for Pharmacy Education Standards 2016. Available online: https://www.acpe-accredit.org/pdf/Standards2016FINAL.pdf (accessed on 27 February 2023).
- Medina, M.S.; Plaza, C.M.; Stowe, C.D.; Robinson, E.T.; DeLander, G.; Beck, D.E.; Melchert, R.B.; Supernaw, R.B.; Roche, V.F.; Gleason, B.L.; et al. Center for the Advancement of Pharmacy Education (CAPE) 2013 Educational Outcomes. Am. J. Pharm. Educ. 2013, 77, 162. [Google Scholar] [CrossRef] [PubMed]
- Butler, L.M.; Arya, V.; Nonyel, N.P.; Moore, T.S. The Rx-HEART Framework to Address Health Equity and Racism Within Pharmacy Education. Am. J. Pharm. Educ. 2021, 85, 8590. [Google Scholar] [CrossRef] [PubMed]
- Sheaffer, S.; DeRemer, C.; Yam, N. Precepting Fundamentals. Preceptors Handbook for Pharmacists, Third Edition. Chapter 1. Available online: https://www.ashp.org/-/media/store-files/p4955-sample-chapter-1.ashx (accessed on 27 February 2023).
- Chen, A.M.H.; Armbruster, A.L.; Buckley, B.; Campbell, J.A.; Dang, D.K.; Devraj, R.; Drame, I.; Edwards, A.; Haack, S.L.; Ma, Q.; et al. Health disparities, cultural competence, and health literacy content integration in U.S. and Canadian pharmacy curricula. Am. J. Pharm. Educ. 2020, 84, 8200. [Google Scholar] [CrossRef] [PubMed]
- Rockich-Winston, N.; Wyatt, T.R. The Case for Culturally Responsive Teaching in Pharmacy Curricula. Am. J. Pharm. Educ. 2019, 83, 7425. [Google Scholar] [CrossRef] [PubMed]
- Avant, N.D.; Gillespie, G.L. Pushing for health equity through structural competency and implicit bias education: A qualitative evaluation of a racial/ethnic health disparities elective course for pharmacy learners. Curr. Pharm. Teach. Learn. 2019, 11, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Schickedanz, A.; Hamity, C.; Rogers, A.; Sharp, A.L.; Jackson, A. Clinician experiences and attitudes regarding screening for social determinants of health in a large integrated health system. Med. Care 2019, 57 (Suppl. 6), S197–S201. [Google Scholar] [CrossRef] [PubMed]
- Kiles, T.M.; Chen, C.; Leibold, C.; Cardosi, L.; Hill, H.; Hohmeier, H. Pharmacy Personnel Comfort and Confidence in Screening for Social Needs—A Pilot Study. J. Am. Pharm. Assoc. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Minshew, L.M.; Williams, C.; White, C.; Fassett, K.T.; McLaughlin, J.E. Investigating preceptor experiences with cultural intelligence in pharmacy education. Res. Soc. Adm. Pharm. 2023, 19, 622–627. [Google Scholar] [CrossRef] [PubMed]
- American Pharmacists Association House of Delegates: Social Determinants of Health. Available online: https://www.pharmacist.com/Portals/0/PDFS/HOD/NBI%207%20-%20Social%20Determinants%20of%20Health_1.pdf?ver=ZPyZUI7fbpvE0kS8PYc_Vw%3D%3D (accessed on 27 February 2023).
- Pharmacy Quality Alliance. PQA Social Determinants of Health Resources Guide. Available online: https://www.pqaalliance.org/sdoh-resource-guide (accessed on 27 February 2023).
- Kiles, T.; Jasmin, H.; Nichols, B.; Haddad, R.; Renfro, C.P. A Scoping Review of Active-Learning Strategies for Teaching Social Determinants of Health in Pharmacy. Am. J. Pharm. Educ. 2020, 84, 8241. [Google Scholar] [CrossRef] [PubMed]
- DiPiro, J.T.; Allen, D.D.; Lin, A.; Scott, S.A.; Sorensen, T.D.; Maine, L.L. Impact of Social Forces and Environmental Factors on Healthcare and Pharmacy Education: The Report of the 2021–2022 AACP Argus Commission. Am. J. Pharm. Educ. 2023, 87, ajpe9452. [Google Scholar] [CrossRef] [PubMed]
- Rahman, H.; Maerten-Rivera, J.L.; Woodruff, A.E.; Prescott, G.M. Students’ knowledge and perceptions of social determinants of health utilizing interactive computer simulation-based learning. Curr. Pharm. Teach. Learn. 2022, 14, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Cernasev, A.; Shofoluwe, A.; Odum, K.; Havrda, D.E. Empowering Student Pharmacists through Social Determinants of Health Activities to Address Patient Outcomes. Pharmacy 2022, 10, 176. [Google Scholar] [CrossRef] [PubMed]
- Crowl, A.N.; Wellner, Z.; Levy, M.; Boyd, C.; Bates, J.; Barnes, J.; Shrader, S. Determining the impact of an interprofessional simulation focused on social determinants of health among pharmacy students. Curr. Pharm. Teach. Learn. 2021, 13, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Artiga, S.; Hinton, E. Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity. Social Determinants of Health. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/ (accessed on 27 February 2023).
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Boynton-Jarrett, R.; Dworkin, P.H. Avoiding the Unintended Consequences of Screening for Social Determinants of Health. JAMA 2016, 316, 813–814. [Google Scholar] [CrossRef] [PubMed]
- Richter, L.M.; Monson, E.; Bye, K.; Frenzel, J.E. Design and Assessment of a Pharmacy Student-Delivered Preceptor Development Program. Am. J. Pharm. Educ. 2023, 87, ajpe8939. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, C.; Natsheh, C.; Leblanc, K.; Fernandes, O.; Mejia, A.B.; Raman-Wilms, L.; Cameron, K. An Analysis of Canadian Doctor of Pharmacy Student Experiences in Non-Traditional Student-Preceptor Models. Am. J. Pharm. Educ. 2019, 83, 7367. [Google Scholar] [CrossRef] [PubMed]
- Our Changing Population: Tennesee. USA Facts.org. Available online: https://usafacts.org/data/topics/people-society/population-and-demographics/our-changing-population/state/tennessee (accessed on 12 April 2023).
- Islam, M.M. Social Determinants of Health and Related Inequalities: Confusion and Implications. Front. Public Health 2019, 7, 11. [Google Scholar] [CrossRef] [PubMed]



| Age, n (%) | All (n = 72) |
|---|---|
| 25–39 years old | 50 (69.4) |
| 40–59 years old | 21 (29.2) |
| >60 years old | 1 (1.4) |
| Gender, n (%) | |
| Female | 52 (72.2) |
| Male | 19 (26.4) |
| Prefer not to disclose | 1 (1.4) |
| Race/Ethnicity, n (%) | |
| White/Caucasian | 62 (86.1) |
| Black/African American | 4 (5.6) |
| Asian/Pacific Islander | 2 (2.8) |
| Multiracial | 2 (2.8) |
| Prefer not to disclose | 2 (2.8) |
| Graduation Year, n (%) | |
| Before 2016 | 51 (70.8) |
| After 2016 | 21 (29.2) |
| Level of Education/Training, n (%) | |
| PharmD, RPh | 72 (100.0) |
| PGY1 Residency * | 39 (50.0) |
| PGY2 Residency * | 14 (19.4) |
| Practice Area, n (%) | |
| Community or Retail | 30 (41.7) |
| Hospital | 30 (41.7) |
| Clinic | 12 (16.7) |
| Percent of Underserved Patients, n (%) | |
| <25% Underserved | 12 (16.7) |
| 25–50% Underserved | 27 (37.5) |
| 50–75% Underserved | 17 (23.6) |
| 75–100% Underserved | 9 (12.5) |
| Unspecified | 7 (9.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiles, T.M.; Kodweis, K.R.; George, C.; Watts, C.D.; Lock, A.; Crill, C. Pharmacist Preceptor Exposure, Comfort and Awareness of Resources to Address the Social Determinants of Health—A Pilot Study. Pharmacy 2023, 11, 83. https://doi.org/10.3390/pharmacy11030083
Kiles TM, Kodweis KR, George C, Watts CD, Lock A, Crill C. Pharmacist Preceptor Exposure, Comfort and Awareness of Resources to Address the Social Determinants of Health—A Pilot Study. Pharmacy. 2023; 11(3):83. https://doi.org/10.3390/pharmacy11030083
Chicago/Turabian StyleKiles, Tyler Marie, Karl R. Kodweis, Christa George, Chelsea Danielle Watts, Adalis Lock, and Catherine Crill. 2023. "Pharmacist Preceptor Exposure, Comfort and Awareness of Resources to Address the Social Determinants of Health—A Pilot Study" Pharmacy 11, no. 3: 83. https://doi.org/10.3390/pharmacy11030083