
Medication Dispensing by Pharmacy Technicians Improves Efficiency and Patient Safety at a Geriatric Ward at a Danish Hospital: A Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
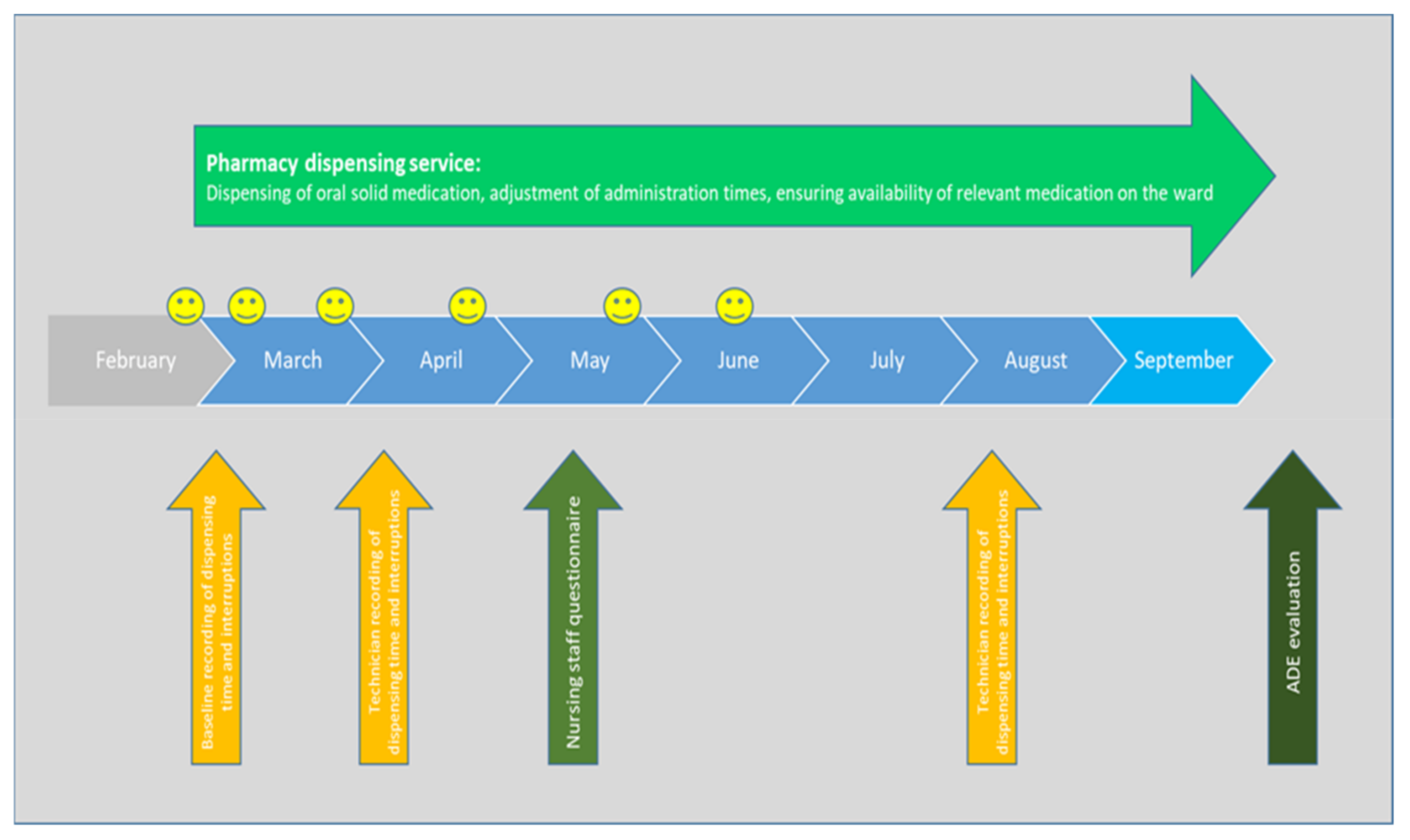
2.1. Pharmacy Dispensing Service
2.2. Dispensing Time and Interruptions
2.3. Medication Errors
2.4. Questionnaire for Nursing Staff
3. Results
3.1. Time Used at Dispensing Medication
3.2. Interruptions While Dispensing Medication
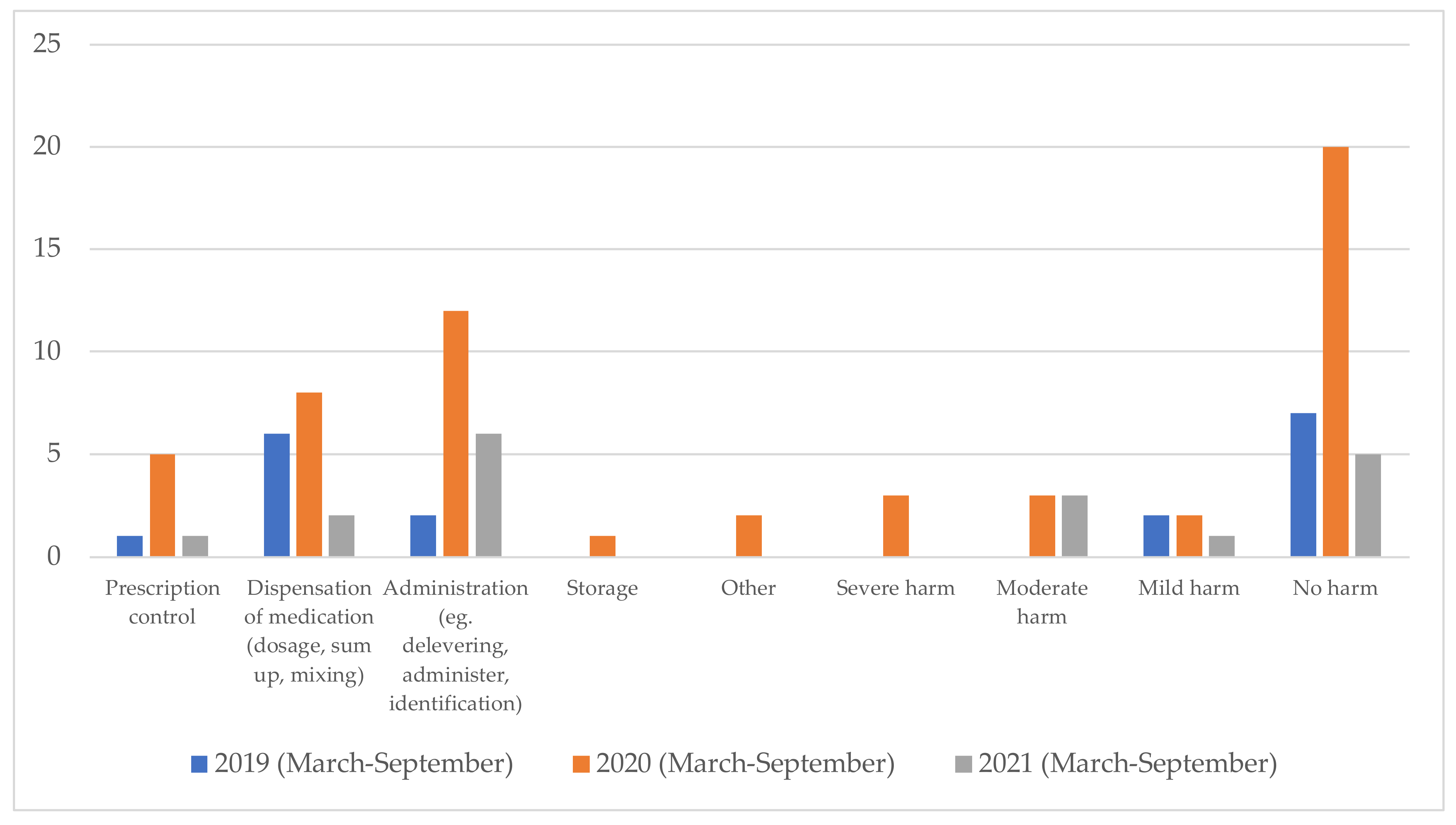
3.3. Reports of Medication Errors and Severity of Harm Caused by Medication Error
3.4. Questionnaire for the Nursing Staff
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Medication Errors; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/252274 (accessed on 2 May 2022).
- World Health Organization. Medication Safety in High-Risk Situations; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/handle/10665/325131 (accessed on 2 May 2022).
- Keers, R.N.; Williams, S.D.; Cooke, J.; Ashcroft, D.M. Causes of medication administration errors in hospitals: A systematic review of quantitative and qualitative evidence. Drug Saf. 2013, 36, 1045–1067. [Google Scholar] [CrossRef] [PubMed]
- Cloete, L. Reducing medication errors in nursing practice. Nurs. Stand. 2015, 29, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Elganzouri, E.S.; Standish, C.A.; Androwich, I. Medication Administration Time Study (MATS): Nursing staff performance of medication administration. J. Nurs. Adm. 2009, 39, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Leape, L.L.; Bates, D.W.; Cullen, D.J.; Cooper, J.; Demonaco, H.J.; Gallivan, T.; Hallisey, R.; Ives, J.; Laird, N.; Laffel, G.; et al. Systems analysis of adverse drug events. JAMA 1995, 274, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Salar, A.; Kaini, F.; Rezaee, N. Preventing the medication errors in hospitals: A qualitative study. Int. J. Afr. Nurs. Sci. 2020, 13, 5. [Google Scholar] [CrossRef]
- Palese, A.; Sartor, A.; Costaperaria, G.; Bresadola, V. Interruptions during nurses’ drug rounds in surgical wards: Observational study. J. Nurs. Manag. 2009, 17, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Huckels-Baumgart, S.; Baumgart, A.; Buschmann, U.; Schüpfer, G.; Manser, T. Separate Medication Preparation Rooms Reduce Interruptions and Medication Errors in the Hospital Setting: A Prospective Observational Study. J. Patient Saf. 2021, 17, e161–e168. [Google Scholar] [CrossRef] [PubMed]
- Keohane, C.A.; Bane, A.D.; Featherstone, E.; Hayes, J.; Woolf, S.; Hurley, A.; Bates, D.W.; Gandhi, T.K.; Poon, E.G. Quantifying nursing workflow in medication administration. J. Nurs. Adm. 2008, 38, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Biron, A.D.; Loiselle, C.G.; Lavoie-Tremblay, M. Work interruptions and their contribution to medication administration errors: An evidence review. Worldviews Evid. Based Nurs. 2009, 6, 70–86. [Google Scholar] [CrossRef] [PubMed]
- Seston, E.M.; Ashcroft, D.M.; Lamerton, E.; Harper, L.; Keers, R.N. Evaluating the implementation and impact of a pharmacy technician-supported medicines administration service designed to reduce omitted doses in hospitals: A qualitative study. BMC Health Serv. Res. 2019, 19, 325. [Google Scholar] [CrossRef] [PubMed]
- Indenrigs-og Sundhedsministeriet. Bekendtgørelse Om Rapportering Af Utilsigtede Hændelser i Sundhedsvæsenet m.v.; Vol BEK nr 1 af 03/01/2011. 2011. Available online: https://www.retsinformation.dk/eli/lta/2011/1 (accessed on 20 April 2023).
- Hartwig, S.C.; Denger, S.D.; Schneider, P.J. Severity-indexed, incident report-based medication error-reporting program. Am. J. Hosp. Pharm. 1991, 48, 2611–2616. [Google Scholar] [CrossRef] [PubMed]
- National Coordinating Council for Medication Error Reporting and Prevention. Categorizing Medication Errors. Available online: http://www.nccmerp.org/types-medication-errors (accessed on 20 April 2023).
- Andersen, N.J. Dansk Patientsikkerhedsdatabase Årsberetning 2020; Styrelsen for Patientsikkerhed: Copenhagen, Denmark, 2020; Volume 34. [Google Scholar]
- Mekonnen, A.B.; Redley, B.; de Courten, B.; Manias, E. Potentially inappropriate prescribing and its associations with health-related and system-related outcomes in hospitalised older adults: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2021, 87, 4150–4172. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, H.; Al-Saeed, E.; Ahmed, Z.; Aslanpour, Z. Reviewing Potentially Inappropriate Medication in Hospitalized Patients Over 65 Using Explicit Criteria: A Systematic Literature Review. Drug Healthc. Patient Saf. 2021, 13, 183–210. [Google Scholar] [CrossRef] [PubMed]
- Samlerapportering—Styrelsen for Patientsikkerhed. Available online: https://stps.dk/da/laering/utilsigtede-haendelser/samlerapportering/ (accessed on 2 May 2022).



{kind=link}
{kind=link}
| Nurse (Baseline) (March 2021) | Pharmacy Technician (April 2021) | Pharmacy Technician (August 2021) | |
|---|---|---|---|
| Avg. number of dispensing instances per day | 38.4 (≈2 disp. per ptt) | 16.4 (=number of ptt) | 18.8 (=number of ptt) |
| Prescription review time per day incl. adjustment of time of administration | 0 min | 34 min | 30 min |
| Clarification of missing medication to be obtained 1 | . | 10 min | 12 min |
| Times used at obtaining and verifying medication per day 2 | 60 min | 16 min | 20 min |
| Dispensing time per day | 220.8 min (3.7 h) | 130 min (2.2 h) | 142 min (2.4 h) |
| Total time per day (3) | 280.8 min (4.7 h) | 190 min (3.2 h) | 204 min (3.4 h) |
| Number of interruptions per week | 97 | 15 | 13 |
| Avg. number of interruptions per day | 19.4 | 3.0 | 2.6 |
| Number of interruptions per dispensation per day | 0.5 (i.e., every 2nd disp. ≈ to appr. every ptt) | 0.2 (i.e., every 5th ptt) | 0.14 (i.e., every 7th ptt |
| Statement | Average | Statement | Average |
|---|---|---|---|
| 1. Do you think that the pharmacy has become an integrated part of daily work in the ward? | 4.1 (18) | 2. Have fewer dosing times given more peace of mind in the workflow at the ward? | 4.2 (18) |
| 3. Do you feel safe in administering medicine to patients, even if you have not dispensed it yourself? | 3.9 (18) | 4. Do you think the pharmacy’s work has improved patient safety in the ward? | 3.7 (18) |
| 5. Has the workload in the morning been reduced after the medicine is dispensed by the pharmacy? | 4.5 (18) | 6. Has the workload generally (not only in the morning) been reduced after the medicine is dispensed by the pharmacy? | 4.1 (18) |
| 7. Have you experienced medication errors in relation to the dispensing of the medicine, while the pharmacy has conducted the dispensing? | 1.4 (18) | 8. Do you spend less time to obtaining medicine from other wards? | 4.1 (18) |
| 9. Do you have a better opportunity to spend time with the patients after the medicine is dispensed by the pharmacy? | 4.1 (17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kjeldsen, L.J.; Schlünsen, M.; Meijers, A.; Hansen, S.; Christensen, C.; Bender, T.; Ratajczyk, B. Medication Dispensing by Pharmacy Technicians Improves Efficiency and Patient Safety at a Geriatric Ward at a Danish Hospital: A Pilot Study. Pharmacy 2023, 11, 82. https://doi.org/10.3390/pharmacy11030082
Kjeldsen LJ, Schlünsen M, Meijers A, Hansen S, Christensen C, Bender T, Ratajczyk B. Medication Dispensing by Pharmacy Technicians Improves Efficiency and Patient Safety at a Geriatric Ward at a Danish Hospital: A Pilot Study. Pharmacy. 2023; 11(3):82. https://doi.org/10.3390/pharmacy11030082
Chicago/Turabian StyleKjeldsen, Lene Juel, Maja Schlünsen, Annette Meijers, Steffan Hansen, Camilla Christensen, Tanja Bender, and Barbara Ratajczyk. 2023. "Medication Dispensing by Pharmacy Technicians Improves Efficiency and Patient Safety at a Geriatric Ward at a Danish Hospital: A Pilot Study" Pharmacy 11, no. 3: 82. https://doi.org/10.3390/pharmacy11030082