
Subjective Perceptions of Occupational Fatigue in Community Pharmacists

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Recruitment
2.3. Data Collection
2.4. Data Analysis
3. Results
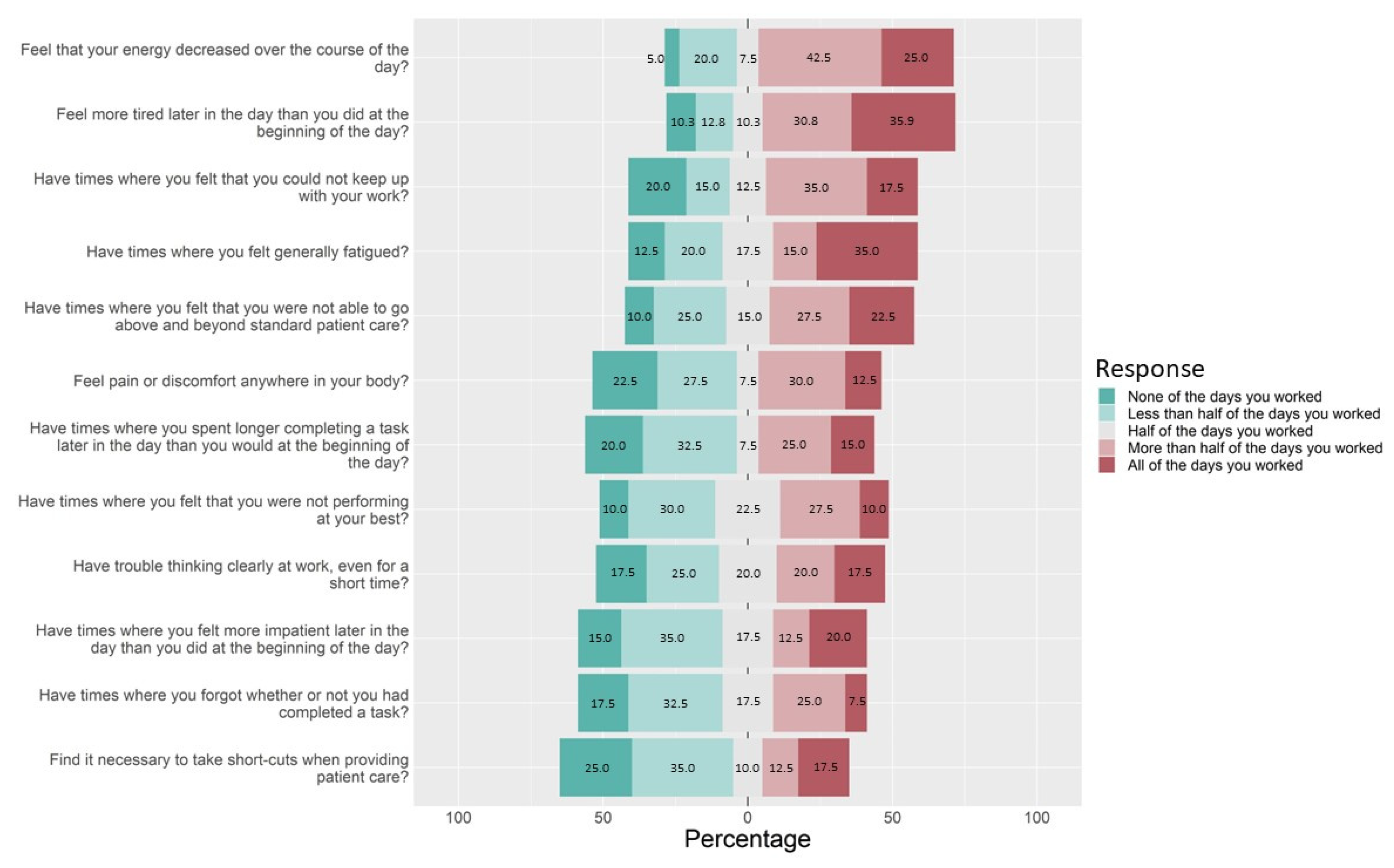
3.1. Pharmacist Fatigue Instrument
3.2. Pharmacist Interviews
3.2.1. Mental Fatigue
You can see a difference in the beginning of the day how we treat customers to the end of the day, which is sad. I don’t ever want to get cranky at customers, but, understandably, they’re losing patience with us since everything’s taking longer, but we’re also losing patience with the fact that they don’t have patience with us. So, admittedly, I’ve been getting a lot more cranky at work, especially these last few weeks.Pharmacist 9
Throughout the day, I can tell we all become a little more irritated with each other. It also depends how the workflow is going, you have your days where nothing is going right, and then you have days where everything’s a cake walk. But, if we’re all caught up and things are going great, we all are like joking around, laughing with each other. But if things are just rough, we’re just snippy with each other, and it’s not fun.Pharmacist 11
And that does wear me out by the end to the day, I don’t want to talk to anybody. I just want to sit down and be quiet for a while. That fatigue. Not fall asleep fatigue, but just … I need rest.Pharmacist 1
I definitely feel, it’s fatigue, but it’s also just almost more of a mental … despair sounds dramatic. It’s not despair. But, ‘oh, there’s so much to do, and I’m not going to get it done,’ kind of a feeling until it starts to slow down.Pharmacist 4
As I start to get towards that end of the day, that foggy hazy feeling. Most of the time I am doing the vaccines, so it’s okay. But, I’ll start to get that foggy, hazy feeling, and I’ll be like, ‘wait, what did I just say? What was I just working on?’Pharmacist 1
3.2.2. Physical Fatigue
Sometimes I do get low back pain. And I don’t know if it’s just from standing for ten hours straight in the same spot for most of the day.Pharmacist 11
Usually, my feet will start to hurt. I’ll be walking back from the flu room or something, and I’ll just notice my feet are sore. I even got these better shoes, and that seemed to work for a little while. But now I’m like ‘ugh.’Pharmacist 20
And especially if [the patient] is going to come yell at you, or you recognize the name and you know it’s a script you have to refuse, and it’s going to probably start an issue, and you have to keep smiling through the whole thing. That does make me get headaches by the end of the day.Pharmacist 1
3.2.3. Active Fatigue
It’s just mentally exhausting helping person after person after person, running back and forth between trying to keep up on product checking. Just physically, mentally, it’s exhausting. And then by the end of the day, my brain just doesn’t, I don’t feel as clear. It’s hard to think.Pharmacist 12
I think for me, one of the signs that I’ll usually pick up on that makes me realize that I’m more tired is usually once I have a chance to actually sit down, I’ll be like, ‘oh, my God, this actually feels really good right now.’ Especially with those long days where I’m working 7:30 a.m. to 8 p.m. I have a lunch break in there, but you’re just continuously working. And then after a while, I sit in my car for a minute, and ‘wow, it’s been a long day.’Pharmacist 8
3.2.4. Passive Fatigue
Because days that we’re super busy, your brain doesn’t have a chance to slow down and stop, whereas a day where you’re slow, it’s hard because your brain’s not constantly stimulated. And then I feel like when you do have the sudden person come in, you’re like, ‘oh, I have to check.’ I’m one of those ones, I function better on a day where we’re consistently busy. I like where it’s like not overwhelming, but yet it’s busy enough where I never actually check out of what I’m doing to have to check back in. I think, when you are having a slow day, and there isn’t a lot going on it’s hard to keep engaged with what’s going on.Pharmacist 35
The scripts start to run into each other. And that’s also when you’re supposed to be checking them against other medications and stuff, and I just notice that I start to really zone out in what I’m doing. And I really have to snap myself and be like, ‘okay, you have to focus. You got to make sure this is correct.’Pharmacist 9
Autopilot, I think is the way I would describe it. Because, there’s been times where once I’ve checked the prescription and I’ll pull it back up, I’ll be like ‘I literally don’t even remember looking at those pills or seeing that prescription.’ Or I guess I’d compare it to the times where I’ve driven home and I’m like ‘how did I just get home? I don’t remember turning here.’ It just goes by, and I’m like ‘what happened?’Pharmacist 11
4. Discussion
4.1. “Despair” and Pharmacist Mental Fatigue
4.2. Fatigue and Interpersonal Relationships
4.3. Active and Passive Fatigue—A Fine Balance in Complex Work Systems
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doucette, W.R.; Gaither, C.A.; Mott, D.A.; Schommer, J.C.; Kreling, D.H.; Bakken, B.K.; Witry, M.J.; Arya, A.V. National Pharmacist Workforce Study 2019 Final Report; Pharmacy Workforce Center: Iowa City, IA, USA, 2020. [Google Scholar]
- Mott, D.A. Pharmacist Job Turnover, Length of Service, and Reasons for Leaving, 1983–1997. Am. J. Health Syst. Pharm. 2000, 57, 975–984. [Google Scholar] [CrossRef] [PubMed]
- Rupp, M.T.; DeYoung, M.; Schondelmeyer, S.W. Prescribing Problems and Pharmacist Interventions in Community Practice. Med. Care 1992, 30, 926–940. [Google Scholar] [CrossRef] [PubMed]
- Dore, D.D. A Day in the Life of a Corporate Retail Pharmacist. Ann. Intern. Med. 2013, 159, 366. [Google Scholar] [CrossRef] [PubMed]
- Chui, M.A.; Look, K.A.; Mott, D.A. The Association of Subjective Workload Dimensions on Quality of Care and Pharmacist Quality of Work Life. Res. Soc. Adm. Pharm. 2014, 10, 328–340. [Google Scholar] [CrossRef]
- Gidman, W.K.; Hassell, K.; Day, J.; Payne, K. The Impact of Increasing Workloads and Role Expansion on Female Community Pharmacists in the United Kingdom. Res. Soc. Adm. Pharm. 2007, 3, 285–302. [Google Scholar] [CrossRef]
- Holden, R.J.; Patel, N.R.; Scanlon, M.C.; Shalaby, T.M.; Arnold, J.M.; Karsh, B.-T. Effects of Mental Demands during Dispensing on Perceived Medication Safety and Employee Well-Being: A Study of Workload in Pediatric Hospital Pharmacies. Res. Soc. Adm. Pharm. 2010, 6, 293–306. [Google Scholar] [CrossRef]
- Malone, D.C.; Abarca, J.; Skrepnek, G.H.; Murphy, J.E.; Armstrong, E.P.; Grizzle, A.J.; Rehfeld, R.A.; Woosley, R.L. Pharmacist Workload and Pharmacy Characteristics Associated With the Dispensing of Potentially Clinically Important Drug-Drug Interactions. Med. Care 2007, 45, 456–462. [Google Scholar] [CrossRef]
- Li, H.; Zheng, S.; Liu, F.; Liu, W.; Zhao, R. Fighting against COVID-19: Innovative Strategies for Clinical Pharmacists. Res. Soc. Adm. Pharm. 2020, 17, 1813–1818. [Google Scholar] [CrossRef]
- Cadogan, C.A.; Hughes, C.M. On the Frontline against COVID-19: Community Pharmacists’ Contribution during a Public Health Crisis. Res. Soc. Adm. Pharm. 2020, 17, 2032–2035. [Google Scholar] [CrossRef]
- Steege, L.M.; Dykstra, J.G. A Macroergonomic Perspective on Fatigue and Coping in the Hospital Nurse Work System. Appl. Ergon. 2016, 54, 19–26. [Google Scholar] [CrossRef]
- Steege, L.M.; Pinekenstein, B.J.; Arsenault Knudsen, É.; Rainbow, J.G. Exploring Nurse Leader Fatigue: A Mixed Methods Study. J. Nurs. Manag. 2017, 25, 276–286. [Google Scholar] [CrossRef]
- Steege, L.M.; Pinekenstein, B. Addressing Occupational Fatigue in Nurses: A Risk Management Model for Nurse Executives. J. Nurs. Adm. 2016, 46, 193–200. [Google Scholar] [CrossRef]
- Ahsberg, E. Dimensions of Fatigue in Different Working Populations. Scand. J. Psychol. 2000, 41, 231–241. [Google Scholar] [CrossRef]
- Steege, L.M.; Drake, D.A.; Olivas, M.; Mazza, G. Evaluation of Physically and Mentally Fatiguing Tasks and Sources of Fatigue as Reported by Registered Nurses. J. Nurs. Manag. 2015, 23, 179–189. [Google Scholar] [CrossRef]
- Steege, L.M.; Pinekenstein, B.J.; Rainbow, J.G.; Arsenault Knudsen, É. Addressing Occupational Fatigue in Nurses: Current State of Fatigue Risk Management in Hospitals, Part 2. J. Nurs. Adm. 2017, 47, 484–490. [Google Scholar] [CrossRef]
- Rogers, A.E.; Hwang, W.-T.; Scott, L.D.; Aiken, L.H.; Dinges, D.F. The Working Hours of Hospital Staff Nurses and Patient Safety. Health Aff. 2004, 23, 202–212. [Google Scholar] [CrossRef]
- Williamson, A.; Lombardi, D.A.; Folkard, S.; Stutts, J.; Courtney, T.K.; Connor, J.L. The Link between Fatigue and Safety. Accid. Anal. Prev. 2011, 43, 498–515. [Google Scholar] [CrossRef]
- Greig, P.; Snow, R. Fatigue and Risk: Are Train Drivers Safer than Doctors? BMJ 2017, 359, j5107. [Google Scholar] [CrossRef]
- Winwood, P.C.; Winefield, A.H.; Dawson, D.; Lushington, K. Development and Validation of a Scale to Measure Work-Related Fatigue and Recovery: The Occupational Fatigue Exhaustion/Recovery Scale (OFER). J. Occup. Environ. Med. 2005, 47, 594–606. [Google Scholar] [CrossRef]
- Hancock, P.A.; Desmond, P.A. (Eds.) Stress, Workload, and Fatigue, 1st ed.; CRC Press: Boca Raton, FL, USA, 2019; ISBN 9780367447311. [Google Scholar]
- Åhsberg, E.; Garnberale, F.; Kjellberg, A. Perceived Quality of Fatigue during Different Occupational Tasks Development of a Questionnaire. Int. J. Ind. Ergon. 1997, 20, 121–135. [Google Scholar] [CrossRef]
- Åhsberg, E.; Gamberale, F. Perceived Fatigue during Physical Work: An Experimental Evaluation of a Fatigue Inventory. Int. J. Ind. Ergon. 1998, 21, 117–131. [Google Scholar] [CrossRef]
- Long, R. House Backs Study of Pharmacy Safety, Consumer Needs after Tribune Investigation. Available online: https://www.chicagotribune.com/investigations/ct-drug-interactions-bill-house-vote-met-20170428-story.html (accessed on 17 January 2020).
- Chui, M.A. Safety in the Retail Pharmacy. Available online: https://psnet.ahrq.gov/perspective/safety-retail-pharmacy (accessed on 18 April 2021).
- Gabler, E. How Chaos at Chain Pharmacies Is Putting Patients at Risk. Available online: https://www.nytimes.com/2020/01/31/health/pharmacists-medication-errors.html (accessed on 31 March 2022).
- Ngo, M. Angry Customers, More Work and Longer Hours Strain Pharmacists. Available online: https://www.nytimes.com/2022/02/10/us/politics/pharmacists-strain-covid.html (accessed on 31 March 2022).
- Levy, S. CVS Health to Give Pharmacists Dedicated Lunch Break. Available online: https://www.drugstorenews.com/cvs-health-give-pharmacists-dedicated-lunch-break (accessed on 9 March 2022).
- Missouri Board of Pharmacy BOARD STATEMENT ON PHARMACY WORKING CONDITIONS. Available online: https://pr.mo.gov/boards/pharmacy/covid-19/WorkingConditions(FINAL).pdf (accessed on 7 July 2021).
- #PizzaIsNotWorking Thread. Available online: https://twitter.com/search?q=%23PizzaIsNotWorking&src=typed_query&f=live (accessed on 1 April 2022).
- Stoller, M. #PizzaIsNotWorking: Inside the Pharmacist Rebellion at CVS and Walgreens. Available online: https://mattstoller.substack.com/p/pizzaisnotworking-inside-the-pharmacist?s=r (accessed on 1 April 2022).
- R/CVS-The Pizza Is Not Enough. Available online: https://www.reddit.com/r/CVS/comments/qthe7b/the_pizza_is_not_enough/?utm_source=BD&utm_medium=Search&utm_name=Bing&utm_content=PSR1 (accessed on 1 April 2022).
- Kostiuk, L. Pizza Is Not Working: Pharmacists Band Together to Raise Awareness About Working Conditions. Available online: https://www.msn.com/en-us/news/us/pizza-is-not-working-pharmacists-band-together-to-raise-awareness-about-working-conditions/ar-AARHpko (accessed on 1 April 2022).
- Torabizadeh, C.; Yousefinya, A.; Zand, F.; Rakhshan, M.; Fararooei, M. A Nurses’ Alarm Fatigue Questionnaire: Development and Psychometric Properties. J. Clin. Monit. Comput. 2017, 31, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- National Steering Committee for Patient Safety. Safer Together: A National Plan to Advance Patient Safety; Institute for Healthcare Improvement: Boston, MA, USA, 2020. [Google Scholar]
- Lee, S.; Seong, S.; Park, S.; Lim, J.; Hong, S.; Cho, Y.; Kim, H. Korean Version of the Swedish Occupational Fatigue Inventory among Construction Workers: Cultural Adaptation and Psychometric Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 4302. [Google Scholar] [CrossRef] [PubMed]
- Ahsberg, E.; Fürst, C.J. Dimensions of Fatigue during Radiotherapy-An Application of the Swedish Occupational Fatigue Inventory (SOFI) on Cancer Patients. Acta Oncol. 2001, 40, 37–43. [Google Scholar]
- González Gutiérrez, J.L.; Jiménez, B.M.; Hernández, E.G.; López López, A. Spanish Version of the Swedish Occupational Fatigue Inventory (SOFI): Factorial Replication, Reliability and Validity. Int. J. Ind. Ergon. 2005, 35, 737–746. [Google Scholar] [CrossRef]
- Leung, A.W.S.; Chan, C.C.H.; He, J. Structural Stability and Reliability of the Swedish Occupational Fatigue Inventory among Chinese VDT Workers. Appl. Ergon. 2004, 35, 233–241. [Google Scholar] [CrossRef]
- Schaeffer, N.C.; Presser, S. The Science of Asking Questions. Annu. Rev. Sociol. 2003, 29, 65–88. [Google Scholar] [CrossRef]
- Watterson, T.L.; Look, K.A.; Steege, L.; Chui, M.A. Operationalizing Occupational Fatigue in Pharmacists: An Exploratory Factor Analysis. Res. Soc. Adm. Pharm. 2020, 17, 1282–1287. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org (accessed on 8 May 2022).
- Elo, S.; Kyngäs, H. The Qualitative Content Analysis Process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Kyngäs, H.; Kaakinen, P. Deductive Content Analysis. In The Application of Content Analysis in Nursing Science Research; Kyngäs, H., Mikkonen, K., Kääriäinen, M., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 23–30. ISBN 9783030301996. [Google Scholar]
- Holden, R.J.; Carayon, P.; Gurses, A.P.; Hoonakker, P.; Hundt, A.S.; Ozok, A.A.; Rivera-Rodriguez, A.J. SEIPS 2.0: A Human Factors Framework for Studying and Improving the Work of Healthcare Professionals and Patients. Ergonomics 2013, 56, 1669–1686. [Google Scholar] [CrossRef]
- Steege, L.M.; Rainbow, J.G. Fatigue in Hospital Nurses—“Supernurse” Culture Is a Barrier to Addressing Problems: A Qualitative Interview Study. Int. J. Nurs. Stud. 2017, 67, 20–28. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Noseworthy, J.H. Executive Leadership and Physician Well-Being. Mayo Clin. Proc. 2017, 92, 129–146. [Google Scholar] [CrossRef]
- Smith, C.D.; Balatbat, C.; Corbridge, S.; Dopp, A.L.; Fried, J.; Harter, R.; Landefeld, S.; Martin, C.Y.; Opelka, F.; Sandy, L.; et al. Implementing Optimal Team-Based Care to Reduce Clinician Burnout. NAM Perspect. 2018, 8, 1–13. [Google Scholar] [CrossRef]
- Cho, H.; Sagherian, K.; Scott, L.D.; Steege, L.M. Occupational Fatigue, Workload and Nursing Teamwork in Hospital Nurses. J. Adv. Nurs. 2022, 78, 2313–2326. [Google Scholar] [CrossRef]
- Mountain, S.A.; Quon, B.S.; Dodek, P.; Sharpe, R.; Ayas, N.T. The Impact of Housestaff Fatigue on Occupational and Patient Safety. Lung 2007, 185, 203–209. [Google Scholar] [CrossRef]
- OSHA Long Work Hours, Extended or Irregular Shifts, and Worker Fatigue—Overview. Available online: https://www.osha.gov/worker-fatigue (accessed on 6 March 2022).
- Gander, P.; Purnell, H.; Garden, A.; Woodward, A. Work Patterns and Fatigue-Related Risk among Junior Doctors. Occup. Environ. Med. 2007, 64, 733–738. [Google Scholar] [CrossRef]
- Anderson, C.; Sullivan, J.P.; Flynn-Evans, E.E.; Cade, B.E.; Czeisler, C.A.; Lockley, S.W. Deterioration of Neurobehavioral Performance in Resident Physicians during Repeated Exposure to Extended Duration Work Shifts. Sleep 2012, 35, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Taffinder, N.J.; McManus, I.C.; Gul, Y.; Russell, R.C.; Darzi, A. Effect of Sleep Deprivation on Surgeons’ Dexterity on Laparoscopy Simulator. Lancet 1998, 352, 1191. [Google Scholar] [CrossRef]
- Dasan, S.; Gohil, P.; Cornelius, V.; Taylor, C. Prevalence, Causes and Consequences of Compassion Satisfaction and Compassion Fatigue in Emergency Care: A Mixed-Methods Study of UK NHS Consultants. Emerg. Med. J. 2015, 32, 588–594. [Google Scholar] [CrossRef]
- Saxby, D.J.; Matthews, G.; Warm, J.S.; Hitchcock, E.M.; Neubauer, C. Active and Passive Fatigue in Simulated Driving: Discriminating Styles of Workload Regulation and Their Safety Impacts. J. Exp. Psychol. Appl. 2013, 19, 287–300. [Google Scholar] [CrossRef]
- Nsiah, I.; Imeri, H.; Jones, A.C.; Bentley, J.P.; Barnard, M.; Kang, M. The Impact of Medication Synchronization Programs on Medication Adherence: A Meta-Analysis. J. Am. Pharm. Assoc. 2021, 61, e202–e211. [Google Scholar] [CrossRef] [PubMed]
- Adams, A.J.; Martin, S.J.; Stolpe, S.F. “Tech-Check-Tech”: A Review of the Evidence on Its Safety and Benefits. Am. J. Health Syst. Pharm. 2011, 68, 1824–1833. [Google Scholar] [CrossRef]
- Hill, J.D.; Anderegg, S.V.; Couldry, R.J. Development of a Pharmacy Technician-Driven Program to Improve Vaccination Rates at an Academic Medical Center. Hosp. Pharm. 2017, 52, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Ahsberg, E.; Gamberale, F.; Gustafsson, K. Perceived Fatigue after Mental Work: An Experimental Evaluation of a Fatigue Inventory. Ergonomics 2000, 43, 252–268. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual; Consulting Psychologists Press: Palo Alto, CA, USA, 1998. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | N = 39 (%) |
|---|---|
| Pharmacy Characteristics | |
| Practice Setting | |
| National Chain | 14 (35.0%) |
| Independent | 15 (37.5%) |
| Other (Mass Merchandiser, Grocery Store, Other) | 11 (27.5%) |
| Scheduled Breaks in the Workday | |
| Yes | 28 (70.0%) |
| No | 12 (30.0%) |
| Average Characteristics | Median (range) |
| Days Worked in the 14-day Period | 10 days (6–14) |
| Shift Length | 9 h (7–12.5) |
| Pharmacist Support | 2 full-time pharmacists (1–10) |
| Staff Support (Technician, Student Intern, Clerk) | 3.5 full-time staff members (0–10) |
| Prescription Volume | 400 prescriptions (17–1500) |
| Pharmacist Characteristics | |
| Gender Identity | |
| Man | 12 (30.8%) |
| Woman | 26 (66.7%) |
| Prefer to Self-Describe | 1 (2.6%) |
| Ethnicity | |
| White, not of Hispanic Origin | 33 (84.6%) |
| Asian or Pacific Islander | 7 (17.9%) |
| Marital Status | |
| Married | 23 (59.0%) |
| Single | 13 (33.3%) |
| Divorced | 3 (7.7%) |
| Average Characteristics | Median (range) |
| Age | 34 years old (25–59) |
| Daily Caffeine Servings | 2 servings (0–4.5) |
| Adults (age 18+) in the Household | 2 adults (1–5) |
| Individuals (under age 18) in the Household | 0 individuals (0–3) |
| Years of Working in the Pharmacy as a Pharmacist | 3 years (0–31) |
| Hours of Sleep | 7 h (5–9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watterson, T.L.; Chui, M.A. Subjective Perceptions of Occupational Fatigue in Community Pharmacists. Pharmacy 2023, 11, 84. https://doi.org/10.3390/pharmacy11030084
Watterson TL, Chui MA. Subjective Perceptions of Occupational Fatigue in Community Pharmacists. Pharmacy. 2023; 11(3):84. https://doi.org/10.3390/pharmacy11030084
Chicago/Turabian StyleWatterson, Taylor L., and Michelle A. Chui. 2023. "Subjective Perceptions of Occupational Fatigue in Community Pharmacists" Pharmacy 11, no. 3: 84. https://doi.org/10.3390/pharmacy11030084