
Nephroprotective Plants: A Review on the Use in Pre-Renal and Post-Renal Diseases

 ,
,  ,
,  , , and
, , and 
Abstract
:
1. Introduction
2. A Combined Therapeutic Approach
3. Nephroprotective Plants
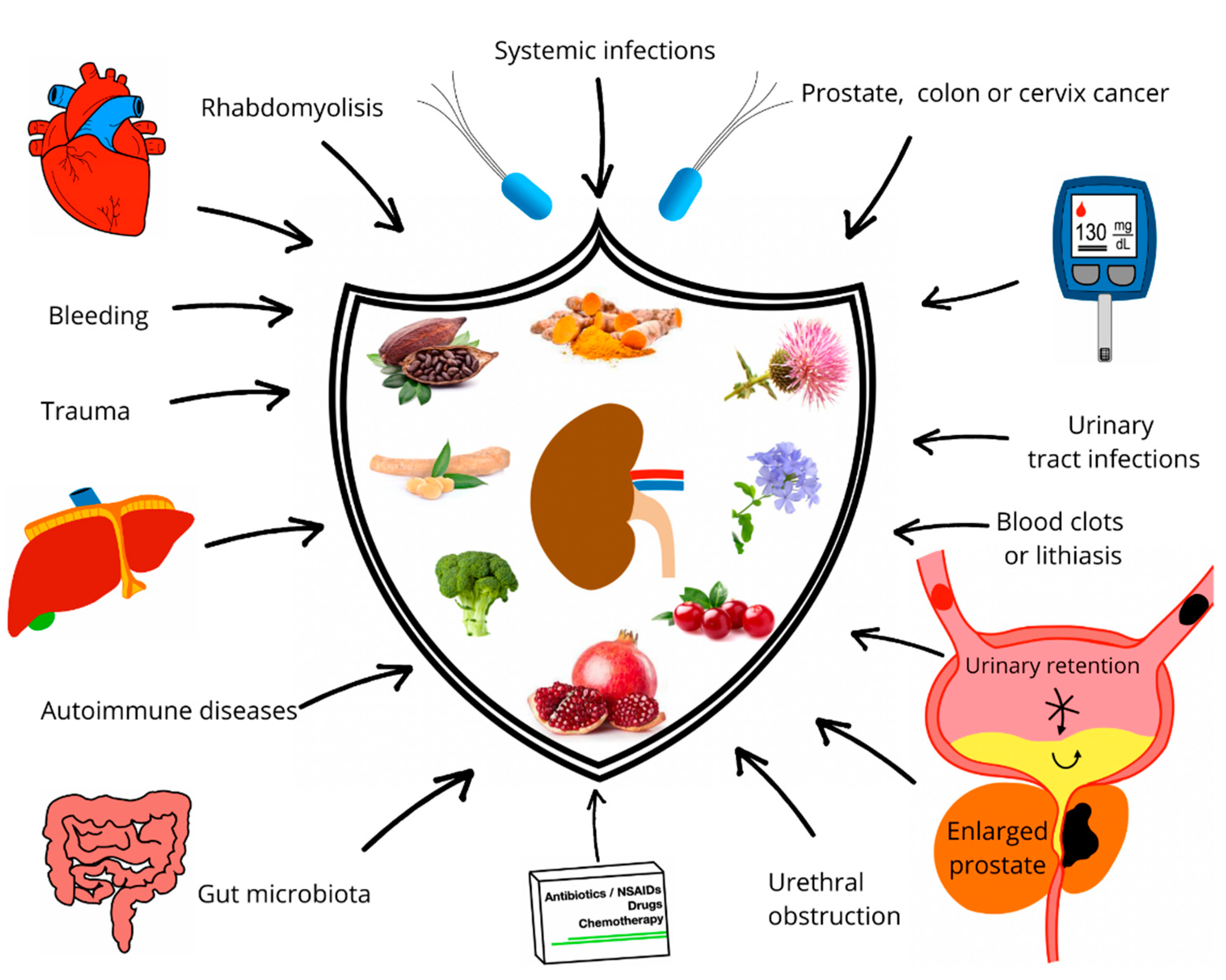
4. The Role of Plants in Renal Pathophysiology
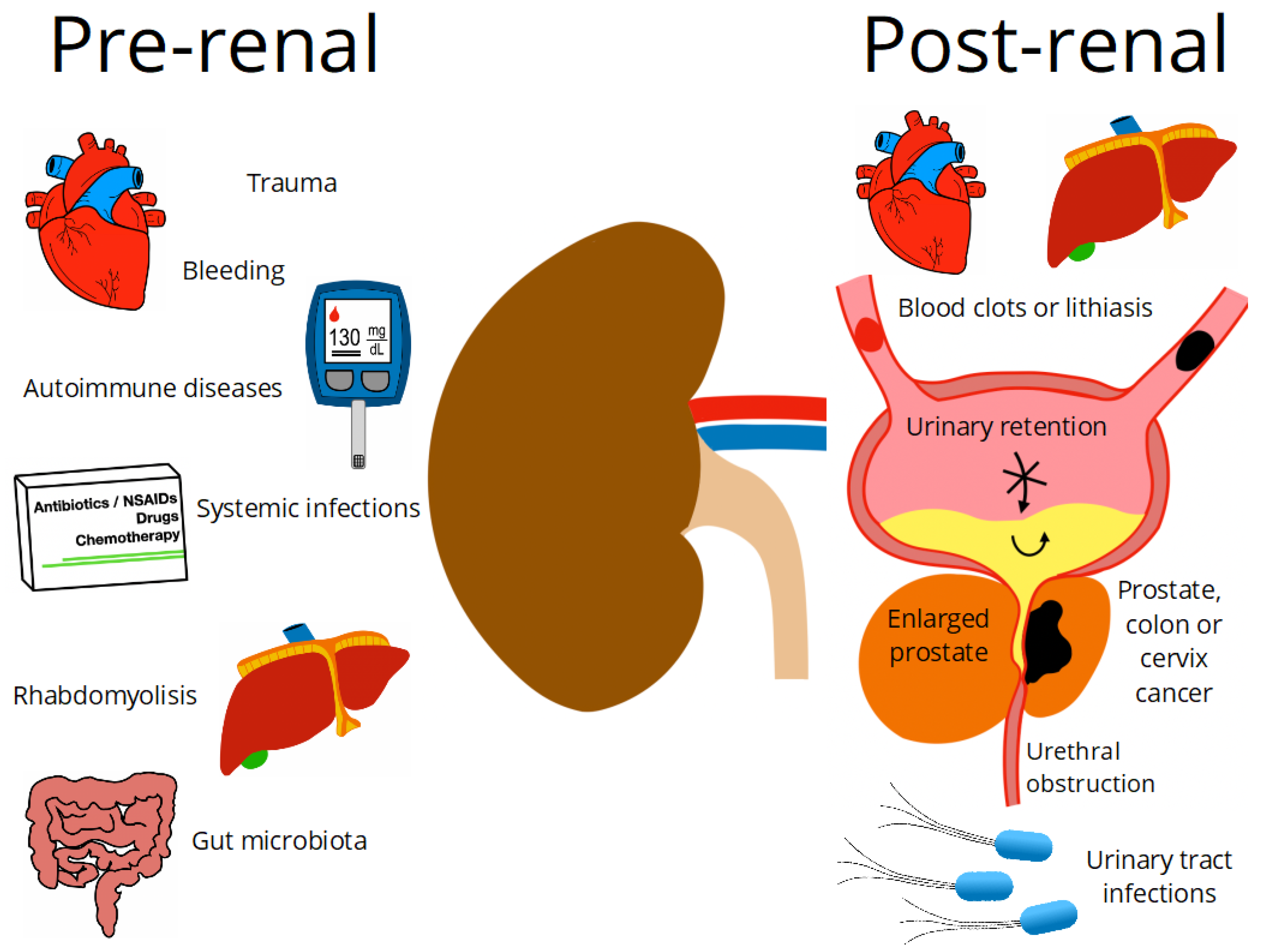
4.1. Pre-Renal Factors
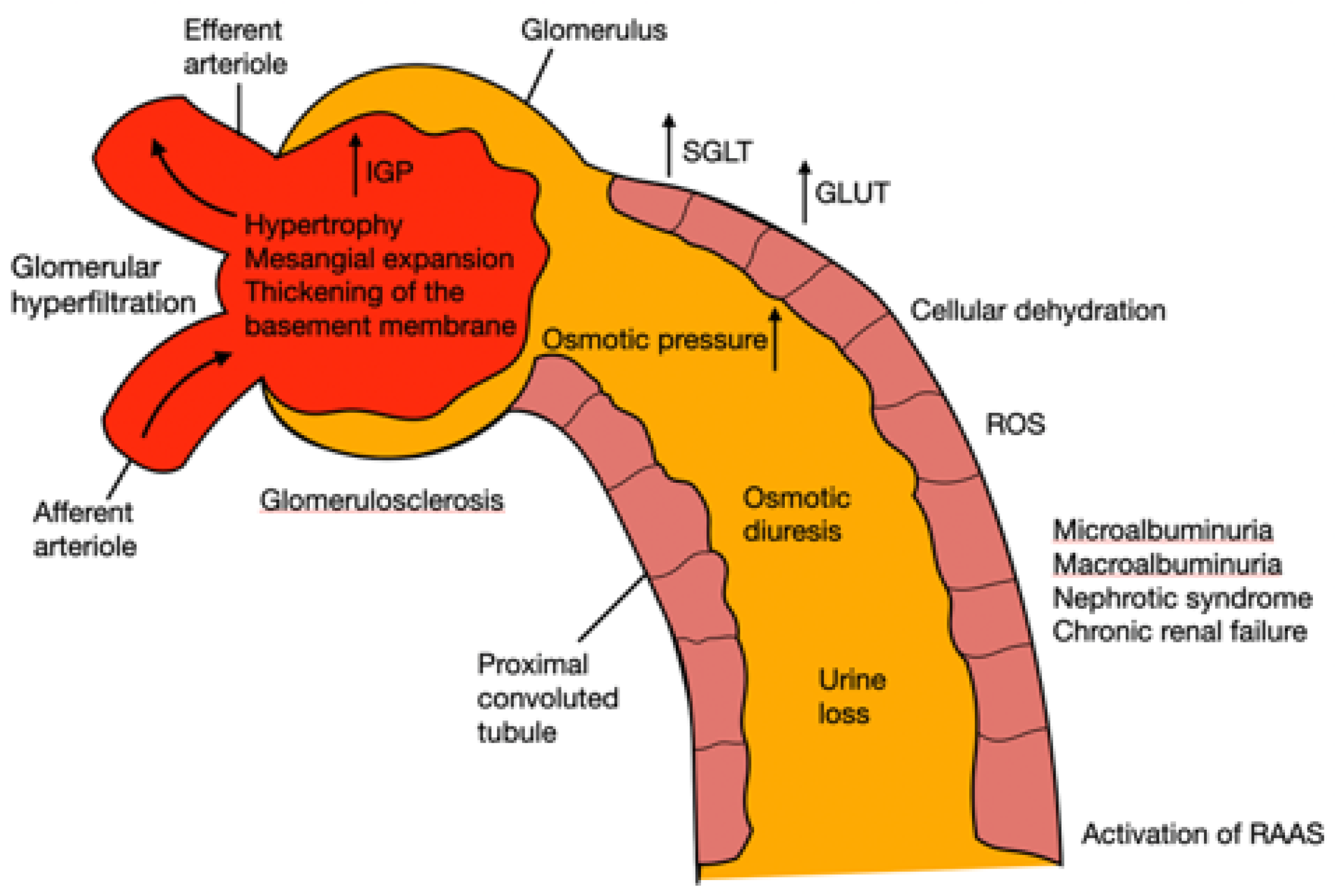
4.1.1. Diabetes Mellitus
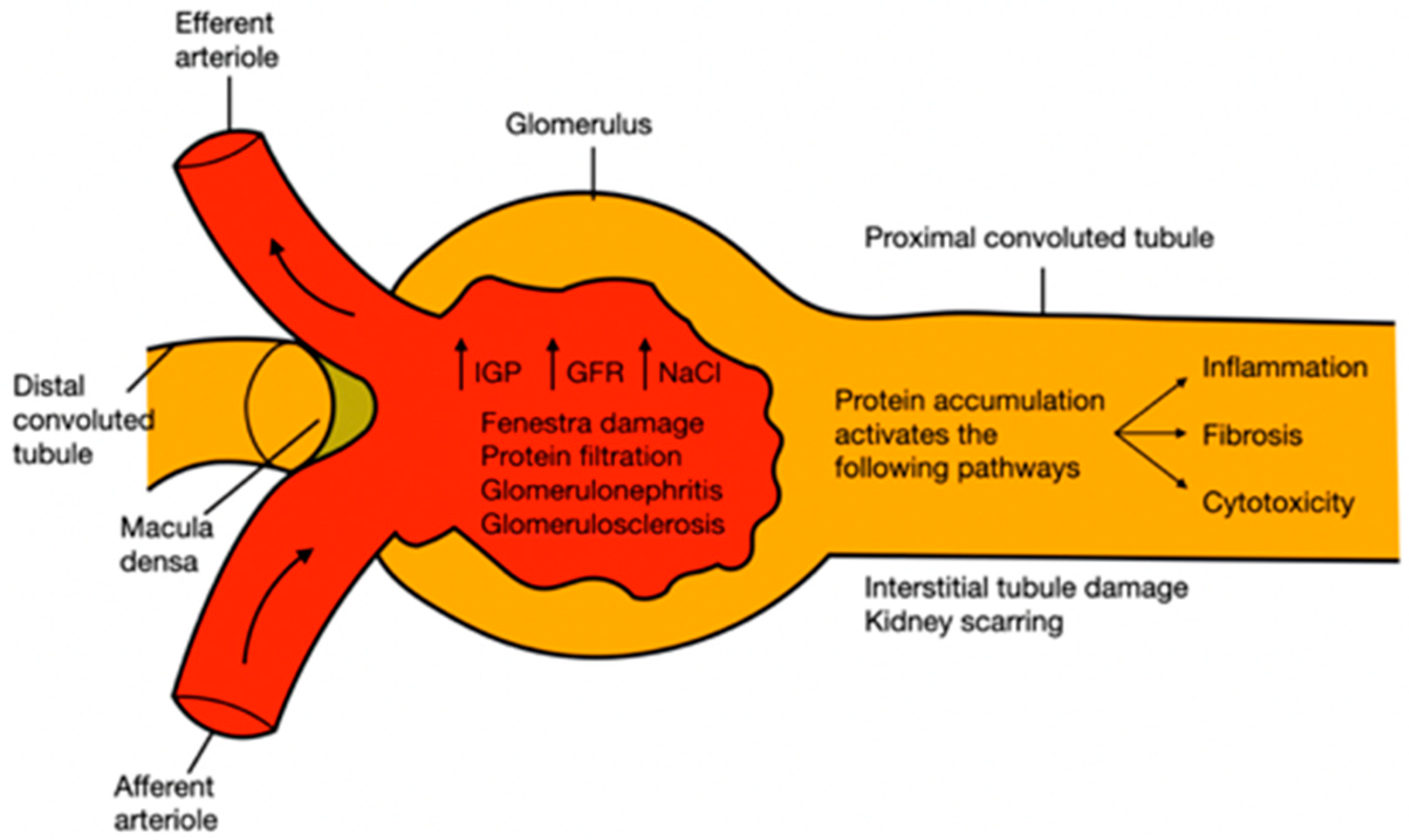
4.1.2. Hypertension
4.1.3. Hepatic Injury
4.1.4. Antibiotic Drugs Damage
4.1.5. The Gut Microbiota
4.1.6. Rhabdomyolysis
4.2. Post-Renal
4.2.1. Urinary Tract Infections
4.2.2. Urinary Tract Obstructions
4.2.3. Prostate Enlargement
5. Conclusions and Future Perspectives
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Little, M.H.; Combes, A.N. Kidney organoids: Accurate models or fortunate accidents. Genes Dev. 2019, 33, 1319–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sujana, D.; Saptarini, N.M.; Sumiwi, S.A.; Levita, J. Nephroprotective activity of medicinal plants: A review on in silico-, in vitro-, and in vivo-based studies. J. Appl. Pharm. Sci. 2021, 11, 113–127. [Google Scholar] [CrossRef]
- Jager, K.J.; Kovesdy, C.; Langham, R.; Rosenberg, M.; Jha, V.; Zoccali, C. A single number for advocacy and communication-worldwide more than 850 million individuals have kidney diseases. Nephrol. Dial. Transplant. 2019, 34, 1803–1805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, B.M.; Lippi, G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int. Urol. Nephrol. 2020, 52, 1193–1194. [Google Scholar] [CrossRef] [Green Version]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- KDIGO. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury workgroup. KDIGO clinical practice guideline for acute kidney injury. Kidney. Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Manzoor, H.; Bhatt, H. Prerenal Kidney Failure; StatPearls Publishing: Las Vegas, NV, USA, 2020. [Google Scholar]
- Matuszkiewicz-Rowińska, J.; Małyszko, J. Acute kidney injury, its definition, and treatment in adults: Guidelines and reality. Pol. Arch. Intern Med. 2020, 130, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Makris, K.; Spanou, L. Acute Kidney Injury: Definition, Pathophysiology and Clinical Phenotypes. Clin. Biochem. Rev. 2016, 37, 85–98. [Google Scholar] [PubMed]
- Horie, S.; Oya, M.; Nangaku, M.; Yasuda, Y.; Komatsu, Y.; Yanagita, M.; Kitagawa, Y.; Kuwano, H.; Nishiyama, H.; Ishioka, C.; et al. Guidelines for treatment of renal injury during cancer chemotherapy 2016. Clin. Exp. Nephrol. 2018, 22, 210–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucas, G.N.C.; Leitão, A.C.C.; Alencar, R.L.; Xavier, R.M.F.; Daher, E.D.F.; Silva, G.B.D. Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. J. Bras. Nefrol. 2019, 41, 124–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petejova, N.; Martinek, A.; Zadrazil, J.; Kanova, M.; Klementa, V.; Sigutova, R.; Kacirova, I.; Hrabovsky, V.; Svagera, Z.; Stejskal, D. Acute kidney injury in septic patients treated by selected nephrotoxic antibiotic agents—Pathophysiology and biomarkers—A review. Int. J. Mol. Sci. 2020, 21, 7115. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Li, D.; Xu, T.; Luo, M.; He, Z.; Li, Y. Proton pump inhibitors associated acute kidney injury and chronic kidney disease: Data mining of US FDA adverse event reporting system. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lawson, S.K.; Satyal, P.; Setzer, W.N. The volatile phytochemistry of seven native american aromatic medicinal plants. Plants 2021, 10, 1061. [Google Scholar] [CrossRef] [PubMed]
- Isah, T. Stress and defense responses in plant secondary metabolites production. Biol. Res. 2019, 52, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.; Vasudeva, N.; Sharma, S. Kidney disorders and management through herbs: A Review. J. Phytopharm. 2019, 8, 21–27. [Google Scholar] [CrossRef]
- Efferth, T.; Saeed, M.E.; Mirghani, E.; Alim, A.; Yassin, Z.; Saeed, E.; Khalid, H.E.; Daak, S. Integration of phytochemicals and phytotherapy into cancer precision medicine. Oncotarget 2017, 8, 50284–50304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Governa, P.; Baini, G.; Borgonetti, V.; Cettolin, G.; Giachetti, D.; Magnano, A.R.; Miraldi, E.; Biagi, M. Phytotherapy in the Management of Diabetes: A Review. Molecules 2018, 23, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabiu, S.; O’Neill, F.H.; Ashafa, A.O.T. The purview of phytotherapy in the management of kidney disorders: A systematic review on Nigeria and South Africa. Afr. J. Tradit. Complement. Altern. Med. 2016, 13, 38–47. [Google Scholar]
- Basist, P.; Parveen, B.; Zahiruddin, S.; Gautam, G.; Parveen, R.; Khan, M.A.; Krishnan, A.; Shahid, M.; Ahmad, S. Potential nephroprotective phytochemicals: Mechanism and future prospects. J. Ethnopharm. 2022, 283, 114743. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Q.Z. An Appraisal of Nephroprotection and the Scope of Natural Products in Combating Renal Disorders. J. Nephrol. Ther. 2014, 04, 170. [Google Scholar] [CrossRef] [Green Version]
- Stub, T.; Quandt, S.A.; Arcury, T.A.; Sandberg, J.C.; Kristoffersen, A.E.; Musial, F.; Salamonsen, A. Perception of risk and communication among conventional and complementary health care providers involving cancer patients’ use of complementary therapies: A literature review. BMC Complement. Altern. Med. 2016, 16, 353. [Google Scholar] [CrossRef] [Green Version]
- Khalil, H.; Huang, C. Adverse drug reactions in primary care: A scoping review. BMC Health Serv. Res. 2020, 20, 5. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Traditional Medicines Strategy 2014–2023; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Li, J.; Li, B.; Zhao, X.K.; Tu, J.Y.; Li, Y. A critical review to grading systems and recommendations of traditional Chinese medicine guidelines. Health Qual. Life Outcomes 2020, 18, 174. [Google Scholar] [CrossRef] [PubMed]
- Mai, W.; Wei, A.; Lin, X.; Wang, F.; Ye, J.; Chen, P. Efficacy and safety of traditional Chinese medicine injection with mecobalamin in treating diabetic peripheral neuropathy: A protocol for systematic review and meta-analysis. Medicine 2021, 100, e23702. [Google Scholar] [CrossRef]
- Kessler, C.S.; Morandi, A.; Kumar, A.; Dhiman, K.S.; Gupta, S.; Icke, K.; Bühner, C.; Stapelfeldt, E.; Wischnewsky, M.; Kronpaß, L.; et al. Reliability of Ayurvedic Diagnosis for Knee Osteoarthritis Patients: A Nested Diagnostic Study Within a Randomized Controlled Trial. J. Altern. Complement. Med. 2019, 25, 910–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, C.T.; Denniston, K.; Chopra, D. Therapeutic uses of Triphala in ayurvedic medicine. J. Altern Complement. Med. 2017, 23, 607–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atanasov, A.G.; Waltenberger, B.; Pferschy-Wenzig, E.-M.; Linder, T.; Wawrosch, C.; Uhrin, P.; Temml, V.; Wang, L.; Schwaiger, S.; Heiss, E.H.; et al. Discovery and resupply of pharmacologically active plant-derived natural products: A review. Biotechnol. Adv. 2015, 33, 1582–1614. [Google Scholar] [CrossRef] [Green Version]
- Atanasov, A.G.; Zotchev, S.B.; Dirsch, V.M.; Supuran, C.T. Natural products in drug discovery: Advances and opportunities. Nat. Rev. Drug Discov. 2021, 20, 200–216. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; He, Y.; Zhang, H.; Zheng, R.; Xu, R.; Liu, Q.; Tang, S.; Ke, X.; Huang, M. Formulation of traditional Chinese medicine and its application on intestinal flora of constipated rats. Microb. Cell Fact. 2020, 19, 212. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Zhao, Y.; Hua, H.; Zhang, Y.; Zhang, X.; Fang, Q.; Li, Q.; Zhang, Y.; Tan, P.; Yang, A.; et al. Research progress on quality assurance of genuine Chinese medicinal in Sichuan. Chin. Med. 2021, 16, 19. [Google Scholar] [CrossRef]
- Nyakudya, T.; Tshabalala, T.; Dangarembizi, R.; Erlwanger, K.; Ndhlala, A.R. The Potential Therapeutic Value of Medicinal Plants in the Management of Metabolic Disorders. Molecules 2020, 25, 2669. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, S. Emanating the specialty clinical practices in Ayurveda: Preliminary observations from an arthritis clinic and its implications. J. Ayurveda Integr. Med. 2020, 12, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Kim, K.; Nam, H.; Lee, D. Discovering Health Benefits of Phytochemicals with Integrated Analysis of the Molecular Network, Chemical Properties and Ethnopharmacological Evidence. Nutrients 2018, 10, 1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, S.-Y.; Litscher, G.; Gao, S.-H.; Zhou, S.-F.; Yu, Z.-L.; Chen, H.-Q.; Zhang, S.-F.; Tang, M.-K.; Sun, J.-N.; Ko, K.-M. Historical Perspective of Traditional Indigenous Medical Practices: The Current Renaissance and Conservation of Herbal Resources. Evid.-Based Complement. Altern. Med. 2014, 2014, 525340. [Google Scholar] [CrossRef] [PubMed]
- Campagne, O.; Mager, D.E.; Brazeau, D.; Venuto, R.C.; Tornatore, K.M. The impact of tacrolimus exposure on extrarenal adverse effects in adult renal transplant recipients. Br. J. Clin. Pharmacol. 2019, 85, 516–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Dobos, G.J.; Rampp, T. The Significance of Ayurvedic Medicinal Plants. J. Evid.-Based Complement. Altern. Med. 2017, 22, 494–501. [Google Scholar] [CrossRef] [Green Version]
- Pfister, B.; Jonsson, J.; Gustafsson, M. Drug-related problems and medication reviews among old people with dementia. BMC Pharmacol. Toxicol. 2017, 18, 52. [Google Scholar] [CrossRef] [Green Version]
- Stocco, G.; Lucafò, M.; Decorti, G. Pharmacogenomics of Antibiotics. Int. J. Mol. Sci. 2020, 21, 5975. [Google Scholar] [CrossRef]
- Phe, K.; Shields, R.K.; Tverdek, F.P.; Aitken, S.; Guervil, D.J.; Lam, W.-Y.M.; Musgrove, R.J.; Luce, A.M.; Tam, V.H. Predicting the risk of nephrotoxicity in patients receiving colistimethate sodium: A multicentre, retrospective, cohort study. J. Antimicrob. Chemother. 2016, 71, 3585–3587. [Google Scholar] [CrossRef] [Green Version]
- Dwyer, J.T.; Coates, P.M.; Smith, M.J. Dietary Supplements: Regulatory Challenges and Research Resources. Nutrients 2018, 10, 41. [Google Scholar] [CrossRef] [Green Version]
- McGraw, N.J.; Krul, E.S.; Grunz-Borgmann, E.; Parrish, A.R. Soy-based renoprotection. World J. Nephrol. 2016, 5, 233–257. [Google Scholar] [CrossRef] [PubMed]
- Moorthi, R.N.; Vorland, C.J.; Gallant, K.M.H. Diet and Diabetic Kidney Disease: Plant Versus Animal Protein. Curr. Diabetes Rep. 2017, 17, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alabi, T.; Brooks, N.; Oguntibeju, O. Leaf Extracts of Anchomanes difformis Ameliorated Kidney and Pancreatic Damage in Type 2 Diabetes. Plants 2021, 10, 300. [Google Scholar] [CrossRef] [PubMed]
- Al-Anbaki, M.; Cavin, A.-L.; Nogueira, R.; Taslimi, J.; Ali, H.; Najem, M.; Mahmood, M.S.; Khaleel, I.A.; Mohammed, A.S.; Hasan, H.R.; et al. Hibiscus sabdariffa, a Treatment for Uncontrolled Hypertension. Pilot Comparative Intervention. Plants 2021, 10, 1018. [Google Scholar] [CrossRef] [PubMed]
- Nasri, H.; Hedayatollah, S. Toxicity and safety of medicinal plants. J. HerbMed. Pharmacol. 2013, 2, 21–22. Available online: http://eprints.skums.ac.ir/4798/1/9.pdf (accessed on 15 March 2022).
- Kharchoufa, L.; Bouhrim, M.; Bencheikh, N.; Addi, M.; Hano, C.; Mechchate, H.; Elachouri, M. Potential Toxicity of Medicinal Plants Inventoried in Northeastern Morocco: An Ethnobotanical Approach. Plants 2021, 10, 1108. [Google Scholar] [CrossRef]
- Oketch-Rabah, H.A.; Roe, A.L.; Rider, C.V.; Bonkovsky, H.L.; Giancaspro, G.I.; Navarro, V.; Paine, M.F.; Betz, J.M.; Marles, R.J.; Casper, S.; et al. United States Pharmacopeia (USP) comprehensive review of the hepatotoxicity of green tea extracts. Toxicol. Rep. 2020, 7, 386–402. [Google Scholar] [CrossRef]
- Rakib, A.; Ahmed, S.; Islam, M.A.; Haye, A.; Uddin, S.M.N.; Uddin, M.M.N.; Hossain, M.K.; Paul, A.; Emran, T.B. Antipyretic and hepatoprotective potential of Tinospora crispa and investigation of possible lead compounds through in silico approaches. Food Sci. Nutr. 2020, 8, 547–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Martínez, E.; Jiménez-Santana, M.; Centeno-Álvarez, M.; Torres-Valencia, J.M.; Shibayama, M.; Cariño-Cortés, R. Hepatoprotective Effects of Nonpolar Extracts from Inflorescences of Thistles Cirsium vulgare and Cirsium ehrenbergii on Acute Liver Damage in Rat. Pharmacogn. Mag. 2018, 13, S860–S867. [Google Scholar] [CrossRef]
- Mohammed, S.A.A.; Khan, R.A.; El-readi, M.Z.; Emwas, A.H.; Sioud, S.; Poulson, B.G.; Jaremko, M.; Eldeeb, H.M.; Al-Omar, M.S.; Mohammed, H.A. Suaeda vermiculata aqueous-ethanolic extract-based mitigation of ccl4-induced hepatotoxicity in rats, and hepg-2 and hepg-2/adr cell-lines-based cytotoxicity evaluations. Plants 2020, 9, 1291. [Google Scholar] [CrossRef] [PubMed]
- Moshaie-Nezhad, P.; Bahari, Z.; Jangravi, Z.; Zarei, S.M.; Iman, M. The Effect of Descurainia Sophia Seed Extract on Nephrotoxicity Markers Induced by Acetaminophen in Mice. J. Adv. Med Biomed. Res. 2021, 29, 139–144. [Google Scholar] [CrossRef]
- Chinnappan, S.M.; George, A.; Thaggikuppe Krishnamurthy, P.; Choudhary, Y.; Choudhary, V.K.; Ramani, Y.; Dewangan, R. Nephroprotective Effect of Herbal Extract Eurycoma longifolia on Paracetamol-Induced Nephrotoxicity in Rats. Evid.-based Complement. Altern. Med. 2019, 2019, 4916519. [Google Scholar] [CrossRef] [Green Version]
- Buzgaia, N.; Awin, T.; Elabbar, F.; Abdusalam, K.; Lee, S.Y.; Rukayadi, Y.; Abas, F.; Shaari, K. Antibacterial Activity of Arbutus pavarii Pamp against Methicillin-Resistant Staphylococcus aureus (MRSA) and UHPLC-MS/MS Profile of the Bioactive Fraction. Plants 2020, 9, 1539. [Google Scholar] [CrossRef] [PubMed]
- Mestry, S.N.; Gawali, N.B.; Pai, S.A.; Gursahani, M.S.; Dhodi, J.B.; Munshi, R.; Juvekar, A.R. Punica granatum improves renal function in gentamicin-induced nephropathy in rats via attenuation of oxidative stress. J. Ayurveda Integr. Med. 2020, 11, 16–23. [Google Scholar] [CrossRef]
- El Bohi, K.M.; Abdel-Motal, S.M.; Khalil, S.R.; Abd-Elaal, M.M.; Metwally, M.M.M.; Elhady, W.M. The efficiency of pomegranate (Punica granatum) peel ethanolic extract in attenuating the vancomycin-triggered liver and kidney tissues injury in rats. Environ. Sci. Pollut. Res. 2021, 28, 7134–7150. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Cilleros, D.; López-Oliva, E.; Goya, L.; Martín, M.Á.; Ramos, S. Cocoa intake attenuates renal injury in Zucker Diabetic fatty rats by improving glucose homeostasis. Food Chem. Toxicol. 2019, 127, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boonphang, O.; Ontawong, A.; Pasachan, T.; Phatsara, M.; Duangjai, A.; Amornlerdpison, D.; Jinakote, M.; Srimaroeng, C. Antidiabetic and Renoprotective Effects of Coffea arabica Pulp Aqueous Extract through Preserving Organic Cation Transport System Mediated Oxidative Stress Pathway in Experimental Type 2 Diabetic Rats. Molecules 2021, 26, 1907. [Google Scholar] [CrossRef] [PubMed]
- Perez-Gutierrez, R.M.; Garcia-Campoy, A.H.; Muñiz-Ramirez, A. Properties of Flavonoids Isolated from the Bark of Eysenhardtia polystachya and Their Effect on Oxidative Stress in Streptozotocin-Induced Diabetes Mellitus in Mice. Oxid. Med. Cell. Longev. 2016, 2016, 9156510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Fierros, F.L.; Guarner-Lans, V.; Soto, M.E.; Manzano-Pech, L.; Díaz-Díaz, E.; Soria-Castro, E.; Rubio-Ruiz, M.E.; Jiménez-Trejo, F.; Pérez-Torres, I. Modulation of Renal Function in a Metabolic Syndrome Rat Model by Antioxidants in Hibiscus sabdariffa L. Molecules 2021, 26, 2074. [Google Scholar] [CrossRef] [PubMed]
- Epure, A.; Pârvu, A.E.; Vlase, L.; Benedec, D.; Hanganu, D.; Gheldiu, A.-M.; Toma, V.A.; Oniga, I. Phytochemical Profile, Antioxidant, Cardioprotective and Nephroprotective Activity of Romanian Chicory Extract. Plants 2020, 10, 64. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Yuan, P.; Fu, Y.; Zhang, Q.; Gao, L.; Wei, Y.; Zheng, X.; Feng, W. Geniposide from Gardenia jasminoides var. radicans Makino Attenuates Myocardial Injury in Spontaneously Hypertensive Rats via Regulating Apoptotic and Energy Metabolism Signalling Pathway. Drug Des. Dev. Ther. 2021, 15, 949–962. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-hue, M.; Garc, C.; Palomino-antol, A.; Rubio-Navarro, A.; Cristina, V.; Herencia, C.; Martín-Sanchez, D.; Farré-Alins, V.; Egea, J.; Cannata, P.; et al. Curcumin reduces renal damage associated with rhabdomyolysis by decreasing ferroptosis-mediated cell death. FASEB J. 2019, 33, 8961–8975. [Google Scholar] [CrossRef] [PubMed]
- Benzer, F.; Kandemir, F.M.; Kucukler, S.; Comaklı, S.; Caglayan, C. Chemoprotective effects of curcumin on doxorubicin-induced nephrotoxicity in wistar rats: By modulating inflammatory cytokines, apoptosis, oxidative stress and oxidative DNA damage. Arch. Physiol. Biochem. 2018, 124, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Nerdy, N.; Ritarwan, K. Hepatoprotective Activity and Nephroprotective Activity of Peel Extract from Three Varieties of the Passion Fruit (Passiflora Sp.) in the Albino Rat. Open Access Maced. J. Med. Sci. 2019, 7, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Yousef, H.M.; Alqahtani, A.S.; Ghani, A.S.; El-Toumy, S.A.; El-Dougdoug, W.I.; Hassan, W.H.B.; Hassan, H.M. Nephroprotective, cytotoxic and antioxidant activities of Euphorbia paralias. Saudi J. Biol. Sci. 2021, 28, 785–792. [Google Scholar] [CrossRef]
- Heidarian, E.; Jafari-Dehkordi, E.; Valipour, P.; Ghatreh-Samani, K.; Ashrafi-Eshkaftaki, L. Nephroprotective and Anti-Inflammatory Effects of Pistacia atlantica Leaf Hydroethanolic Extract Against Gentamicin-Induced Nephrotoxicity in Rats. J. Diet. Suppl. 2017, 14, 489–502. [Google Scholar] [CrossRef]
- Ezejiofor, A.N.; Udowelle, N.A.; Orisakwe, O.E. Nephroprotective and antioxidant effect of aqueous leaf extract of Costus afer Ker gawl on cyclosporin-a (Csa) induced nephrotoxicity. Clin. Phytosci. 2016, 2, 11. [Google Scholar] [CrossRef] [Green Version]
- Ranfaing, J.; Dunyach-Remy, C.; Lavigne, J.-P.; Sotto, A. Propolis potentiates the effect of cranberry (Vaccinium macrocarpon) in reducing the motility and the biofilm formation of uropathogenic Escherichia coli. PLoS ONE 2018, 13, e0202609. [Google Scholar] [CrossRef]
- Scharf, B.; Sendker, J.; Dobrindt, U.; Hensel, A. Influence of Cranberry Extract on Tamm-Horsfall Protein in Human Urine and its Antiadhesive Activity Against Uropathogenic Escherichia coli. Planta Med. 2018, 85, 126–138. [Google Scholar] [CrossRef]
- Saremi, J.; Hasheminasab, M.; Sadeghi, N.; Jahromi, H.K. Preventive and curative effects of aqueous extracts of Descurainia sophia L on nephrolithiasis induced in rats. Asian J. Pharm. 2018, 2018, 228–233. [Google Scholar]
- Carneiro, D.M.; Freire, R.C.; Honório, T.C.D.D.; Zoghaib, I.; Cardoso, F.F.D.S.E.S.; Tresvenzol, L.M.F.; De Paula, J.R.; Sousa, A.L.L.; Jardim, P.C.B.V.; Da Cunha, L.C. Randomized, Double-Blind Clinical Trial to Assess the Acute Diuretic Effect ofEquisetum arvense(Field Horsetail) in Healthy Volunteers. Evid.-Based Complement. Altern. Med. 2014, 2014, 760683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallag, A.; Filip, G.A.; Olteanu, D.; Clichici, S.; Baldea, I.; Jurca, T.; Micle, O.; Vicaş, L.; Marian, E.; Soriţău, O.; et al. Equisetum arvense L. Extract Induces Antibacterial Activity and Modulates Oxidative Stress, Inflammation, and Apoptosis in Endothelial Vascular Cells Exposed to Hyperosmotic Stress. Oxid. Med. Cell. Longev. 2018, 2018, 3060525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, G.; Shin, J.; Choi, H.; Jo, A.; Pan, S.; Bae, D.; Lee, Y.; Choi, C. Cynanchum wilfordii Ameliorates Testosterone-Induced Benign Prostatic Hyperplasia by Regulating 5α-Reductase and Androgen Receptor Activities in a Rat Model. Nutrients 2017, 9, 1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leibbrand, M.; Siefer, S.; Schön, C.; Perrinjaquet-Moccetti, T.; Kompek, A.; Csernich, A.; Bucar, F.; Kreuter, M.H. Effects of an Oil-Free Hydroethanolic Pumpkin Seed Extract on Symptom Frequency and Severity in Men with Benign Prostatic Hyperplasia: A Pilot Study in Humans. J. Med. Food 2019, 22, 551–559. [Google Scholar] [CrossRef] [Green Version]
- Csikós, E.; Horváth, A.; Ács, K.; Papp, N.; Balázs, V.L.; Dolenc, M.S.; Kenda, M.; Glavač, N.K.; Nagy, M.; Protti, M.; et al. Treatment of Benign Prostatic Hyperplasia by Natural Drugs. Molecules 2021, 26, 7141. [Google Scholar] [CrossRef]
- Beaver, L.M.; Lӧhr, C.V.; Clarke, J.; Glasser, S.T.; Watson, G.W.; Wong, C.P.; Zhang, Z.; Williams, D.E.; Dashwood, R.H.; Shannon, J.; et al. Broccoli Sprouts Delay Prostate Cancer Formation and Decrease Prostate Cancer Severity with a Concurrent Decrease in HDAC3 Protein Expression in Transgenic Adenocarcinoma of the Mouse Prostate (TRAMP) Mice. Curr. Dev. Nutr. 2018, 2, nzy002. [Google Scholar] [CrossRef]
- Stephens, J.W.; Brown, K.E.; Min, T. Chronic kidney disease in type 2 diabetes: Implications for managing glycaemic control, cardiovascular and renal risk. Diabetes Obes. Metab. 2020, 22, 32–45. [Google Scholar] [CrossRef]
- Bharadwaj, D.; Singh, A. Genetic basis for increased risk for vascular diseases in diabetes. In Mechanisms of Vascular Defects in Diabetes Mellitus; Kartha, C., Ramachandran, S., Pillai, R.M., Eds.; India Springer: New Delhi, India, 2017; pp. 27–45. [Google Scholar]
- Cupisti, A.; Giannese, D.; Moriconi, D.; D’Alessandro, C.; Torreggiani, M.; Piccoli, G.B. Nephroprotection by SGLT2i in CKD Patients: May It Be Modulated by Low-Protein Plant-Based Diets? Front. Med. 2020, 7, 622593. [Google Scholar] [CrossRef]
- Hall, J.; Hall, M. Adrenocorcical hormones. In Guyton and Hall Textbook of Medical Physiology, 14th ed.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 955–987. [Google Scholar]
- Esquivel-Gutiérrez, E.R.; Manzo-Avalos, S.; Peña-Montes, D.J.; Saavedra-Molina, A.; Morreeuw, Z.P.; Reyes, A.G. Hypolipidemic and Antioxidant Effects of Guishe Extract from Agave lechuguilla, a Mexican Plant with Biotechnological Potential, on Streptozotocin-Induced Diabetic Male Rats. Plants 2021, 10, 2492. [Google Scholar] [CrossRef]
- Cardador-Martínez, A. Medicinal plants with the potential to treat hypertension: Studies that were done in the last decade. In Medicinal Plants for the Treatment of Metabolic Disorders, 1st ed.; Cardador Martínez, A., Rodriguez, V., Manzano-Santana, P., Alonzo, M., Eds.; Nova Medicine & Health: Mexico, NM, USA, 2020; pp. 24–25. [Google Scholar]
- O’Shea, P.; Griffin, T.P.; Fitzgibbon, M. Hypertension: The role of biochemistry in the diagnosis and management. Clin. Chim. Acta 2017, 465, 131–143. [Google Scholar] [CrossRef]
- Kjeldsen, S.; Feldman, R.D.; Lisheng, L.; Mourad, J.-J.; Chiang, C.-E.; Zhang, W.; Wu, Z.; Liu, L.; Williams, B. Updated National and International Hypertension Guidelines: A Review of Current Recommendations. Drugs 2014, 74, 2033–2051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugh, D.; Gallacher, P.J.; Dhaun, N. Management of Hypertension in Chronic Kidney Disease. Drugs 2019, 79, 365–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxena, T.; Ali, A.O.; Saxena, M. Pathophysiology of essential hypertension: An update. Expert Rev. Cardiovasc. Ther. 2018, 16, 879–887. [Google Scholar] [CrossRef]
- Ku, E.; McCulloch, C.E.; Vittinghoff, E.; Lin, F.; Johansen, K.L. Use of Antihypertensive Agents and Association with Risk of Adverse Outcomes in Chronic Kidney Disease: Focus on Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers. J. Am. Hear. Assoc. 2018, 7, e009992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levi, M.; Takahashi, S.; Wang, X.; Levi, M. The Kidney in Liver Disease. In The Liver Biology and Pathobiol, 6th ed.; John Wiley & Sons, Ltd.: Chichister, UK, 2020; pp. 619–638. [Google Scholar]
- Ramachandran, A.; Visschers, R.G.J.; Duan, L.; Akakpo, J.Y.; Jaeschke, H. Mitochondrial dysfunction as a mechanism of drug-induced hepatotoxicity: Current understanding and future perspectives. J. Clin. Transl. Res. 2018, 4, 75–100. [Google Scholar]
- Rajakumar, A.; Appuswamy, E.; Kaliamoorthy, I.; Rela, M. Renal Dysfunction in Cirrhosis: Critical Care Management. Indian J. Crit. Care Med. 2021, 25, 207–214. [Google Scholar] [CrossRef]
- Ramachandran, A.; Jaeschke, H. Experimental Models of Hepatotoxicity for the Testing of Natural Products [Internet]; Reference Module in Chemistry, Molecular Sciences and Chemical Engineering; Elsevier Inc.: Amsterdam, The Netherlands, 2016; pp. 1–9. [Google Scholar] [CrossRef]
- Weber, E.J.; Lidberg, K.A.; Wang, L.; Bammler, T.K.; Macdonald, J.W.; Li, M.J.; Redhair, M.; Atkins, W.M.; Tran, C.; Hines, K.; et al. Human kidney on a chip assessment of polymyxin antibiotic nephrotoxicity. JCI Insight 2018, 3, e123673. [Google Scholar] [CrossRef] [Green Version]
- Winther, S.A.; Øllgaard, J.C.; Hansen, T.W.; von Scholten, B.J.; Reinhard, H.; Ahluwalia, T.S.; Wang, Z.; Gæde, P.; Parving, H.-H.; Hazen, S.; et al. Plasma trimethylamine N-oxide and its metabolic precursors and risk of mortality, cardiovascular and renal disease in individuals with type 2-diabetes and albuminuria. PLoS ONE 2021, 16, e0244402. [Google Scholar] [CrossRef] [PubMed]
- Wiese, G.N.; Biruete, A.; Moorthi, R.N.; Moe, S.M.; Lindemann, S.R.; Gallant, K.M.H. Plant-Based Diets, the Gut Microbiota, and Trimethylamine N-Oxide Production in Chronic Kidney Disease: Therapeutic Potential and Methodological Considerations. J. Ren. Nutr. 2021, 31, 121–131. [Google Scholar] [CrossRef]
- Du, F.; Huang, R.; Lin, D.; Wang, Y.; Yang, X.; Huang, X.; Zheng, B.; Chen, Z.; Huang, Y.; Wang, X.; et al. Resveratrol Improves Liver Steatosis and Insulin Resistance in Non-alcoholic Fatty Liver Disease in Association with the Gut Microbiota. Front. Microbiol. 2021, 12, 611323. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Chen, T.; Ma, D.; Wang, X.; Zhao, X.; Tian, P.; Wang, H.; Hai, Z.; Shen, L.; Tang, X.; et al. Reclamation of Herb Residues Using Probiotics and Their Therapeutic Effect on Diarrhea. Mediat. Inflamm. 2017, 2017, 4265898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boudhabhay, I.; Poillerat, V.; Grunenwald, A.; Torset, C.; Leon, J.; Daugan, M.V.; Lucibello, F.; El Karoui, K.; Ydee, A.; Chauvet, S. Complement activation is a crucial driver of acute kidney injury in rhabdomyolysis. Kidney Int. 2021, 99, 581–597. [Google Scholar] [CrossRef] [PubMed]
- Cortés, R.; Kleinsteuber, K.; Vargas, C.P.; Avaria, M.D.L. Ángeles Rabdomiólisis metabólica: Actualización. Rev. Médica Clínica Las Condes 2018, 29, 553–559. [Google Scholar] [CrossRef]
- Teng, C.; Baus, C.; Wilson, J.P.; Frei, C.R. Rhabdomyolysis Associations with Antibiotics: A Pharmacovigilance Study of the FDA Adverse Event Reporting System (FAERS). Int. J. Med. Sci. 2019, 16, 1504–1509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okubo, K.; Kurosawa, M.; Kamiya, M.; Urano, Y.; Suzuki, A.; Yamamoto, K.; Hase, K.; Homma, K.; Sasaki, J.; Miyauchi, H.; et al. Macrophage extracellular trap formation promoted by platelet activation is a key mediator of rhabdomyolysis-induced acute kidney injury. Nat. Med. 2018, 24, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Chen, A.-B.; Duan, Y.-C.; Liao, R.; Xu, Y.-W.; Tao, L.-L. Multiple organ dysfunction and rhabdomyolysis associated with moonwort poisoning: Report of four cases. World J. Clin. Cases 2020, 8, 479–486. [Google Scholar] [CrossRef]
- Kang, C.-I.; Kim, J.; Park, D.W.; Kim, B.-N.; Ha, U.-S.; Lee, S.-J.; Yeo, J.; Min, S.K.; Lee, H.; Wie, S.-H. Clinical Practice Guidelines for the Antibiotic Treatment of Community-Acquired Urinary Tract Infections. Infect. Chemother. 2018, 50, 67–100. [Google Scholar] [CrossRef] [PubMed]
- Kline, K.A.; Lewis, A.L. Gram-Positive Uropathogens, Polymicrobial Urinary Tract Infection, and the Emerging Microbiota of the Urinary Tract. Microbiol. Spectr. 2016, 4, 459–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, P.D.; McLellan, L.K.; Liu, A.; Briden, K.E.; Tiemann, K.M.; Daugherty, A.L.; Hruska, K.A.; Hunstad, D.A. Correction: Renal scar formation and kidney function following antibiotic-treated murine pyelonephritis. Dis. Model. Mech. 2018, 11, 1371–1379. [Google Scholar] [CrossRef] [Green Version]
- Nirumand, M.C.; Hajialyani, M.; Rahimi, R.; Farzaei, M.H.; Zingue, S.; Nabavi, S.M.; Bishayee, A. Dietary Plants for the Prevention and Management of Kidney Stones: Preclinical and Clinical Evidence and Molecular Mechanisms. Int. J. Mol. Sci. 2018, 19, 765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, F.M.D.; Peres, A.K.; Mandotti, M.R.; Peres, L.A.B. Metabolic investigation in patients with nephrolithiasis. Einstein 2017, 15, 452–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.; Zhao, D.; Spring, D.J.; Depinho, R.A. Genetics and biology of prostate cancer. Genes Dev. 2018, 32, 1105–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardwell, C.R.; O’Sullivan, J.M.; Jain, S.; Hicks, B.M.; Devine, P.A.; McMenamin, Ú.C. Hormone therapy use and the risk of acute kidney injury in patients with prostate cancer: A population-based cohort study. Prostate Cancer Prostatic Dis. 2021, 24, 1055–1062. [Google Scholar] [CrossRef]
- Daskivich, T.J. Androgen deprivation therapy and acute kidney injury in prostate cancer: Room for debate? Prostate Cancer Prostatic Dis. 2021, 24, 933–934. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plant | Origin | Extract/Compounds | Model of Study | Disease | Mechanism of Action | Renal Effect | Reference |
|---|---|---|---|---|---|---|---|
| Tinospora crispa | Southeast Asia and Africa | Genkwanin | Albino Wistar rats + CCl4 | Hepatic injury | Increase SOD activity | Pre-renal | [50] |
| Cirsium vulgare and Cirsium ehrenbergii | Amazon basin | Lupeol acetate | Male Wistar rats + CCl4 | Hepatic injury | Prevent depletion of glycogen, antioxidant and anti-inflammatory effects | Pre-renal | [51] |
| Suaeda vermiculata | South Africa | Quercetin, quercetin-3-O-rutinoside, and kaempferol-O-(acetyl)-hexoside-pentoside | Male Sprague Dawley rats + CCl4 | Hepatic injury | Decrease AST and ALT | Pre-renal | [52] |
| Descurainia Sophia | Europe and northern Africa | Dried seed ethyl alcohol Extract | Swiss albino mice + acetaminophen | Hepatic injury by NSAID | Reduce inflammation, swelling and necrosis | Pre-renal | [53] |
| Eurycoma longifolia | Indonesia | Standardized aqueous extract of the roots (“Physta” from the brand Biotropics) | Wistar rats + paracetamol | Hepatic injury by NSAID | Increase antioxidant enzymes, improves biomarkers of kidney function, and histopathology changes | Pre-renal | [54] |
| Arbutus pavarii | Libya | Gallic acid, epicatechin, dimeric forms of B-type Proanthocyanidins, quercetin, flavonoids, and phenolic acid | Disc Diffusion Assay | Hepatic injury by antibiotics | Exert bacteriostatic and bactericidal effect, against different methicillin-resistant Staphylococcus aureus strains | Pre-renal | [55] |
| Punica granatum | India | Dulcitol, loganin, bergenin, quercitrin, cosmosin, folic acid, khayanthone | Wistar rats + gentamicin | Antibiotics/infections | Improve kidney function biomarkers, exerted antioxidant activity, and ameliorated histological changes | Pre-renal and intrinsic | [56] |
| Punica granatum | India | Fruit peel ethanolic extract. Polyphenols. | Wistar rats + gentamicin | Antibiotic-induced liver and kidney damage | Protect the tissues against ROS-mediated oxidative damage and modulate the inflammatory response | Pre-renal and intrinsic | [57] |
| Cocoa (Theobroma cacao) | Mexico | Hydroalcoholic extract of Natural Forastero cocoa powder. | Zucker diabetic fatty rats | Type 2 DM | Decrease glucose levels | Pre-renal | [58] |
| Coffea arabica | Africa | Pulp aqueous extract | Wistar rats + high-fat diet | Type 2 DM | Raise catalase levels | Pre-renal and intrinsic | [59] |
| Eysenhardtia polystachya | Mexico | Methanolic bark extract | Mice + streptozotocin | Type 2 DM | Decrease oxidative stress | Pre-renal and intrinsic | [60] |
| Anchomanes difformis | Africa | Aqueous leaf extract | Wistar rats + fructose and streptozotocin | DM related with pancreas | Induce dissociation of Nrf2/keap, activating Nrf2, reduced oxidative stress | Pre-renal | [45] |
| Hibiscus sabdariffa | Asia, Africa, Central America | Calyx aqueous extract | Wistar rats + 30% sucrose | Metabolic syndrome | Increase the antioxidant systems including non-enzymatic and enzymatic effect | Pre-renal | [61] |
| Hibiscus sabdariffa | Asia, Africa, Central America | Calyx aqueous extract and dried powdered calyx Hibiscus acid, anthocyanins, chlorogenic acid | Humans with uncontrolled hypertension | Hypertension | Regulate blood pressure | Pre-renal | [46] |
| Cichorium intybus | Saudi Arabia | 1,4- naphthalenedione, oleic acid, β-asarone, naphtho furanone, p-methoxycinnamate, hexadecanoic acid | Wistar albino rats + ISO-induced myocardial ischemia model | Hypertension | Improve the systolic function and increase the levels of LVEF and LVFS | Pre-renal and post-renal | [62] |
| Gardenia jasminoides | Asia | Geniposide | Wistar SHR, and Wistar Kyoto rats | Myocardial ischemia | Exert antioxidant activity and decreased CK-MB, AST, ALT, and MDA levels. | Pre-renal and post-renal | [63] |
| Curcuma longa | India | Curcumin | C57BL/6J mice Glycerol | Rhabdomyolysis | Reduce ROS, inflammation, and histopathology changes | Pre-renal | [64] |
| Curcuma longa | India | Curcumin | Wistar rats + doxorubicin | Nephrotoxicity | Increase enzymatic antioxidant activity | Pre-renal and intrinsic | [65] |
| Passion fruit (Passiflora spp.) | North America | Methanolic peel extract Gallic acid, Ellagic acid, Kaempferol and Quercetin glycosides | Albino rats + paracetamol | Nephrotoxicity | Keep urea and creatinine at normal levels | Pre-renal and intrinsic | [66] |
| Euphorbia paralias | Europe, western Asia, and northern Africa | Methanolic extract of aerial parts | Sprague-Dawley rats + thioacetamide | Nephrotoxicity | Reduce levels of urea and creatinine | Pre-renal and intrinsic | [67] |
| Pistacia atlantica | North Africa, Middle East, Iran, and Afghanistan | Leaf hydroethanolic extract | Wistar rats + gentamicin | Nephrotoxicity | Decrease levels of urea, creatinine, and uric acid | Pre-renal and intrinsic | [68] |
| Costus afer | Africa | Aqueous leaf extract | Wistar rats + cyclosporine | Nephrotoxicity | Decrease serum potassium and BUN levels | Pre-renal and Intrinsic | [69] |
| Cranberry (Vaccinium sp.) | North America | “Exocyan” brand natural cranberry extract. “Nutrican” brand cranberry dry extract. | Uropathogenic Escherichia coli | Urinary tract infections | Decrease E. coli adhesion, and reduce bacterial motility and biofilm formation | Post-renal | [70,71] |
| Descurainia sophia | Europe and northern Africa | Aqueous seed extract | Male Wistar rats + Ammonium chloride + ethylene glycol | Lithiasis | Decrease the deposition of calcium oxalate and amount of tissue damage | Post-renal | [72] |
| Equisetum arvense | Spain | Dry standardized extract of aerial parts. Alcoholic extract of sterile stems | Clinical trial Healthy male volunteers | Urinary retention andinfections | Diuretic action and effective against Candida tropicalis, Candida glabrata, Candida albicans, Staphylococcus epidermidis, Streptococcus mutans and Staphylococcus aureus | Post-renal | [73,74] |
| Cynanchum wilfordii | Korea | 4-hydroxyacetophenone and 2,4-hydroxyacetophenone | Male Sprague-Dawley rats + testosterone | Benign prostatic hyperplasia | Decreased testosterone and DHT, via downregulation of androgen receptor 5α gene expression | Post-renal | [75] |
| Pumpkin (Cucurbita pepo) | Mexico | Oil-free hydroethanolic pumpkin seed extract.Phytosterols and fatty acids | Open mono-center trial men with symptomatic benign prostatic hyperplasia. | Benign prostatic hyperplasia | Decrease residual urine volume and nocturia.Inhibit 5α reductase and decrease DHT level. | Post-renal | [76,77] |
| Broccoli (Brassica oleracea var. Italica) | Italy | Broccoli Sprouts Powder from Natural Sprouts Company, LLC | TRAMP | Prostate cancer | Decrease HDAC expression, and decline the acetylation of histone H3 lysine 18 and H3K9 | Post-renal | [78] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tienda-Vázquez, M.A.; Morreeuw, Z.P.; Sosa-Hernández, J.E.; Cardador-Martínez, A.; Sabath, E.; Melchor-Martínez, E.M.; Iqbal, H.M.N.; Parra-Saldívar, R. Nephroprotective Plants: A Review on the Use in Pre-Renal and Post-Renal Diseases. Plants 2022, 11, 818. https://doi.org/10.3390/plants11060818
Tienda-Vázquez MA, Morreeuw ZP, Sosa-Hernández JE, Cardador-Martínez A, Sabath E, Melchor-Martínez EM, Iqbal HMN, Parra-Saldívar R. Nephroprotective Plants: A Review on the Use in Pre-Renal and Post-Renal Diseases. Plants. 2022; 11(6):818. https://doi.org/10.3390/plants11060818
Chicago/Turabian StyleTienda-Vázquez, Mario Adrián, Zoé P. Morreeuw, Juan Eduardo Sosa-Hernández, Anaberta Cardador-Martínez, Ernesto Sabath, Elda M. Melchor-Martínez, Hafiz M. N. Iqbal, and Roberto Parra-Saldívar. 2022. "Nephroprotective Plants: A Review on the Use in Pre-Renal and Post-Renal Diseases" Plants 11, no. 6: 818. https://doi.org/10.3390/plants11060818