

Ethnobotanical Survey of Medicinal Plants Used in the Treatment of COVID-19 and Related Respiratory Infections in Ogbomosho South and North Local Government Areas, Oyo State, Nigeria

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
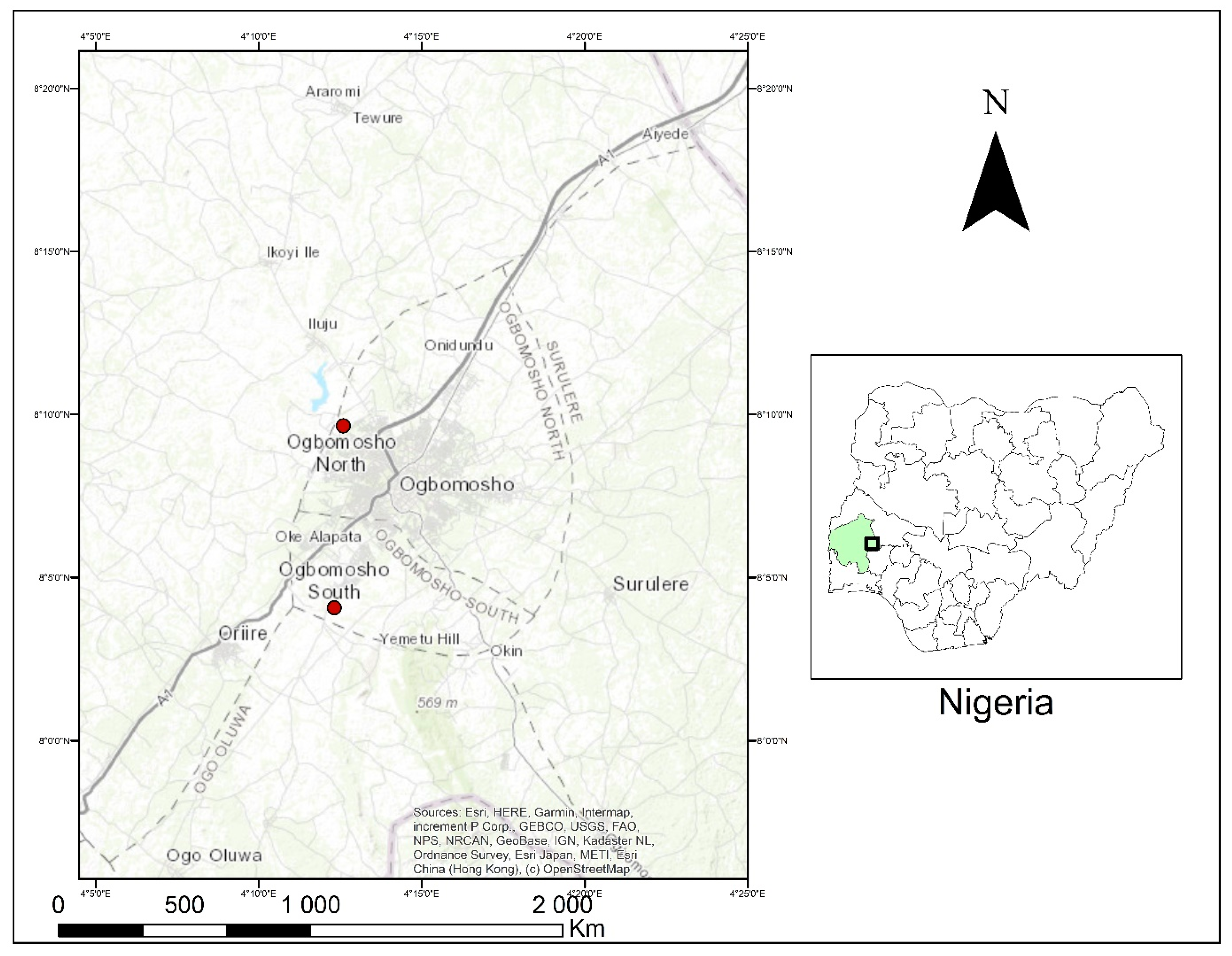
2.1. Study Area
2.2. Collection of Data
2.3. Collection and Identification of Medicinal Plants
2.4. Data Analysis
2.5. Ethical Approval
3. Results and Discussion
3.1. Demographic Information
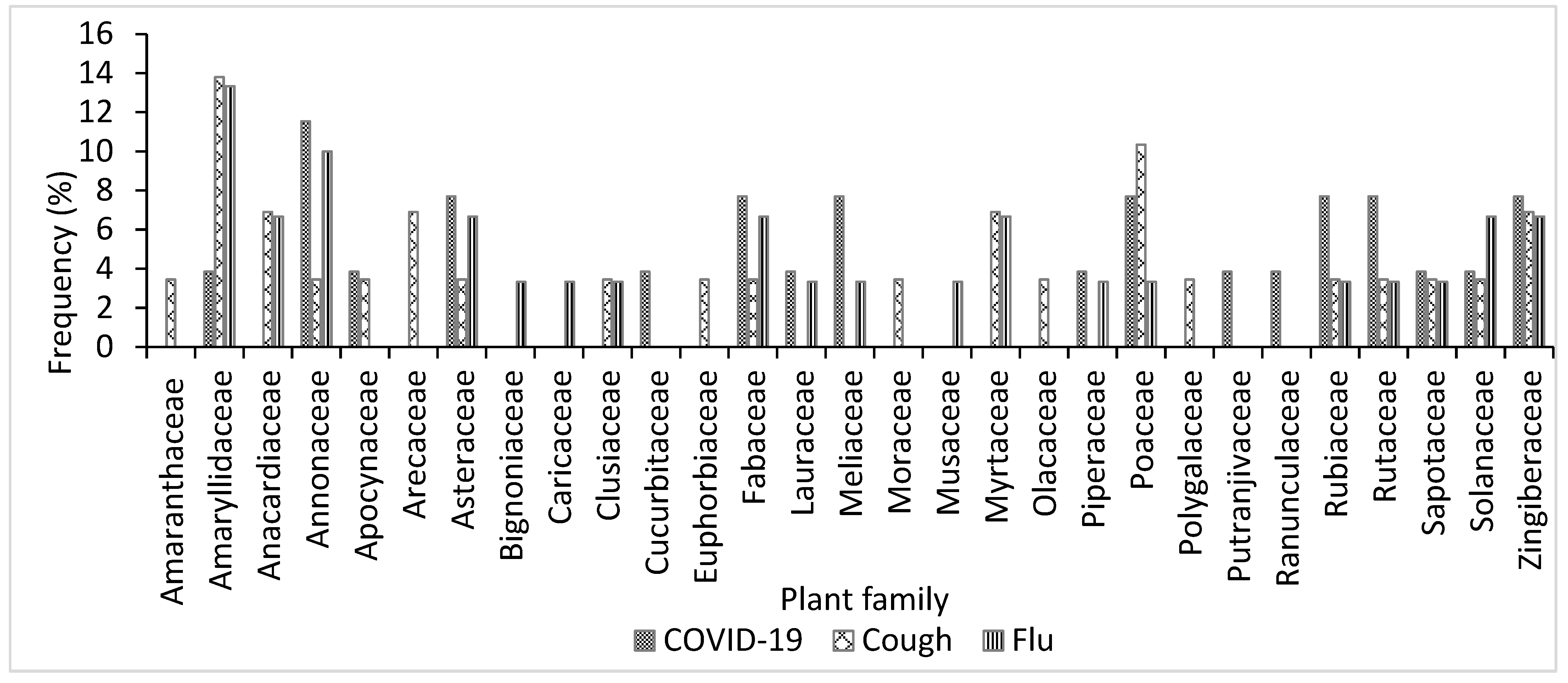
3.2. Medicinal Plants Recorded
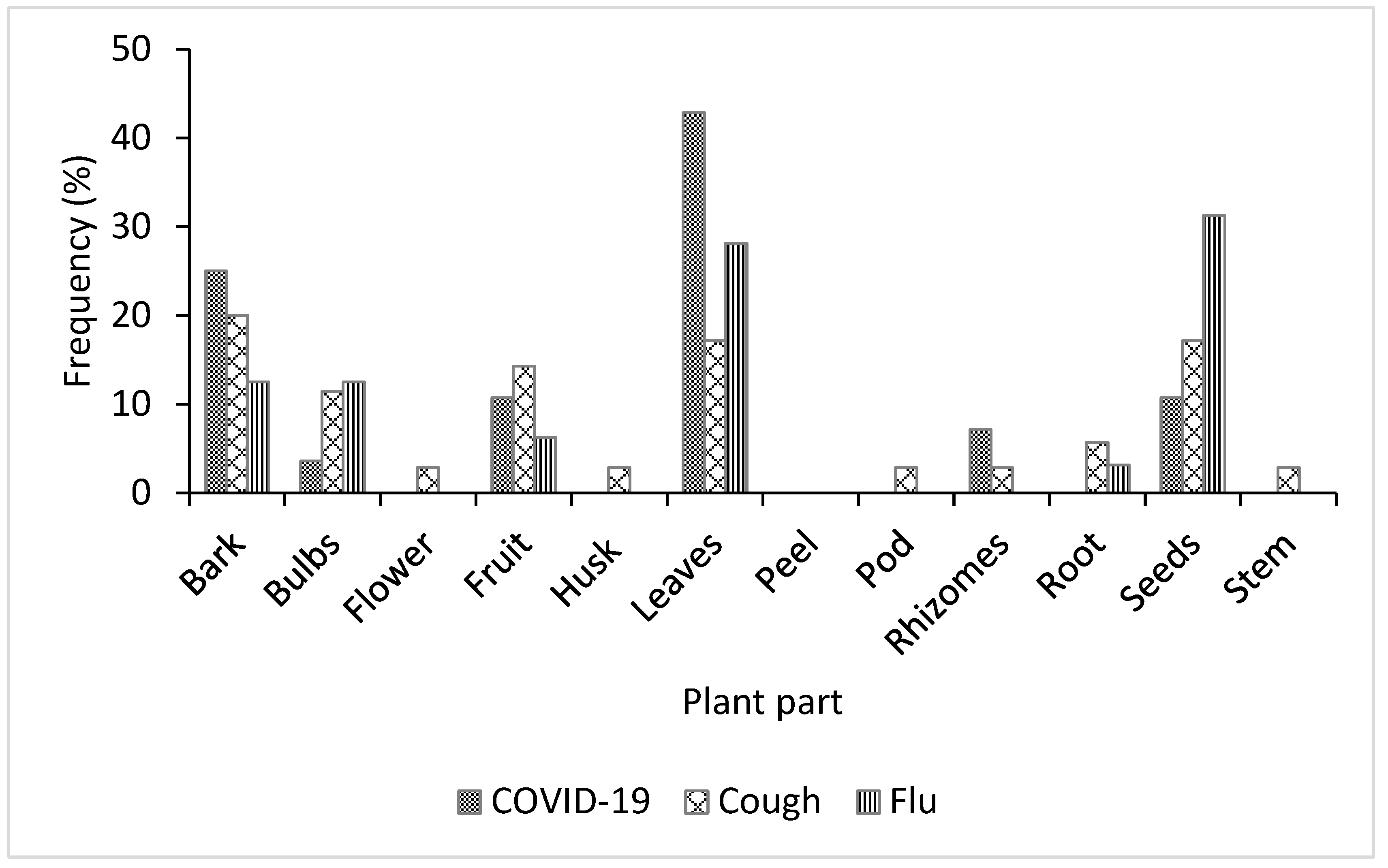
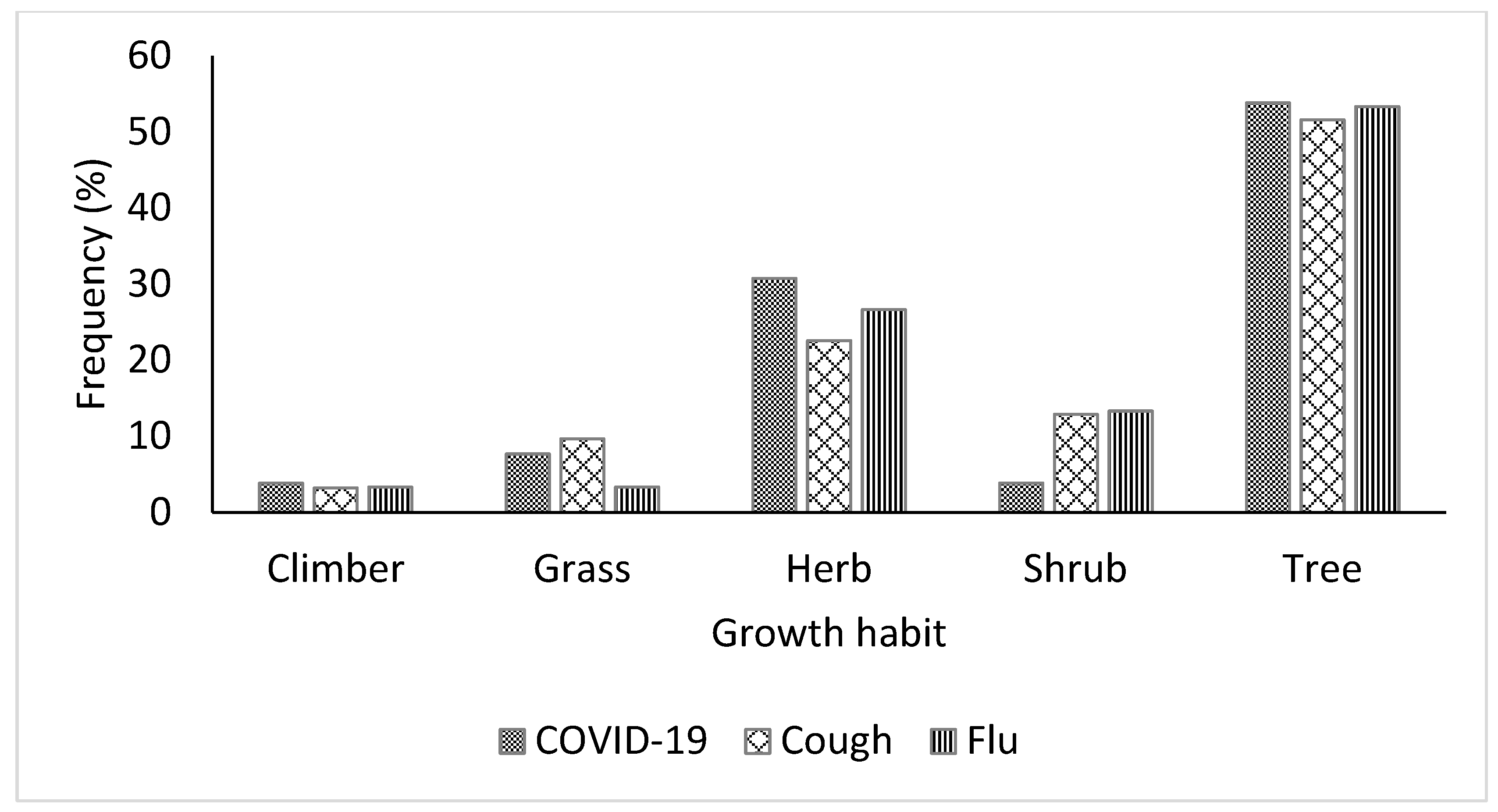
3.3. Plant Parts and Growth Forms of Medicinal Plants Used for Treating COVID-19, Cough, and Flu
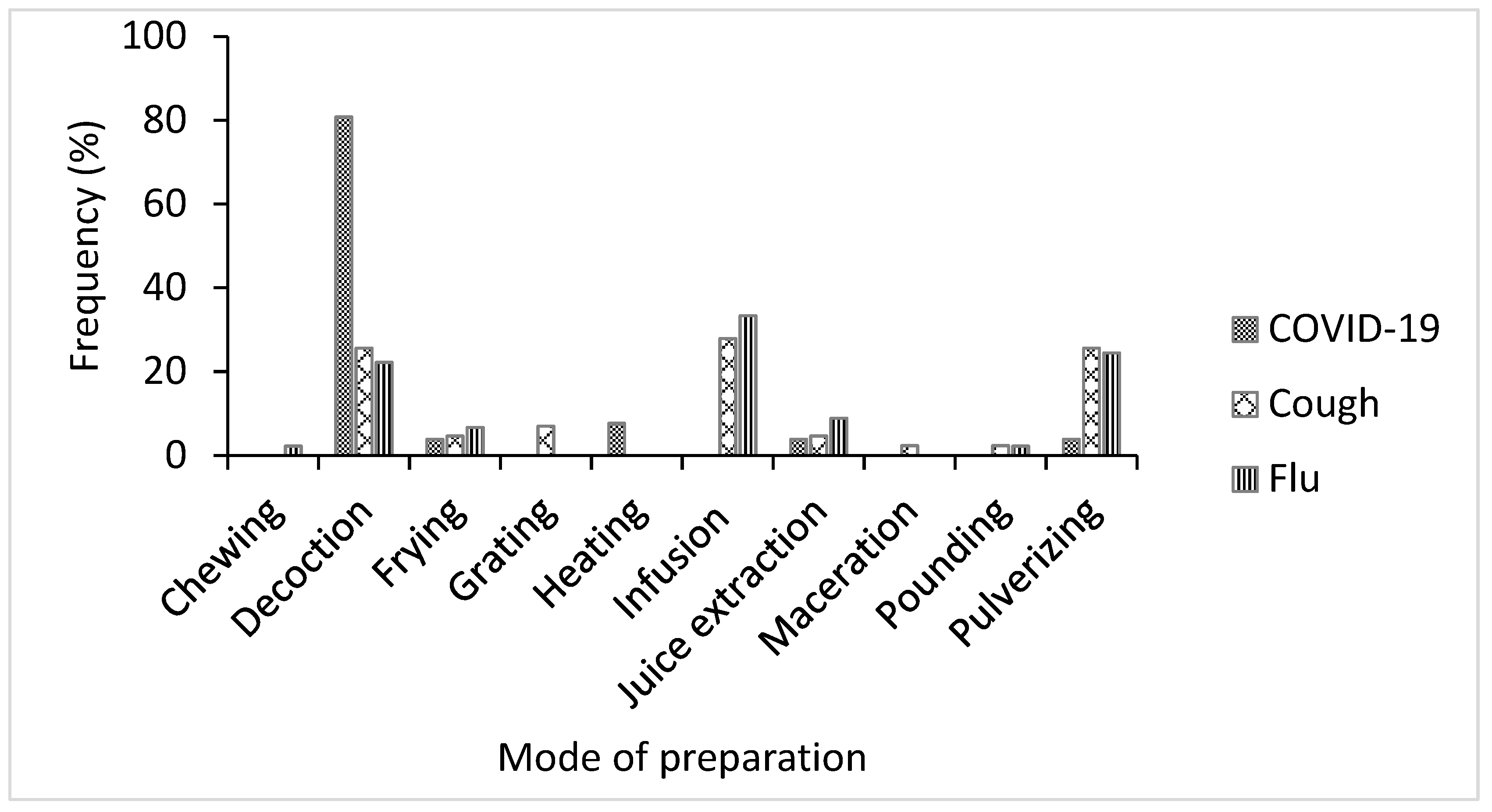
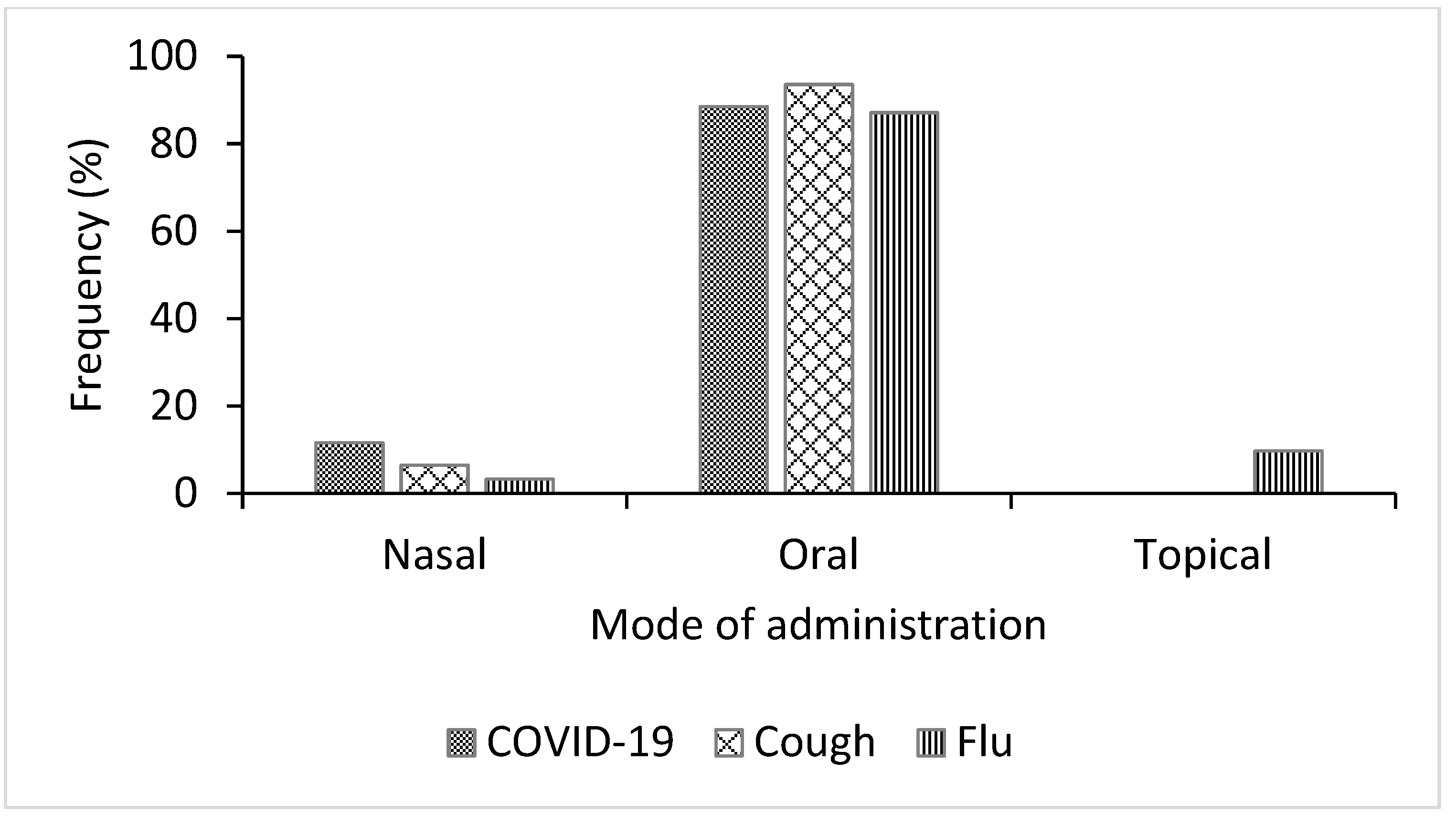
3.4. Method of Preparation and Mode of Administration of Medicinal Plants Species Used for Treating COVID-19, Cough, and Flu
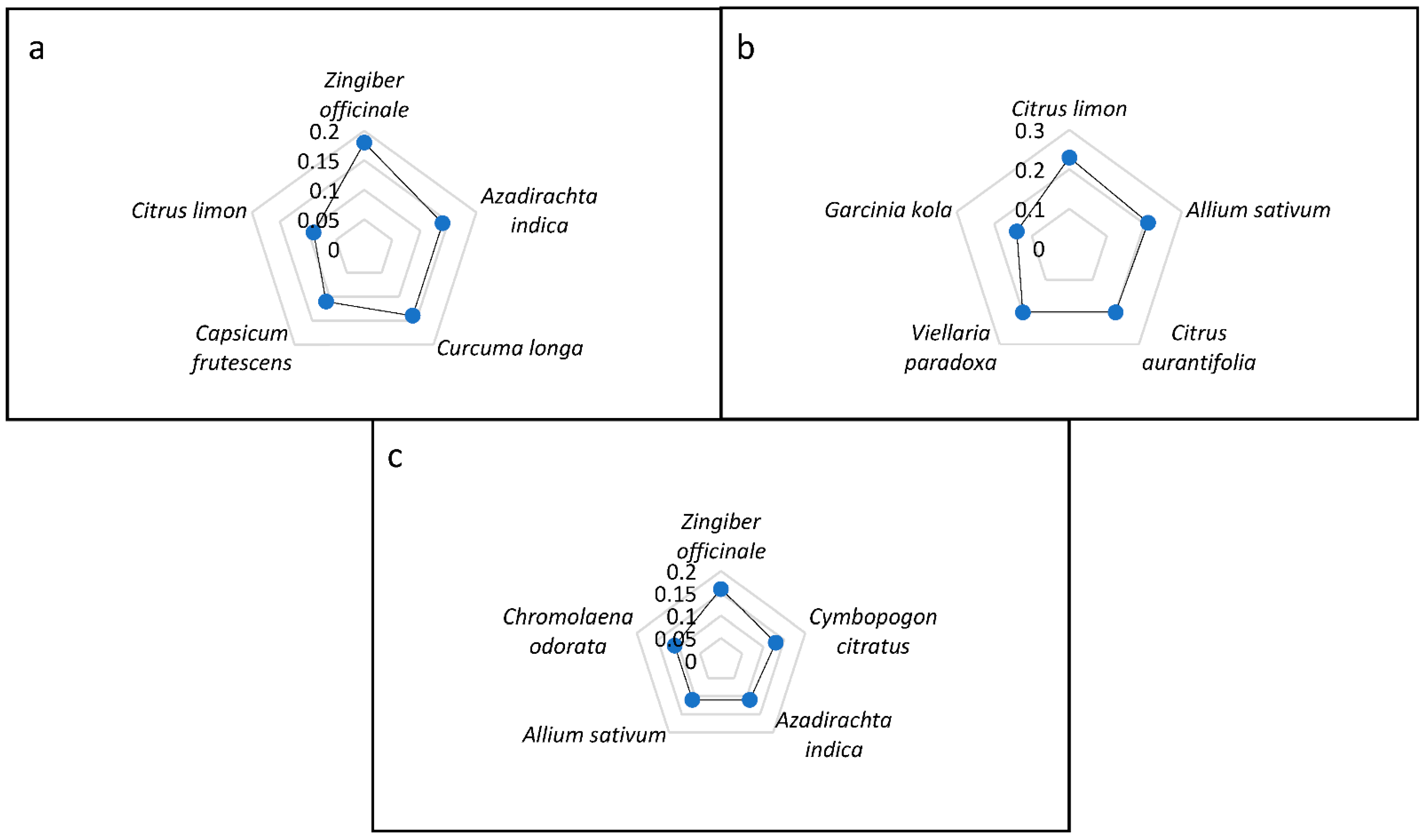
3.5. Ethnobotanical Indices of Medicinal Plants Recorded
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jin, X.; Ren, J.; Li, R.; Gao, Y.; Zhang, H.; Li, J.; Zhang, J.; Wang, X.; Wang, G. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. E Clin. Med. 2021, 37, 100986. [Google Scholar] [CrossRef]
- José, R.J. Respiratory infections: A global burden. Ann. Res. Hosp. 2018, 2, 1–4. [Google Scholar] [CrossRef]
- Kyere, K.; Aremu, T.O.; Ajibola, O.A. Availability bias and the COVID-19 pandemic: A case study of Legionella Pneumonia. Cureus 2022, 14, e25846. [Google Scholar] [CrossRef]
- Juscamayta-Lopez, T.D.; Valdivia, F.R.; Carhuaricra, D.M. Phylogenomics reveals multiple introductions and early spread of SARS-CoV-2 into Peru. BioRxiv 2020, 10, 5961–5968. [Google Scholar] [CrossRef]
- González-Bustamante, B. Evolution and early government responses to COVID-19 in South America. World Dev. 2021, 1, 105180. [Google Scholar] [CrossRef]
- Viner, R.M.; Ward, J.L.; Hudson, L.D.; Ashe, M.P.; Hargreaves, D.; Whittaker, E. Systematic review of reviews of symptoms and signs of COVID-19 in children and adolescents. Arch. Dis. Child. 2021, 106, 802–807. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). Coronavirus: Symptoms. Available online: https://www.who.int/health-topics/coronavirus#tab%20=%20tab_32021 (accessed on 2 June 2022).
- World Health Organization (WHO). 14.9 Million Excess Deaths Associated with the COVID-19 Pandemic in 2020 and 2021. 2022. Available online: https://www.who.int/news/item/05-05-2022-14.9-million-excess-deaths-were-associated-with-the-covid-19-pandemic-in-2020-and-2021 (accessed on 27 May 2022).
- Pradhan, D.; Biswasroy, P.; Naik, P.K.; Ghosh, G.; Rath, G. A review of current interventions for COVID-19 prevention. Arch. Med. Res. 2020, 51, 363–374. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration (FDA). Coronavirus (COVID-19) Update: FDA Authorizes First Oral Antiviral for Treatment of COVID-19. FDA. 2021. Published 22 December 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-oral-antiviral-treatment-covid-19 (accessed on 26 June 2022).
- Farly, J. FDA Updates on Paxlovid for Health Care Providers. U.S. Food & Drug Administration (FDA). 2022. Published online 4 May 2022. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-updates-paxlovid-health-care-providers (accessed on 26 June 2022).
- Nugraha, R.V.; Ridwansyah, H.G.; Khairani, A.F.; Atik, N. Traditional herbal medicine candidates as complementary treatments for COVID-19: A review of their mechanisms, pros and cons. Evid. -Based Complement. Altern. Med. 2020, 2560645. [Google Scholar] [CrossRef]
- Thimmulappa, R.K.; Mudnakudu-Nagaraju, K.K.; Shivamallu, C.; Subramaniam, K.T.; Radhakrishnan, A.; Bhojraj, S.; Kuppusamy, G. Antiviral and immunomodulatory activity of curcumin: A case for prophylactic therapy for COVID-19. Heliyon 2021, 7, e06350. [Google Scholar] [CrossRef]
- Paudyal, V.; Sun, S.; Hussain, R.; Abutaleb, M.H.; Hedima, E.W. Complementary and alternative medicines use in COVID-19: A global perspective on practice, policy and research. Res. Soc. Adm. Pharm. 2022, 18, 2524–2528. [Google Scholar] [CrossRef]
- Shrestha, P.M.; Dhillion, S.S. Medicinal plant diversity and use in the highlands of Dolakha district, Nepal. J. Ethnopharmacol. 2003, 86, 81–96. [Google Scholar] [CrossRef]
- Hughes, G.D.; Aboyade, O.M.; Okonji, C.O.; Clark, B.; Mabweazara, S.Z. Comparison of the prevalence of non-communicable diseases and traditional herbal medicine use in urban and rural communities in South Africa. Adv. Integr. Med. 2021, 8, 136–143. [Google Scholar] [CrossRef]
- Ssenku, J.E.; Okurut, S.A.; Namuli, A.; Kudamba, A.; Tugume, P.; Matovu, P.; Walusansa, A. Medicinal plant use, conservation, and the associated traditional knowledge in rural communities in Eastern Uganda. Trop. Med. Health 2022, 50, 39. [Google Scholar] [CrossRef]
- Iwu, M.M.; Duncan, A.R.; Okunji, C.O. New Antimicrobials of Plant Origin. In Perspectives on New Crops and New Uses; Janick, J., Ed.; ASHS Press: Alexandria, VA, USA, 1999; pp. 457–462. ISBN 13: 9780961502706. [Google Scholar]
- Okaiyeto, K.; Oguntibeju, O.O. African herbal medicines: Adverse effects and cytotoxic potentials with different therapeutic applications. Int. J. Environ. Res. Public Health 2021, 18, 5988. [Google Scholar] [CrossRef]
- Khadka, D.; Dhamala, M.K.; Li, F.; Aryal, P.C.; Magar, P.R.; Bhatta, S. The use of medicinal plants to prevent COVID-19 in Nepal. J. Ethnobiol. Ethnomed. 2021, 17, 26. [Google Scholar] [CrossRef]
- Silva, F.S.; Ramos, M.A.; Hanazaki, N.; UPd, A. Dynamics of traditional knowledge of medicinal plants in a rural community in the Brazilian semi-arid region. Rev. Bras. Farmacogn. 2011, 21, 382–391. [Google Scholar] [CrossRef]
- Arshad, M.; Ahmad, M.; Ahmed, E.; Saboor, A.; Abbas, A.; Sadiq, S. An ethnobiological study in Kala Chitta hills of Pothwar region, Pakistan: Multinomial logit specification. J. Ethnobiol. Ethnomed. 2014, 10, 13. [Google Scholar] [CrossRef] [Green Version]
- Cox, P.A. Will tribal knowledge survive the millennium? Science 2000, 287, 44–45. [Google Scholar] [CrossRef] [Green Version]
- Falemara, B.C.; Joshua, V.I.; Ogunkanmi, T.I.; Mbeng, W.O. Ethnomedicinal survey of indigenous medicinal plants in Jos Metropolis, Nigeria. J. Med. Plants Econ. Dev. 2021, 5, 128. [Google Scholar] [CrossRef]
- Borokini, T.I.; Lawal, I.O. Traditional medicine practices among the Yoruba people of Nigeria: A historical perspective. J. Med. Plants Stud. 2014, 2, 20–33. [Google Scholar]
- Ajao, A.A.; Mukaila, Y.O.; Sabiu, S. Wandering through southwestern Nigeria: An inventory of Yoruba useful angiosperm plants. Heliyon 2021, 8, e08668. [Google Scholar] [CrossRef]
- Olorunnisola, O.S.; Adetutu, A.; Afolayan, A.J. An inventory of plants commonly used in the treatment of some disease conditions in Ogbomoso, South West, Nigeria. J. Ethnopharmacol. 2015, 161, 60–68. [Google Scholar] [CrossRef]
- Federal Republic of Nigeria, 2006 Population Census. Available online: http://www.nigerianstat.gov.ng/nbsapps/Connections/Pop2006.pdf (accessed on 20 May 2022).
- Thiers, B. Index Herbariorum: A global Directory of Public Herbaria and Associated Staff. New York Botanical Garden’s Virtual Herbarium. (continuously updated). Available online: http://sweetgum.nybg.org/ih/ (accessed on 4 October 2022).
- Tardìo, J.; Pardo-De-Santayana, M. Cultural importance indices: A comparative analysis based on the useful wild plants of Southern Cantabria (Northern Spain). Econ. Bot. 2008, 62, 24–39. [Google Scholar] [CrossRef]
- Friedman, J.; Yaniv, Z.; Dafni, A.; Palewitch, D. A preliminary classification of the healing potential of medicinal plants, based on a rational analysis of an ethnopharmacological field survey among Bedouins in the Negev Desert, Israel. J. Ethnopharmacol. 1986, 16, 275–287. [Google Scholar] [CrossRef]
- Brahmi, F.; Iblhoulen, Y.; Issaadi, H.; Elsebai, M.F.; Madani, K.; Boulekbache-Makhlouf, L. Ethnobotanical survey of medicinal plants of bejaia localities from algeria to prevent and treat coronavirus (COVID-19) infection shortened title: Phytomedicine to manage COVID-19 pandemic. Adv. Tradit. Med. 2022, 1–13. [Google Scholar] [CrossRef]
- Chukwuma, D.M.; Chukwuma, E.C.; Adekola, O.O. An ethnobotanical survey of Malaria-treating plants in Ado-Ekiti Local Government Area, Ekiti State, Nigeria. Ethnobot. Res. Appl. 2019, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Tavilla, G.; Crisafulli, A.; Ranno, V.; Picone, R.M.; Redouan, F.Z.; del Galdo, G.G. First contribution to the ethnobotanical knowledge in the Peloritani Mounts (NE Sicily). Res. J. Ecol. Environ. Sci. 2022, 4, 1–34. [Google Scholar] [CrossRef]
- Olatokun, W.M.; Ayanbode, O.F. Use of indigenous knowledge by women in a Nigerian rural community. Indian J. Tradit. Knowl. 2009, 8, 287–295. [Google Scholar]
- Benkhaira, N.; Koraichi, S.I.; Fikri-Benbrahim, K. Ethnobotanical survey on plants used by traditional healers to fight against COVID-19 in Fez city, Northern Morocco. Ethnobot. Res. Appl. 2021, 21, 1–18. [Google Scholar] [CrossRef]
- Singh, B.; Singh, B.; Kishor, A.; Singh, S.; Bhat, M.N.; Surmal, O.; Musarella, C.M. Exploring plant-based ethnomedicine and quantitative ethnopharmacology: Medicinal plants utilized by the population of Jasrota Hill in Western Himalaya. Sustainability 2020, 12, 7526. [Google Scholar] [CrossRef]
- Bhat, M.N.; Singh, B.; Surmal, O.; Singh, B.; Shivgotra, V.; Musarella, C.M. Ethnobotany of the Himalayas: Safeguarding medical practices and traditional uses of Kashmir regions. Biology 2021, 10, 851. [Google Scholar] [CrossRef] [PubMed]
- Lawal, I.O.; Rafiu, B.O.; Ale, J.E.; Majebi, O.E.; Aremu, A.O. Ethnobotanical survey of local flora used for medicinal purposes among indigenous people in five areas in Lagos State, Nigeria. Plants 2022, 11, 633. [Google Scholar] [CrossRef] [PubMed]
- Lawal, I.O.; Olufade, I.I.; Rafiu, B.O.; Aremu, A.O. Ethnobotanical survey of plants used for treating cough associated with respiratory conditions in Ede South local government area of Osun State, Nigeria. Plants 2020, 9, 647. [Google Scholar] [CrossRef] [PubMed]
- Zakariya, A.M.; Adamu, A.; Nuhu, A.; Kiri, I.Z. Assessment of indigenous knowledge on medicinal plants used in the management of malaria in Kafin Hausa, north-western Nigeria. Ethnobot. Res. Appl. 2021, 22, 1–18. [Google Scholar] [CrossRef]
- Ahmad, M.; Sultana, S.; Fazl-i-Hadi, S.; Ben Hadda, T.; Rashid, S.; Zafar, M.; Yaseen, G. An ethnobotanical study of medicinal plants in high mountainous region of Chail valley (District Swat-Pakistan). J. Ethnobiol. Ethnomed. 2014, 10, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tugume, P.; Kakudidi, E.K.; Buyinza, M. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve, Uganda. J. Ethnobiol. Ethnomed. 2016, 12, 5. [Google Scholar] [CrossRef] [Green Version]
- Suroowan, S.; Mahomoodally, M.F. A comparative ethnopharmacological analysis of traditional medicine used against respiratory tract diseases in Mauritius. J. Ethnopharmacol. 2016, 177, 61–80. [Google Scholar] [CrossRef]
- Ishtiaq, M.; Maqbool, M.; Ajaib, M.; Ahmed, M.; Hussain, I.; Khanam, H.; Mushtaq, W.; Hussain, T.; Azam, S.; Hayat, B.K.; et al. Ethnomedicinal and folklore inventory of wild plants used by rural communities of valley Samahni, District Bhimber Azad Jammu and Kashmir, Pakistan. PLoS ONE 2021, 16, e0243151. [Google Scholar] [CrossRef]
- Nagalingam, A. Drug Delivery Aspects of Herbal Medicines. Jpn Kampo Med. Treat Common Dis. Focus Inflamm. 2017, 17, 143. [Google Scholar]
- Hoffman, B.; Gallaher, T. Importance indices in ethnobotany. Ethnobot. Res. Appl. 2007, 5, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Weckerle, C.S.; De Boer, H.J.; Puri, R.K.; Van, A.T.; Bussmann, R.W.; Leonti, M. Recommended standards for conducting and reporting ethnopharmacological field studies. J. Ethnopharmacol. 2018, 210, 125–132. [Google Scholar] [CrossRef]
- Leonti, M. The relevance of quantitative ethnobotanical indices for ethnopharmacology and ethnobotany. J. Ethnopharmacol. 2022, 288, 115008. [Google Scholar] [CrossRef]
- Rajagopal, K.; Byran, G.; Jupudi, S.; Vadivelan, R. Activity of phytochemical constituents of black pepper, ginger, and garlic against coronavirus (COVID-19): An in silico approach. Int. J. Health Allied Sci. 2020, 9, 43–50. [Google Scholar] [CrossRef]
- Supriyanto, S.; Widjanarko, S.; Rifa’i, M.; Yunianta, Y. Immunomodulatory activity of methanol leaf extract of neem (Azadirachta Indica Juss.) against suppressor and proinflammatory molecules. J. Trop. Life Sci. 2021, 11, 309–316. [Google Scholar] [CrossRef]
- Gonzalez-Paz, L.; Lossada, C.; Moncayo, L.; Romero, F.; Paz, J.; Vera-Villalobos, J.; Pérez, A.; San-Blas, E.; Alvarado, Y. Theoretical molecular docking study of the structural disruption of the viral 3CL-protease of COVID19 induced by binding of capsaicin, piperine and curcumin part 1: A comparative study with chloroquine and hydrochloroquine two antimalaric drugs. Res. Sq. 2020. [Google Scholar] [CrossRef] [Green Version]
- Khan, J.; Sakib, S.; Mahmud, S.; Khan, Z.; Islam, M.; Sakib, M.; Simal-Gandara, J. Identification of potential phytochemicals from Citrus limon against main protease of SARS-CoV-2: Molecular docking, molecular dynamic simulations and quantum computations. J. Biomol. Struct. Dyn. 2021, 1–12. [Google Scholar] [CrossRef]
- Josling, P. Preventing the common cold with a garlic supplement: A double-blind, placebo-controlled survey. Adv Ther. 2001, 18(4), 189–193. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Yan, Y.X.; Yu, Q.T.; Deng, Y.; Wu, D.T.; Wang, Y.J. Comparison of immunomodulatory effects of fresh garlic and black garlic polysaccharides on RAW 264.7 macrophages. J. Food Sci. 2017, 82, 765–771. [Google Scholar] [CrossRef]
- Rouf, R.; Uddin, S.J.; Sarker, D.K.; Islam, M.T.; Ali, E.S.; Shilpi, J.A.; Sarker, S.D. Antiviral potential of garlic (Allium sativum) and its organosulfur compounds: A systematic update of pre-clinical and clinical data. Trends Food Sci. Technol. 2020, 104, 219–234. [Google Scholar] [CrossRef]
- Ashfaq, U.A.; Jalil, A.; Qamar, M.T. Antiviral phytochemicals identification from Azadirachta indica leaves against HCV NS3 protease: An in silico approach. Nat. Prod. Res. 2016, 30, 1866–1869. [Google Scholar] [CrossRef]
- Olwenyi, O.A.; Asingura, B.; Naluyima, P. In-vitro Immunomodulatory activity of Azadirachta indica A.Juss. Ethanol: Water mixture against HIV associated chronic CD4+ T-cell activation/exhaustion. BMC Complement Med. 2021, 21, 114. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, R.; Majeed, S.; Saghir, S.; Saad, M.; Ashraf, H.; Fayyaz, I. Antiviral activity of extract of neem (Azadirachta Indica) leaves: An in vivo study. Pak. J. Med. Health Sci. 2022, 16, 10. [Google Scholar] [CrossRef]
- Viveros-Paredes, J.M.; Puebla-Pérez, A.M.; Gutiérrez-Coronado, O.; Macías-Lamas, A.M.; Hernández-Flores, G.; Ortiz-Lazareno, P.C.; Villaseñor-García, M.M. Capsaicin attenuates immunosuppression induced by chronic stress in BALB/C mice. Int. Immunopharmacol. 2021, 93, 107341. [Google Scholar] [CrossRef]
- Nudo, L.P.; Catap, E.S. Anti-immunosuppressive effects of Chromolaena odorata (Lf.) King & Robinson (Asteraceae) leaf extract in cyclophosphamide-injected Balb/C mice. Philipp. J. Sci. 2012, 141, 35–43. [Google Scholar]
- Boudjeko, T.; Megnekou, R.; Woguia, A.L.; Kegne, F.M.; Ngomoyogoli, J.E.K.; Tchapoum, C.D.N.; Koum, O. Antioxidant and immunomodulatory properties of polysaccharides from Allanblackia floribunda Oliv stem bark and Chromolaena odorata (L.) King and HE Robins leaves. BMC Res. Notes 2015, 8, 759. [Google Scholar] [CrossRef] [Green Version]
- Lappas, C.M.; Lappas, N.T. D-Limonene modulates T lymphocyte activity and viability. Cell. Immunol. 2012, 279, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Nagy, M.M.; Al-Mahdy, D.A.; Abd El Aziz, O.M.; Kandil, A.M.; Tantawy, M.A.; El Alfy, T.S. Chemical composition and antiviral activity of essential oils from Citrus reshni hort. ex Tanaka (Cleopatra mandarin) cultivated in Egypt. J. Essent. Oil Bear. Plants 2018, 21, 264–272. [Google Scholar] [CrossRef]
- Meeran, M.N.; Seenipandi, A.; Javed, H.; Sharma, C.; Hashiesh, H.M.; Goyal, S.N.; Ojha, S. Can limonene be a possible candidate for evaluation as an agent or adjuvant against infection, immunity, and inflammation in COVID-19? Heliyon 2021, 7, e05703. [Google Scholar] [CrossRef]
- Diab, K.A. In vitro studies on phytochemical content, antioxidant, anticancer, immunomodulatory, and antigenotoxic activities of lemon, grapefruit, and mandarin citrus peels. Asian Pac. J. Cancer Prev. 2016, 17, 3559–3567. [Google Scholar]
- Abd, A.J.; Al-Shammarie, A.M.; Abd, A.H. Antiviral activity of limonin against Newcastle disease virus in vitro. Res. J. Biotechnol. 2019, 14, 320–328. [Google Scholar]
- Afolayan, F.I.; Erinwusi, B.; Oyeyemi, O.T. Immunomodulatory activity of curcumin-entrapped poly d, l-lactic-co-glycolic acid nanoparticles in mice. Integr. Med. Res. 2018, 7, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Gu, L.; Su, Y.; Wang, Q.; Zhao, Y.; Chen, X.; Li, K. Inhibition of curcumin on influenza A virus infection and influenzal pneumonia via oxidative stress, TLR2/4, p38/JNK MAPK and NF-κB pathways. Int. Immunopharmacol. 2018, 54, 177–187. [Google Scholar] [CrossRef]
- Duran, N.; Kaya, D.A. Chemical composition of essential oils from Origanum onites L. and Cymbopogon citratus, and their synergistic effects with acyclovir against HSV-1. In Proceedings of the 7th International Conference on Advanced Materials and Systems 2018, Bucharest, Romania, 18–20 October 2018; The National Research & Development Institute for Textiles and Leather: București, Romania, 2018; pp. 243–248. [Google Scholar]
- Goncalves, E.C.; Assis, P.M.; Junqueira, L.A.; Cola, M.; Santos, A.R.; Raposo, N.R.; Dutra, R.C. Citral inhibits the inflammatory response and hyperalgesia in mice: The role of TLR4, TLR2/Dectin-1, and CB2 cannabinoid receptor/ATP-sensitive K+ channel pathways. J. Nat. Prod. 2020, 83, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Rosmalena, R.; Elya, B.; Dewi, B.E.; Fithriyah, F.; Desti, H.; Angelina, M.; Seto, D. The antiviral effect of indonesian medicinal plant extracts against dengue virus in vitro and in silico. Pathogens 2019, 8, 85. [Google Scholar] [CrossRef] [Green Version]
- Nworu, C.S.; Akah, P.A.; Esimone, C.O.; Okoli, C.O.; Okoye, F.B.C. Immunomodulatory activities of kolaviron, a mixture of three related biflavonoids of Garcinia kola Heckel. Immunopharmacol. Immunotoxicol. 2008, 30, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Awogbindin, I.O.; Olaleye, D.O.; Farombi, E.O. Kolaviron improves morbidity and suppresses mortality by mitigating oxido-inflammation in BALB/c mice infected with influenza virus. Viral Immunol. 2015, 28, 367–377. [Google Scholar] [CrossRef]
- Farombi, E.O.; Awogbindin, I.O.; Farombi, T.H.; Ikeji, C.N.; Adebisi, A.; Adedara, I.A.; Aruoma, O.I. Possible role of Kolaviron, a Garcinia kola bioflavonoid in inflammation associated COVID-19 infection. Am. J. Biopharmacy Pharm. Sci. 2022, 2, 1–13. [Google Scholar] [CrossRef]
- Kudi, A.C.; Myint, S.H. Antiviral activity of some Nigerian medicinal plant extracts. J. Eethnopharmacol. 1999, 68, 289–294. [Google Scholar] [CrossRef]
- Foyet, H.S.; Tsala, D.E.; Zogo, E.B.; Carine, A.N.; Heroyne, L.T.; Oben, E.K. Anti-inflammatory and anti-arthritic activity of a methanol extract from Vitellaria paradoxa stem bark. Pharmacogn. Res. 2014, 7, 367–377. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Moneim, A.; Morsy, B.M.; Mahmoud, A.M.; Abo-Seif, M.A.; Zanaty, M.I. Beneficial therapeutic effects of Nigella sativa and/or Zingiber officinale in HCV patients in Egypt. EXCLI J. 2013, 11, 43–55. [Google Scholar]
- Li, C.; Dong, Z.; Zhang, B.; Huang, Q.; Liu, G.; Fu, X. Structural characterization and immune enhancement activity of a novel polysaccharide from Moringa oleifera leaves. Carbohydr. Polym. 2020, 234, 115897. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wei, S.; Lu, X.; Qiao, X.; Simal-Gandara, J.; Capanoglu, E.; Li, N. A neutral polysaccharide with a triple helix structure from ginger: Characterization and immunomodulatory activity. Food Chem. 2021, 350, 129261. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Group | Number | Percentage (%) |
|---|---|---|---|
| Gender | Male | 23 | 41.1 |
| Female | 33 | 58.9 | |
| Age (Years) | 20–30 | 4 | 7.14 |
| 31–40 | 7 | 12.5 | |
| 41–50 | 14 | 25 | |
| 51 and above | 31 | 55.4 | |
| Local Government Area | Ogbomosho South | 41 | 73.21 |
| Ogbomosho North | 16 | 26.79 | |
| Educational Level | Primary | 26 | 46.43 |
| Secondary | 19 | 33.93 | |
| Tertiary | 11 | 19.64 | |
| Occupation | Herb seller | 27 | 48.2 |
| Traditional health practitioner | 6 | 10.7 | |
| Farmer | 1 | 1.8 | |
| Other | 22 | 39.3 |
| S/N | Scientific Name and Voucher Specimen Number | Common Name | Local Name | Family | Mode of Preparation | Growth Form | Mode of Administration | Plant Part | Plant Source | Material | FC | RFC | FL (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Allium sativum L. IFE18082 | Garlic | Ayu | Amaryllidaceae | Frying | Herb | Nasal | Bulbs | C | F | 3 | 0.05 | 5 |
| 2 | Alstonia boonei De Wild. IFE18083 | Stool weed | Doctor igbo | Apocynaceae | Decoction | Tree | Oral | Leaves | C | F | 1 | 0.02 | 2 |
| 3 | Azadirachta indica A. Juss. IFE18086 | Neem | Dongoyaro | Meliaceae | Decoction | Tree | Oral | Leaves, bark | WP | F | 8 | 0.14 | 14 |
| 4 | Capsicum frutescens L. IFE18088 | Pepper | Ata wewe | Solanaceae | Decoction | Herb | Oral | Fruit | C | F | 6 | 0.11 | 11 |
| 5 | Cinnamomum camphora (L.) J. Presl IFE18091 | Camphor | Kafura | Lauraceae | Heating | Tree | Nasal | Bark | WP | F | 1 | 0.02 | 2 |
| 6 | Citrus limon (L.) Osbeck IFE18093 | Lime | Oronbo | Rutaceae | Juice extraction | Tree | Oral | Fruit | C | F | 5 | 0.014 | 9 |
| 7 | Clausena anisata (Willd.) Hook.f. ex Benth. IFE18094 | Horsewood | Agbasa | Rutaceae | Decoction | Tree | Oral | Leaves | WP | F | 1 | 0.02 | 2 |
| 8 | Curcuma longa L. IFE18134 | Turmeric | Ata ile pupa | Zingiberaceae | Decoction | Herb | Oral | Rhizomes | C | D | 8 | 0.14 | 14 |
| 9 | Cymbopogon citratus (DC.) Stapf IFE18097 | Lemon Grass | Ewe tea | Poaceae | Decoction | Grass | Oral | Leaves | C | F | 1 | 0.02 | 2 |
| 10 | Drypetes gossweileri S.Moore IFE18099 | Horse radish Tree | Epo aganwo | Putranjivaceae | Decoction | Tree | Oral | Bark | WP | D | 1 | 0.02 | 2 |
| 11 | Gymnanthemum amygdalinum (Delile) Sch.Bip. IFE18127 | Bitter leaf | Ewuro | Asteraceae | Decoction | Shrub | Oral | Leaves | C | F | 2 | 0.04 | 4 |
| 12 | Momordica charantia L. IFE18108 | Bitter lemon | Ejinrin | Cucurbitaceae | Decoction | Climber | Oral | Leaves | C | F | 1 | 0.02 | 2 |
| 13 | Morinda lucida Benth. IFE18109 | Brimstone Tree | Oruwo | Rubiaceae | Decoction | Tree | Oral | Leaves, bark | WP | D | 3 | 0.05 | 5 |
| 14 | Neonauclea excelsa (Blume) Merr. IFE18111 | Nauclea | Egbeesi | Rubiaceae | Decoction | Tree | Oral | Bark | WP | F | 1 | 0.02 | 2 |
| 15 | Nigella sativa L. IFE18113 | Black seed | Asofeyeje | Ranunculaceae | Decoction | Herb | Oral | Seeds | WP | D | 1 | 0.02 | 2 |
| 16 | Peperomia pellucida (L.) Kunth IFE18115 | Shiny bush | Ewe rinrin | Piperaceae | Pulverizing | Herb | Oral | Leaves | C | D | 1 | 0.02 | 2 |
| 17 | Pseudocedrela kotschyi Harms IFE18117 | Dry zone cedar | Emigbegi | Meliaceae | Decoction | Tree | Oral | Leaves | WP | F | 1 | 0.02 | 2 |
| 18 | Senna alata (L.) Roxb. IFE18121 | Candle bush | Asunwon oyinbo | Fabaceae | Decoction | Tree | Oral | Leaves | WP | F | 2 | 0.04 | 4 |
| 19 | Tetrapleura tetraptera (Schum. and Thonn.) Taub. IFE18123 | Aidan Tree | Aridan | Fabaceae | Decoction | Tree | Oral | Fruit | C | F | 3 | 0.05 | 5 |
| 20 | Tithonia diversifolia (Hemsl.) A.Gray IFE18124 | Tree marigold | Sepeleba | Asteraceae | Decoction | Herb | Oral | Leaves | WP | F | 1 | 0.02 | 2 |
| 21 | Uvaria afzelii Scott. Elliot IFE18125 | Monkey finger | Gbogbonise | Annonaceae | Decoction | Tree | Oral | Bark | WP | D | 1 | 0.02 | 2 |
| 22 | Uvaria chamae P. Beauv. IFE18126 | Finger root | Eruiju | Annonaceae | Decoction | Herb | Oral | Bark | C | F | 1 | 0.02 | 2 |
| 23 | Vitellaria paradoxa C.F Gaertn IFE18128 | Shea butter | Ori | Sapotaceae | Heating | Tree | Nasal | Seeds | WP | D | 6 | 0.11 | 11 |
| 24 | Xylopia villosa Chipp IFE18130 | Black palufon | Eeru awonka | Annonaceae | Decoction | Tree | Oral | Leaves | WP | F | 1 | 0.02 | 2 |
| 25 | Zea mays L. IFE18131 | Maize | Agbado | Poaceae | Decoction | Grass | Oral | Seeds | C | F | 1 | 0.02 | 2 |
| 26 | Zingiber officinale Roscoe IFE18132 | Ginger | Ata ile | Zingiberaceae | Decoction | Herb | Oral | Rhizomes | C | F | 10 | 0.18 | 18 |
| S/N | Scientific Name and Voucher Specimen Number | Common Name | Local Name | Family | Mode of Preparation | Growth Form | Mode of Administration | Plant Part | Plant Source | Material | FC | RFC | FL (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Abrus precatorius L. IFE18077 | Rosary pea | Omisinmisin | Fabaceae | Decoction | Climber | Oral | Leaves | WP | F | 7 | 0.13 | 13 |
| 2 | Aframomum melegueta K. Schum. IFE18079 | Alligator pepper | Ataare | Zingiberaceae | Pulverizing | Herb | Oral | Seeds, fruit | C | D | 5 | 0.09 | 9 |
| 3 | Allium ascalonicum L. IFE18080 | Spring onion | Alubosa elewe | Amaryllidaceae | Grating, Infusion | Herb | Oral | Bulbs | C | F | 1 | 0.02 | 2 |
| 4 | Allium cepa L. IFE18081 | Onion | Alubosa | Amaryllidaceae | Pulverizing | Shrub | Oral | Bulbs | C | F | 3 | 0.05 | 5 |
| 5 | Allium sativum L. IFE18082 | Garlic | Ayu | Amaryllidaceae | Frying | Herb | Nasal | Bulbs | C | F | 12 | 0.21 | 21 |
| 6 | Amaranthus spinosus L. IFE18084 | Spinach | Igi teteregun | Amaranthaceae | Decoction | Herb | Oral | Bark | C | F | 2 | 0.04 | 4 |
| 7 | Capsicum frutescens L. IFE18088 | Hot pepper | Ata wewe | Solanaceae | Pulverizing, Infusion | Herb | Oral | Seeds | C | D | 2 | 0.04 | 4 |
| 8 | Citrus aurantiifolia (Christm.) Swingle IFE18092 | Lemon | Osan wewe | Rutaceae | Juice extraction | Tree | Oral | Fruit | C | F | 11 | 0.2 | 20 |
| 9 | Citrus limon (L.) Osbeck IFE18093 | Lime | Orombo | Rutaceae | Juice extraction | Tree | Oral | Fruit | C | F | 13 | 0.23 | 23 |
| 10 | Cocos nucifera L. IFE18095 | Coconut | Agbon | Arecaceae | Decoction | Tree | Oral | Pod | C | F | 2 | 0.04 | 4 |
| 11 | Crinum jagus (J.Thomps.) Dandy IFE18096 | Poison bulb | Ogede odo | Amaryllidaceae | Pulverizing, grating, Infusion | Herb | Oral | Bulbs | WP | F | 2 | 0.04 | 4 |
| 12 | Cymbopogon citratus Stapf IFE18097 | Lemon Grass | Ewe tea | Poaceae | Decoction | Grass | Oral | Leaves | C | F | 2 | 0.04 | 4 |
| 13 | Elaeis guineensis Jacq. IFE18100 | Palm Tree | Ope | Arecaceae | Infusion | Tree | Oral | Seeds | C | F | 2 | 0.04 | 4 |
| 14 | Eucalyptus globulus Labill IFE18101 | Bluegum Eucalyptus | Eucalyptus | Myrtaceae | Decoction | Tree | Oral | Leaves | WP | F | 2 | 0.04 | 4 |
| 15 | Ficus asperifolia Hook. ex Miq. IFE18103 | Sandpaper | Ewe ipin | Moraceae | Infusion | Tree | Oral | Leaves | WP | D | 2 | 0.04 | 4 |
| 16 | Garcinia kola Heckel IFE18105 | Bitter cola | Orogbo | Clusiaceae | Infusion, pulverizing | Tree | Oral | Seeds | C | F | 8 | 0.14 | 14 |
| 17 | Gymnanthemum amygdalinum (Delile) Sch.Bip. IFE18127 | Bitter leaf | Ewuro | Asteraceae | Pulverizing, Infusion | Shrub | Oral | Flower | C | F | 4 | 0.07 | 7 |
| 18 | Jatropha curcas L. IFE18106 | Jatropha | Lapalapa | Euphorbiaceae | Decoction | Shrub | Oral | Fruit | WP | F | 4 | 0.07 | 7 |
| 19 | Mangifera indica L. IFE18107 | Mango | Mangoro | Anacardiaceae | Decoction | Tree | Oral | Bark | C | F | 2 | 0.04 | 4 |
| 20 | Marsdenia latifolia (Benth.) K.Schum. IFE18104 | Bush buck | Arokeke, Madunmaro | Apocynaceae | Maceration, infusion | Shrub | Oral | Leaves, bark | WP | F | 1 | 0.02 | 2 |
| 21 | Neonauclea excelsa (Blume) Merr. IFE18111 | Nauclea | Egbeesi | Rubiaceae | Infusion | Tree | Oral | Root | WP | F | 5 | 0.09 | 9 |
| 22 | Olax subscorpioidea Oliv. IFE18114 | Ivory coast | Ifon | Olacaceae | Pulverizing | Tree | Oral | Bark | WP | D | 2 | 0.04 | 4 |
| 23 | Psidium guajava L. IFE18118 | Guava | Groofa | Myrtaceae | Decoction | Tree | Oral | Bark, Leaves | C | F | 3 | 0.05 | 5 |
| 24 | Saccharum officinarum L. IFE18119 | Sugarcane | Ireke | Poaceae | Pounding, Infusion | Grass | Oral | Stem | C | F | 1 | 0.02 | 2 |
| 25 | Securidaca longipedunculata Fresen. IFE18120 | Violet Tree | Ipeta | Polygalaceae | Pulverizing | Tree | Oral | Bark | WP | D | 3 | 0.05 | 5 |
| 26 | Spondias mombin L. IFE18122 | Hog plum | Iyeye | Anacardiaceae | Decoction | Tree | Oral | Bark | WP | F | 5 | 0.09 | 9 |
| 27 | Tetrapleura tetraptera (Schum. and Thonn.) Taub. IFE18123 | Aidan Tree | Aridan/ Aidan | Fabaceae | Pulverizing, grating, Infusion | Tree | Oral | Fruit | C | F | 1 | 0.02 | 2 |
| 28 | Vitellaria paradoxa C.F Gaertn IFE18128 | Shea butter | Ori | Sapotaceae | Frying | Tree | Nasal | Seeds | WP | D | 11 | 0.2 | 20 |
| 29 | Xylopia aethiopica A. Rich IFE18129 | African pepper | Eeru | Annonaceae | Pulverizing, Infusion | Tree | Oral | Seeds | WP | D | 6 | 0.11 | 11 |
| 30 | Zea mays L. IFE18131 | Maize | Agbado | Poaceae | Decoction | Grass | Oral | Husk | C | F | 2 | 0.04 | 4 |
| 31 | Zingiber officinale Roscoe IFE18132 | Ginger | Ata ile | Zingiberaceae | Decoction, pulverizing | Herb | Oral | Rhizomes, root | C | F | 3 | 0.05 | 5 |
| S/N | Scientific Name and Voucher Specimen Number | Common Name | Local Name | Family | Mode of Preparation | Growth Form | Mode of Administration | Plant Part | Plant Source | Material | FC | RFC | FL (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Aframomum melegueta K. Schum. IFE18079 | Alligator pepper | Ataare | Zingiberaceae | Decoction | Herb | Oral | Seeds | C | D | 2 | 0.04 | 4 |
| 2 | Allium ascalonicum L. IFE18080 | Spring onion | Alubosa elewe | Amaryllidaceae | Juice extraction | Herb | Oral | Bulbs | C | F | 2 | 0.04 | 4 |
| 3 | Allium cepa L. IFE18081 | White onion | Alubosa funfun | Amaryllidaceae | Infusion | Shrub | Oral | Bulbs | C | F | 2 | 0.04 | 4 |
| 4 | Allium sativum L. IFE18082 | Garlic | Ayu | Amaryllidaceae | Chewing, frying | Herb | Oral, nasal | Bulbs | C | F | 6 | 0.11 | 11 |
| 5 | Annona senegalensis Pers. IFE18085 | Wild soursop | Ewe abo | Annonaceae | Decoction | Shrub | Oral | Leaves | WP | F | 2 | 0.04 | 4 |
| 6 | Azadirachta indica A. Juss IFE18086 | Neem | Dongoyaro | Meliaceae | Decoction, infusion | Tree | Oral | Leaves, bark | WP | F | 6 | 0.11 | 11 |
| 7 | Capsicum annuum L. IFE18087 | Hot pepper | Ata ijoosi | Solanaceae | Pulverizing | Herb | Oral | Seeds | C | D | 2 | 0.04 | 4 |
| 8 | Carica papaya L. IFE18089 | Pawpaw | Eso ibepe | Caricaceae | Decoction | Tree | Oral | Seeds | C | F | 3 | 0.05 | 5 |
| 9 | Chromolaena odorata (L.) R.M.King and H.Rob. IFE18090 | Siam weed | Ewe akintola | Asteraceae | Pulverizing, infusion | Shrub | Oral | Leaves | C | F,D | 6 | 0.11 | 11 |
| 10 | Cinnamomum camphora (L.) J.Presl IFE18091 | Camphor | Kafura | Lauraceae | Frying | Tree | Topical | Bark | WP | F | 1 | 0.02 | 2 |
| 11 | Citrus limon (L.) Osbeck IFE18093 | Lime | Oronbo | Rutaceae | Juice extraction | Tree | Topical | Fruit | C | F | 3 | 0.05 | 5 |
| 12 | Crinum jagus (J.Thomps.) Dandy IFE18096 | Poison bulb | Ogede odo | Amaryllidaceae | Pounding | Herb | Oral | Bulbs | WP | F | 2 | 0.04 | 4 |
| 13 | Cymbopogon citratus (DC.) Stapf IFE18097 | Lemon Grass | Ewe tea | Poaceae | Decoction, infusion | Grass | Oral | Leaves | C | F | 7 | 0.13 | 13 |
| 14 | Eucalyptus globulus LabillIFE18101 | Bluegum Eucalyptus | Eucalyptus | Myrtaceae | Juice extraction | Tree | Oral | Leaves | WP | F | 1 | 0.02 | 2 |
| 15 | Garcinia kola Heckel IFE18105 | Bitter cola | Orogbo | Clusiaceae | Pulverizing | Tree | Oral | Seeds | C | F | 5 | 0.09 | 9 |
| 16 | Gymnanthemum amygdalinum (Delile) Sch.Bip IFE18127 | Bitter leaf | Ewuro | Asteraceae | Pulverizing, infusion | Shrub | Oral | Leaves | C | F | 4 | 0.07 | 7 |
| 17 | Kigelia africana (Lam.) Benth. IFE18133 | Sausage Tree | Pandoro | Bignoniaceae | Pulverizing, infusion | Tree | Oral | Bark | WP | D | 2 | 0.04 | 4 |
| 18 | Mangifera indica L. IFE18107 | Mango | Mango | Anacardiaceae | Infusion | Tree | Oral | Leaves | C | F | 2 | 0.04 | 4 |
| 19 | Morinda lucida Benth. IFE18109 | Brimstone Tree | Oruwo | Rubiaceae | Pulverizing, infusion | Tree | Oral | Bark | WP | D | 2 | 0.04 | 4 |
| 20 | Musa × paradisiaca L. IFE18110 | Banana | Ogede | Musaceae | Juice extraction | Herb | Oral | Leaves | C | F | 1 | 0.02 | 2 |
| 21 | Nicotiana tabacum L. IFE18112 | Tobacco | Taba | Solanaceae | Infusion | Herb | Oral | Leaves | C | F | 1 | 0.02 | 2 |
| 22 | Piper nigrum L. IFE18116 | Black pepper | Iyere | Piperaceae | Decoction | Climber | Oral | Seeds | C | D | 1 | 0.02 | 2 |
| 23 | Syzygium aromaticum (L.) Merr. and L.M. Perry IFE18102 | Cloves | kannafuru | Myrtaceae | Infusion, pulverizing | Tree | Oral | Seeds | C | D, F | 1 | 0.02 | 2 |
| 24 | Tetrapleura tetraptera (Schum. and Thonn.) Taub. IFE18123 | Aidan Tree | Aridan | Fabaceae | Decoction, infusion, pulverizing | Tree | Oral | Fruit | C | D, F | 1 | 0.02 | 2 |
| 25 | Uvariopsis tripetala (Baker f.) G.E.Schatz IFE18098 | Pepper fruit | Ata dudu, ata igbere | Annonaceae | Decoction | Tree | Oral | Seeds | WP | D | 1 | 0.02 | 2 |
| 26 | Vachellia nilotica (L.) P.J.H.Hurter and Mabb. IFE18078 | Gum Arabic Tree | Booni | Fabaceae | Pulverizing, infusion | Tree | Oral | Seeds | WP | D, F | 1 | 0.02 | 2 |
| 27 | Vitellaria paradoxa C.F.Gaertn IFE18128 | Shea butter | Ori | Sapotaceae | Frying | Tree | Topical | Seeds | WP | D | 1 | 0.02 | 2 |
| 28 | Xylopia aethiopica A. Rich. IFE18129 | African pepper | Eeru | Annonaceae | Pulverizing, infusion, decoction | Tree | Oral | Seeds | WP | D | 2 | 0.04 | 4 |
| 29 | Zingiber officinale Roscoe IFE18132 | Ginger | Ata ile | Zingiberaceae | Pulverizing, infusion | Herb | Oral | Root | C | F | 9 | 0.16 | 16 |
| Species | Antiviral Activities | Immunomodulatory Activities | Active Compounds | Mechanism of Action | References |
|---|---|---|---|---|---|
| Allium sativum L. | Clinical study revealed that allicin–garlic capsule prevented common cold in active treatment group than the placebo group. | In vitro study showed that polysaccharides isolated from fresh garlic promoted immune functions of RAW 264.7 macrophages | Allicin | Antiviral effects of allicin by enhancing immune response. Immunomodulatory effect by promotion of phagocytosis, release of NO, and expressions of several immune-related cytokines. | [54,55,56] |
| Azadirachta indica A.Juss. | In vivo study showed that aqueous A. indica leaf extract significantly decreased HCV seropositivity and inhibited the replication of HCV. | In vitro study showed that ethanol extract of A. indica downregulated the levels of CD4 + T cell activation, and inhibited SEB induced CD4+ T-cell activation/exhaustion | Azadirachtin 3-Deacetyl-3-azadirachtin | Antiviral effects by binding to NS3 protease of HCV. | [57,58,59] |
| Capsicum frutescens L. | Molecular dynamics and strategies docking study showed that capsaicin caused structural disruption of viral 3CL-protease of COVID-19. | Capsaicin attenuated chronic stress-induced immunosuppression in BALB/c mice. | Capsaicin | Antiviral effect by binding to 3CL-protease of COVID-19. Immunomodulatory activity through increased production of Th1 cytokines and decreased production of Th2 cytokines and TGF-β1. | [53,60] |
| Chromolaena odorata (L.) R.M.King and H.Rob. | NR | Ethanolic extract of C. odorata showed immunopotentiating activities on the innate immunity of Balb/C mice, and reverse a drug-induced immunosuppression. In another report, soluble polysaccharides (PoS) fraction of C. odorata showed immunostimulatory activity. | Polysaccharides | Immunostimulatory activity of PoS fraction via stimulation of peripheral blood mononuclear cells, and production of IFN-γ. | [61,62] |
| Citrus aurantiifolia (Christm.) Swingle | Limonene showed moderate inhibition of the avian influenza A virus (H5N1). | Limonene showed immunoregulatory activity in lipopolysaccharides (LPS)-induced pleurisy model. | Limonene | Antiviral effects of limonene by the inhibition of viral replication via direct action on the virus. Immunomodulatory effects by the inhibition of NO and the cytokines IFN-γ and IL-4. | [63,64,65] |
| Citrus limon (L.) Osbeck | In vitro study showed that limonin reduced the replication of New-castle disease virus (NDV) in all cell lines. | Ethanolic extract of lemon peel increased proliferation of mouse splenocytes signifying immunostimulation activity | Limonin | Antiviral activity of limoin by downregulation of NDV- haemagglutinin-neuraminidase and matrix genes. Immunomodulatory effect by augmentation of proliferation of T-lymphocytes. | [66,67] |
| Curcuma longa L. | In vitro study showed that curcumin directly inactivated influenza A virus (IAV) blocked IAV adsorption, and inhibited IAV proliferation. | Poly D,L-lactic-co-glycolic acid entrapped curcumin nanoparticle significantly stimulated primary humoral immune response in mice. | Curcumin | Antiviral effects by Increasing Nrf2, HO-1, NQO1, GSTA3 and IFN-β production; suppression of IAV-induced activation of TLR2/4/7, Akt, p38/JNK MAPK and NF-κB pathways. | [68,69] |
| Cymbopogon citratus (DC.) Stapf | In vitro and in silico studies showed that the methanolic extract of C. citratus demonstrated anti-dengue activities. Additionally, E-Citral, Z-Citral, and β-Myrcene from the essential oil of C. citratus showed significant inhibitory effect on herpes simplex virus-1 (HSV-1) replication. | Oral citral administration showed marked immunomodulatory effects in lipopolysaccharides (LPS)- induced paw edema in mice. | Citral | Immunomodulatory effects by the inhibition of oxidative activity, activation of nuclear factor kappa B, peroxisome proliferator-activated receptor (PPAR)-α and γ. | [70,71,72] |
| Garcinia kola Heckel | Kolaviron, extracted from G. kola seeds impaired IAV-induced mortality and was effective in delaying the clinical symptoms of IAV in BALB/c mice. | In vivo and in vitro studies revealed that kolaviron demonstrated immunomodulatory and immunorestorative properties in immunocompetent and immunocompromised animal models. | Kolaviron | Antiviral effects by attenuating nitric oxide production and suppression of myeloperoxidase activity, immunomodulatory effect by inhibition of delayed-type hypersensitivity response and enhancement of leukocytes counts. | [73,74,75] |
| Vitellaria paradoxa C.F.Gaertn. | Ethanolic extract of V. paradoxa inhibited 50% of human polio virus (Type 1) and Astrovirus. | Methnolic extract of V. paradoxa displayed significant suppression of inflammation response in carrageenan-induced inflammation in Wistar albino rats. | Catechins | Inflammation suppression effects by the inhibition of the pro-inflammatory cytokines IL-1, IL-6, and TNF-α. | [76,77] |
| Zingiber officinale Roscoe | In a clinical study, ethanolic extract of Z. officinale showed significant decrease in the viral load of patients with hepatitis C virus (HCV). In a recent in silico docking study, 8-gingerol and 10-gingerol isolated from Z. officinale were active against COVID-19 with significantly higher Glide scores when compared to hydroxychloroquine. | Neutral ginger polysaccharide fraction (NGP) significantly showed immunomodulatory activity on RAW264.7 cells without cytotoxicity, | Gingerol Neutral ginger polysaccharide | Immunomodulatory effects by the promotion of TNF-α production by macrophage cells. | [78,79,80] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odebunmi, C.A.; Adetunji, T.L.; Adetunji, A.E.; Olatunde, A.; Oluwole, O.E.; Adewale, I.A.; Ejiwumi, A.O.; Iheme, C.E.; Aremu, T.O. Ethnobotanical Survey of Medicinal Plants Used in the Treatment of COVID-19 and Related Respiratory Infections in Ogbomosho South and North Local Government Areas, Oyo State, Nigeria. Plants 2022, 11, 2667. https://doi.org/10.3390/plants11192667
Odebunmi CA, Adetunji TL, Adetunji AE, Olatunde A, Oluwole OE, Adewale IA, Ejiwumi AO, Iheme CE, Aremu TO. Ethnobotanical Survey of Medicinal Plants Used in the Treatment of COVID-19 and Related Respiratory Infections in Ogbomosho South and North Local Government Areas, Oyo State, Nigeria. Plants. 2022; 11(19):2667. https://doi.org/10.3390/plants11192667
Chicago/Turabian StyleOdebunmi, Christiana Adeyinka, Tomi Lois Adetunji, Ademola Emmanuel Adetunji, Ahmed Olatunde, Oluwatosin Esther Oluwole, Idowu Ayodeji Adewale, Abdulrasak Opeyemi Ejiwumi, Chinwenwa Esther Iheme, and Taiwo Opeyemi Aremu. 2022. "Ethnobotanical Survey of Medicinal Plants Used in the Treatment of COVID-19 and Related Respiratory Infections in Ogbomosho South and North Local Government Areas, Oyo State, Nigeria" Plants 11, no. 19: 2667. https://doi.org/10.3390/plants11192667