1. Introduction
Stroke is one of the leading causes of death and disability in adults worldwide [
1]. At least 65% of stroke patients have hand impairment [
2]. It has been reported that hand dysfunction can be a major obstacle in daily life and labor [
3]. Therefore, it is important for patients to undergo hand rehabilitation in order to recover from stroke side effects [
4,
5]. Constant high-quality rehabilitation is necessary for effective hand rehabilitation during motor paralysis [
6]. Generally, rehabilitation is performed under the guidance and assistance of a therapist; thus, a facility where therapists work with the other specialists is usually the place for rehabilitation. However, the recent spread of infectious diseases and the shortage of visiting therapists have reduced the frequency of rehabilitation that can be provided to patients [
7]. Furthermore, most therapists are often located in urban centers, so patients living in underpopulated areas may be unable to participate in rehabilitation [
3].
Telerehabilitation is gaining attention as a new means to address such problems, improving access for patients living in remote areas and reducing the financial and time costs associated with outpatient rehabilitation [
8]. However, in a telerehabilitation environment, the therapist and patient are normally far away from each other, making it difficult for the therapist to palpate and understand the condition of the patient’s hand [
9].
Finger flexor spasticity, a motor disorder that causes involuntary muscle contractions due to impaired reflex function, is a common aftereffect of stroke [
10]. Spasticity not only increases the stiffness of the fingers but also decreases their range of motion, affecting the recovery of the patient’s motor function [
11]. Therefore, understanding a patient’s spasticity condition can help therapists determine optimal rehabilitation [
12]. However, spasticity is difficult to evaluate without direct contact with the therapist, as is the degree of muscle tone that fluctuates from day to day [
13]. Therefore, a method to objectively quantify spasticity by non-palpation is necessary in telerehabilitation. Up to now, dedicated stiffness measurement devices that have been developed are large and heavy because they consist of many rigid body parts [
14,
15,
16]. When rehabilitation is performed at a patient’s home, the available space is assumed to be limited, and it is desirable to minimize the number of devices by accomplishing simultaneous functions, such as the evaluation of spasticity condition and rehabilitation using the same device.
Heung et al. developed a system that combines the two functions of finger motor support and spasticity condition evaluation by using a soft elastic composite actuator (SECA), a hand rehabilitation device, to estimate finger joint stiffness [
17]. Soft actuators are suitable devices for hand rehabilitation in a telerehabilitation environment because of their flexibility, lightweight, high affinity with the body, and portability. In [
18], the stiffness estimation method using a SECA was found to agree with standard joint stiffness quantification methods. Furthermore, it was suggested that a SECA could be used to quantitatively assess the stiffness of the passive metacarpophalangeal (MCP) joint during the performance of various tasks in hand rehabilitation. The stiffness estimation method using a SECA estimates stiffness from an analytical model using the input air pressure of the soft actuator and a finger joint angle, which requires a structure-dependent soft actuator analytical model and a joint angle measurement. In addition, there are several technical problems with its application in telerehabilitation.
Firstly, a whole-finger soft actuator with a single-pocket structure with multiple air chambers connected to each other, such as the SECA, is not suitable for home environments because it requires high air pressure to achieve high bending performance [
17,
19,
20]. Secondly, this type of actuator has only one pneumatic input and cannot support individual joints. Thirdly, the dimensions of the actuator need to be changed to accommodate individual differences such as finger size, but this change may cause unintended changes in actuator motion [
21]. Finally, it is costly to customize the actuator for each patient. Yun et al. and Kokubu et al. developed joint modular soft actuators that are divided into parts corresponding to each finger joint [
20,
21]. By using spacers to connect each actuator, the actuators can accommodate differences in the length of the user’s fingers without changing the dimensions of the actuator. This enables personalized customization at a low cost. In addition, the actuator does not require high air pressure because it transmits force better than a whole-finger soft actuator does [
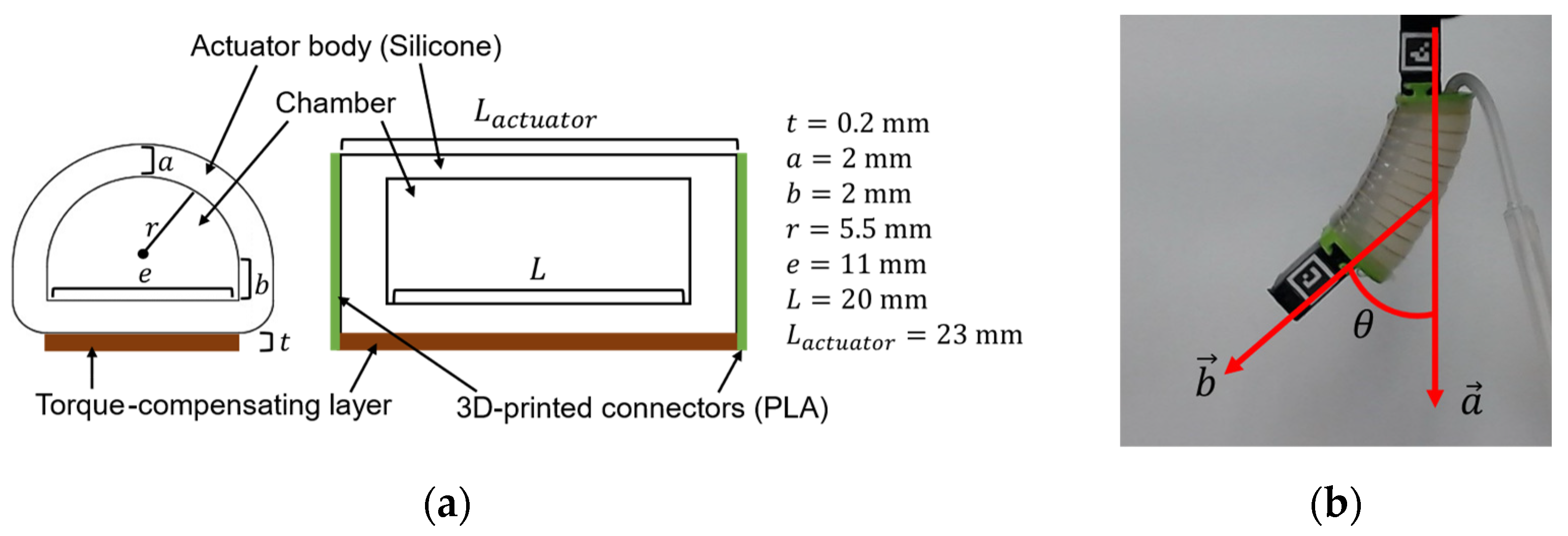
20]. Based on these considerations, the joint modular soft actuator can be considered a suitable soft actuator for use in a telerehabilitation environment because it provides high bending performance with minimal energy and can accommodate individual differences with minimal effort. However, it is necessary to incorporate an estimation of the stiffness of the finger joints (i.e., spasticity condition evaluation function), though stiffness estimation with joint modular soft actuators has not been studied yet. In this study, we designed a modular version of the SECA for actuating individual joints (Modular-SECA). However, as explained in the following paragraph, the analytical model of SECA for estimating finger joint stiffness is not completely applicable to this new type of actuator.
The analytical model of the SECA is derived from the air chamber unit energy conservation law, so the length of the air chamber is included in the analytical model, but not the length of the actuator itself. When the lengths of the air chambers are equal, the analytical model can be interpreted as indicating that the SECA and Modular-SECA have the same bending performance. Therefore, it is possible to estimate the stiffness of the Modular-SECA using the original analytical model of the SECA. However, unlike the SECA, the joint modular soft actuator has rigid connectors at both ends, and the length ratio of the actuator body to the chamber is different [
17,
20]. Therefore, the two types of soft actuators may exhibit different bending performances, and the analytical model of the SECA cannot be applied directly to that of the Modular-SECA.
Another problem of the stiffness estimation method described in [
17] is caused by using a marker-based joint angle measurement. However, it is difficult for the patient or his/her family members to attach the markers at precise positions, which limits its application to telerehabilitation.
Furthermore, using 2D markers limits the acquisition of joint angles on a flat surface, making it impossible to measure the joint angles of the middle and ring fingers, and thus making it difficult to estimate the joint stiffness of them. Zhou et al. have developed a system that simultaneously obtains the joint angles of multiple fingers and estimates their stiffness by integrating a flex sensor into an actuator [
22]. Flex sensors do not interfere with the bending response of soft actuators too much, but they must be calibrated individually for each actuator and cannot measure finger or hand orientation [
23,
24]. Moreover, using this system, it is not possible to measure joint angles when a soft actuator is not attached. By designing a system that can measure joint angles without having the soft actuators attached, it is also possible to measure joint range of motion, increasing the system’s functionality. In addition, having a high-cost system can limit how many devices can be provided for telerehabilitation [
25].
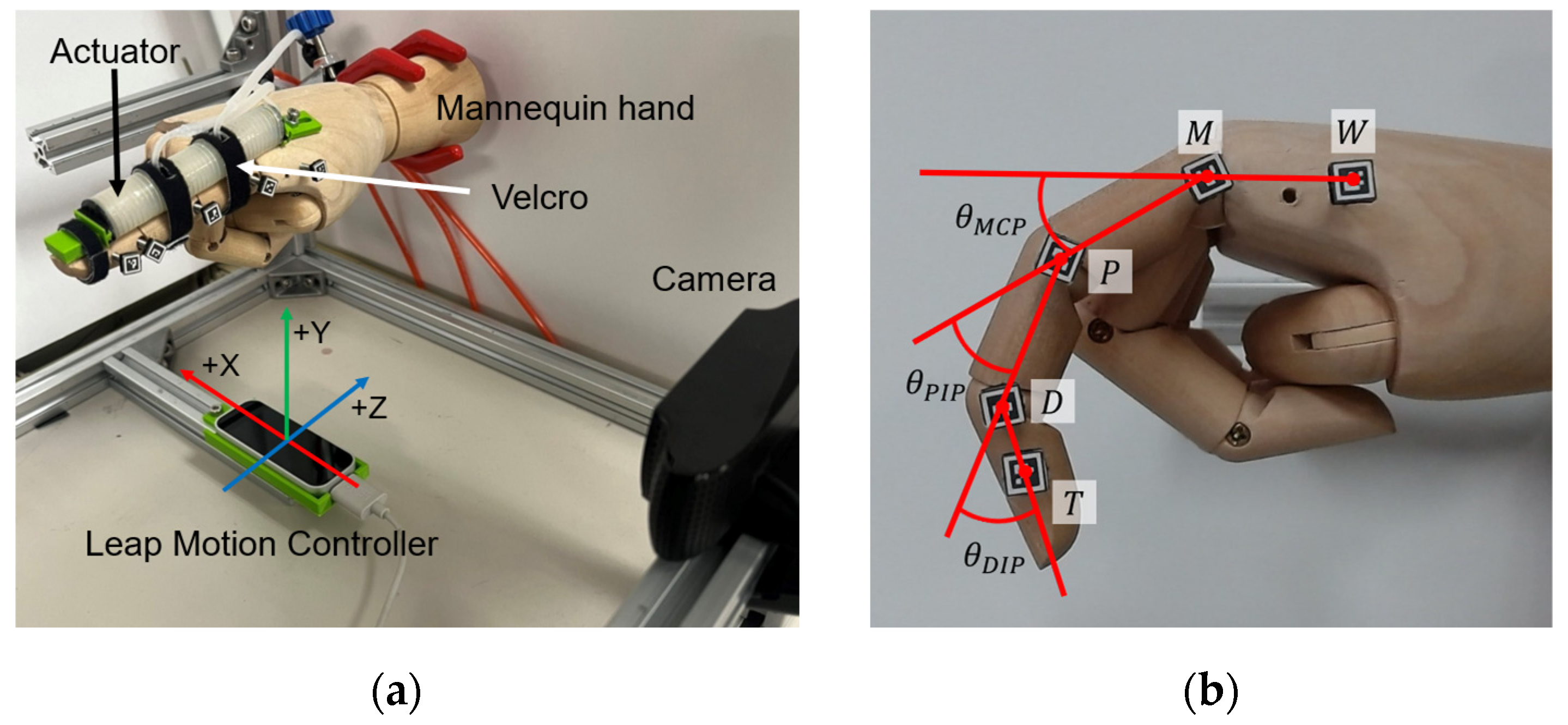
The leap motion controller (LMC) is an inexpensive and compact marker-less measurement device for tracking and acquiring the position of hand joints. Although the accuracy of hand joint angle measurement is not sufficient for rehabilitation purposes [
26], it is possible to improve the measurement accuracy by fitting a regression model of joint angle [
27]. However, the combined use of LMC and soft actuators has not yet been investigated. Especially, joint modular soft actuators may cause the motion of one single joint, which is different from most natural hand motions. It is also unclear how the attachment of the soft actuator affects the LMC and whether or not the measurement accuracy can be improved in the same way as when the soft actuator is not attached.
In this study, we proposed finger joint stiffness estimation for hand–finger joints using Modular-SECAs and the LMC, and verified the feasibility of this procedure by performing stiffness estimation on a mannequin hand and a subject’s MCP joint, respectively. We designed the Modular-SECA, a joint modular soft actuator incorporating the finger joint stiffness estimation function. In addition, correction terms (or parameters) were added to the previous analytical model for the bending analysis of a Modular-SECA supporting a joint for the purpose of hand rehabilitation. The correction parameters were determined by comparing the values of the bending angles obtained from the analytical model with measured angles from a free bending experiment with the Modular-SECAs. Moreover, a regression model accounting for the actuation for and motion of the neighboring joints was proposed to correct the direct outputs of LMC.
This paper is organized as follows: First, the design and improved analytical model of the joint modular soft actuator for stiffness estimation are presented. Next, the regression model method to improve the accuracy of LMC joint angle measurement is presented. Finally, validation experiments using a mannequin hand and a subject’s hand are presented in which stiffness estimation is performed using a combination of these methods.
4. Discussion
The results show that the SECA and Modular-SECA have different bending performances, and the interaction of joints affected the output of LMC when the Modular-SECA was attached. Furthermore, it was confirmed that the accuracy of the stiffness estimation with the Modular-SECA could be improved by correcting the analytical model of stiffness estimation and the joint angles.
4.1. Analytical Model of Modular-SECA
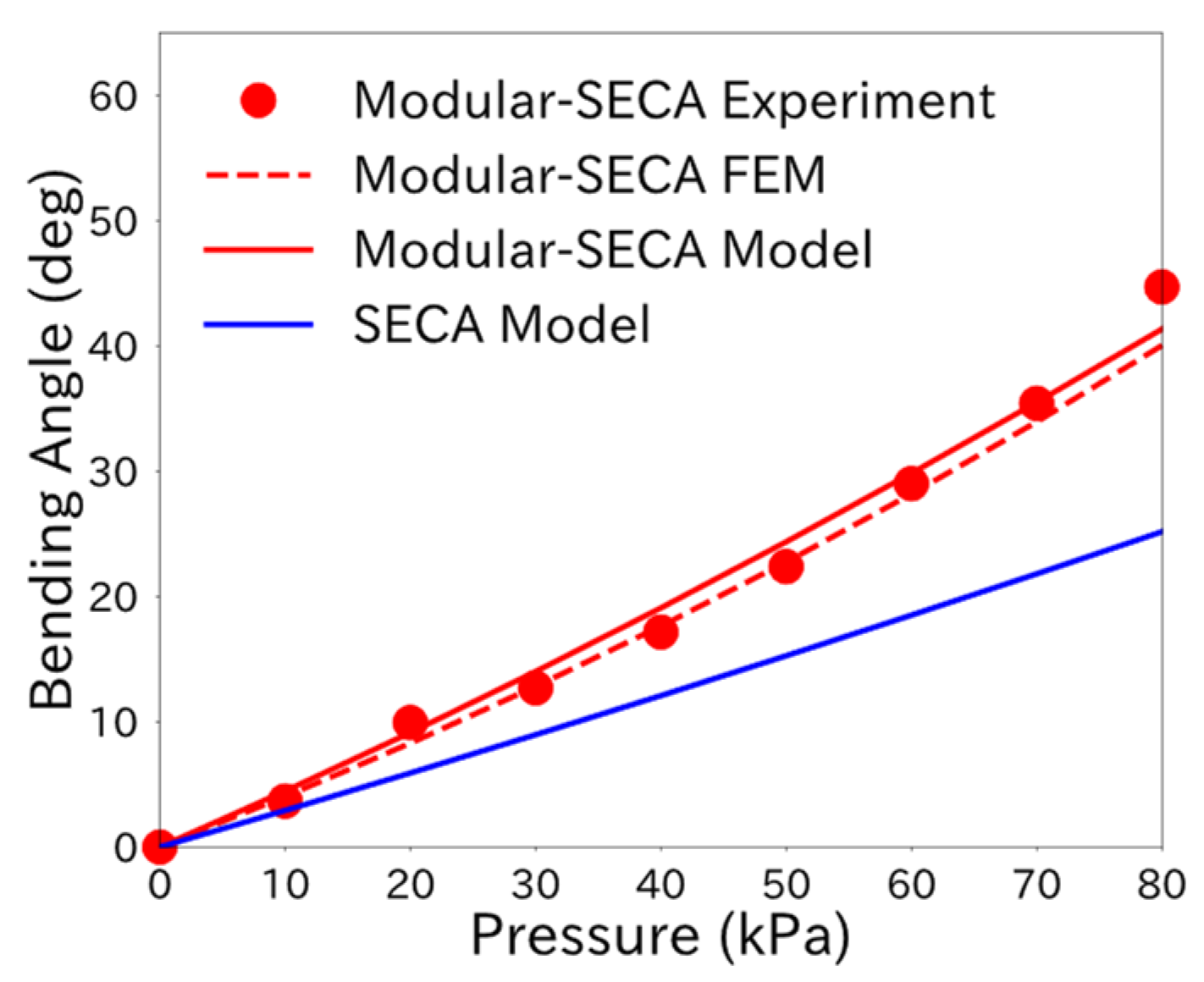
The free space bending analysis results suggest a difference in the energy distribution in the actuator between the Modular-SECA and SECA. It was confirmed that the chamber volume increase,
, relative to the air pressure input was larger for the Modular-SECA than that for the SECA. The bending strain energy,
, stored in the torque compensation layer was smaller for the Modular-SECA. This may have been due to the rigid connectors attached to both ends of the Modular-SECA, which reduced the energy allocated to
within the energy conservation law. In previous studies,
was modeled as a cantilever beam subjected to a pure bending moment [
17]. However, the Modular-SECA is considered to be subjected to an additional bending moment in the torque compensation layer. Therefore, at the same air pressure input, the energy required to bend the torque compensating layer is reduced, and the volume increase in the chamber is considered to have increased.
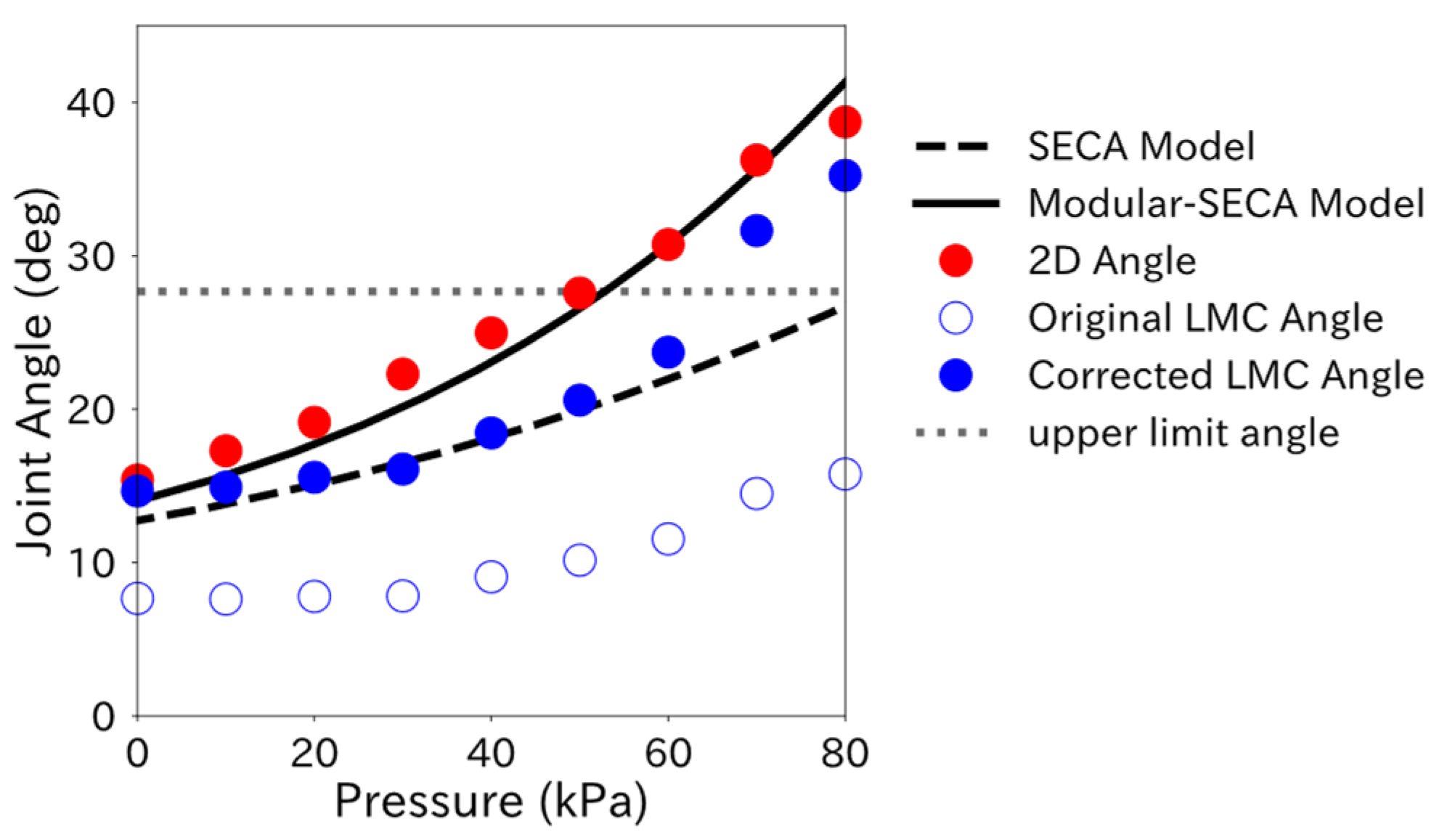
From
Figure 8, the difference between the 2D Angle and the bending angle obtained from the Modular-SECA analytical model is smaller than that in the SECA analytical model results. However, the estimated values for Method 2 (Modular-SECA Model with 2D Angle measurement) in
Table 5 did not reach the target values. This may be due to the lack of correction in the Modular-SECA analytical model. In particular, the difference between the experimental and Modular-SECA model bending angles at 0 kPa suggests that the correction may be insufficient. This difference is thought to have persisted afterward, preventing the estimation results of Method 2 from reaching the target values. A feature of the SECA is that the torque compensation layer provides a supplementary bending moment to return the finger to its initial position under reduced pressure.
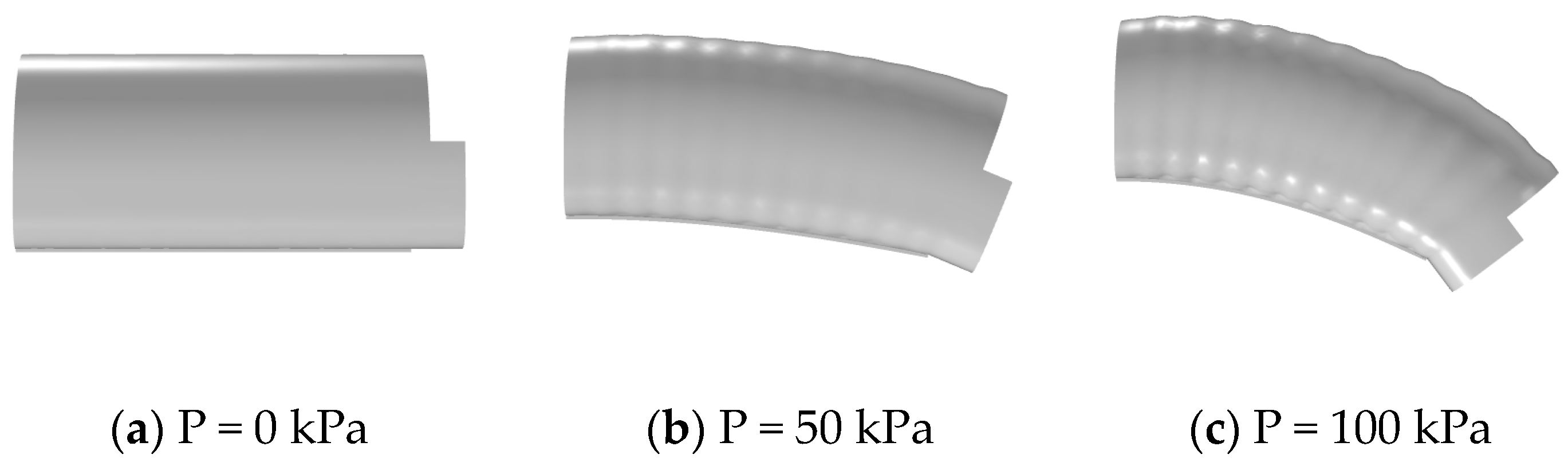
Figure 5 shows that the bending angle of Modular-SECA is larger than that of the SECA under applied pressure and that the force in the bending direction is greater. However, under reduced pressure, the auxiliary bending moment provided by the torque-compensating layer of the Modular-SECA is smaller than that of the SECA, and the force in the extension direction may be smaller.
in Equation (8) is a term that expresses the effect of the bending moment of the torque compensation layer on the bending angle. If the bending moment provided by the torque-compensation layer of the Modular-SECA is small, a correction parameter may also need to be provided for this term.
4.2. Finger Joint Angle Measurement Using Leap Motion Controller
First,
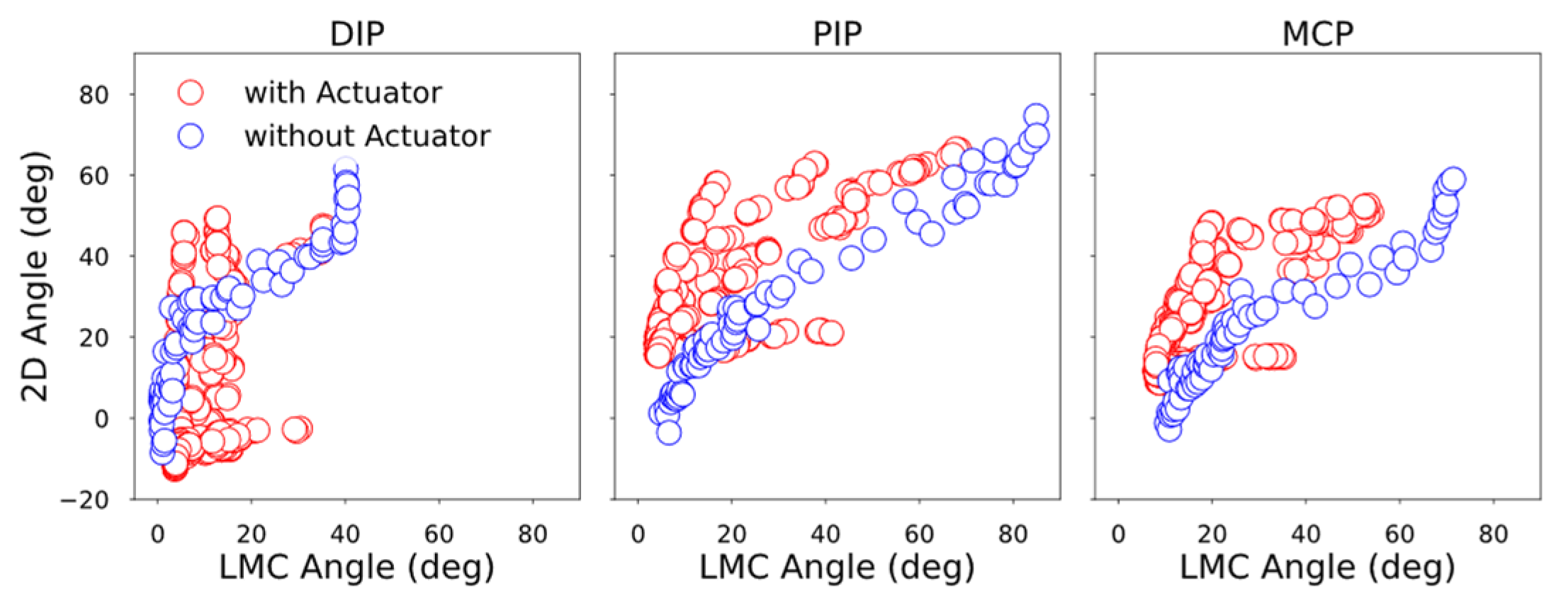
Appendix E shows that the LMC Angle change trend changes with the attachment of the soft actuator. In
Figure A2a,d, the trend of the LMC Angle change around 80 kPa is altered compared to that at the previous pressure point. Briefly, 80 kPa is when the mannequin hand’s index finger is bent to the point where the soft actuator is visible from LMC’s camera. Therefore, LMC recognized the soft actuator as a part of the finger, and the output angle changed.
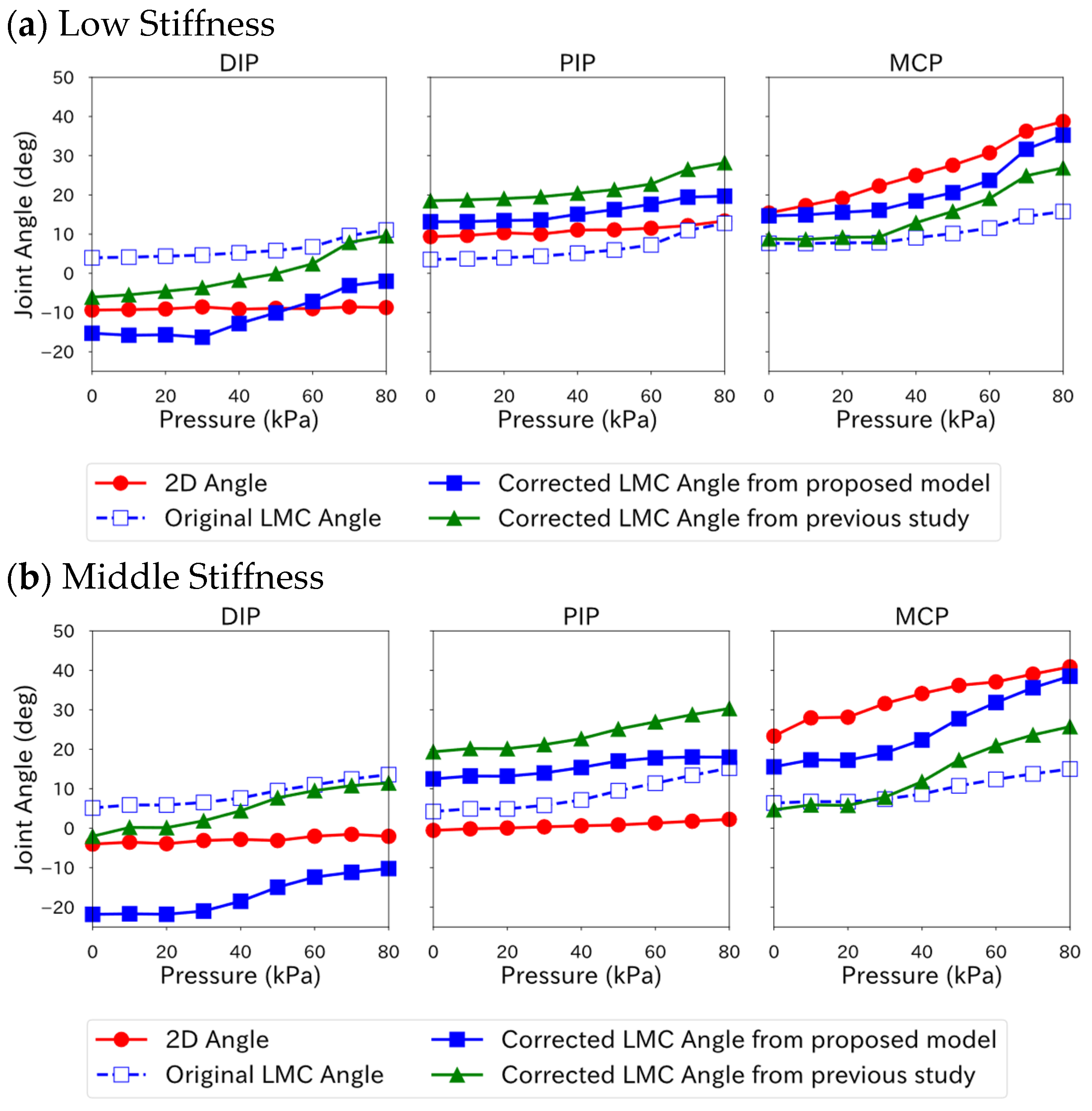
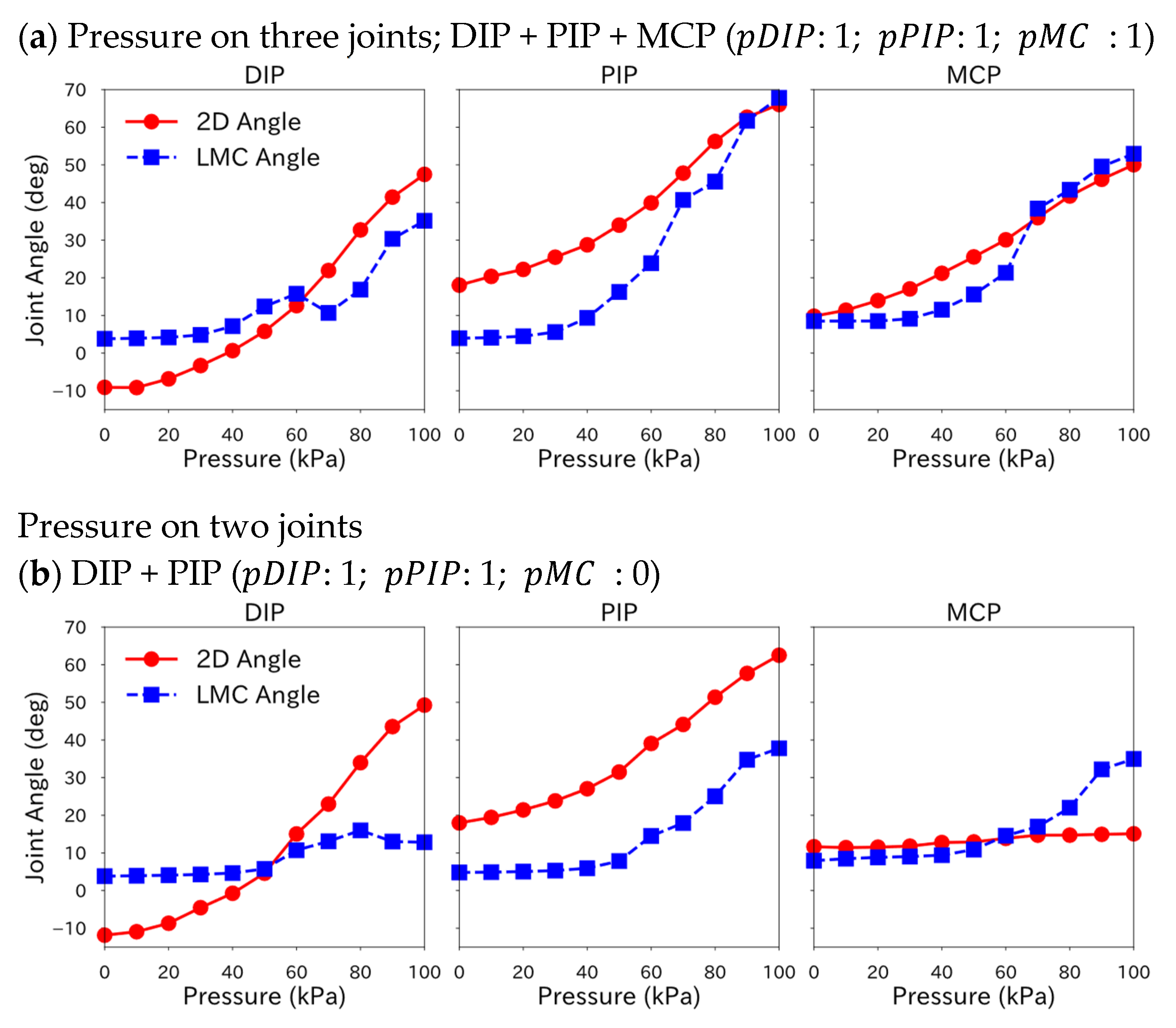
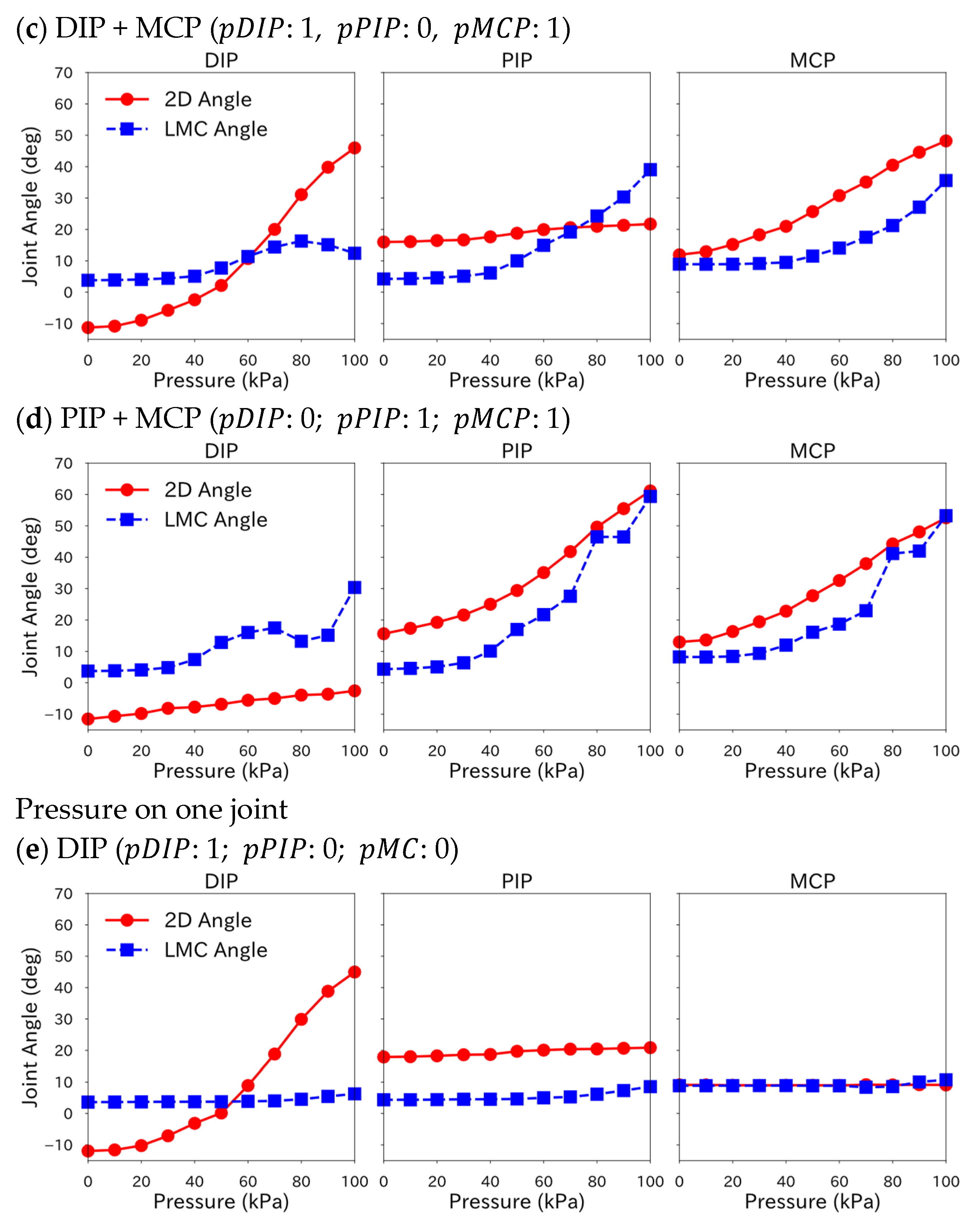
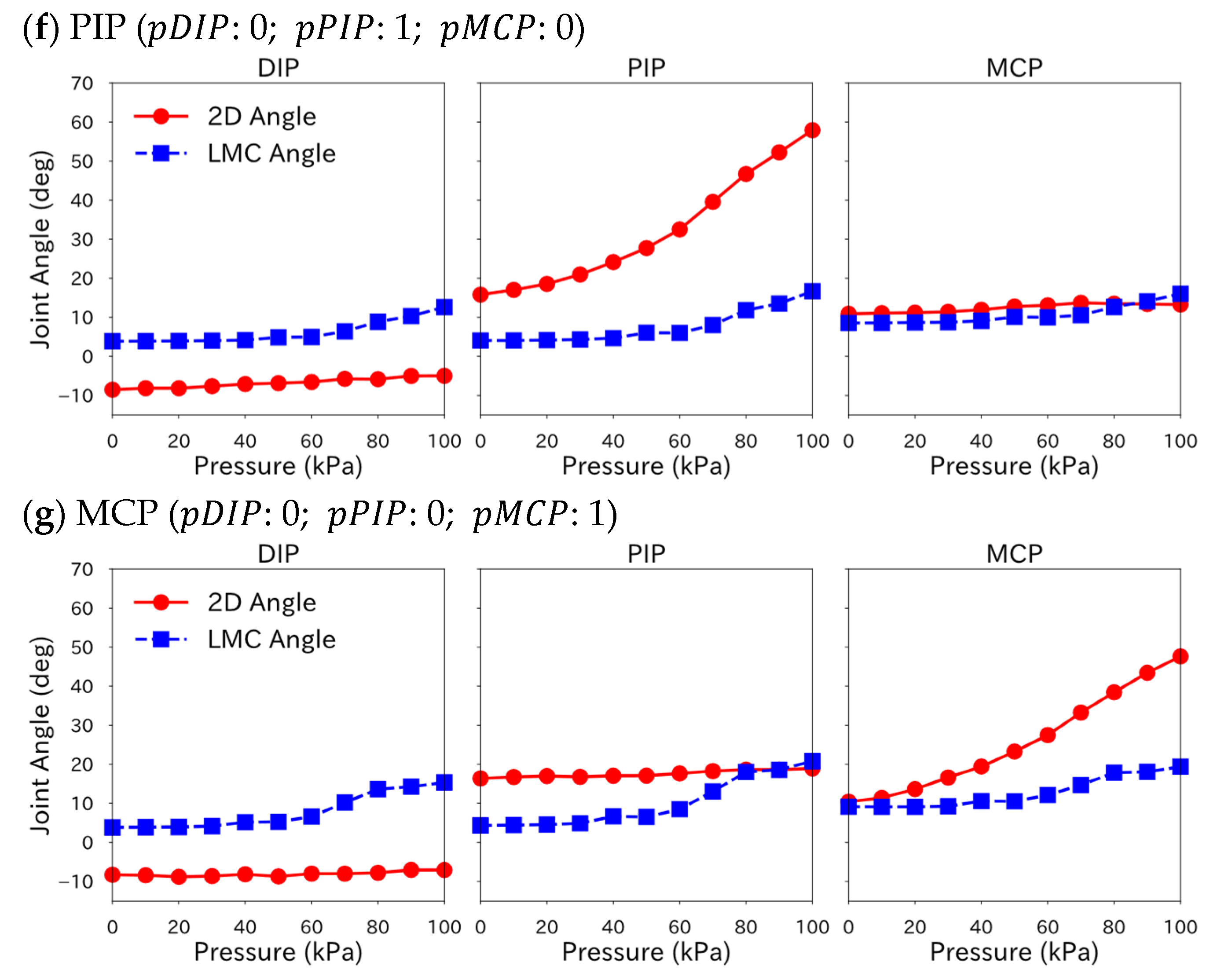
When the soft actuator was applied, the angle correction model included the angle of other joints, suggesting that LMC Angle is affected by the interaction between joints within the same finger.
Table 4 shows that the correction performance of the angle correction model is high for joints with large angle changes when the soft actuator is pressurized. However, it may be low for joints that are not pressurized and have small angle changes. This may be due to biased training data for the joints where the soft actuators are not pressurized, resulting in lower model prediction accuracy. It also suggests that including the angles of other joints in the explanatory variables may lead to an increase in correction accuracy but may also lead to a decrease. Correction performance varies with stiffness level in
Table 4 because correction accuracy varied with the angles of other joints. Although the model of the previous study can improve correction performance by increasing the order of the regression model, it requires separate models for each combination of joints to which the soft actuator applies pressure.
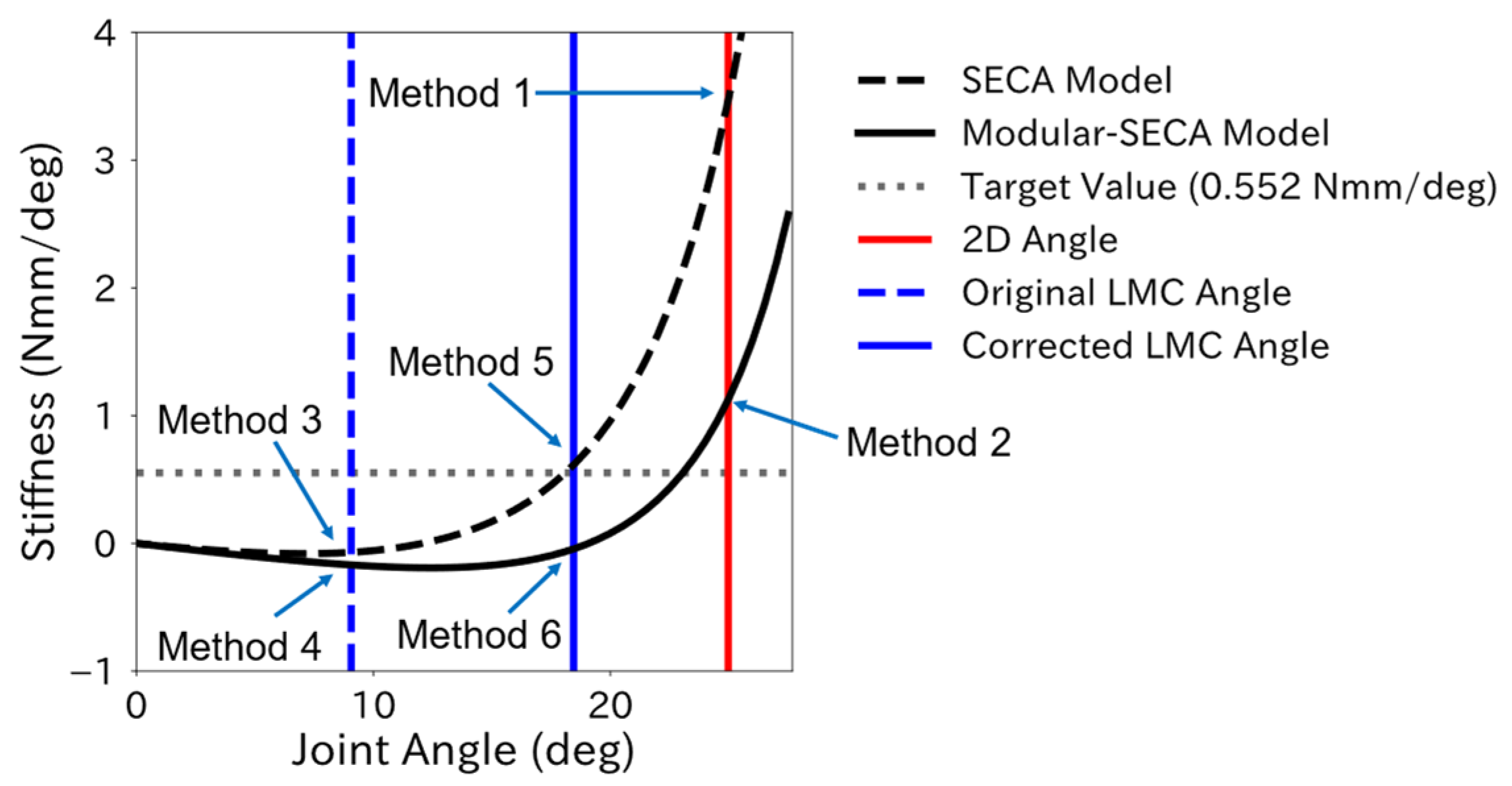
Figure 6 and
Figure 8 show that the upper limit of the stiffness estimation range using the LMC Angle is wider than that using the 2D Angle because the LMC Angle is output smaller than the 2D Angle even after correction. In
Figure 8, the stiffness estimation range for 2D Angle is 0 kPa to 50 kPa, while corrected LMC Angle is 0 kPa to 60 kPa; the stiffness estimation using the LMC Angle includes a greater stiffness value at each pressure in the final estimate stiffness value than that using the 2D Angle. Therefore, to improve the estimation performance, it is considered effective not only to improve the correction accuracy of the LMC Angle but also to change the stiffness estimation range.
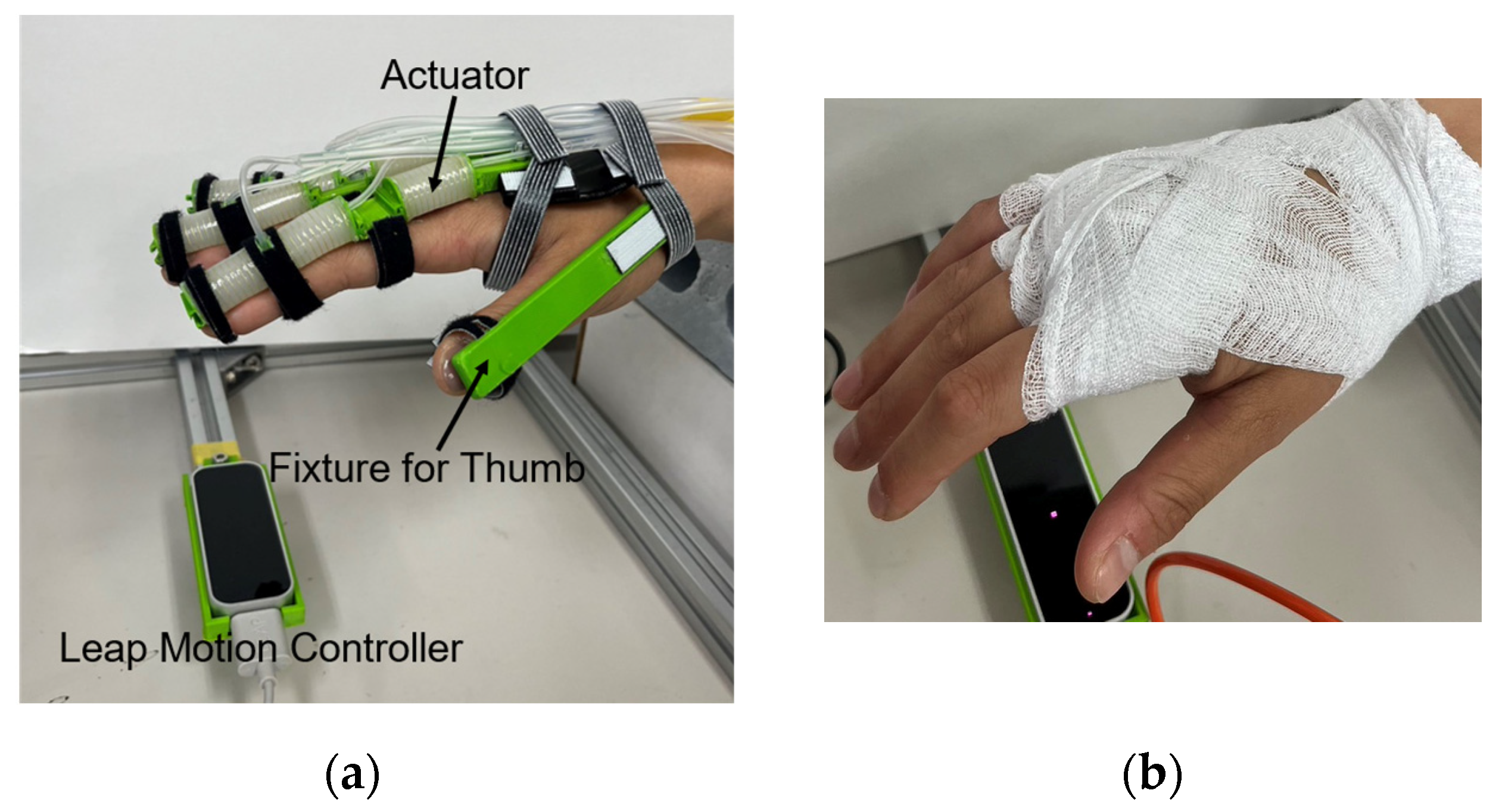
When the Modular-SECA was attached to a human hand, MCP joints were constantly flexed during the experiment, while the LMC Angle showed an extension angle. Since none of the LMC Angle of the MCPs showed an extension angle in the data when the regression model was created, the correction performance of the regression model at the extension angle was insufficient, leading to the under-correction of the LMC Angle.
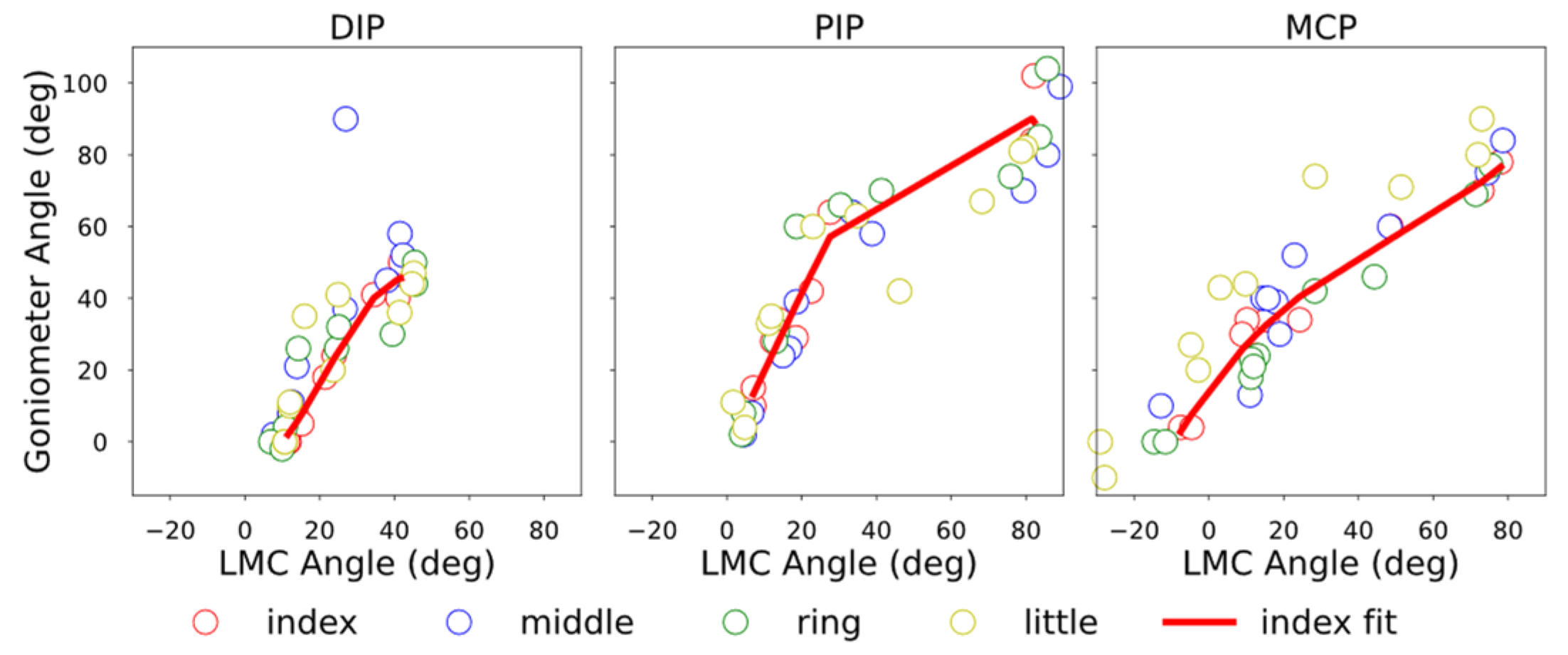
Since the angle correction model for the index finger could not be applied to the middle and ring fingers, it is necessary to derive an angle correction model for each finger separately. However, since it is difficult to measure joint angles using 2D markers for the middle and ring fingers, it is not possible to derive an angle correction model using the same method as in this study. Therefore, it is thought that the angle correction model for the index finger can be applied by excluding from the candidate explanatory variables for the regression model for the index finger those variables that include the angle of the DIP joint, which has a low degree of fit with that of the index finger.
4.3. Proposed Method for Finger Joint Stiffness Estimation
The stiffness estimation using LMC and the Modular-SECA showed that the correction of the analytical model and joint angle improves the stiffness estimation results. However, the current estimation performance of the proposed method is insufficient due to the lack of both corrections, and the correction method needs to be improved. The final stiffness estimate is the average for each pressure in the stiffness estimation range, but variations exist among the estimates for each pressure. Therefore, the performance of the proposed method may be improved by weighting the more reliable estimates in the stiffness estimation range.
4.4. Contribution and Limitations
By using joint modular soft actuators, high bending performance can be achieved with minimal energy for telerehabilitation, and individual differences such as different finger sizes and different joint stiffness values can be accommodated with minimal effort.
Our contribution includes the following:
To the best of our knowledge, for the first time, finger joint stiffness estimation for using joint modular soft actuators was proposed and implemented. The accuracy of stiffness estimation needs further improvement, though the possibility has been shown and the direction for improvement has been made clear. In addition, the proposed stiffness estimation method enables the simultaneous measurement of multiple fingers, although the analytical model and the correction method for joint angles need to be improved.
The analytic model was updated from a previous model for the SECA, a whole-finger soft actuator, with additional parameters for accounting for the features of the joint modular soft actuator. The model could be regressed from experimental data and give a better prediction of the behavior of the joint modular actuators.
Leap Motion Controller was used for the first time for the angle measurement of joints of fingers supported by the joint modular soft actuators. A regression model was proposed to correct measurement results, taking into consideration multiple joint interaction intensified by wearing the soft actuators, and the influence of the actuation of the joint modular soft actuators. The effectiveness of the correction was validated by the experiment results. LMC can be used to measure the angles of finger joints not only when soft actuators are attached, regardless of whether they are actuated or not, but also when soft actuators are not attached.
On the other hand, there are several methodological and implementational limitations:
The high stiffness of joint cannot be estimated with the Modular-SECA. The reference value for high stiffness (a MAS (modified Ashworth scale) score of about 3) is 9.60 N mm/deg. Because the extension of the highly stiff finger caused by wearing the Modular-SECA was small compared with that of the SECA, the joint angle, , was not within the stiffness estimation range, . To estimate high stiffness as well, it is necessary to design a joint modular actuator that can extend the finger sufficiently with its intrinsic stiffness, or add another component to actively extend the joint extension.
Only the stiffness estimation of MCP joints of multiple fingers was tested. The stiffness estimation of DIP and PIP joints of multiple fingers needs to be tested in future.
The regression model used to correct the LMC Angle generated using data acquired from mannequin hands did not apply to human hands. Although mannequin hands are effective for multiple measurements due to their low data variability, they are unsuitable for model generation because they do not reproduce human finger movements such as intra-finger constraint. Therefore, if an angle correction model is generated using data acquired from a human hand, it may apply to both mannequin hands and human hands. Moreover, this may allow the generated regression model to be adaptable to the individual difference of hand dimensions.
The manually controlled input air pressure affected the human hand’s stiffness estimation. The speed at which the joint moves, which is affected by the input air pressure, is a factor that influences joint stiffness [
37,
38]. In the case of manual control, the rotational speed of the joints differed from measurement to measurement, which may have increased the variation in data. Thus, automatic pneumatic input control is necessary to realize the proposed method.
In this study, we did not test stiffness estimation in a telerehabilitation setting. In the near future, it is necessary to verify the effectiveness of the proposed method in such a setting.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}












