
Unique Biomarkers of Collagen Type III Remodeling Reflect Different Information Regarding Pathological Kidney Tissue Alterations in Patients with IgA Nephropathy
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Data Collection
2.3. Kidney Biopsy and Fibrosis Evaluation
2.4. Assays
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Study Cohort and Association with Collagen Type III Biomarkers
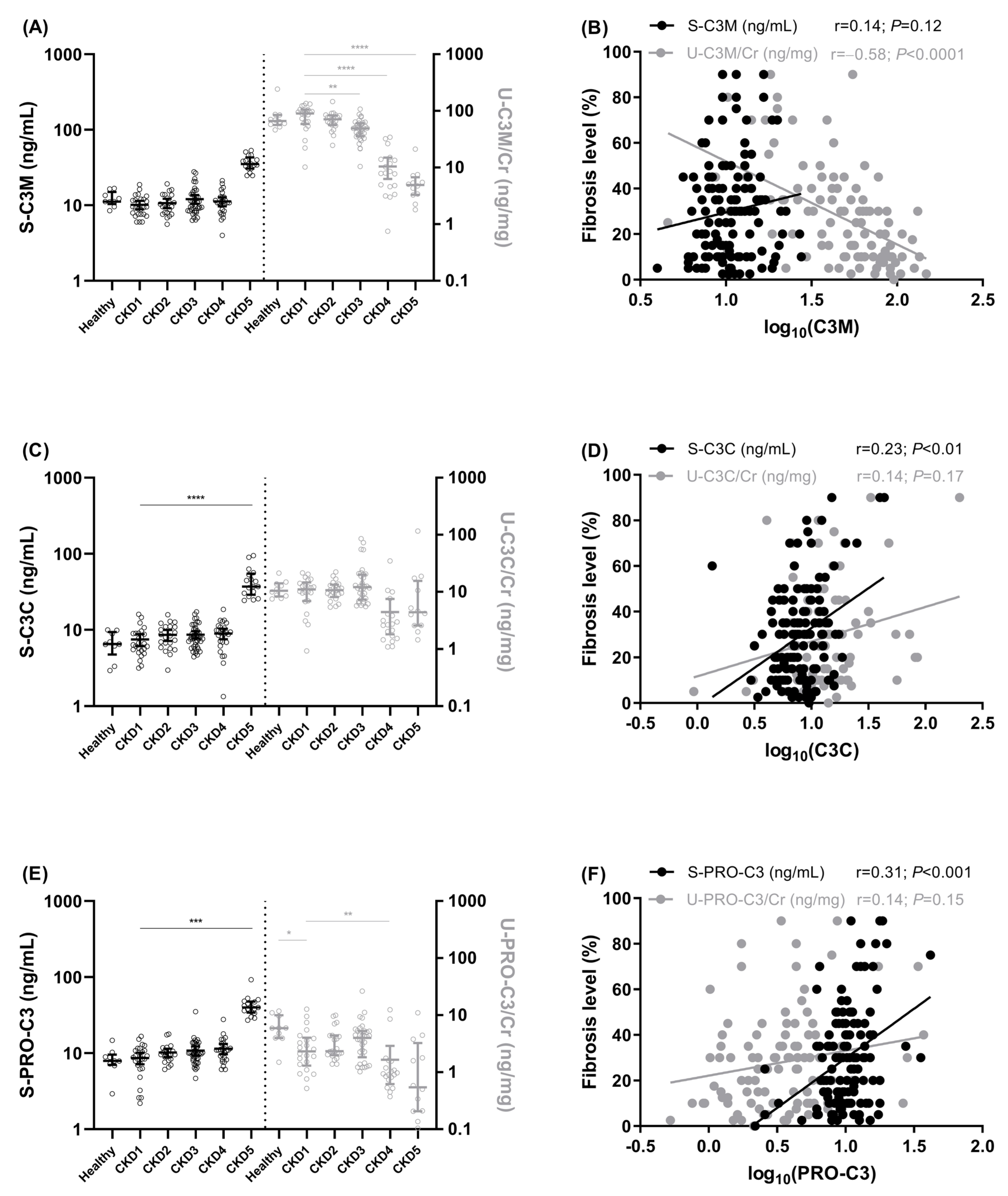
3.2. Association of Collagen Type III Biomarkers with Kidney Fibrosis
3.3. Comparison of Biomarker Association with Fibrosis Levels
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Penfold, R.S.; Prendecki, M.; McAdoo, S.; Tam, F.W.K. Primary IgA Nephropathy: Current Challenges and Future Prospects. Int. J. Nephrol. Renovasc. Dis. 2018, 11, 137–148. [Google Scholar] [PubMed] [Green Version]
- Maixnerova, D.; Jancova, E.; Skibova, J.; Rysava, R.; Rychlik, I.; Viklicky, O.; Merta, M.; Kolsky, A.; Reiterova, J.; Neprasova, M.; et al. Nationwide Biopsy Survey of Renal Diseases in the Czech Republic during the Years 1994–2011. J. Nephrol. 2014, 28, 39–49. [Google Scholar] [CrossRef]
- Suzuki, H.; Kiryluk, K.; Novak, J.; Moldoveanu, Z.; Herr, A.B.; Renfrow, M.B.; Wyatt, R.J.; Scolari, F.; Mestecky, J.; Gharavi, A.G.; et al. The Pathophysiology of IgA Nephropathy. J. Am. Soc. Nephrol. 2011, 22, 1795–1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, S.C.; Cheung, C.K.; Barratt, J. New Insights into the Pathogenesis of IgA Nephropathy. Pediatr. Nephrol. 2018, 33, 763–777. [Google Scholar] [CrossRef] [Green Version]
- Kuivaniemi, H.; Tromp, G. Type III Collagen (COL3A1): Gene and Protein Structure, Tissue Distribution, and Associated Diseases. Gene 2019, 707, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Karsdal, M.A.; Genovese, F.; Rasmussen, D.G.K.; Bay-Jensen, A.C.; Mortensen, J.H.; Holm Nielsen, S.; Willumsen, N.; Jensen, C.; Manon-Jensen, T.; Jennings, L.; et al. Considerations for Understanding Protein Measurements: Identification of Formation, Degradation and More Pathological Relevant Epitopes. Clin. Biochem. 2021, 97, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Genovese, F.; Manresa, A.A.; Leeming, D.J.; Karsdal, M.A.; Boor, P. The Extracellular Matrix in the Kidney: A Source of Novel Non-Invasive Biomarkers of Kidney Fibrosis? Fibrogenes. Tissue Repair 2014, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Genovese, F.; Akhgar, A.; Lim, S.S.; Farris, A.B.; Sinibaldi, D.; Karsdal, M.A.; White, W.I.; Battle, M.; Cobb, J. Collagen Type III and VI Remodeling Biomarkers Are Associated with Kidney Fibrosis in Lupus Nephritis. KIDNEY360 2021, 2, 1473–1481. [Google Scholar]
- Genovese, F.; Rasmussen, D.G.K.; Karsdal, M.A.; Jesky, M.; Ferro, C.; Fenton, A.; Cockwell, P. Imbalanced Turnover of Collagen Type III Is Associated with Disease Progression and Mortality in High-Risk Chronic Kidney Disease Patients. Clin. Kidney J. 2021, 14, 593–601. [Google Scholar] [CrossRef] [Green Version]
- Genovese, F.; Boor, P.; Papasotiriou, M.; Leeming, D.J.; Karsdal, M.A.; Floege, J. Turnover of Type III Collagen Reflects Disease Severity and Is Associated with Progression and Microinflammation in Patients with IgA Nephropathy. Nephrol. Dial. Transplant. 2016, 31, 472–479. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, D.G.K.; Sand, J.M.B.; Karsdal, M.A.; Genovese, F. Development of a Novel Enzyme-Linked Immunosorbent Assay Targeting a Neo-Epitope Generated by Cathepsin-Mediated Turnover of Type III Collagen and Its Application in Chronic Obstructive Pulmonary Disease. PLoS ONE 2017, 12, e0170023. [Google Scholar] [CrossRef] [Green Version]
- Sparding, N.; Genovese, F.; Rasmussen, D.G.K.; Karsdal, M.A.; Neprasova, M.; Maixnerova, D.; Satrapova, V.; Frausova, D.; Hornum, M.; Bartonova, L.; et al. Endotrophin, a Collagen Type VI-Derived Matrikine, Reflects the Degree of Renal Fibrosis in Patients with IgA Nephropathy and in Patients with ANCA-Associated Vasculitis. Nephrol. Dial. Transplant. 2022, 37, 1099–1108. [Google Scholar] [CrossRef]
- Neprasova, M.; Maixnerova, D.; Sparding, N.; Genovese, F.; Karsdal, M.A.; Koprivova, H.; Kollar, M.; Suchanek, M.; Hruskova, Z.; Tesar, V. Serum and Urine Biomarkers Related to Kidney Fibrosis Predict Kidney Outcome in Czech Patients with IgA Nephropathy. Int. J. Mol. Sci. 2023, 24, 2064. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro III, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate Disclosure of Conflicts of Interest: We Have Received Confirmation from Drs. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [PubMed]
- Loupy, A.; Haas, M.; Solez, K.; Racusen, L.; Glotz, D.; Seron, D.; Nankivell, B.J.; Colvin, R.B.; Afrouzian, M.; Akalin, E.; et al. The Banff 2015 Kidney Meeting Report: Current Challenges in Rejection Classification and Prospects for Adopting Molecular Pathology. Am. J. Transplant. 2017, 17, 28–41. [Google Scholar] [CrossRef]
- Trimarchi, H.; Barratt, J.; Cattran, D.C.; Cook, H.T.; Coppo, R.; Haas, M.; Liu, Z.-H.; Roberts, I.S.D.; Yuzawa, Y.; Zhang, H.; et al. Oxford Classification of IgA Nephropathy 2016: An Update from the IgA Nephropathy Classification Working Group. Kidney Int. 2017, 91, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, M.J.; Nedergaard, A.F.; Sun, S.; Veidal, S.S.; Larsen, L.; Zheng, Q.; Suetta, C.; Henriksen, K.; Christiansen, C.; Karsdal, M.A.; et al. The Neo-Epitope Specific PRO-C3 ELISA Measures True Formation of Type III Collagen Associated with Liver and Muscle Parameters. Am. J. Transl. Res. 2013, 5, 303–315. [Google Scholar] [PubMed]
- Barascuk, N.; Veidal, S.S.; Larsen, L.; Larsen, D.V.; Larsen, M.R.; Wang, J.; Zheng, Q.; Xing, R.; Cao, Y.; Rasmussen, L.M.; et al. A Novel Assay for Extracellular Matrix Remodeling Associated with Liver Fibrosis: An Enzyme-Linked Immunosorbent Assay (ELISA) for a MMP-9 Proteolytically Revealed Neo-Epitope of Type III Collagen. Clin. Biochem. 2010, 43, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Papasotiriou, M.; Genovese, F.; Klinkhammer, B.M.; Kunter, U.; Nielsen, S.H.; Karsdal, M.A.; Floege, J.; Boor, P. Serum and Urine Markers of Collagen Degradation Reflect Renal Fibrosis in Experimental Kidney Diseases. Nephrol. Dial. Transplant. 2015, 30, 1112–1121. [Google Scholar] [CrossRef] [Green Version]
- Djudjaj, S.; Boor, P. Cellular and Molecular Mechanisms of Kidney Fibrosis. Mol. Asp. Med. 2019, 65, 16–36. [Google Scholar] [CrossRef]
- Lennon, R.; Byron, A.; Humphries, J.D.; Randles, M.J.; Carisey, A.; Murphy, S.; Knight, D.; Brenchley, P.E.; Zent, R.; Humphries, M.J. Global Analysis Reveals the Complexity of the Human Glomerular Extracellular Matrix. J. Am. Soc. Nephrol. 2014, 25, 939–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, B.; Yu, M.; Zheng, J. Transport and Interactions of Nanoparticles in the Kidneys. Nat. Rev. Mater. 2018, 3, 358–374. [Google Scholar] [CrossRef]
- Koide, H.; Nakamura, T.; Ebihara, I.; Tomino, Y. Increased MRNA Expression of Metalloproteinase-9 in Peripheral Blood Monocytes from Patients with Immunoglobulin A Nephropathy. Am. J. Kidney Dis. 1996, 28, 32–39. [Google Scholar] [CrossRef]
- Paunas, F.T.I.; Finne, K.; Leh, S.; Osman, T.A.-H.; Marti, H.-P.; Berven, F.; Vikse, B.E. Characterization of Glomerular Extracellular Matrix in IgA Nephropathy by Proteomic Analysis of Laser-Captured Microdissected Glomeruli. BMC Nephrol. 2019, 20, 410. [Google Scholar] [CrossRef] [Green Version]
- Cocchiaro, P.; De Pasquale, V.; Morte, R.D.; Tafuri, S.; Avallone, L.; Pizard, A.; Moles, A.; Pavone, L.M. The Multifaceted Role of the Lysosomal Protease Cathepsins in Kidney Disease. Front. Cell Dev. Biol. 2017, 5, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Yang, Y.; Wu, Y. The Clinical Significance and Potential Role of Cathepsin S in IgA Nephropathy. Front. Pediatr. 2021, 9, 631473. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Liu, X.; Li, Y.; Lu, Y.; Zhong, H.; Jiang, W.; Chen, A.F.; Billiar, T.R.; Yuan, H.; Cai, J. Cathepsin L Activity Correlates with Proteinuria in Chronic Kidney Disease in Humans. Int. Urol. Nephrol. 2017, 49, 1409–1417. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Name | Description | Target Gene | Target Sequence | Biological Function | References |
|---|---|---|---|---|---|
| C3M | A fragment of type III collagen released by MMP-9 | COL3A1 | KNGETGPQGP | Interstitial matrix degradation | [18,19] |
| C3C | A fragment of type III collagen released by cathepsin-B, -L, and -S | COL3A1 | GLPGTGGPPG | Interstitial matrix degradation | [11] |
| PRO-C3 | N-terminal type III collagen pro-peptide released by ADAMTS-2 | COL3A1 | PTGGQNYSP | Interstitial matrix formation | [17,19] |
| Variables | Healthy | IgAN | N (IgAN) |
|---|---|---|---|
| N | 10 | 134 | 134 |
| Women, % | 90 **** | 31 | 134 |
| Age, year | 41 (39–42) ns | 43 (32–54) | 134 |
| sCr, mg/dL | NA | 1.7 (1.0–2.4) | 134 |
| eGFR, mL/min/1.73 m2 | NA | 46 (26–82) | 134 |
| PU, g/day | NA | 1.7 (0.8–3.2) | 131 |
| CRP, mg/L | NA | 2.5 (1.0–4.8) | 126 |
| CKD stage (1,2,3,4,5), % | NA | 19, 16, 31, 20, 13 | 134 |
| Level of fibrosis, % | NA | 30 (10–40) | 128 |
| Banff score (ci0, ci1, ci2, ci3), % | NA | 11, 34, 38, 17 | 133 |
| T-score (T0, T1, T2), % | NA | 45, 36, 19 | 130 |
| Hypertension a, % | NA | 64 | 134 |
| Diabetes b, % | NA | 8 | 134 |
| Variables | Level of Fibrosis | S-C3M | U-C3M/Cr | S-C3C | U-C3C/Cr | S-PRO-C3 | U-PRO-C3/Cr | |
|---|---|---|---|---|---|---|---|---|
| IgAN | Age | 0.11 | 0.04 | −0.30 ** | 0.04 | 0.22 * | 0.08 | 0.13 |
| sCr | 0.64 **** | 0.18 * | −0.70 **** | 0.33 *** | 0.20 * | 0.31 *** | 0.26 ** | |
| eGFR | −0.63 **** | −0.18 * | 0.66 **** | −0.34 *** | −0.24 * | −0.36 **** | −0.34 *** | |
| PU | 0.18 * | −0.05 | −0.32 ** | 0.10 | 0.06 | 0.05 | 0.07 | |
| CRP | 0.02 | 0.29 ** | −0.08 | 0.34 *** | 0.13 | 0.18 * | 0.07 |
| Biomarkers | AUC | 95% CI | p-Value | Sensitivity | Specificity | Criterion | Correct Classification |
|---|---|---|---|---|---|---|---|
| sCr | 0.87 | 0.80–0.92 | <0.0001 | 77.3 | 87.4 | >2.6 | 85.0% |
| S-C3M | 0.61 | 0.52–0.69 | 0.11 | 59.1 | 65.8 | >11.5 | 64.7% |
| U-C3M/Cr | 0.81 | 0.72–0.88 | <0.0001 (vs. sCr p = 0.64) | 81.3 | 71.4 | ≤38.5 | 72.9% |
| S-C3C | 0.72 | 0.64–0.79 | <0.001 (vs. sCr p = 0.06) | 54.6 | 83.8 | >11.7 | 78.2% |
| U-C3C/Cr | 0.58 | 0.48–0.67 | 0.35 | 50.0 | 73.6 | >14.6 | 70.1% |
| S-PRO-C3 | 0.64 | 0.55–0.72 | 0.06 | 54.6 | 76.6 | >11.9 | 72.2% |
| U-PRO-C3/Cr | 0.52 | 0.42–0.61 | 0.86 | 25.0 | 86.8 | >7.9 | 77.6% |
| Linear Regression | Univariate | Multivariate |
|---|---|---|
| Variables | r | rpartial |
| sCr | 0.62 **** | 0.29 ** |
| PU | 0.14 | NR |
| S-C3M | 0.13 | NR |
| U-C3M/Cr | −0.51 **** | −0.24 ** |
| S-C3C | 0.24 ** | NR |
| U-C3C/Cr | 0.23 * | NR |
| S-PRO-C3 | 0.30 *** | NR |
| U-PRO-C3/Cr | 0.18 | NR |
| Hypertension, yes | 0.17 | NR |
| Diabetes, yes | −0.15 | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sparding, N.; Neprasova, M.; Maixnerova, D.; Genovese, F.; Karsdal, M.A.; Kollar, M.; Koprivova, H.; Hruskova, Z.; Tesar, V. Unique Biomarkers of Collagen Type III Remodeling Reflect Different Information Regarding Pathological Kidney Tissue Alterations in Patients with IgA Nephropathy. Biomolecules 2023, 13, 1093. https://doi.org/10.3390/biom13071093
Sparding N, Neprasova M, Maixnerova D, Genovese F, Karsdal MA, Kollar M, Koprivova H, Hruskova Z, Tesar V. Unique Biomarkers of Collagen Type III Remodeling Reflect Different Information Regarding Pathological Kidney Tissue Alterations in Patients with IgA Nephropathy. Biomolecules. 2023; 13(7):1093. https://doi.org/10.3390/biom13071093
Chicago/Turabian StyleSparding, Nadja, Michaela Neprasova, Dita Maixnerova, Federica Genovese, Morten Asser Karsdal, Marek Kollar, Helena Koprivova, Zdenka Hruskova, and Vladimir Tesar. 2023. "Unique Biomarkers of Collagen Type III Remodeling Reflect Different Information Regarding Pathological Kidney Tissue Alterations in Patients with IgA Nephropathy" Biomolecules 13, no. 7: 1093. https://doi.org/10.3390/biom13071093