

Biliverdin Reductase B Is a Plasma Biomarker for Intraplaque Hemorrhage and a Predictor of Ischemic Stroke in Patients with Symptomatic Carotid Atherosclerosis
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Study
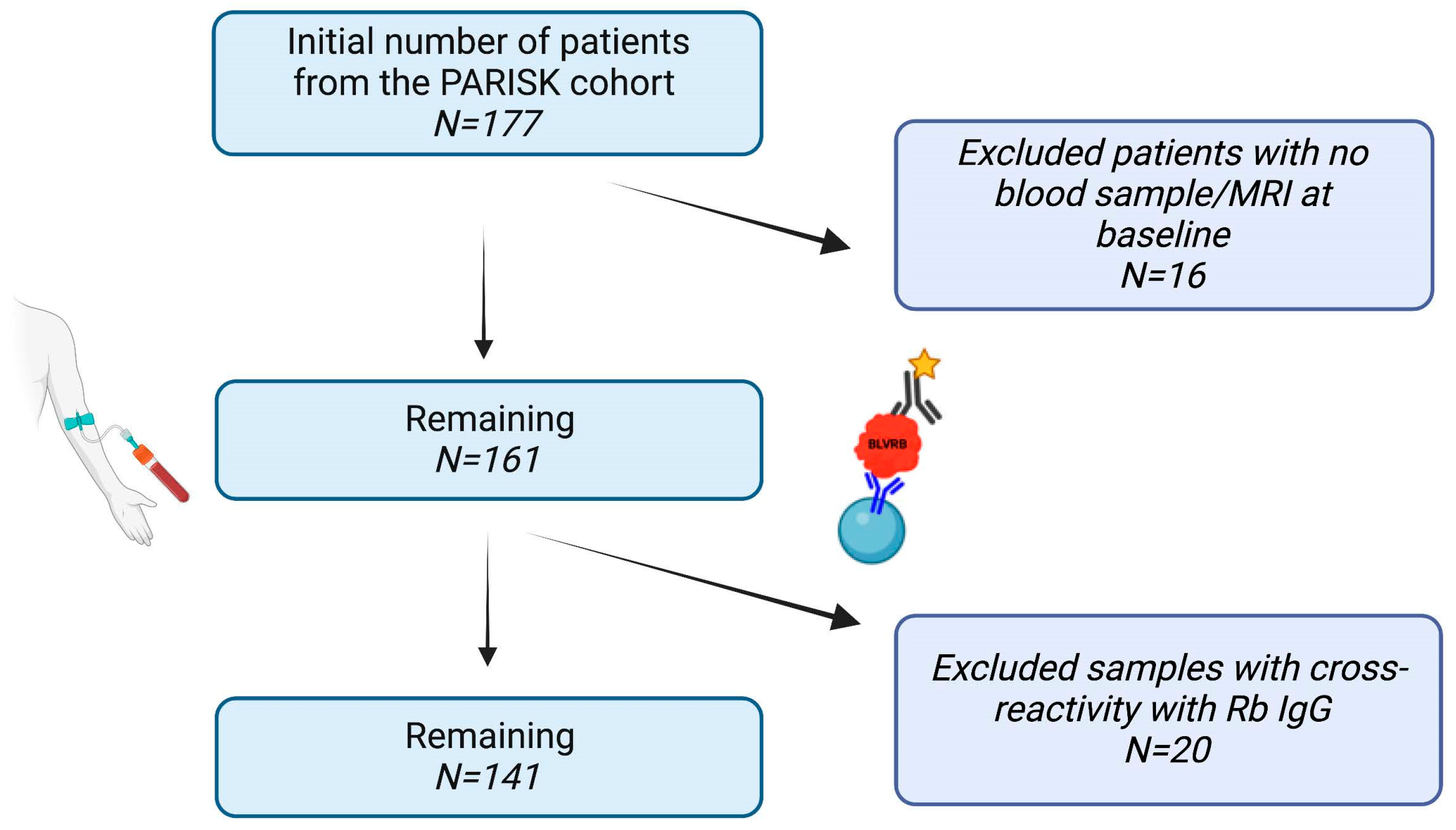
2.1.1. Patient Cohort
2.1.2. Magnetic Resonance Imaging (MRI)
2.2. Animal Study
2.2.1. Vein Graft Model
2.2.2. Histological and Immunohistochemical Analysis
2.3. Analysis of Plasma BLVRB Levels
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics and IPH
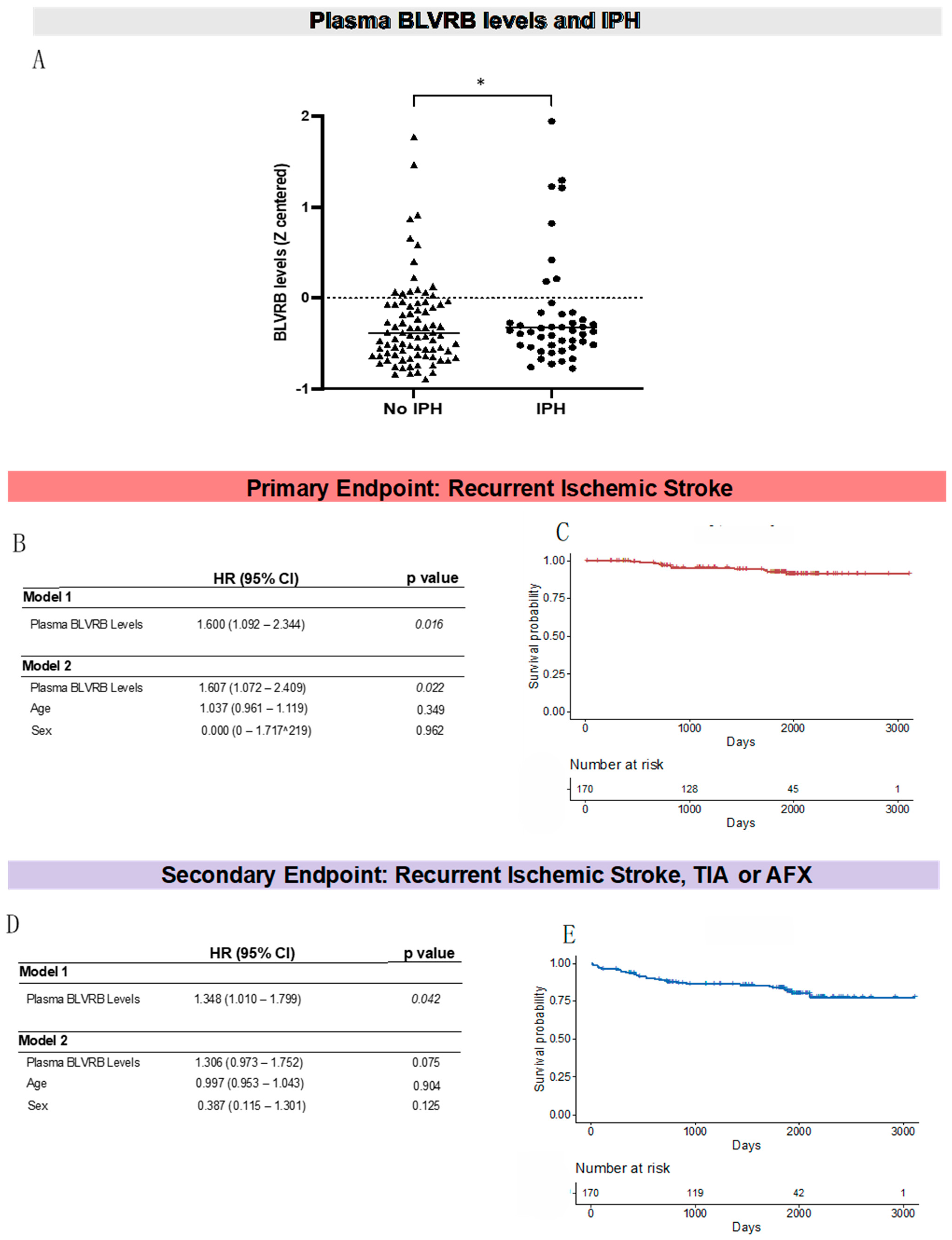
3.2. Plasma BLVRB Levels Are Significantly Higher in Patients with Carotid Plaque IPH
3.3. Plasma BLVRB Levels Associate with Recurrent Ischemic Stroke
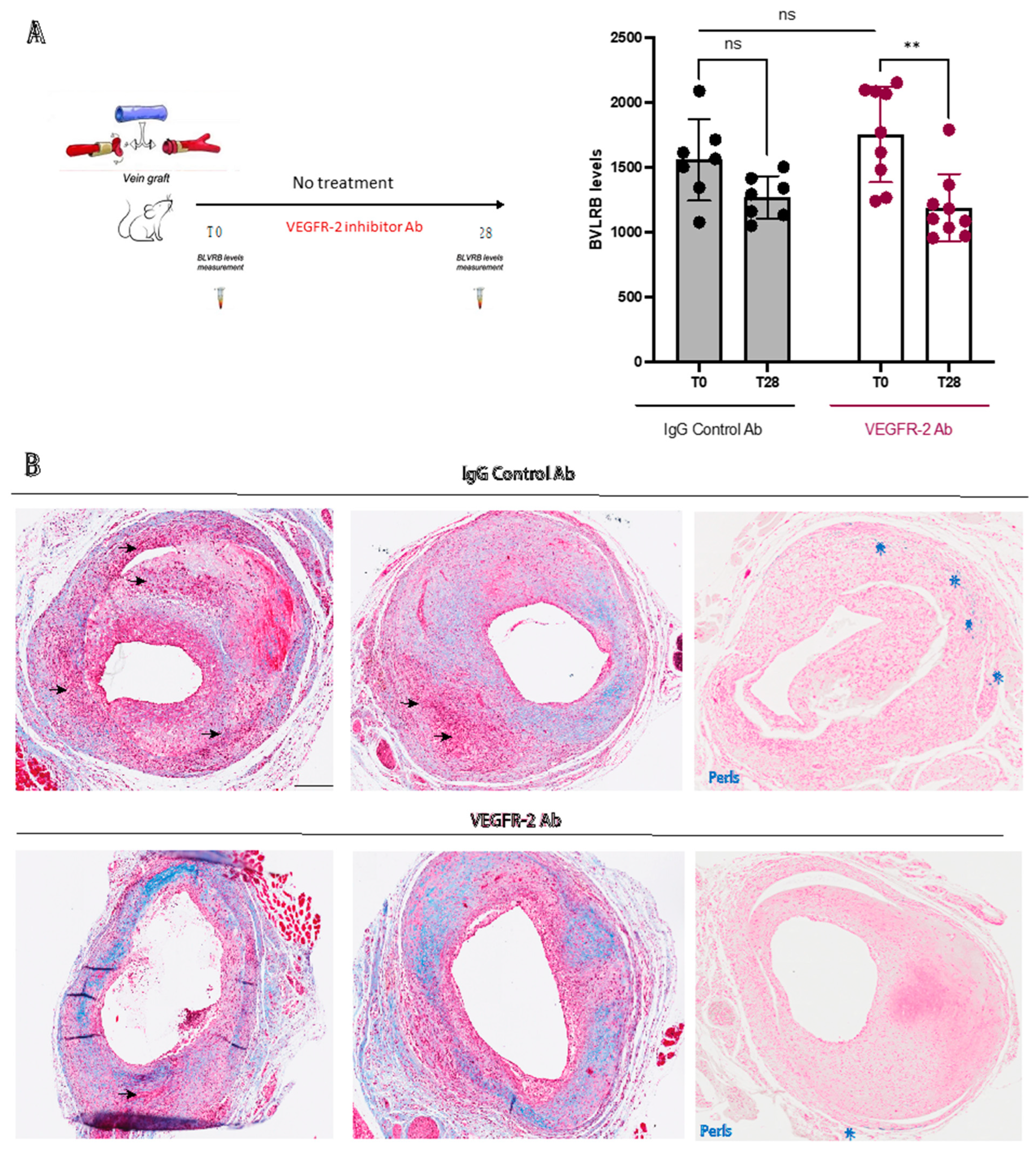
3.4. Plasma BLVRB Levels Reflect Inhibition of IPH in Mice
4. Discussion
4.1. Plasma BLVRB Levels Are Associated with IPH in Patients with Symptomatic Carotid Atherosclerosis
4.2. Plasma BLVRB Levels Predict Recurrent Ischemic Stroke in Patients with Symptomatic Carotid Atherosclerosis
4.3. Plasma BLVRB Measurement Can Be Used to Monitor Response to Antiangiogenic Therapy
4.4. Limitations
5. Conclusions
6. Clinical Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BLVRB | Biliverdin reductase B |
| IPH | Intraplaque hemorrhage |
| MRI | Magnetic resonance imaging |
| VEGFR-2 | Vascular endothelial growth factor receptor 2 |
| BiKE | Biobank of Karolinska Endarterectomies |
| PARISK | Plaque At RISK |
References
- Heck, D.; Jost, A. Carotid stenosis, stroke, and carotid artery revascularization. Prog. Cardiovasc. Dis. 2021, 65, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.-B.; Virmani, R.; Arbustini, E.; Pasterkamp, G. Intraplaque haemorrhages as the trigger of plaque vulnerability. Eur. Heart J. 2011, 32, 1977–1985. [Google Scholar] [CrossRef]
- Hosseini, A.A.; Kandiyil, N.; MacSweeney, S.T.S.; Altaf, N.; Auer, D.P. Carotid plaque hemorrhage on magnetic resonance imaging strongly predicts recurrent ischemia and stroke. Ann. Neurol. 2013, 73, 774–784. [Google Scholar] [CrossRef] [PubMed]
- Dijk, A.C.v.; Truijman, M.T.B.; Hussain, B.; Zadi, T.; Saiedie, G.; Rotte, A.A.J.d.; Liem, M.I.; van der Steen, A.F.W.; Daemen, M.J.A.P.; Koudstaal, P.J.; et al. Intraplaque Hemorrhage and the Plaque Surface in Carotid Atherosclerosis: The Plaque At RISK Study (PARISK). Am. J. Neuroradiol. 2015, 36, 2127–2133. [Google Scholar] [CrossRef]
- Parma, L.; Baganha, F.; Quax, P.H.A.; de Vries, M.R. Plaque angiogenesis and intraplaque hemorrhage in atherosclerosis. Eur. J. Pharmacol. 2017, 816, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Levy, A.P.; Moreno, P.R. Intraplaque Hemorrhage. Curr. Mol. Med. 2006, 6, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.-B.; Martin-Ventura, J.L.; Nicoletti, A.; Ho-Tin-Noé, B. Pathology of human plaque vulnerability: Mechanisms and consequences of intraplaque haemorrhages. Atherosclerosis 2014, 234, 311–319. [Google Scholar] [CrossRef]
- Van der Veken, B.; De Meyer, G.R.; Martinet, W. Intraplaque neovascularization as a novel therapeutic target in advanced atherosclerosis. Expert Opin. Ther. Targets 2016, 20, 1247–1257. [Google Scholar] [CrossRef]
- de Vries, M.R.; Parma, L.; Peters, H.A.B.; Schepers, A.; Hamming, J.F.; Jukema, J.W.; Goumans, M.J.T.H.; Guo, L.; Finn, A.V.; Virmani, R.; et al. Blockade of vascular endothelial growth factor receptor 2 inhibits intraplaque haemorrhage by normalization of plaque neovessels. J. Intern. Med. 2019, 285, 59–74. [Google Scholar] [CrossRef]
- Touyz, R.M.; Lang, N.N.; Herrmann, J.; van den Meiracker, A.H.; Jan Danser, A.H. Recent advances in hypertension and cardiovascular toxicities with vascular endothelial growth factor (VEGF) inhibition. Hypertension 2017, 70, 220–226. [Google Scholar] [CrossRef]
- Mura, M.; Della Schiava, N.; Long, A.; Chirico, E.N.; Pialoux, V.; Millon, A. Carotid intraplaque haemorrhage: Pathogenesis, histological classification, imaging methods and clinical value. Ann. Transl. Med. 2020, 8, 1273. [Google Scholar] [CrossRef] [PubMed]
- Kassem, M.; Florea, A.; Mottaghy, F.M.; van Oostenbrugge, R.; Kooi, M.E. Magnetic resonance imaging of carotid plaques: Current status and clinical perspectives. Ann. Transl. Med. 2020, 8, 1266. [Google Scholar] [CrossRef] [PubMed]
- Saam, T.; Hetterich, H.; Hoffmann, V.; Yuan, C.; Dichgans, M.; Poppert, H.; Koeppel, T.; Hoffmann, U.; Reiser, M.F.; Bamberg, F. Meta-analysis and systematic review of the predictive value of carotid plaque hemorrhage on cerebrovascular events by magnetic resonance imaging. J. Am. Coll. Cardiol. 2013, 62, 1081–1091. [Google Scholar] [CrossRef] [PubMed]
- McNally, J.S.; Kim, S.-E.; Mendes, J.; Hadley, J.R.; Sakata, A.; De Havenon, A.H.; Treiman, G.S.; Parker, D.L. Magnetic Resonance Imaging Detection of Intraplaque Hemorrhage. Magn. Reson. Insights 2017, 10, 1–8. [Google Scholar] [CrossRef]
- Nies, K.P.H.; Smits, L.J.M.; Kassem, M.; Nederkoorn, P.J.; van Oostenbrugge, R.J.; Kooi, M.E. Emerging Role of Carotid MRI for Personalized Ischemic Stroke Risk Prediction in Patients With Carotid Artery Stenosis. Front. Neurol. 2021, 12, 718438. [Google Scholar] [CrossRef]
- Koole, D.; Heyligers, J.; Moll, F.L.; Pasterkamp, G. Intraplaque neovascularization and hemorrhage: Markers for cardiovascular risk stratification and therapeutic monitoring. J. Cardiovasc. Med. 2012, 13, 635–639. [Google Scholar] [CrossRef]
- Pereira, P.J.; Macedo-Ribeiro, S.; Párraga, A.; Pérez-Luque, R.; Cunningham, O.; Darcy, K.; Mantle, T.J.; Coll, M. Structure of human biliverdin IXbeta reductase, an early fetal bilirubin IXbeta producing enzyme. Nat. Struct. Biol. 2001, 8, 215–220. [Google Scholar] [CrossRef]
- Matic, L.P.; Jesus Iglesias, M.; Vesterlund, M.; Lengquist, M.; Hong, M.-G.; Saieed, S.; Sanchez-Rivera, L.; Berg, M.; Razuvaev, A.; Kronqvist, M.; et al. Novel Multiomics Profiling of Human Carotid Atherosclerotic Plaques and Plasma Reveals Biliverdin Reductase B as a Marker of Intraplaque Hemorrhage. JACC Basic Transl. Sci. 2018, 3, 464–480. [Google Scholar] [CrossRef]
- Truijman, M.T.B.; Kooi, M.E.; van Dijk, A.C.; de Rotte, A.A.J.; van der Kolk, A.G.; Liem, M.I.; Schreuder, F.H.B.M.; Boersma, E.; Mess, W.H.; van Oostenbrugge, R.J.; et al. Plaque at RISK (PARISK): Prospective Multicenter Study to Improve Diagnosis of High-Risk Carotid Plaques. Int. J. Stroke 2014, 9, 747–754. [Google Scholar] [CrossRef]
- van Dam-Nolen, D.H.K.; Truijman, M.T.B.; van der Kolk, A.G.; Liem, M.I.; Schreuder, F.H.B.M.; Boersma, E.; Daemen, M.J.A.P.; Mess, W.H.; van Oostenbrugge, R.J.; van der Steen, A.F.W.; et al. Carotid Plaque Characteristics Predict Recurrent Ischemic Stroke and TIA: The PARISK (Plaque At RISK) Study. JACC Cardiovasc. Imaging 2022, 15, 1715–1726. [Google Scholar] [CrossRef]
- Dilba, K.; van Dijk, A.C.; Crombag, G.A.J.C.; van der Steen, A.F.W.; Daemen, M.J.; Koudstaal, P.J.; Nederkoorn, P.J.; Hendrikse, J.; Kooi, M.E.; van der Lugt, A.; et al. Association between Intraplaque Hemorrhage and Vascular Remodeling in Carotid Arteries: The Plaque at RISK (PARISK) Study. CED 2021, 50, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Mitsumori, L.M.; Ferguson, M.S.; Polissar, N.L.; Echelard, D.; Ortiz, G.; Small, R.; Davies, J.W.; Kerwin, W.S.; Hatsukami, T.S. In Vivo Accuracy of Multispectral Magnetic Resonance Imaging for Identifying Lipid-Rich Necrotic Cores and Intraplaque Hemorrhage in Advanced Human Carotid Plaques. Circulation 2001, 104, 2051–2056. [Google Scholar] [CrossRef] [PubMed]
- Cappendijk, V.C.; Cleutjens, K.B.J.M.; Heeneman, S.; Schurink, G.W.H.; Welten, R.J.T.J.; Kessels, A.G.H.; van Suylen, R.J.; Daemen, M.J.A.P.; van Engelshoven, J.M.A.; Kooi, M.E. In vivo detection of hemorrhage in human atherosclerotic plaques with magnetic resonance imaging. J. Magn. Reson. Imaging 2004, 20, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Lardenoye, J.; de Vries, M.; Löwik, C.; Xu, Q.; Dhore, C.; Cleutjens, J.; van Hinsbergh, V.; van Bockel, J.; Quax, P. Accelerated Atherosclerosis and Calcification in Vein Grafts. Circ. Res. 2002, 91, 577–584. [Google Scholar] [CrossRef] [PubMed]
- De Vries, M.R.; Niessen, H.W.M.; Löwik, C.W.G.M.; Hamming, J.F.; Jukema, J.W.; Quax, P.H.A. Plaque Rupture Complications in Murine Atherosclerotic Vein Grafts Can Be Prevented by TIMP-1 Overexpression. PLoS ONE 2012, 7, e47134. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.; Schinner, R.; Altaf, N.; Hosseini, A.A.; Simpson, R.J.; Esposito-Bauer, L.; Singh, N.; Kwee, R.M.; Kurosaki, Y.; Yamagata, S.; et al. Prediction of Stroke Risk by Detection of Hemorrhage in Carotid Plaques: Meta-Analysis of Individual Patient Data. JACC Cardiovasc. Imaging 2020, 13, 395–406. [Google Scholar] [CrossRef]
- Naylor, A.R.; Sillesen, H.; Schroeder, T.V. Clinical and imaging features associated with an increased risk of early and late stroke in patients with symptomatic carotid disease. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 513–523. [Google Scholar] [CrossRef]
- Aday, A.W.; Ridker, P.M. Targeting Residual Inflammatory Risk: A Shifting Paradigm for Atherosclerotic Disease. Front. Cardiovasc. Med. 2019, 6, 16. [Google Scholar] [CrossRef]
- Wang, Y.; Osborne, M.T.; Tung, B.; Li, M.; Li, Y. Imaging Cardiovascular Calcification. J. Am. Heart Assoc. 2018, 7, e008564. [Google Scholar] [CrossRef]
- Verhoeven, B.; Hellings, W.E.; Moll, F.L.; de Vries, J.P.; de Kleijn, D.P.V.; de Bruin, P.; Busser, E.; Schoneveld, A.H.; Pasterkamp, G. Carotid atherosclerotic plaques in patients with transient ischemic attacks and stroke have unstable characteristics compared with plaques in asymptomatic and amaurosis fugax patients. J. Vasc. Surg. 2005, 42, 1075–1081. [Google Scholar] [CrossRef]
- Baganha, F.; de Jong, R.C.M.; Peters, E.A.; Voorham, W.; Jukema, J.W.; Delibegovic, M.; de Vries, M.R.; Quax, P.H.A. Atorvastatin pleiotropically decreases intraplaque angiogenesis and intraplaque haemorrhage by inhibiting ANGPT2 release and VE-Cadherin internalization. Angiogenesis 2021, 24, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Mao, W.; Chai, Y.; Dai, J.; Chen, Q.; Wang, L.; Zhuang, Q.; Pan, Y.; Chen, M.; Ni, G.; et al. Angiogenesis Inhibitor, Endostar, Prevents Vasa Vasorum Neovascularization in a Swine Atherosclerosis Model. J. Atheroscler. Thromb. 2015, 22, 1100–1112. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Chandramouli, C.; Allocco, B.; Gong, E.; Lam, C.S.P.; Yan, L.L. Women’s Participation in Cardiovascular Clinical Trials From 2010 to 2017. Circulation 2020, 141, 540–548. [Google Scholar] [CrossRef] [PubMed]
- van Dam-Nolen, D.H.K.; van Egmond, N.C.M.; Dilba, K.; Nies, K.; van der Kolk, A.G.; Liem, M.I.; Kooi, M.E.; Hendrikse, J.; Nederkoorn, P.J.; Koudstaal, P.J.; et al. Sex Differences in Plaque Composition and Morphology Among Symptomatic Patients With Mild-to-Moderate Carotid Artery Stenosis. Stroke 2022, 53, 370–378. [Google Scholar] [CrossRef]
- Naylor, A.R.; Ricco, J.-B.; de Borst, G.J.; Debus, S.; de Haro, J.; Halliday, A.; Hamilton, G.; Kakisis, J.; Kakkos, S.; Lepidi, S.; et al. Editor’s Choice-Management of Atherosclerotic Carotid and Vertebral Artery Disease: 2017 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 3–81. [Google Scholar] [CrossRef]
- Kamtchum-Tatuene, J.; Nomani, A.Z.; Falcione, S.; Munsterman, D.; Sykes, G.; Joy, T.; Spronk, E.; Vargas, M.I.; Jickling, G.C. Non-stenotic Carotid Plaques in Embolic Stroke of Unknown Source. Front. Neurol. 2021, 12, 719329. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | No IPH (n = 96) | IPH (n = 65) | p-Value * |
|---|---|---|---|
| (%) | (%) | ||
| Male | 61.5 | 89.2 | <0.001 |
| Baseline event between groups: | |||
| Ischemic stroke | 38.5 | 55.4 | 0.071 |
| TIA | 50.0 | 32.3 | |
| AFX | 11.5 | 12.3 | |
| Hemispheric symptoms only: | |||
| Ischemic stroke | 43.5 | 63.2 | 0.022 |
| TIA | 56.5 | 36.8 | |
| Major compared to minor events: | |||
| Ischemic stroke | 38.5 | 55.4 | 0.035 |
| TIA or AFX | 61.5 | 44.6 | |
| Smoking | |||
| Never | 28.4 | 18.5 | 0.027 |
| Former | 46.3 | 67.7 | |
| Current | 25.3 | 13.8 | |
| Hypertension | 63.3 | 73.8 | 0.156 |
| Diabetes mellitus | 21.9 | 23.1 | 0.857 |
| Hypercholesterolemia | 59.8 | 69.2 | 0.225 |
| Antihypertensive therapy | 58.3 | 64.6 | 0.423 |
| Antidiabetic drug use | 18.8 | 18.5 | 0.963 |
| Statin drug use | 49 | 50 | 0.897 |
| Antiplatelet drug use | 36.5 | 51.6 | 0.058 |
| Oral ACO drug use | 4.2 | 0 | 0.096 |
| Stenosis degree (NASCET) | 13.6 ± 16.3 | 22.6 ± 17.2 | 0.002 |
| Mean ± SD | Mean ± SD | p value | |
| Age (years) | 68.1 ± 9.5 | 70.7 ± 7.7 | 0.068 |
| BMI (kg/m2) | 26.9 ± 4.3 | 26.4 ± 4.3 | 0.464 |
| CRP levels (mg/L) | 3.6 ± 5.3 | 2.7 ± 6.9 | 0.397 |
| LDL-C (mmol/L) | 3.4 ± 1.0 | 2.9 ± 1.0 | 0.033 |
| Parameters | N | Mean | Std. Deviation | Q1–Q3 | * p-Value | |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male | 103 | 633.2 | 605.1 | 287.0–644.8 | 0.330 | |
| Female | 38 | 524.0 | 540.2 | 227.7–567.1 | ||
| Clinical admission | ||||||
| Ischemic stroke | 66 | 579.8 | 527.4 | 273.2–661.5 | 0.223 | |
| TIA | 60 | 681.9 | 701.8 | 263.5–632.4 | ||
| AFX | 15 | 397.2 | 114.8 | 258.3–505.9 | ||
| Smoking | ||||||
| Never | 32 | 756.3 | 674.3 | 289.7–1135.9 | 0.164 | |
| Former | 78 | 525.7 | 508.2 | 227.0–567.5 | ||
| Current | 30 | 641.7 | 675.5 | 271.7–613.0 | ||
| Hypertension | ||||||
| No | 43 | 626.4 | 692.5 | 262.9–574.4 | 0.761 | |
| Yes | 97 | 593.4 | 543.0 | 268.1–628.1 | ||
| Diabetes mellitus | ||||||
| No | 107 | 634.7 | 626.5 | 285.5–574.4 | 0.271 | |
| Yes | 34 | 506.7 | 442.3 | 221.1–543.5 | ||
| Hypercholesterolemia | ||||||
| No | 52 | 672.7 | 749.2 | 228.2–707.2 | 0.360 | |
| Yes | 86 | 577.3 | 472.5 | 310.4–593.7 | ||
| Antihypertensive therapy | ||||||
| No | 53 | 731.1 | 735.0 | 268.5–786.2 | 0.120 | |
| Yes | 88 | 527.2 | 467.5 | 226.6–564.8 | ||
| Antidiabetic drug use | ||||||
| No | 112 | 636.2 | 614.8 | 285.9–583.4 | 0.220 | |
| Yes | 29 | 478.7 | 461.1 | 211.1–629.1 | ||
| Statin drug use | ||||||
| No | 69 | 670.0 | 675.8 | 253.5–684.2 | 0.270 | |
| Yes | 71 | 543.9 | 489.4 | 282.6–584.1 | ||
| Antiplatelet drug use | ||||||
| No | 81 | 587.0 | 580.0 | 233.7–582.6 | 0.656 | |
| Yes | 59 | 632.2 | 607.3 | 299.4–636.0 | ||
| Oral ACO drug use | ||||||
| No | 137 | 604.7 | 596.3 | 264.0–581.1 | 0.914 | |
| Yes | 4 | 572.2 | 199.8 | 361.9–722.6 | ||
| Stenosis Degree median (NASCET) | ||||||
| Stenosis < 30% | 87 | 605.4 | 618.9 | 248.1–581.2 | 0.907 | |
| Stenosis > 30% | 37 | 619.4 | 594.1 | 269.5–579.3 | ||
| IPH | ||||||
| Absent | 87 | 520.9 | 499.4 | 237.8–581.1 | 0.033 | |
| Present (>0) | 54 | 737.3 | 693.2 | 300.9–910.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chemaly, M.; Marlevi, D.; Iglesias, M.-J.; Lengquist, M.; Kronqvist, M.; Bos, D.; van Dam-Nolen, D.H.K.; van der Kolk, A.; Hendrikse, J.; Kassem, M.; et al. Biliverdin Reductase B Is a Plasma Biomarker for Intraplaque Hemorrhage and a Predictor of Ischemic Stroke in Patients with Symptomatic Carotid Atherosclerosis. Biomolecules 2023, 13, 882. https://doi.org/10.3390/biom13060882
Chemaly M, Marlevi D, Iglesias M-J, Lengquist M, Kronqvist M, Bos D, van Dam-Nolen DHK, van der Kolk A, Hendrikse J, Kassem M, et al. Biliverdin Reductase B Is a Plasma Biomarker for Intraplaque Hemorrhage and a Predictor of Ischemic Stroke in Patients with Symptomatic Carotid Atherosclerosis. Biomolecules. 2023; 13(6):882. https://doi.org/10.3390/biom13060882
Chicago/Turabian StyleChemaly, Melody, David Marlevi, Maria-Jesus Iglesias, Mariette Lengquist, Malin Kronqvist, Daniel Bos, Dianne H. K. van Dam-Nolen, Anja van der Kolk, Jeroen Hendrikse, Mohamed Kassem, and et al. 2023. "Biliverdin Reductase B Is a Plasma Biomarker for Intraplaque Hemorrhage and a Predictor of Ischemic Stroke in Patients with Symptomatic Carotid Atherosclerosis" Biomolecules 13, no. 6: 882. https://doi.org/10.3390/biom13060882