
Concurrent Change in Serum Cholinesterase Activity and Midregional-Proadrennomedullin Level Could Predict Patient Outcome following Liver Transplantation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
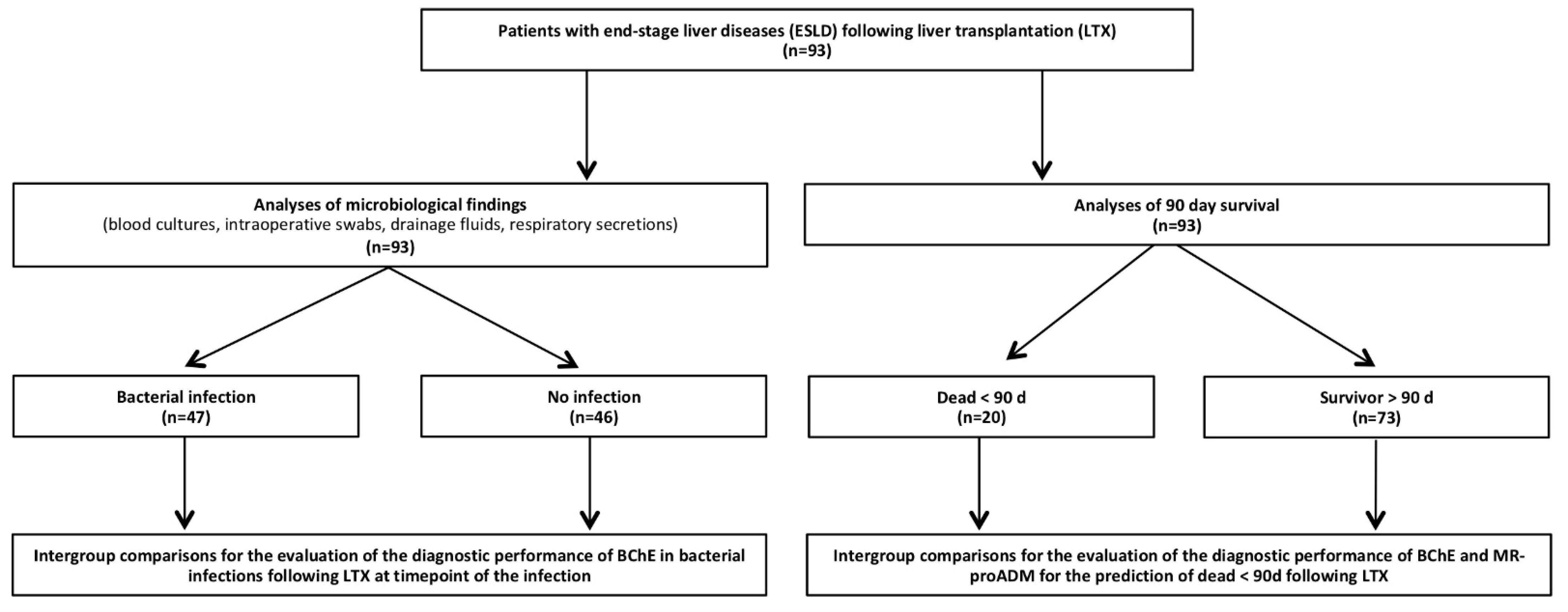
2.1. Study Design
2.2. Study Group Definitions
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
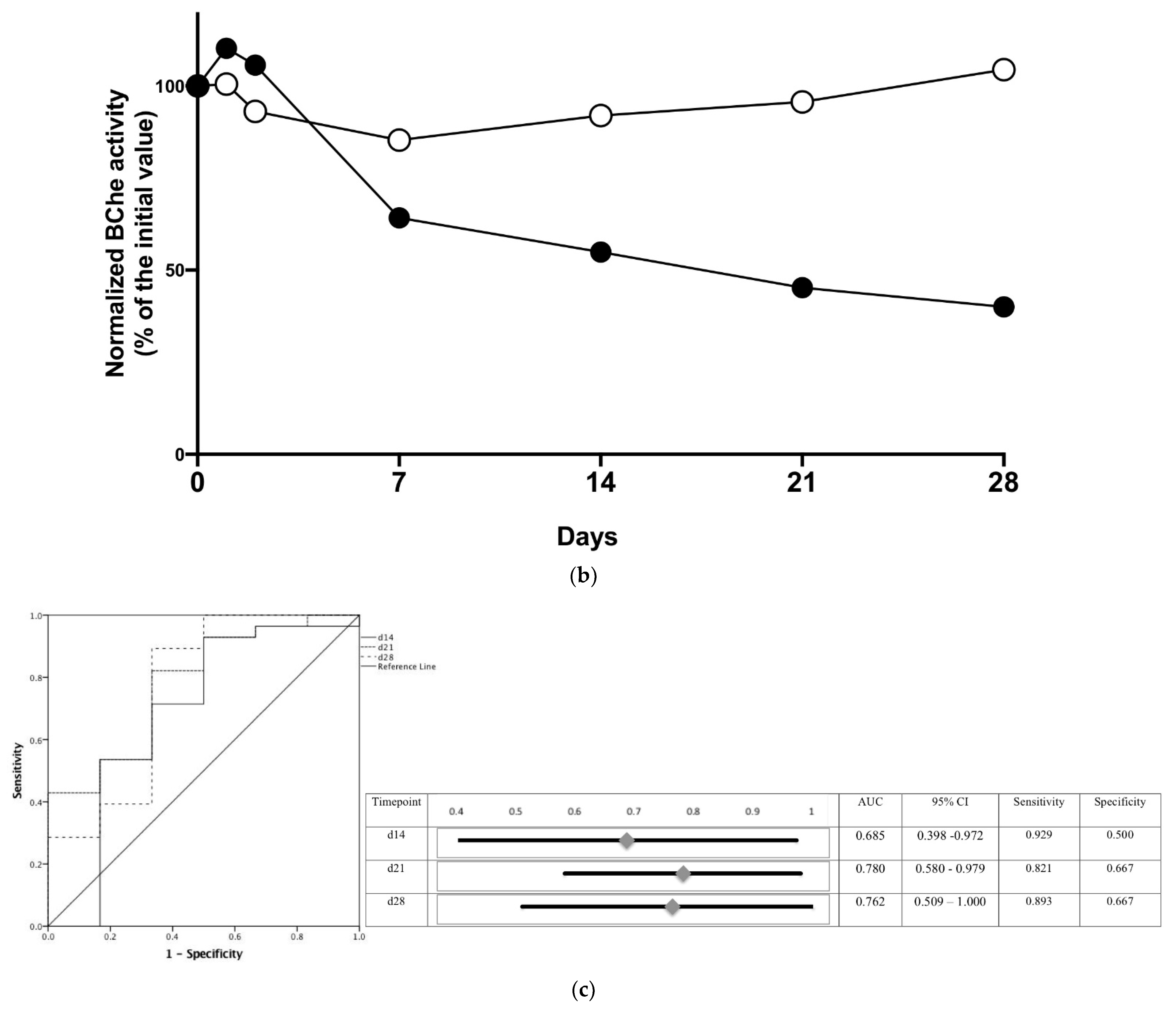
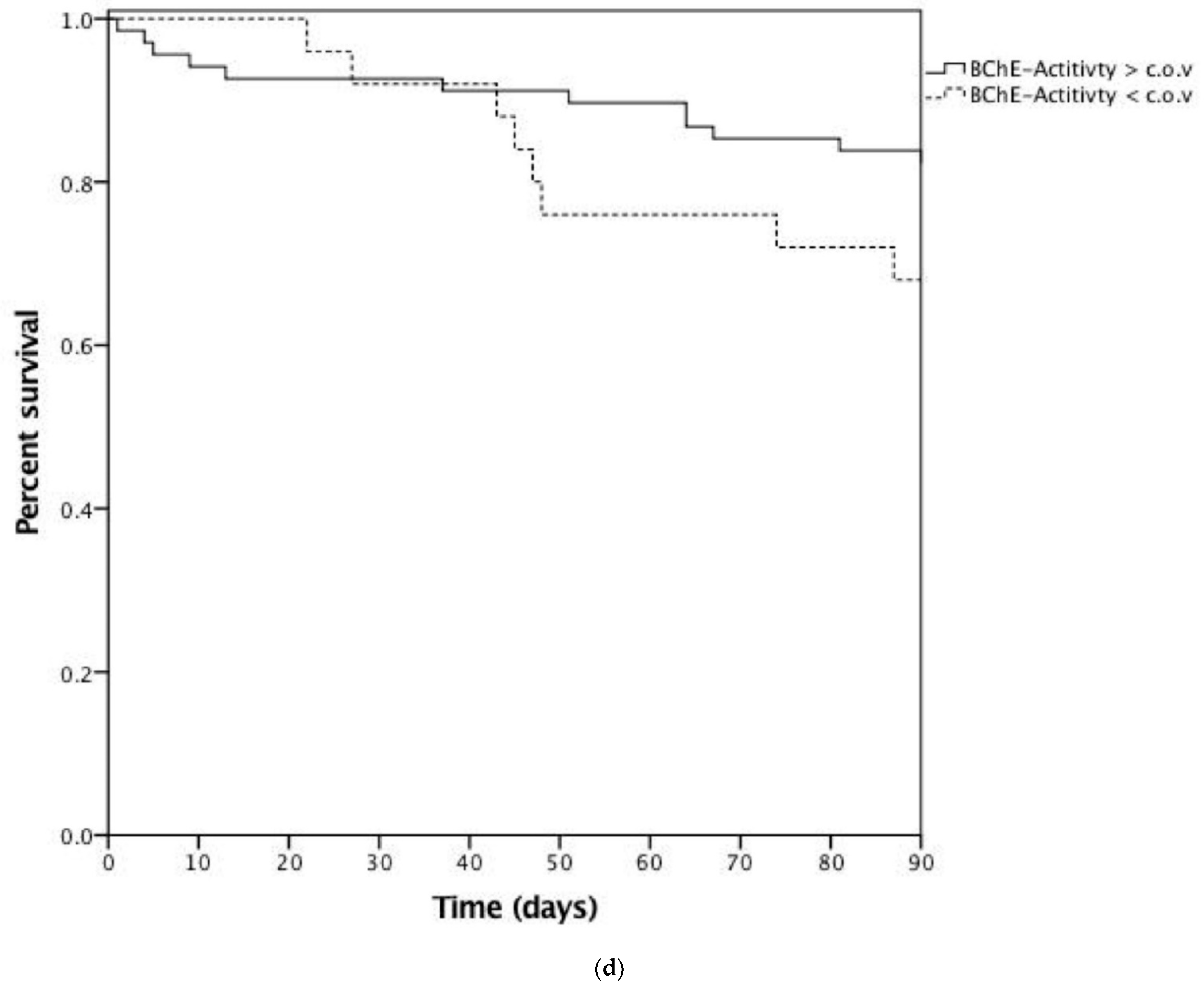
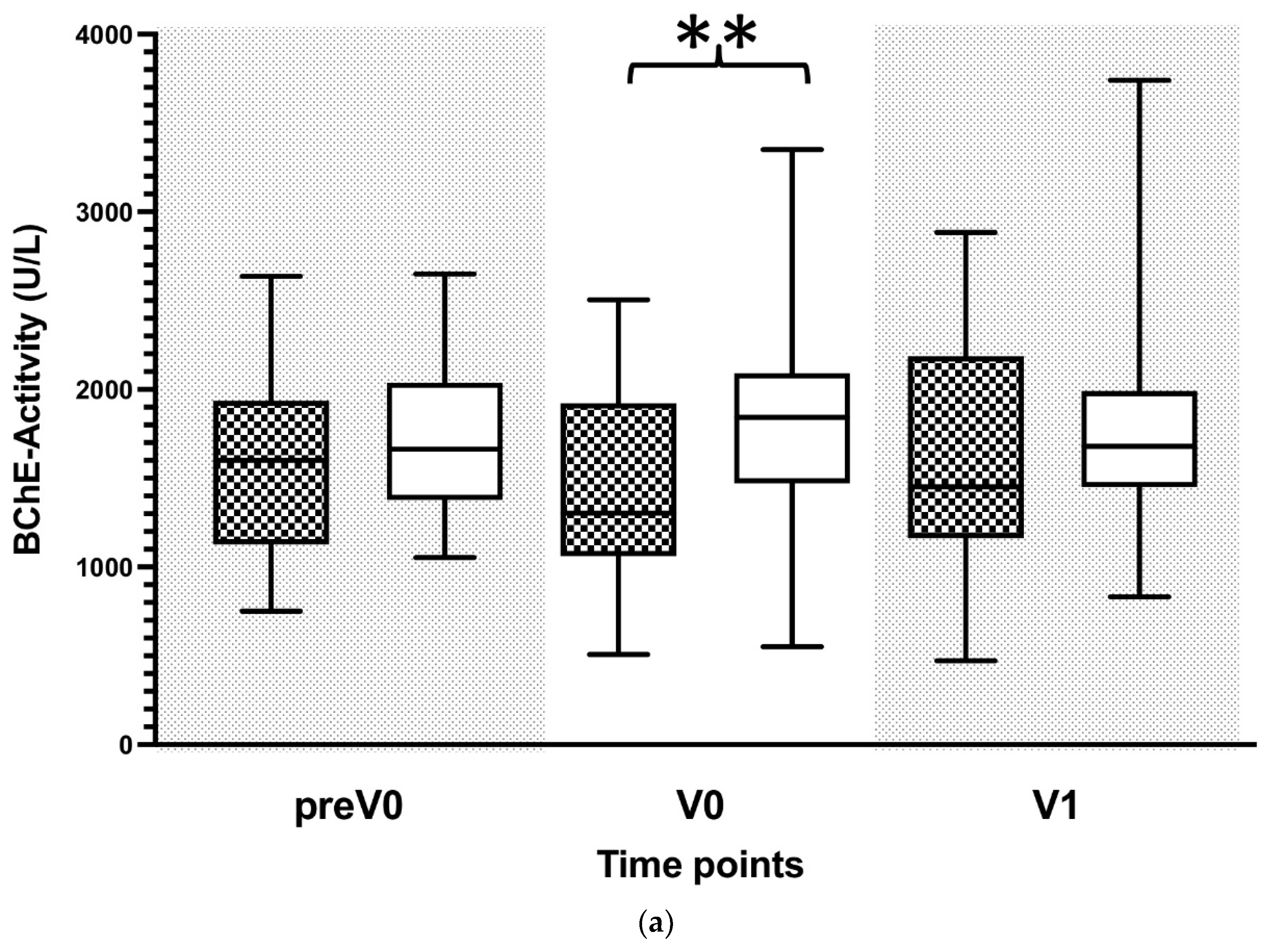
3.2. Reduced BChE Activity Predicts Patient Outcome
3.3. Reduced BChE Activity Is Associated with Systemic Inflammation
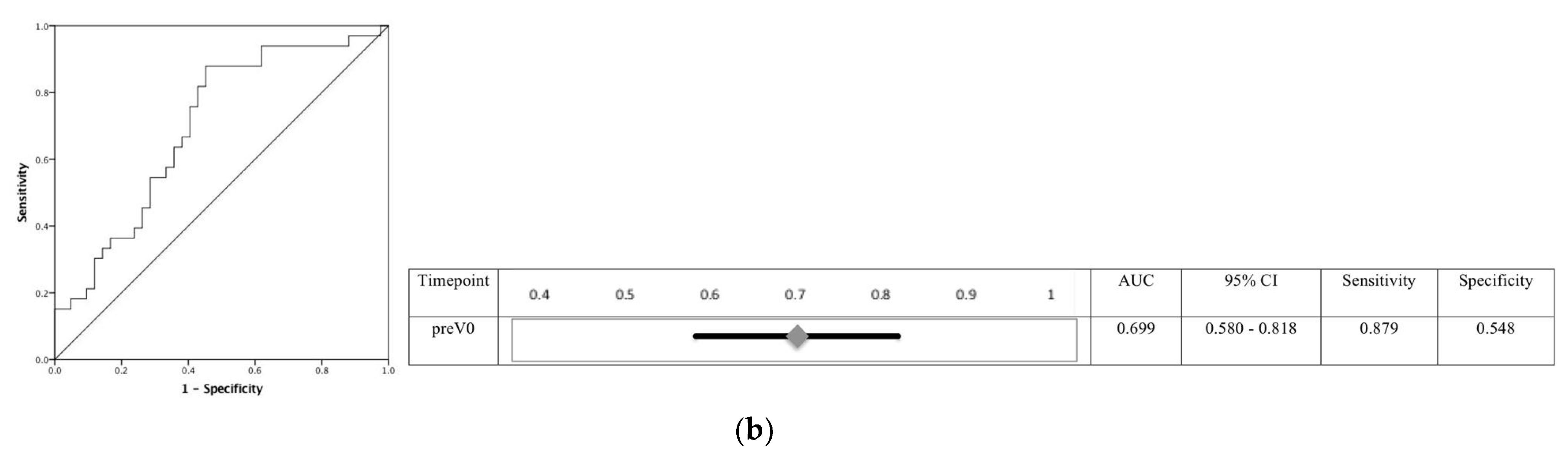
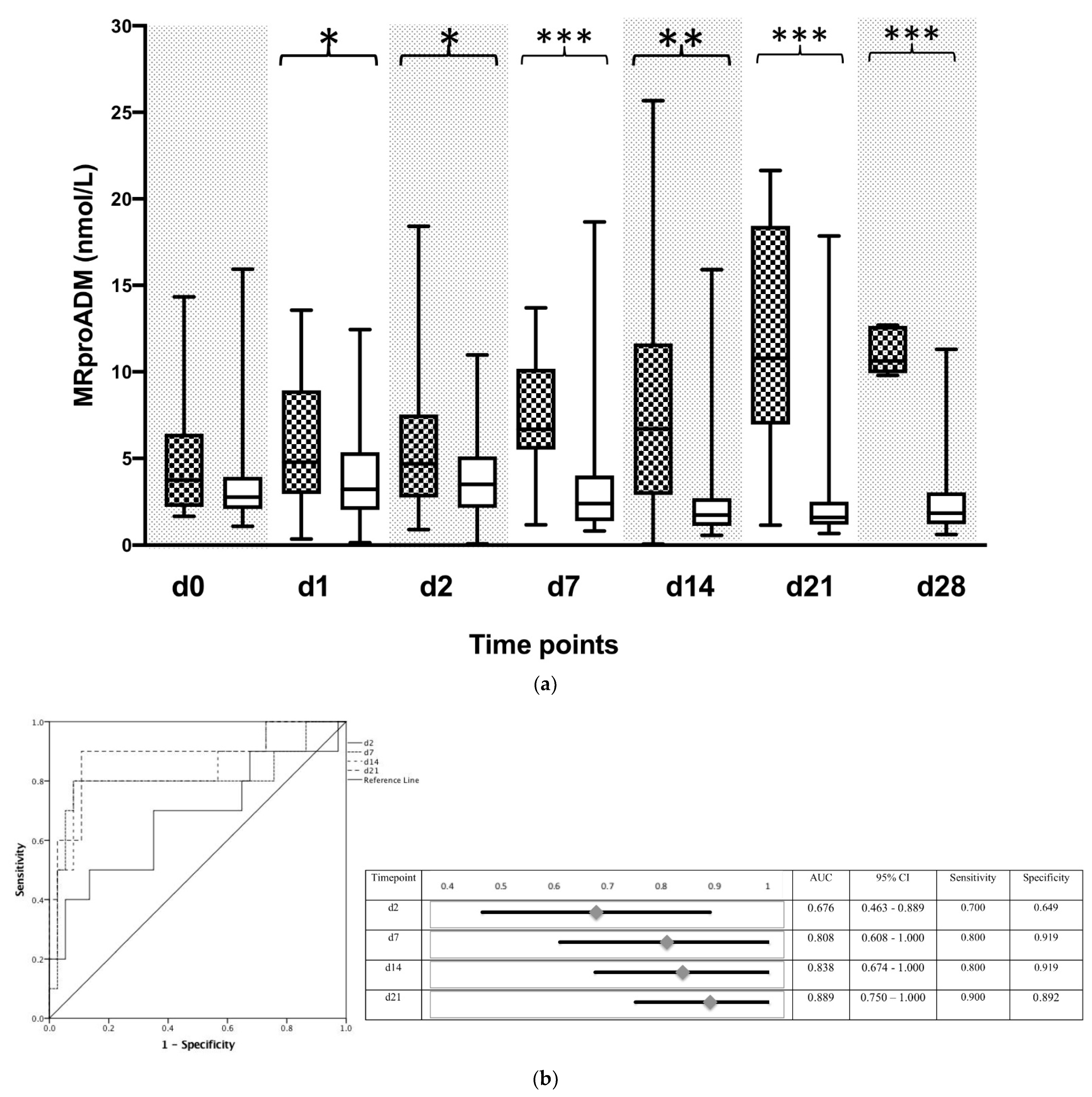
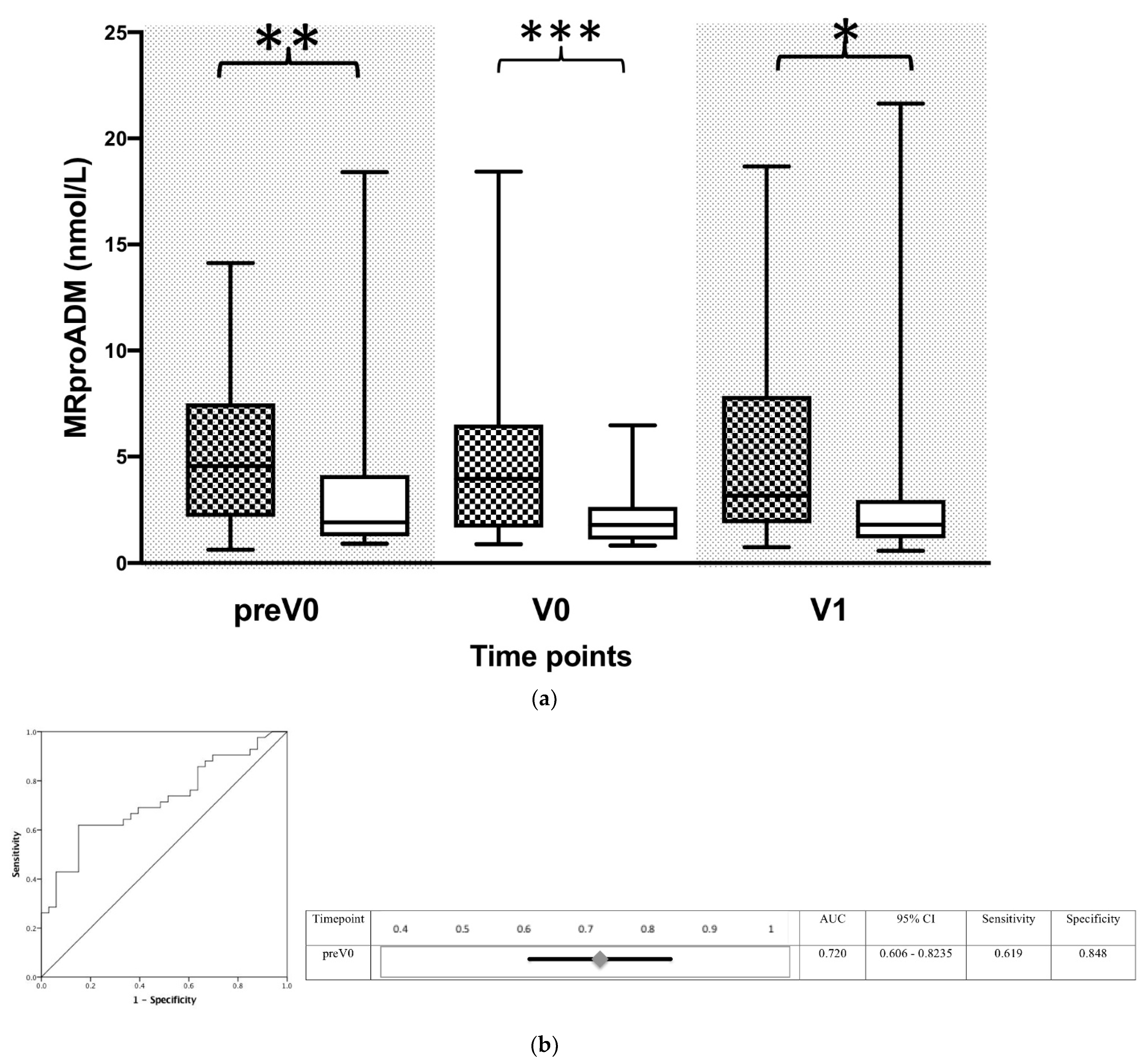
3.4. Increased MR-ProADM Activity in Blood Indicates a Commencing Bacterial Infection in Transplanted Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trunecka, P. Immunosuppression after liver transplant, now and in future. Vnitr. Lek. 2013, 59, 671–677. [Google Scholar] [PubMed]
- Astarcioglu, I.; Egeli, T.; Gulcu, A.; Ozbilgin, M.; Agalar, C.; Cesmeli, E.B.; Kaya, E.; Karademir, S.; Unek, T. Vascular complications after liver transplantation. Exp. Clin. Transplant. 2019, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Winston, D.J.; Emmanouilides, C.; Busuttil, R.W. Infections in liver transplant recipients. Clin. Infect. Dis. 1995, 21, 1077–1089. [Google Scholar] [CrossRef] [PubMed]
- Zeair, S.; Stasiuk, R.; Zair, L.; Wawrzynowicz-Syczewska, M.; Rybicka, A.; Grochans, E.; Kazimierczak, A. Incidents and risk factors of biliary complications after orthotropic liver transplantation. Medicine 2021, 100, e26994. [Google Scholar] [CrossRef]
- Fishman, J.A. Infection in solid-organ transplant recipients. N. Engl. J. Med. 2007, 357, 2601–2614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.I. Bacterial infection after liver transplantation. World J. Gastroenterol. 2014, 20, 6211–6220. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kim, S.I.; Wie, S.H.; Kim, Y.R.; Hur, J.A.; Choi, J.Y.; Yoon, S.K.; Moon, I.S.; Kim, D.G.; Lee, M.D.; et al. Infectious complications in living-donor liver transplant recipients: A 9-year single-center experience. Transpl. Infect. Dis. 2008, 10, 316–324. [Google Scholar] [CrossRef]
- Varghese, J.; Gomathy, N.; Rajashekhar, P.; Venugopal, K.; Olithselvan, A.; Vivekanandan, S.; Naresh, S.; Sujatha, C.; Vijaya, S.; Jayanthi, V.; et al. Perioperative bacterial infections in deceased donor and living donor liver transplant recipients. J. Clin. Exp. Hepatol. 2012, 2, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Swoboda-Kopec, E.; Kawecki, D.; Wroblewska, M.; Krawczyk, M.; Luczak, M. Epidemiology and susceptibility to antifungal agents of fungi isolated from clinical specimens from patients hospitalized in the department of general and liver surgery of the medical university of warsaw. Transplant. Proc. 2003, 35, 2298–2303. [Google Scholar] [CrossRef]
- Biron, B.M.; Ayala, A.; Lomas-Neira, J.L. Biomarkers for sepsis: What is and what might be? Biomark. Insights 2015, 10, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Gur, A.; Oguzturk, H.; Kose, A.; Turtay, M.G.; Ersan, V.; Bayindir, Y.; Ince, V.; Gurbuz, S.; Yucel, N. Prognostic value of procalcitonin, crp, serum amyloid a, lactate and il-6 markers in liver transplant patients admitted to ed with suspected infection. In Vivo 2017, 31, 1179–1185. [Google Scholar] [PubMed] [Green Version]
- Zant, R.; Melter, M.; Knoppke, B.; Ameres, M.; Kunkel, J. Kinetics of interleukin-6, procalcitonin, and c-reactive protein after pediatric liver transplantation. Transplant. Proc. 2014, 46, 3507–3510. [Google Scholar] [CrossRef] [PubMed]
- Huston, J.M.; Ochani, M.; Rosas-Ballina, M.; Liao, H.; Ochani, K.; Pavlov, V.A.; Gallowitsch-Puerta, M.; Ashok, M.; Czura, C.J.; Foxwell, B.; et al. Splenectomy inactivates the cholinergic antiinflammatory pathway during lethal endotoxemia and polymicrobial sepsis. J. Exp. Med. 2006, 203, 1623–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huston, J.M.; Wang, H.; Ochani, M.; Ochani, K.; Rosas-Ballina, M.; Gallowitsch-Puerta, M.; Ashok, M.; Yang, L.; Tracey, K.J.; Yang, H. Splenectomy protects against sepsis lethality and reduces serum hmgb1 levels. J. Immunol. 2008, 181, 3535–3539. [Google Scholar] [CrossRef] [PubMed]
- Rosas-Ballina, M.; Ochani, M.; Parrish, W.R.; Ochani, K.; Harris, Y.T.; Huston, J.M.; Chavan, S.; Tracey, K.J. Splenic nerve is required for cholinergic antiinflammatory pathway control of tnf in endotoxemia. Proc. Natl. Acad. Sci. USA 2008, 105, 11008–11013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronte, V.; Pittet, M.J. The spleen in local and systemic regulation of immunity. Immunity 2013, 39, 806–818. [Google Scholar] [CrossRef] [Green Version]
- Shih-Ching, K.; Choudhry, M.A.; Matsutani, T.; Schwacha, M.G.; Rue, L.W.; Bland, K.I.; Chaudry, I.H. Splenectomy differentially influences immune responses in various tissue compartments of the body. Cytokine 2004, 28, 101–108. [Google Scholar] [CrossRef]
- Hodler, J.; Kubik-Huch, R.A.; von Schulthess, G.K. (Eds.) Diseases of the Abdomen and Pelvis 2018–2021: Diagnostic Imaging—Idkd Book; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Andersson, U.; Tracey, K.J. Neural reflexes in inflammation and immunity. J. Exp. Med. 2012, 209, 1057–1068. [Google Scholar] [CrossRef]
- Zivkovic, A.R.; Decker, S.O.; Zirnstein, A.C.; Sigl, A.; Schmidt, K.; Weigand, M.A.; Hofer, S.; Brenner, T. A sustained reduction in serum cholinesterase enzyme activity predicts patient outcome following sepsis. Mediat. Inflamm. 2018, 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Zivkovic, A.R.; Schmidt, K.; Sigl, A.; Decker, S.O.; Brenner, T.; Hofer, S. Reduced serum butyrylcholinesterase activity indicates severe systemic inflammation in critically ill patients. Mediat. Inflamm. 2015, 2015, 274607. [Google Scholar] [CrossRef]
- Valenzuela-Sanchez, F.; Valenzuela-Mendez, B.; Rodriguez-Gutierrez, J.F.; Estella-Garcia, A.; Gonzalez-Garcia, M.A. New role of biomarkers: Mid-regional pro-adrenomedullin, the biomarker of organ failure. Ann. Transl. Med. 2016, 4, 329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, J.; Sun, Y.; Qu, H.; Wang, A.; Cao, Y.; Li, X. Prognostic value of serum proadrenomedullin in catheter-related bloodstream infection in the intensive care unit: A prospective observational study. Medicine 2018, 97, e12821. [Google Scholar] [CrossRef] [PubMed]
- Peacock, W.F. Novel biomarkers in acute heart failure: Mr-pro-adrenomedullin. Clin. Chem. Lab. Med. 2014, 52, 1433–1435. [Google Scholar] [CrossRef] [PubMed]
- Decker, S.O.; Kruger, A.; Wilk, H.; Grumaz, S.; Vainshtein, Y.; Schmitt, F.C.F.; Uhle, F.; Bruckner, T.; Zimmermann, S.; Mehrabi, A.; et al. New approaches for the detection of invasive fungal diseases in patients following liver transplantation-results of an observational clinical pilot study. Langenbecks Arch. Surg. 2019, 404, 309–325. [Google Scholar] [CrossRef]
- Mieth, M.; Schemmer, P.; Encke, J.; Weigand, M.; Weitz, J.; Werner, J.; Friess, H.; Beimler, J.; Schmied, B.; Mehrabi, A.; et al. Heidelberger Manual der Lebertransplantation; Heidelberg University Hospital: Heidelberg, Germany, 2006. [Google Scholar]
- Humar, A.; Michaels, M.; AST ID Working Group on Infectious Disease Monitoring. American society of transplantation recommendations for screening, monitoring and reporting of infectious complications in immunosuppression trials in recipients of organ transplantation. Am. J. Transplant. 2006, 6, 262–274. [Google Scholar] [CrossRef]
- Decker, S.O.; Hildebrand, D.; Bruckner, T.; Lichtenstern, C.; Heeg, K.; Weigand, M.A.; Brenner, T.; Uhle, F. Delta-like canonical notch ligand 1 in patients following liver transplantation-a secondary analysis of a prospective cohort study. Diagnostics 2020, 10, 894. [Google Scholar] [CrossRef]
- Tracey, K.J. The inflammatory reflex. Nature 2002, 420, 853–859. [Google Scholar] [CrossRef]
- Agudo, R.L.; Grande, M.A.; Roux, P.D.; Martín, E.E.; Pérez, A.P.; Martín, G.L. Procalcitonin after liver transplantation. Kinetics and correlation with postoperative complications: 12ap5-10. Eur. J. Anaesthesiol. 2014, 31, 209. [Google Scholar] [CrossRef] [Green Version]
- Ayvazoglu Soy, E.H.; Akdur, A.; Yildirim, S.; Arslan, H.; Haberal, M. Early postoperative infections after liver transplant. Exp. Clin. Transplant. 2018, 16 (Suppl. S1), 145–148. [Google Scholar]
- van Delden, C.; Stampf, S.; Hirsch, H.H.; Manuel, O.; Meylan, P.; Cusini, A.; Hirzel, C.; Khanna, N.; Weisser, M.; Garzoni, C.; et al. Burden and timeline of infectious diseases in the first year after solid organ transplantation in the swiss transplant cohort study. Clin. Infect. Dis. 2020, 71, e159–e169. [Google Scholar] [CrossRef] [Green Version]
- Berlakovich, G.A.; Imhof, M.; Karner-Hanusch, J.; Gotzinger, P.; Gollackner, B.; Gnant, M.; Hanelt, S.; Laufer, G.; Muhlbacher, F.; Steininger, R. The importance of the effect of underlying disease on rejection outcomes following orthotopic liver transplantation. Transplantation 1996, 61, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Lozanovski, V.J.; Dohler, B.; Weiss, K.H.; Mehrabi, A.; Susal, C. The differential influence of cold ischemia time on outcome after liver transplantation for different indications-who is at risk? A collaborative transplant study report. Front. Immunol. 2020, 11, 892. [Google Scholar] [CrossRef] [PubMed]
- Wacker, C.; Prkno, A.; Brunkhorst, F.M.; Schlattmann, P. Procalcitonin as a diagnostic marker for sepsis: A systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 426–435. [Google Scholar] [CrossRef]
- Sandkovsky, U.; Kalil, A.C.; Florescu, D.F. The use and value of procalcitonin in solid organ transplantation. Clin. Transplant. 2015, 29, 689–696. [Google Scholar] [CrossRef]
- Berry, P.A.; Melendez, H.V.; Wendon, J.A. Postoperative care of the liver-transplant patient. In Surgical Intensive Care Medicine; O’Donnell, J.M., Nácul, F.E., Eds.; Springer: Boston, MA, USA, 2010; pp. 629–638. [Google Scholar]
- Hickman, P.E.; Potter, J.M.; Pesce, A.J. Clinical chemistry and post-liver-transplant monitoring. Clin. Chem. 1997, 43, 1546–1554. [Google Scholar] [CrossRef]
- Jokanovic, M.; Maksimovic, M. Abnormal cholinesterase activity: Understanding and interpretation. Eur. J. Clin. Chem. Clin. Biochem. 1997, 35, 11–16. [Google Scholar]
- Rickett, D.L.; Glenn, J.F.; Beers, E.T. Central respiratory effects versus neuromuscular actions of nerve agents. Neurotoxicology 1986, 7, 225–236. [Google Scholar]
- Vucinic, S.; Zlatkovic, M.; Antonijevic, B.; Curcic, M.; Boskovic, B. Fresh frozen plasma as a successful antidotal supplement in acute organophosphate poisoning. Arh. Hig. Rada Toksikol. 2013, 64, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Ryniak, S.; Harbut, P.; Gozdzik, W.; Sokolowski, J.; Paciorek, P.; Halas, J. Whole blood transfusion in the treatment of an acute organophosphorus poisoning—A case report. Med. Sci. Monit. 2011, 17, CS109–CS111. [Google Scholar] [CrossRef] [Green Version]
- Lovely, M.J.; Patteson, S.K.; Beuerlein, F.J.; Chesney, J.T. Perioperative blood transfusion may conceal atypical pseudocholinesterase. Anesth. Analg. 1990, 70, 326–327. [Google Scholar] [CrossRef]
- Ostergaard, D.; Viby-Mogensen, J.; Hanel, H.K.; Skovgaard, L.T. Half-life of plasma cholinesterase. Acta Anaesthesiol. Scand. 1988, 32, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Muzyka, J.L.; Zhan, C.G. Model of human butyrylcholinesterase tetramer by homology modeling and dynamics simulation. J. Phys. Chem. B 2009, 113, 6543–6552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miguel, D.; Prieto, B.; Alvarez, F.V. Biological variation and prognosis usefulness of new biomarkers in liver transplantation. Clin. Chem. Lab. Med. 2013, 51, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Fabrega, E.; Crespo, J.; Casafont, F.; de La Pena, J.; Garcia-Unzueta, M.T.; Amado, J.A.; Pons-Romero, F. Adrenomedullin in liver transplantation and its relationship with vascular complications. Liver Transpl. Surg. 1999, 5, 485–490. [Google Scholar] [CrossRef]
- Geny, B.; Ellero, B.; Charloux, A.; Brandenberger, G.; Doutreleau, S.; Piquard, F. Circulating adrenomedullin is increased in relation with increased creatinine and atrial natriuretic peptide in liver-transplant recipients. Regul. Pept. 2003, 114, 61–66. [Google Scholar] [CrossRef]
- Parikh, A.; Washburn, K.W.; Matsuoka, L.; Pandit, U.; Kim, J.E.; Almeda, J.; Mora-Esteves, C.; Halff, G.; Genyk, Y.; Holland, B.; et al. A multicenter study of 30 days complications after deceased donor liver transplantation in the model for end-stage liver disease score era. Liver Transpl. 2015, 21, 1160–1168. [Google Scholar] [CrossRef]
- Eyraud, D.; Ben Ayed, S.; Tanguy, M.L.; Vezinet, C.; Siksik, J.M.; Bernard, M.; Fratea, S.; Movschin, M.; Vaillant, J.C.; Coriat, P.; et al. Procalcitonin in liver transplantation: Are high levels due to donors or recipients? Crit. Care 2008, 12, R85. [Google Scholar] [CrossRef] [Green Version]
- Cousin, V.L.; Lambert, K.; Trabelsi, S.; Galetto-Lacour, A.; Posfay-Barbe, K.M.; Wildhaber, B.E.; McLin, V.A. Procalcitonin for infections in the first week after pediatric liver transplantation. BMC Infect. Dis. 2017, 17, 149. [Google Scholar] [CrossRef] [Green Version]
- Dong, R.; Wan, B.; Lin, S.; Wang, M.; Huang, J.; Wu, Y.; Wu, Y.; Zhang, N.; Zhu, Y. Procalcitonin and liver disease: A literature review. J. Clin. Transl. Hepatol. 2019, 7, 51–55. [Google Scholar]
- Brenner, T.; Rosenhagen, C.; Brandt, H.; Schmitt, F.C.; Jung, G.E.; Schemmer, P.; Schmidt, J.; Mieth, M.; Bruckner, T.; Lichtenstern, C.; et al. Cell death biomarkers as early predictors for hepatic dysfunction in patients after orthotopic liver transplantation. Transplantation 2012, 94, 185–191. [Google Scholar] [CrossRef]
- Volkmann, X.; Anstaett, M.; Hadem, J.; Stiefel, P.; Bahr, M.J.; Lehner, F.; Manns, M.P.; Schulze-Osthoff, K.; Bantel, H. Caspase activation is associated with spontaneous recovery from acute liver failure. Hepatology 2008, 47, 1624–1633. [Google Scholar] [CrossRef] [PubMed]
- Chae, M.S.; Moon, K.U.; Chung, H.S.; Park, C.S.; Lee, J.; Choi, J.H.; Hong, S.H. Serum interleukin-6 and tumor necrosis factor-alpha are associated with early graft regeneration after living donor liver transplantation. PLoS ONE 2018, 13, e0195262. [Google Scholar] [CrossRef] [PubMed]
- Friedman, B.H.; Wolf, J.H.; Wang, L.; Putt, M.E.; Shaked, A.; Christie, J.D.; Hancock, W.W.; Olthoff, K.M. Serum cytokine profiles associated with early allograft dysfunction in patients undergoing liver transplantation. Liver Transpl. 2012, 18, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Chae, M.S.; Kim, J.W.; Chung, H.S.; Park, C.S.; Lee, J.; Choi, J.H.; Hong, S.H. The impact of serum cytokines in the development of early allograft dysfunction in living donor liver transplantation. Medicine 2018, 97, e0400. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Unit | All Patients (n = 93) | 90 d Non Survivor (n = 20) | 90 d Survivor (n = 73) | p for Non Survivor vs. Survivor |
|---|---|---|---|---|---|
| male | 58 (62%) | 9 (45%) | 49 (67.2%) | 0.062 | |
| age | (years) | 52.0 (42.0–58.0) | 52 (39.5–58.3) | 52 (45.0–58.0) | 0.626 |
| BMI | (kg/m2) | 25.5 (22.9–29.8) | 25.52 (23.2–30.5) | 26.26 (22.9–29.5) | 0.786 |
| MELD-Score | 18.0 (11.0–28.0) | 19 (12.8–25.3) | 17 (10.0–28.0) | 0.797 | |
| BAR-Score | 8.0 (3.0–13.0) | 8 (4.0–12.0) | 8 (3.0–130.) | 0.825 | |
| Causes of liver cirrhosis | |||||
| Alcohol | 27 (29%) | 9 (45%) | 18 (24.6%) | 0.070 | |
| Hepatitis B | 6 (6.5%) | 1 (5%) | 5 (6.8%) | 0.617 | |
| Hepatitis C | 10 (10.8%) | 2 (10%) | 8 (10.9%) | 0.633 | |
| HCC | 25 (26.9%) | 5 (25%) | 20 (27.4%) | 0.538 | |
| PSC | 16 (17.2%) | 1 (5%) | 15 (20.5%) | 0.090 | |
| PBC | 5 (5.4%) | 1 (5%) | 4 (5.4%) | 0.708 | |
| NASH | 7 (7.5%) | 0 (0%) | 7 (9.6%) | 0.172 | |
| Other | 20 (21.5%) | 6 (30%) | 14 (19.2%) | 0.226 | |
| Need for catecholamines before LTPL | 3 (3.2%) | 3 (15%) | 0 (0%) | 0.009 ** | |
| NYHA 0-I | 90 (96.8%) | 18 (90%) | 72 (98.6%) | 0.116 | |
| Diabetes mellitus | 18 (19.4%) | 4 (20%) | 14 (19.2%) | 0.579 | |
| Arterial hypertension | 28 (30.1%) | 5 (25%) | 23 (31.5%) | 0.548 | |
| Coronary heart disease | 10 (10.8%) | 2 (10%) | 8 (13.7%) | 0.591 | |
| Chronic obstructive lung disease | 7 (7.5%) | 2 (10%) | 5 (6.8%) | 0.489 | |
| Smoker | 21 (22.6%) | 5 (25%) | 15 (20.5%) | 0.471 | |
| Renal insufficiency | 20 (21.5%) | 4 (20%) | 16 (21.9%) | 0.535 | |
| Pre-existing ARF | 10 (10.8%) | 5 (25%) | 5 (7.1%) | 0.289 | |
| Pre-existing thrombosis | 18 (19.3%) | 8 (40%) | 10 (13.7%) | 0.132 | |
| Neurological disorder | 43 (46.2%) | 13 (65%) | 30 (41.1%) | 0.074 | |
| High-urgency | 32 (34.4%) | 4 (20%) | 28 (38.4%) | 0.101 | |
| Re-LTPL | 16 (17.2%) | 4 (20%) | 12 (16.4%) | 0.467 | |
| Immunosuppressive medication | |||||
| Corticosteroids | 93 (100%) | 23 (100%) | 70 (100%) | — | |
| Mycophenolate mofetil | 92 (98.6%) | 20 (100%) | 72 (98.6%) | 0.785 | |
| Ciclosporin | 39 (41.9%) | 8 (40%) | 31 (42.5%) | 0.526 | |
| Tacrolimus | 54 (58.1%) | 12 (60%) | 42 (57.5%) | 0.526 | |
| Parameter | Unit | All Patients (n = 93) | 90 d Non Survivor (n = 20) | 90 d Survivor (n = 73) | p for Non Survivor vs. Survivor |
|---|---|---|---|---|---|
| APACHE II+ | 27.0 (17.0–32.0) | 29.5 (23.3–34.0) | 25.0 (16.0–31.0) | 0.071 | |
| SOFA+ | 13.0 (7.0–15.0) | 13.0 (11.0–17.3) | 12.0 (6.0–15.0) | 0.017 * | |
| SAPS+ | 52.0 (30.0–69.0) | 66.5 (46.0–78.0) | 44.0 (29.0–67.0) | 0.118 | |
| Time of mechanical Ventilation | (days) | 1.0 (1.0–4.0) | 7.0 (3.3–16.3) | 1.0 (1.0–2.0) | <0.001 *** |
| Tracheostomy | 11 (11.8%) | 9 (45%) | 2 (2.7%) | <0.001 *** | |
| Hospital stay before LTPL | (days) | 1.0 (1.0–7.0) | 1.0 (1.0–1.0) | 1.0 (1.0–7.5) | 0.228 |
| ICU stay | (days) | 13.0 (8.0–24.0) | 31.5 (8.0–46.3) | 13.0 (8.0–21.0) | 0.163 |
| Hospital stay | (days) | 34.0 (25.0–52.0) | 43.0 (16.5–67.6) | 32.0 (25.0–52.0) | 0.793 |
| ALF after LTPL | 16 (16.1%) | 13 (65%) | 3 (4.1%) | <0.001 *** | |
| ARF after LTPL | 31 (33.3%) | 15 (75%) | 16 (21.9%) | <0.001 *** | |
| Dialysis | |||||
| Directly after LTPL | 6 (6.5%) | 4 (20%) | 2 (2.7%) | 0.018 * | |
| In time course | 27 (20%) | 14 (70%) | 13 (17.8%) | <0.001 *** | |
| BDA | 22 (23.7%) | 4 (20%) | 18 (24.7%) | 0.420 | |
| Duration of surgery | (min) | 347.0 (289.0–405.0) | 395.0 (306.3–441.0) | 335.0 (289.0–385.0) | 0.111 |
| Intraoperative blood loss | (L) | 3.0 (1.5–4.4) | 2.8 (1.9–7.9) | 3 (1.4–4.1) | 0.457 |
| Rejection | 20 (21.5%) | 2 (10%) | 18 (24.7%) | 0.132 | |
| Perforation of the intestine or stomach | 4 (4.3%) | 3 (15%) | 1 (1.4%) | 0.03 * | |
| BDA-insufficiency (n = 22) | 5 (22.7%) | 2 (50%) | 3 (16.7%) | 0.292 | |
| Stenosis of the bile duct | 9 (9.7%) | 2 (10%) | 7 (9.6%) | 0.620 | |
| Leakage of the bile duct | 10 (10.8%) | 2 (10%) | 8 (11%) | 0.594 | |
| Need for surgical intervention | 44 (47.3%) | 20 (100%) | 24 (32.9%) | <0.001 *** | |
| Vascular complications | 13 (14%) | 6 (30%) | 6 (8.2%) | 0.030 * | |
| Need for endoscopic diagnostics | 13 (14%) | 7 (35%) | 6 (8.2%) | 0.006 ** |
| Cause of Death | Number of Patients (n = 20) |
|---|---|
| Septic shock | 14 (70.0%) |
| Primary graft failure | 5 (25.0%) |
| Mesenterial ischemia | 1 (5.0%) |
| Ischemic graft failure | 2 (10.0%) |
| Myocardial infarction | 1 (5.0%) |
| Cerebral infarction | 1 (5.0%) |
| Systemic mycosis caused by Rhizopus microsporus | 1 (5.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Decker, S.O.; Krüger, A.; Wilk, H.; Uhle, F.; Bruckner, T.; Hofer, S.; Weigand, M.A.; Brenner, T.; Zivkovic, A.R. Concurrent Change in Serum Cholinesterase Activity and Midregional-Proadrennomedullin Level Could Predict Patient Outcome following Liver Transplantation. Biomolecules 2022, 12, 989. https://doi.org/10.3390/biom12070989
Decker SO, Krüger A, Wilk H, Uhle F, Bruckner T, Hofer S, Weigand MA, Brenner T, Zivkovic AR. Concurrent Change in Serum Cholinesterase Activity and Midregional-Proadrennomedullin Level Could Predict Patient Outcome following Liver Transplantation. Biomolecules. 2022; 12(7):989. https://doi.org/10.3390/biom12070989
Chicago/Turabian StyleDecker, Sebastian O., Albert Krüger, Henryk Wilk, Florian Uhle, Thomas Bruckner, Stefan Hofer, Markus A. Weigand, Thorsten Brenner, and Aleksandar R. Zivkovic. 2022. "Concurrent Change in Serum Cholinesterase Activity and Midregional-Proadrennomedullin Level Could Predict Patient Outcome following Liver Transplantation" Biomolecules 12, no. 7: 989. https://doi.org/10.3390/biom12070989